Abstract
Suicide is a global public health problem. The goal of this study was to evaluate the psychometric properties of the measurement of suicide severity based on the Columbia suicide severity rating scale. We worked with a sample of 516 Argentinean adults, aged 18 to 75. The fit of a measurement model that differentiates between the various degrees of suicidal severity was verified. The specified model returns fit values above the suggested cut-off points, both for the occurrence and frequency indicators. The internal consistency indices from the composite reliability coefficient also show values above the cut-off points for both occurrence and frequency. Finally, evidence of construct validity was obtained from the relationship with external variables. The results are consistent with the theory, showing stronger effects of hopelessness on suicidal ideation compared to suicide attempts. Overall, evidence of construct validity for the measurement of suicidal severity is presented, a contribution that is essential in remedying the lack of studies on suicide in the region and promoting prevention strategies.
1. Introduction
Suicide constitutes a public health problem that has a significant economic, social, and psychological impact globally [1,2,3]. In 2019, more than 700,000 cases of death by suicide were recorded worldwide. However, it is important to highlight that 77% of these suicide cases have been recorded in low- and middle-income countries [4]. The latest epidemiological data on Argentina [5] indicate that in 2020, a total of 3171 deaths by suicide were recorded, which is equivalent to a rate of 7.6 per 100,000 population. Of the recorded causes of violent death, suicide ranks as the main cause (35%). Therefore, while the suicide rate has fallen 12.1% compared to 2019, it is important that this public health problem continues to be addressed. Looking beyond the cases of death by suicide, the world mental health report [6] estimates that there are 20 suicide attempts per every death globally. All this has led various world academic, governmental, and non-governmental bodies to continue their calls for measures to be taken to prevent suicide [4,7].
A prerequisite for the prevention and treatment of the problem of suicide is for these prevention and intervention actions to be based on reliable scientific evidence [8]. Unfortunately, the accuracy and reliability of suicide statistics remain an issue to be solved in numerous countries [9]. To improve the quality of data linked to suicide, it is essential and necessary to have measurements that allow for valid inferences to be drawn on suicidal thoughts and behaviours [10]. One of the instruments developed for the purpose of providing valid measurements of suicidal thoughts and behaviour is the Columbia Suicide Severity Rating Scale (C-SSRS). The C-SSRS was designed to (i) offer definitions of suicidal ideation and behaviour, non-suicidal self-injurious behaviour, and corresponding assessments; (ii) quantify the full spectrum of suicidal ideation and suicidal behaviour and measure their severity over set periods; and (iii) distinguish between suicidal behaviour and non-suicidal self-injurious behaviour. These criteria are deemed indispensable in gauging the utility of suicide rating scales [11]. This study will address the construct validity of suicide severity measurement based on the application of the self-report version of the C-SSRS [12].
Globally, to date, we have identified few prior studies that have applied the self-report version of the C-SSRS [13,14,15,16], and only one prior study that has obtained evidence of construct validity based on the application of this type of version [12]. In their study, Viguera et al. [12] present evidence of validity in the use of cut-off points to establish the presence of suicide risk based on suicidal ideation and behaviour indicators. In comparison with the use of item 9 of the Patient Health Questionnaire-9, the C-SSRS showed greater sensitivity and specificity. In Argentina, although there is a specific prior example concerning the application and assessment of the psychometric properties that arise from applying the C-SSRS [17], some significant limitations are identified that merit a complementary study in this area. Firstly, it should be mentioned that the report is not clear regarding the format of the C-SSRS that has been applied. It is important to clarify at this point that different formats of application of the C-SSRS have been proposed, such as self-report versions, semi-structured interviews, or computerised versions (the different formats of the C-SSRS can be viewed at: https://cssrs.columbia.edu/, accessed on 15 September 2022). Judging by the contents of this study, it is likely that the Spanish version has been used, which is in the format of a semi-structured interview [18]. The limitations of this earlier study include (a) the use of a convenience sampling method with university students and the use of a specific region in Argentina (i.e., Rosario); (b) the application of non-recommended methods for factor analysis from a latent variable approach, as is the case of principal component analysis when applying exploratory factor analysis; and (c) not considering estimation methods suitable for the dichotomous and polytomous nature of many of the answer options in this scale. On this last point, it should be noted that the scale assesses two distinct facets of suicide severity and uses a specific response format for each one (i.e., it assesses the occurrence of indicators based on dichotomous responses and assesses the frequency with which these indicators have presented using a 5-point Likert scale). This aspect of relevance has not been considered in the earlier study. In light of the above, this project aims to overcome these limitations by (1) using a sample of Argentinian men and women from regions of the country that are more heterogenous and (2) using factorial methods that are more suited to the aims of the analysis and the characteristics of the data (i.e., polychoric and tetrachoric correlation matrices and appropriate estimation methods, such as weighted least squares).
Thus, the main goal of this study is to assess the psychometric properties derived from the self-report version of the C-SSRS. Specifically, it seeks to assess construct validity by assessing internal structure, an aspect which, to date, has not been assessed in the prior literature reviewed. Additionally, evidence of validity will also be obtained based on the relationship with the measurement of hopelessness (i.e., an external source of construct validity). It is held that the results of this project will be relevant in expanding global evidence of the validity of suicide severity ratings derived from the self-report version of the C-SSRS. Therefore, we aim to contribute to the campaign to meet suicide detection, prevention, treatment, and monitoring goals, specifically in Argentina and countries in the region.
2. Materials and Methods
2.1. Participants and Sampling Procedure
A total of 516 subjects participated in the survey. They were selected using a non-probability open-mode online sample method [19]. This data collection method has proven to be equivalent to traditional forms of collection (i.e., face-to-face) [20], returning similar results in terms of means, internal consistency indexes, correlations, response rates, and level of conformity with the questionnaire. The sample for this observational, cross-sectional study was collected using an online survey format to gather information through the Google Forms platform and was delivered by Facebook. The data were collected in September and October of 2022.
Ages ranged from 18 to 75 (M = 34.87, SD = 11.92). Of the total sample, most identified as female (79.46%) (see Table 1). Table 2 shows participants’ academic education and Table 3 shows the distribution by participants’ employment status and income. The vast majority have primary (99.42%) and secondary (97.48%) education, and almost half report having completed tertiary or university studies (48.64%). Finally, the majority indicate that they are dependent employed (39.92%) or self-employed (26.94%), with the most frequent income being 80K pesos or less (36.39%).

Table 1.
Sociodemographic descriptors.
Table 2.
Academic education descriptors.
Table 3.
Employment status and income descriptors.
2.2. Data Collection Instruments
Columbia Suicide Severity Rating Scale (C-SSRS). The version applied herein is the format intended for the C-SSRS self-report screener [12,14], which employs the translation into Spanish by Al-Halabí et al. [18]. The instrument was developed with the aim of measuring two main dimensions according to the degree of suicidal severity: (a) suicidal ideation and (b) suicidal behaviour. The first dimension explores suicidal thoughts in a progressive manner (i.e., from lesser to greater severity) subdivided into passive suicidal ideation, with no specific plan or intent to act, and active suicidal ideation, with a plan and intent to act. The second dimension, suicidal behaviour, examines suicide attempts (i.e., action targeted at ending one’s life) and interrupted suicide attempts (i.e., action targeted at ending one’s life which is self-interrupted or interrupted by an external actor). Both dimensions probe both the occurrence (i.e., yes or no) and frequency (e.g., from less than once a week to many times per day) of the various suicide severity indicators. In total, the instrument comprised 14 items, 7 to measure occurrence and 7 to measure frequency. Whereas the occurrence indicators use a dichotomous response format, the frequency indicators use a format that has 5 response options (from 1: less than once a week to 5: many times per day) in addition to an open format allowing the respondent to freely indicate the frequency (the instrument is included in https://osf.io/7rscg/, accessed on 20 December 2022).
Beck Hopelessness Scale (BHS) [21]. The version validated in Argentina by Flores-Kanter et al. [22] was applied. The scale consists of 11 dichotomous response items (i.e., true, false), and is applied to assess negative expectations about the future. The evidence for Argentina suggests an essentially single-factor structure. In predictive terms, the factor score derived from this factor structure presents a high discrimination capacity between people with high and no suicidal ideation. This discrimination capacity is higher than that achieved using the total raw score [22].
2.3. Data Analysis Process
With regard to the data analysis procedure followed, the following methodological decisions were made:
- 1-
- Due to the variability in items 6 and 7 on frequency and so as to use consistent criteria for the response format, these indicators were respecified prior to subsequent analysis. The original response format for items 6 and 7 is open and does not provide categorised response options. In this case, the question refers to indicating the number of times the person has made suicide attempts. Since the originally reported frequencies ranged from 0 to 15, the recoding consisted of requesting that values greater than 5 be taken with the value 5, while the rest of the values remained with the original value. So here, respecification consisted of recoding the responses with the range of 0 to 5, as is the case with the rest of the questions on frequency.
- 2-
- Because the scale assesses two distinct facets of suicide severity and uses a specific response format for each one (i.e., it assesses the occurrence of indicators based on dichotomous responses and the frequency with which these indicators have presented using a 5-point Likert scale), we decided to carry out two separate factor analyses: a factor analysis for the occurrence indicators and a factor analysis for the frequency indicators.
- 3-
- Measurement models for three correlated factors were specified, which examine suicide severity in ascending order. This model is consistent with the aim of the C-SSRS where the intention is to distinguish the domains of suicidal ideation and suicidal behaviour based on their severity degree [11]. In this sense, the elaboration and objectives followed by the C-SSRS are contrary to the traditional view that considers suicidal ideation and suicidal behaviour a unidimensional construct. In line with previous applications of the C-SSRS [12], the specified measurement models defined the factors based on the degree of severity. Thus, the following factors were specified in the measurement models: (1) passive suicidal ideation (i.e., no intent to act); (2) active suicidal ideation (i.e., intent to act); and (3) suicide attempt. Although it would be possible to specify a two-factor measurement model, separating only between suicidal ideation and suicidal behaviour, the C-SSRS has been constructed for the purpose of gradually differentiating different levels of suicidal severity. In this sense, we consider that the fact of not differentiating within the dimension of suicidal ideation between passive and active suicidal ideation detracts from the discriminative capacity of the measurements in terms of being able to distinguish between less severe ideation (i.e., passive suicidal ideation) and more severe ideation (i.e., active suicidal ideation).
- 4-
- Regarding the structural model, the specified model considers the effect of the hopelessness factor on the suicide severity factors (i.e., passive suicidal ideation, active suicidal ideation, and suicide attempt). Here, we hypothesise that hopelessness will have a stronger relationship with suicidal ideation than suicide attempts. This hypothesis is based on the cognitive model of suicidal behaviour [22], where it is postulated that suicidal ideation is the strongest predictor of the suicidal act, whereas hopelessness is the strongest predictor of suicidal ideation.
In the data analysis, the data were specified entirely in the R Studio program [23]. The analysis consisted of applying structural equation modelling (SEM). This analysis set was applied so as to verify the fit of both measurement and structural models. In both cases, the WLSMV (weighted least squares with mean- and variance-adjusted standard errors) model was used, given that the indicators for the respective factors are categorical [24]. Model fit was assessed using comparative fit indexes (CFI), root mean square error of approximation (RMSEA), and standardised root mean square residual (SRMR). CFI values equal to or above 0.90 and 0.95 are deemed indicators of acceptable and optimum data fit, respectively, while RMSEA values below 0.8 and 0.5 indicate acceptable and optimum fit, respectively [25]. For SRMR, it is suggested that values below or equal to 0.8 are an indicator of acceptable fit [26]. The lavaan package was used for the above-mentioned purposes [27]. Finally, internal consistency was calculated according to the composite reliability index (also termed omega), using the measurement model estimated in SEM as direct input [28]. We used the semTools package here [29].
3. Results
3.1. Measurement Models: Source of Structural Evidence
The specified model returns fit values above the suggested cut-off points both for the occurrence indicators (χ2 = 17.14, df = 11, p = 0.10, CFI = 1.00, RMSEA = 0.03, SRMR = 0.05) and the frequency indicators (χ2 = 13.28, df = 11, p = 0.28, CFI = 1.00, RMSEA = 0.02, SRMR = 0.03).
The measurement models are laid out below with their respective standardised factor loadings (Figure 1 and Figure 2).
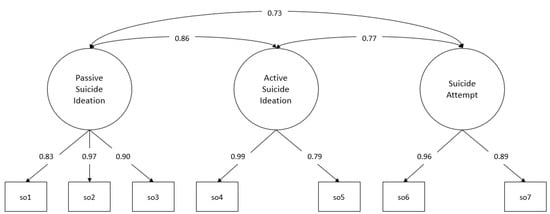
Figure 1.
Measurement model: occurrence. so1–so7: suicide severity indicators, items 1 to 7. Standardised factor loadings and interfactor correlations.
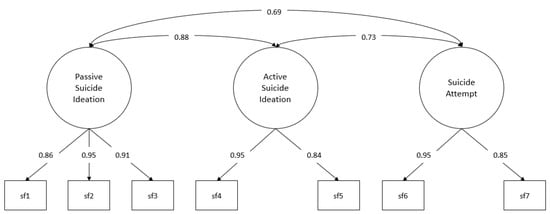
Figure 2.
Measurement model: frequency. sf1–sf7: suicide severity indicators, items 1 to 7. Standardised factor loadings and interfactor correlations.
For both occurrence and frequency, all the factor loadings obtained reach statistical significance (p < 0.001), with these loadings ranging from 0.83 to 0.99 for occurrence and 0.85 to 0.95 for frequency (the standard errors for the estimate in the occurrence measurement model are in the range between 0.056 and 0.096, while in the frequency measurement model, it is in the range between 0.033 and 0.083).
Lastly, we present evidence of internal consistency. To do so, composite reliability was considered. The results showed values above the suggested cut-off points both for occurrence (CR Passive Ideation = 0.80, CR Active Ideation = 0.78, CR Attempt = 0.76) and frequency (CR Passive Ideation = 0.87, CR Active Ideation = 0.79, CR Attempt = 0.78).
3.2. Structural Models: Source of External Evidence
The hopelessness rating was considered here and the structural model was assessed, in which the effect of hopelessness on the passive suicidal ideation, active suicidal ideation, and attempt factors are specified (Figure 3 and Figure 4).
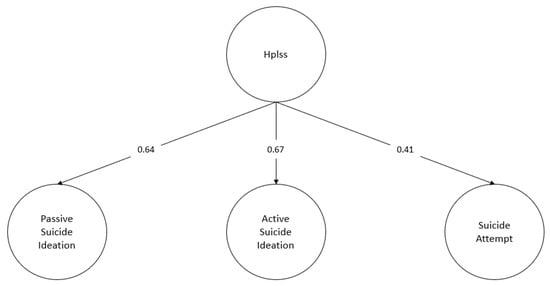
Figure 3.
Structural model: occurrence. Hplss: hopelessness. Standardised regression coefficients. For the sake of clarity, observable indicators for each latent factor considered in the model are omitted from the diagram. Likewise, the interfactor correlations between the suicide severity factors were omitted.
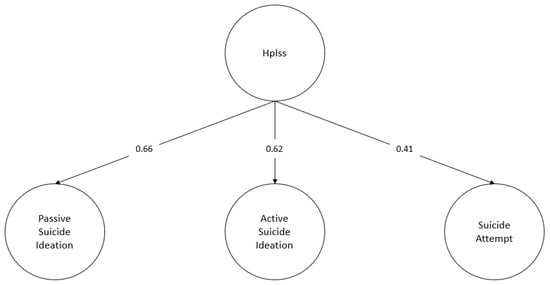
Figure 4.
Structural model: frequency. Hplss: hopelessness. Standardised regression coefficients. For the sake of clarity, observable indicators for each latent factor considered in the model are omitted from the diagram. Likewise, the interfactor correlations between the suicide severity factors were omitted.
Both specified structural models obtain fit indicators above the specified cut-off points for both occurrence (χ2 = 178.75, df = 129, p = 0.002, CFI = 0.99, RMSEA = 0.03, SRMR = 0.08) and frequency (χ2 = 180.73, df = 129, p = 0.002, CFI = 0.99, RMSEA = 0.03, SRMR = 0.07). Additionally, all standardised regression weights are statistically significant (p < 0.001). The regression coefficients obtained for the structural part of the model range from 0.41 to 0.67 for the occurrence case, and from 0.41 to 0.66 for the frequency case. Finally, a stronger effect of hopelessness on the dimensions of suicidal ideation compared to the dimension of suicide attempt is observed. The latter result is similar for both suicidal occurrence (β Passive Ideation = 0.64; β Active Ideation = 0.62; β Attempt = 0.41) and suicidal frequency (β Passive Ideation = 0.66; β Active Ideation = 0.62; β Attempt = 0.41).
4. Discussion
The main goal of this study was to assess the psychometric properties derived from the self-report version of the C-SSRS. To do so, construct validity was assessed based on (a) a source of structural evidence and (b) a source of external evidence.
With regard to the source of structural evidence, it was verified that the measurement model for three correlated factors, which examines suicide severity on a rising scale, presents an optimal fit according to the commonly adopted criteria in the international literature. This measurement model screens the following factors: (1) passive suicidal ideation (i.e., no intent to act); (2) active suicidal ideation (i.e., intent to act); and (3) suicide attempt. Moreover, the specified factors and their respective items show evidence of internal consistency, measured using composite reliability, which was also above the commonly accepted cut-off points. These results are consistent with the original aim of the C-SSRS, which was designed to offer multidimensional measurement covering related but differing constructs [11], in an effort to distinguish the domains of suicidal ideation and suicidal behaviour.
With regard to external evidence, the hopelessness scale showed a stronger effect with measurements of suicidal ideation than those of suicide attempts. These results are consistent with the theoretical cognitive models of suicide, which posit hopelessness as the determining factor in suicidal thoughts [2]. In this model, suicidal ideation is the strongest predictor of suicidal behaviour [30].
These data are relevant both globally and regionally. Global relevance is due to the fact that they provide evidence that, to date, we have been unable to find on structural evidence or measurement model fit based on C-SSRS measurements, as well as structural model fit, including external evidence with a hopelessness measurement. Regionally, they are relevant because while in Argentina instruments are used to measure suicidal ideation (i.e., Patient Health Questionnaire-9) and suicide risk (i.e., ISO-30), these scales have a series of limitations, which means that using them is not advisable. In the case of Patient Health Questionnaire-9, it has been demonstrated that using item 9 as an indicator generated much higher rates of false-positive findings than the self-report version of the C-SSRS [12]. The ISO-30 suicide orientation scale attempts to offer a measurement for suicide risk. However, there is no evidence supporting the use of a general measurement (i.e., total score) of risk by means of ISO-30, and the constructs that have been theoretically taken into consideration in the creation of this scale also do not offer clear or stable structural evidence, except in the case of the suicidal ideation factor [31]. Therefore, this study offers an alternative measurement for use in the region, especially in Argentina, to obtain accurate and reliable data on suicide, by examining suicide severity on a rising scale and including measurements of suicidal ideation and suicidal behaviour.
This study presents some limitations that must be addressed in future applications of the scale. We note that (a) the sample size did not allow for analysis of invariance in the measurement and structural models, covering important variables such as the region in the country, gender, and age; (b) a general set value was considered in this study assessing the occurrence and frequency of suicidal ideations and behaviours, but other possibilities, such as the lifetime set value, were not included or compared; and (c) the stability of the measurement and structural models was not assessed in separate samples or over time. Finally, we would like to add a comment on the response format used by the C-SSRS. The C-SSRS asks about two aspects, the occurrence and frequency of indicators of suicidal severity. However, one of the reviewers has pertinently pointed out that the occurrence responses can easily be derived from the frequency of the responses; therefore, the number of questions in the C-SSRS could be reduced by half (i.e., by eliminating the questions referring to occurrence). Related to this last point, the reviewer also rightly noted that the results derived from the structural equation models are very similar for the occurrence and frequency indicators, which makes the added value of considering both indicators debatable. The latter can also be taken as evidence in favour of reducing the number of questions in the C-SSRS by considering only the frequency indicators. Of course, in the latter case, it would be relevant to incorporate a response option referring to “Never happened to me”. So as to continue securing evidence of construct validity for the measurements derived from the self-report version of the C-SSRS applied herein, it is important that future research pays attention to these limitations and be able to provide data on the matter.
5. Conclusions
This study provides evidence of construct validity for measurements taken using a self-report version of the C-SSRS. This proves relevant as the version used herein meets the criteria given by Roaten et al. [14] to inform the selection of suicide severity and risk scales (1) measurement validity/reliability, (2) brevity of application, (3) open access or availability in the public domain, and (4) administration with minimal training. Thus, C-SSRS, supported with timely clinical assessment, in conjunction with other measurement methods [10] (e.g., smartphone apps, wearable technology), may be a useful and efficient method of screening for suicide severity and suicide risk [14]. We hope that this report constitutes a key step in promoting more accurate and reliable data in the Central and South America region.
Author Contributions
Conceptualization, P.E.F.-K., C.A. and J.M.A.; methodology, P.E.F.-K. and J.M.A.; formal analysis, P.E.F.-K. and J.M.A.; investigation, P.E.F.-K. and C.A.; writing—original draft preparation, P.E.F.-K., C.A. and J.M.A.; writing—review and editing, P.E.F.-K., C.A. and J.M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (or Ethics Committee) of Centro de Bioética from Universidad Católica de Córdoba, Argentina.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting the reported results can be downloaded at https://osf.io/7rscg/ (accessed on 20 December 2022). The files are hosted in an Open Science Framework (OSF) repository and can be accessed at any time.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Flores Kanter, P.E. El Lugar de La Psicología En Las Investigaciones Empíricas Del Suicidio En Argentina: Un Estudio Bibliométrico. Interdiscip. Rev. Psicol. Cienc. Afines 2017, 34, 25–37. [Google Scholar] [CrossRef]
- Flores-Kanter, P.E.; García-Batista, Z.E.; Moretti, L.S.; Medrano, L.A. Towards an Explanatory Model of Suicidal Ideation: The Effects of Cognitive Emotional Regulation Strategies, Affectivity and Hopelessness. Span. J. Psychol. 2019, 22, E43. [Google Scholar] [CrossRef] [PubMed]
- Naghavi, M. Global, Regional, and National Burden of Suicide Mortality 1990 to 2016: Systematic Analysis for the Global Burden of Disease Study. BMJ 2019, 364, l94. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Suicide Worldwide in 2019: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2021; ISBN 978-92-4-002664-3.
- Ministerio de Seguridad Argentina Suicidios (Sistema de Alerta Temprana—Suicidios). 2022. Available online: https://estadisticascriminales.minseg.gob.ar/reports/Informe_Suicidios.pdf (accessed on 15 September 2022).
- World Health Organization. World Mental Health Report: Transforming Mental Health for All; World Health Organization: Geneva, Switzerland, 2022; ISBN 978-92-4-004933-8.
- Reifels, L.; Krishnamoorthy, S.; Kõlves, K.; Francis, J. Implementation Science in Suicide Prevention. Crisis 2022, 43, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kirtley, O.J.; Janssens, J.J.; Kaurin, A. Open Science in Suicide Research Is Open for Business. Crisis 2022, 43, 355–360. [Google Scholar] [CrossRef]
- Arensman, E.; Scott, V.; De Leo, D.; Pirkis, J. Suicide and Suicide Prevention from a Global Perspective. Crisis 2020, 41, S3–S7. [Google Scholar] [CrossRef]
- Millner, A.J.; Robinaugh, D.J.; Nock, M.K. Advancing the Understanding of Suicide: The Need for Formal Theory and Rigorous Descriptive Research. Trends Cogn. Sci. 2020, 24, 704–716. [Google Scholar] [CrossRef] [PubMed]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; et al. The Columbia–Suicide Severity Rating Scale: Initial Validity and Internal Consistency Findings from Three Multisite Studies with Adolescents and Adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef] [PubMed]
- Viguera, A.C.; Milano, N.; Laurel, R.; Thompson, N.R.; Griffith, S.D.; Baldessarini, R.J.; Katzan, I.L. Comparison of Electronic Screening for Suicidal Risk with the Patient Health Questionnaire Item 9 and the Columbia Suicide Severity Rating Scale in an Outpatient Psychiatric Clinic. Psychosomatics 2015, 56, 460–469. [Google Scholar] [CrossRef]
- Chang, B.P.; Tan, T.M. Suicide Screening Tools and Their Association with Near-Term Adverse Events in the ED. Am. J. Emerg. Med. 2015, 33, 1680–1683. [Google Scholar] [CrossRef]
- Roaten, K.; Johnson, C.; Genzel, R.; Khan, F.; North, C.S. Development and Implementation of a Universal Suicide Risk Screening Program in a Safety-Net Hospital System. Jt. Comm. J. Qual. Patient Saf. 2018, 44, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.K.; Ursano, R.J.; Heeringa, S.G.; Stein, M.B.; Jain, S.; Raman, R.; Sun, X.; Chiu, W.T.; Colpe, L.J.; Fullerton, C.S.; et al. Mental Disorders, Comorbidity, and Pre-Enlistment Suicidal Behavior among New Soldiers in the U.S. Army: Results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). Suicide Life. Threat. Behav. 2015, 45, 588–599. [Google Scholar] [CrossRef] [PubMed]
- DeVylder, J.E.; Jahn, D.R.; Doherty, T.; Wilson, C.S.; Wilcox, H.C.; Schiffman, J.; Hilimire, M.R. Social and Psychological Contributions to the Co-Occurrence of Sub-Threshold Psychotic Experiences and Suicidal Behavior. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1819–1830. [Google Scholar] [CrossRef]
- Universidad Nacional de Rosario. Rosario, Argentina., Universidad Nacional de Rosario.; Serrani Azcurra, D. Psychometric Validation of the Columbia-Suicide Severity Rating Scale in Spanish-Speaking Adolescents. Colomb. Médica 2017, 48, 174–182. [Google Scholar] [CrossRef]
- Al-Halabí, S.; Sáiz, P.A.; Burón, P.; Garrido, M.; Benabarre, A.; Jiménez, E.; Cervilla, J.; Navarrete, M.I.; Díaz-Mesa, E.M.; García-Álvarez, L.; et al. Validación de la versión en español de la Columbia-Suicide Severity Rating Scale (Escala Columbia para Evaluar el Riesgo de Suicidio). Rev. Psiquiatr. Salud Ment. 2016, 9, 134–142. [Google Scholar] [CrossRef]
- The International Test Commission. International Guidelines on Computer-Based and Internet-Delivered Testing. Int. J. Test. 2006, 6, 143–171. [Google Scholar] [CrossRef]
- Weigold, A.; Weigold, I.K.; Russell, E.J. Examination of the Equivalence of Self-Report Survey-Based Paper-and-Pencil and Internet Data Collection Methods. Psychol. Methods 2013, 18, 53–70. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The Measurement of Pessimism: The Hopelessness Scale. J. Consult. Clin. Psychol. 1974, 42, 861–865. [Google Scholar] [CrossRef]
- Flores-Kanter, P.E.; Toro, R.; Alvarado, J.M. Internal Structure of Beck Hopelessness Scale: An Analysis of Method Effects Using the CT-C(M–1) Model. J. Pers. Assess. 2021, 1–9. [Google Scholar] [CrossRef]
- RStudio Team. RStudio: Integrated Development for R, RStudio, Inc.: Boston, MA, USA, 2020.
- Rhemtulla, M.; Brosseau-Liard, P.É.; Savalei, V. When Can Categorical Variables Be Treated as Continuous? A Comparison of Robust Continuous and Categorical SEM Estimation Methods under Suboptimal Conditions. Psychol. Methods 2012, 17, 354–373. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Schreiber, J.B. Update to Core Reporting Practices in Structural Equation Modeling. Res. Soc. Adm. Pharm. 2017, 13, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48. [Google Scholar] [CrossRef]
- Cho, E. Neither Cronbach’s Alpha nor McDonald’s Omega: A Commentary on Sijtsma and Pfadt. Psychometrika 2021, 86, 877–886. [Google Scholar] [CrossRef]
- Rosseel, T.D.; Pornprasertmanit, S.; Schoemann, A.M.; Rosseel, Y. SemTools: Useful Tools for Structural Equation Modeling. R Package Version 0.5-6. Available online: https://cran.r-project.org/package=semTools (accessed on 15 October 2022)2022.
- Beck, A.T.; Rush, A.J. (Eds.) Cognitive Therapy of Depression; The Guilford Clinical Psychology and Psychotherapy Series; Guilford Press: New York, NY, USA, 1979; ISBN 978-0-89862-919-4. [Google Scholar]
- Vecco, G.A.; Flores-Kanter, P.E.; Luque, L.E. Análisis Psicométrico Del Inventario de Orientación Suicida ISO-19, En Adolescentes Cordobeses Escolarizados. Rev. Evaluar 2021, 21, 39–52. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).