
The Effect of Mouthrinse with 0.05% Dexamethasone Solution on the Oral Bacterial Community of Oral Lichen Planus Patients: Prospective Pilot Study




Abstract
:1. Introduction
2. Materials and Methods
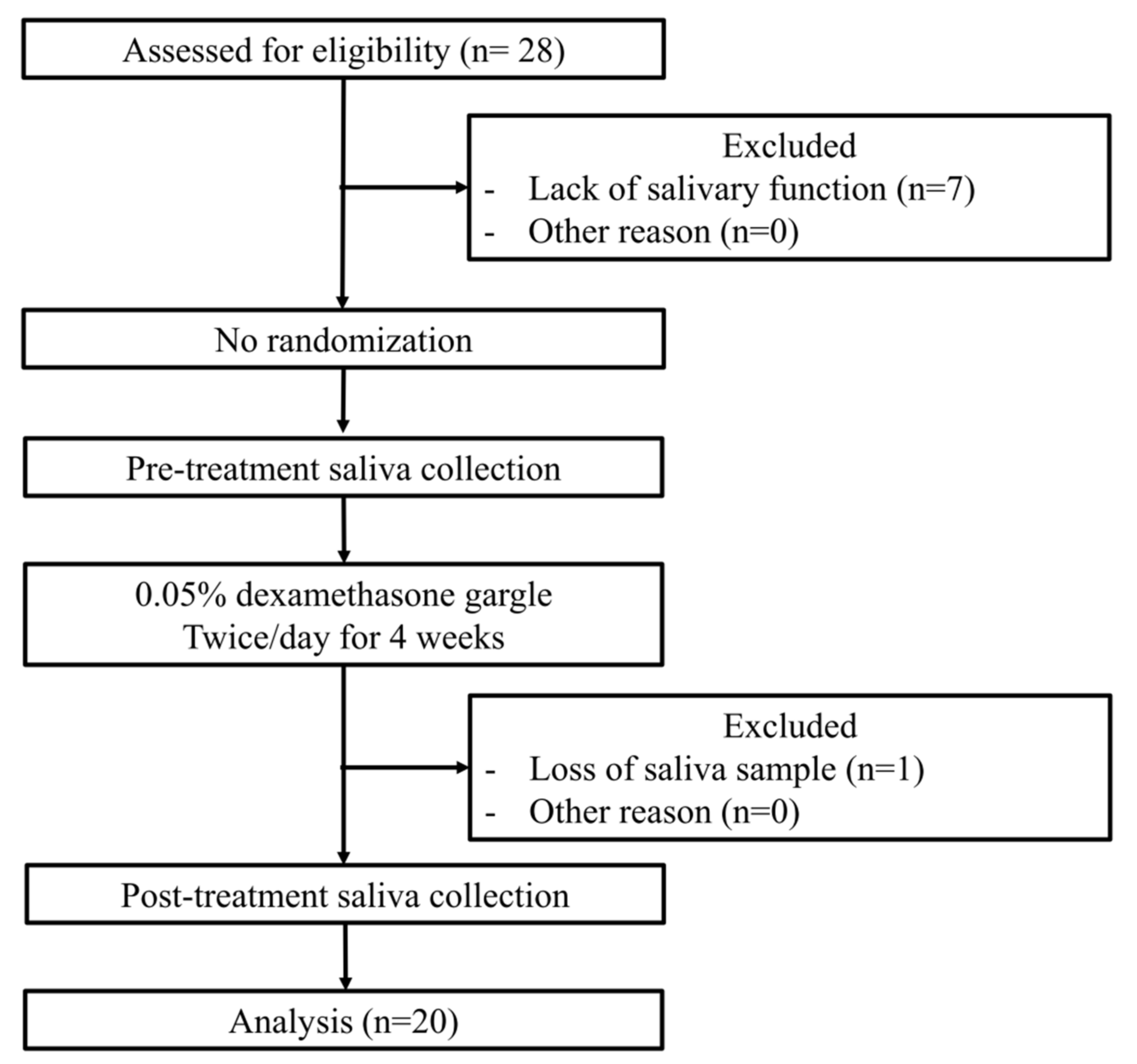
2.1. Patients
2.2. Saliva Analysis
2.3. Multiplex Quantitative Real-Time Polymerase Chain Reaction (qPCR)
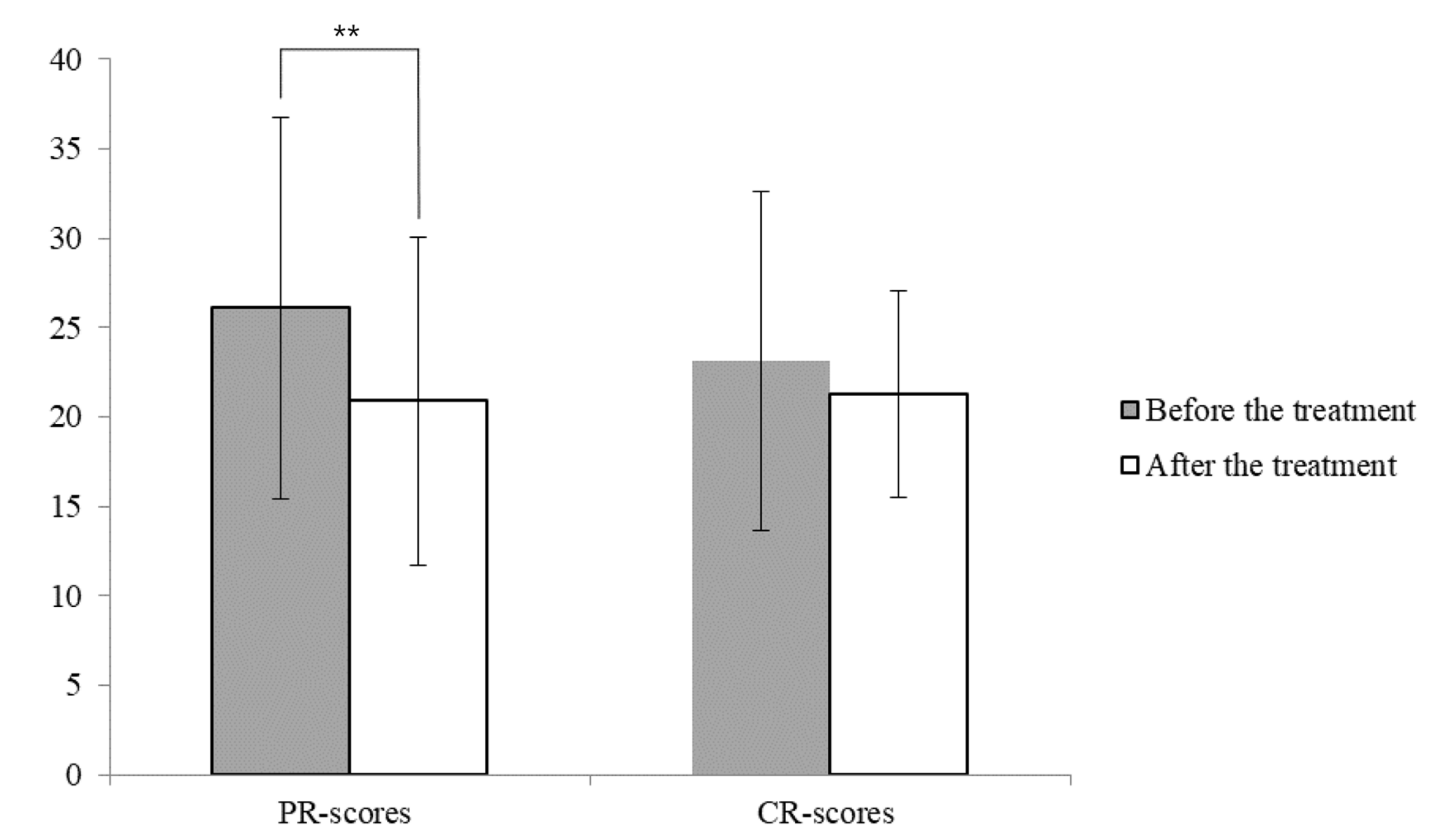
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lodi, G.; Scully, C.; Carrozzo, M.; Griffiths, M.; Sugerman, P.B.; Thongprasom, K. Current controversies in oral lichen planus: Report of an international consensus meeting. Part 1. Viral infections and etiopathogenesis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2005, 100, 40–51. [Google Scholar] [CrossRef]
- Sugerman, P.B.; Savage, N.W. Oral lichen planus: Causes, diagnosis and management. Aust. Dent. J. 2002, 47, 290–297. [Google Scholar] [CrossRef]
- Masaki, M.; Sato, T.; Sugawara, Y.; Sasano, T.; Takahashi, N. Detection and identification of non-Candida albicans species in human oral lichen planus. Microbiol. Immunol. 2011, 55, 66–70. [Google Scholar] [CrossRef]
- Levin, C.; Maibach, H.I. Topical corticosteroid-induced adrenocortical insufficiency: Clinical implications. Am. J. Clin. Dermatol. 2002, 3, 141–147. [Google Scholar] [CrossRef]
- Hegarty, A.M.; Hodgson, T.A.; Lewsey, J.D.; Porter, S.R. Fluticasone propionate spray and betamethasone sodium phosphate mouthrinse: A randomized crossover study for the treatment of symptomatic oral lichen planus. J. Am. Acad. Dermatol. 2002, 47, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Gibson, N.; Ferguson, J.W. Steroid cover for dental patients on long-term steroid medication: Proposed clinical guidelines based upon a critical review of the literature. Br. Dent. J. 2004, 197, 681–685. [Google Scholar] [CrossRef] [Green Version]
- Lodi, G.; Manfredi, M.; Mercadante, V.; Murphy, R.; Carrozzo, M. Interventions for treating oral lichen planus: Corticosteroid therapies. Cochrane Database Syst. Rev. 2020, 2, CD001168. [Google Scholar] [CrossRef] [PubMed]
- Scattarella, A.; Petruzzi, M.; Ballini, A.; Grassi, F.R.; Nardi, G.M. Oral lichen planus and dental hygiene: A case report. Int. J. Dent. Hyg. 2010, 9, 163–166. [Google Scholar] [CrossRef] [PubMed]
- González-García, A.; Diniz-Freitas, M.; Vila, P.G.; Blanco-Carrión, A.; Garcia-Garcia, A.; Gándara-Rey, J. Triamcinolone acetonide mouth rinses for treatment of erosive oral lichen planus: Efficacy and risk of fungal over-infection. Oral Dis. 2006, 12, 559–565. [Google Scholar] [CrossRef]
- Mirsepasi, H.C.; Persson, S.; Struve, C.; Andersen, L.O.B.; Petersen, A.M.; Krogfelt, K.A. Microbial diversity in fecal samples depends on DNA extraction method: easyMag DNA extraction compared to QIAamp DNA stool mini kit extraction. BMC Res. Notes 2014, 7, 50. [Google Scholar] [CrossRef] [Green Version]
- Takeshita, T.; Nakano, Y.; Kumagai, T.; Yasui, M.; Kamio, N.; Shibata, Y.; Shiota, S.; Yamashita, Y. The ecological proportion of indigenous bacterial populations in saliva is correlated with oral health status. ISME J. 2008, 3, 65–78. [Google Scholar] [CrossRef]
- Kim, S.-J.; Rim, D.; Heo, J.U.; Cho, H.-J. Possibility of predicting missing teeth using deep learning: A pilot study. J. Korean Acad. Oral Health 2019, 43, 210–216. [Google Scholar] [CrossRef] [Green Version]
- Aas, J.A.; Paster, B.J.; Stokes, L.N.; Olsen, I.; Dewhirst, F.E. Defining the Normal Bacterial Flora of the Oral Cavity. J. Clin. Microbiol. 2005, 43, 5721–5732. [Google Scholar] [CrossRef] [Green Version]
- Ballini, A.; DiPalma, G.; Isacco, C.G.; Boccellino, M.; Di Di Domenico, M.; Santacroce, L.; Nguyễn, K.C.; Scacco, S.; Calvani, M.; Boddi, A.; et al. Oral Microbiota and Immune System Crosstalk: A Translational Research. Biology 2020, 9, 131. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Martelli, F.S.; Isacco, C.G.; Borsani, E.; Cantore, S.; Corcioli, F.; Boddi, A.; Nguyễn, K.C.; De Vito, D.; Aityan, S.K.; et al. Chronic Periodontitis and Immunity, Towards the Implementation of a Personalized Medicine: A Translational Research on Gene Single Nucleotide Polymorphisms (SNPs) Linked to Chronic Oral Dysbiosis in 96 Caucasian Patients. Biomedicines 2020, 8, 115. [Google Scholar] [CrossRef] [PubMed]
- Lundström, I.M.; Anneroth, G.B.; Holmberg, K. Candida in patients with oral lichen planus. Int. J. Oral Surg. 1984, 13, 226–238. [Google Scholar] [CrossRef]
- Riggio, M.P.; Lennon, A.; Wray, D. Detection of Helicobacter pylori DNA in recurrent aphthous stomatitis tissue by PCR. J. Oral Pathol. Med. 2000, 29, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Shimoyama, T.; Horie, N.; Kato, T.; Kaneko, T.; Komiyama, K. Helicobacter pylori in oral ulcerations. J. Oral Sci. 2000, 42, 225–229. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Hakimi, B.; Persson, G.R. Microbiological Findings in Subjects With Asymptomatic Oral Lichen Planus: A Cross-Sectional Comparative Study. J. Periodontol. 2008, 79, 2347–2355. [Google Scholar] [CrossRef]
- Holmstrup, P.; Schiøtz, A.W.; Westergaard, J. Effect of dental plaque control on gingival lichen planus. Oral Surg. Oral Med. Oral Pathol. 1990, 69, 585–590. [Google Scholar] [CrossRef]
- Backman, K.; Jontell, M. Microbial-associated oral lichenoid reactions. Oral Dis. 2007, 13, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Brasil-Oliveira, R.; Cruz, Á.A.; Sarmento, V.A.; Souza-Machado, A.; Lins-Kusterer, L. Corticosteroid Use and Periodontal Disease: A Systematic Review. Eur. J. Dent. 2020, 14, 496–501. [Google Scholar]
- Wang, K.; Lu, W.; Tu, Q.; Ge, Y.; He, J.; Zhou, Y.; Gou, Y.; Van Nostrand, J.; Qin, Y.; Li, J.; et al. Preliminary analysis of salivary microbiome and their potential roles in oral lichen planus. Sci. Rep. 2016, 6, 22943. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Kim, Y.; Yoon, H.-J.; Baek, K.J.; Alam, J.; Park, H.K.; Choi, Y. The presence of bacteria within tissue provides insights into the pathogenesis of oral lichen planus. Sci. Rep. 2016, 6, 29186. [Google Scholar] [CrossRef]
- Baek, K.; Choi, Y. The microbiology of oral lichen planus: Is microbial infection the cause of oral lichen planus? Mol. Oral Microbiol. 2017, 33, 22–28. [Google Scholar] [CrossRef] [Green Version]
- Allaker, R.P.; Stephen, A.S. Use of Probiotics and Oral Health. Curr. Oral Health Rep. 2017, 4, 309–318. [Google Scholar] [CrossRef] [Green Version]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9, 69. [Google Scholar] [CrossRef]
- Costa-Pinto, A.; Lemos, A.; Tavaria, F.; Pintado, M. Chitosan and Hydroxyapatite Based Biomaterials to Circumvent Periprosthetic Joint Infections. Materials 2021, 14, 804. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Patient Number | Age | Sex | Qualitative Results of Oral Bacterial Species | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pg | Tf | Td | Fn | Pi | Pn | Sm | Smu | Ss | Change | |||
| #1 | 58 | F | N | P | N | P | N | - | P | P | - | ● |
| #2 | 67 | F | - | P | N | P | N | P | P | P | N | ● |
| #3 | 81 | F | N | N | N | P | N | N | P | N | N | |
| #4 | 70 | F | P | P | + | P | N | - | P | N | N | ● |
| #5 | 72 | F | P | P | N | P | N | P | P | N | N | |
| #6 | 67 | F | P | N | N | P | - | P | P | P | N | ● |
| #7 | 68 | F | P | P | N | P | N | P | P | + | N | ● |
| #8 | 54 | F | P | P | P | P | - | P | P | N | N | ● |
| #9 | 73 | F | P | N | N | P | N | N | P | P | N | |
| #10 | 59 | F | + | + | N | P | - | N | P | N | N | ● |
| #11 | 39 | F | N | P | N | P | N | P | P | P | N | |
| #12 | 60 | F | P | P | - | P | P | - | P | P | - | ● |
| #13 | 56 | F | N | P | N | P | N | P | P | N | N | |
| #14 | 56 | F | N | - | N | P | N | P | P | N | N | ● |
| #15 | 59 | F | + | - | - | P | N | - | P | N | N | ● |
| #16 | 72 | F | P | N | N | P | P | + | P | N | N | ● |
| #17 | 73 | M | P | N | N | P | N | N | P | P | N | |
| #18 | 53 | F | N | N | N | P | P | - | P | N | N | ● |
| #19 | 33 | F | - | - | N | P | N | P | P | N | N | ● |
| #20 | 52 | F | N | - | N | P | N | P | P | - | N | ● |
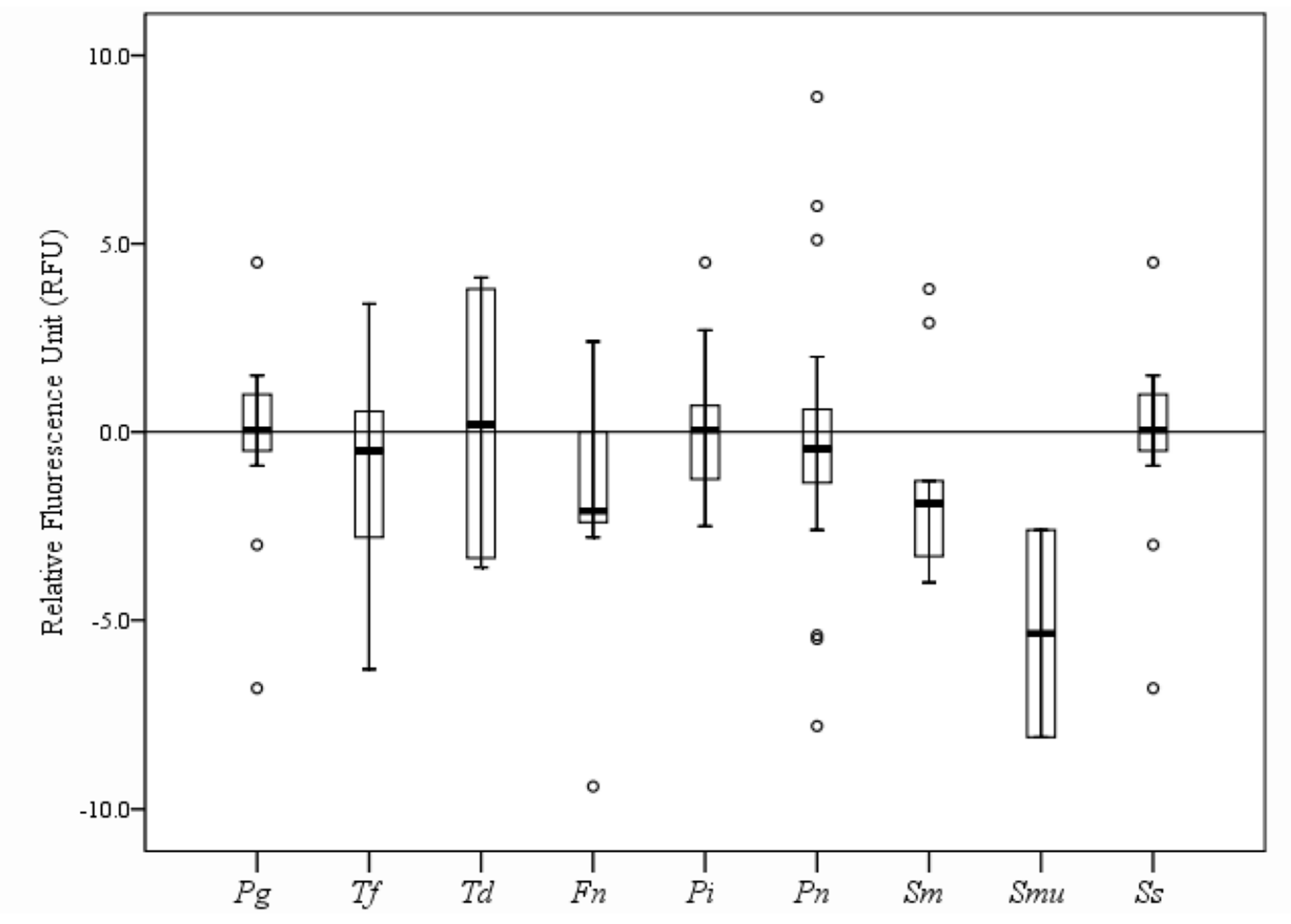
| Patient Number | Relative Fluorescence Unit (RFU) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Pg (105) | Tf (105) | Td (104) | Fn (106) | Pi (106) | Pn (104) | Sm (106) | Smu (105) | Ss (105) | |
| Total | 1.5 (2.1) | 1.5 (1.8) | 0.7 (1.5) | 1.2 (1.7) | 1.1 (2.2) | 1.1 (1.2) | 2.5 (2.8) | 1.2 (1.5) | 0.5 (1.9) |
| p-value * | 0.001 | 0.002 | 0.068 | 0.000 | 0.018 | 0.001 | 0.000 | 0.008 | 0.180 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ku, J.-K.; Park, S.-Y.; Hwang, K.-G.; Yun, P.-Y. The Effect of Mouthrinse with 0.05% Dexamethasone Solution on the Oral Bacterial Community of Oral Lichen Planus Patients: Prospective Pilot Study. Appl. Sci. 2021, 11, 6286. https://doi.org/10.3390/app11146286
Ku J-K, Park S-Y, Hwang K-G, Yun P-Y. The Effect of Mouthrinse with 0.05% Dexamethasone Solution on the Oral Bacterial Community of Oral Lichen Planus Patients: Prospective Pilot Study. Applied Sciences. 2021; 11(14):6286. https://doi.org/10.3390/app11146286
Chicago/Turabian StyleKu, Jeong-Kui, Shin-Young Park, Kyung-Gyun Hwang, and Pil-Young Yun. 2021. "The Effect of Mouthrinse with 0.05% Dexamethasone Solution on the Oral Bacterial Community of Oral Lichen Planus Patients: Prospective Pilot Study" Applied Sciences 11, no. 14: 6286. https://doi.org/10.3390/app11146286
APA StyleKu, J.-K., Park, S.-Y., Hwang, K.-G., & Yun, P.-Y. (2021). The Effect of Mouthrinse with 0.05% Dexamethasone Solution on the Oral Bacterial Community of Oral Lichen Planus Patients: Prospective Pilot Study. Applied Sciences, 11(14), 6286. https://doi.org/10.3390/app11146286