Effect of a Standardized Four-Week Desensitization and Counter-Conditioning Training Program on Pre-Existing Veterinary Fear in Companion Dogs


Simple Summary
Abstract
1. Introduction
2. Materials and Methods
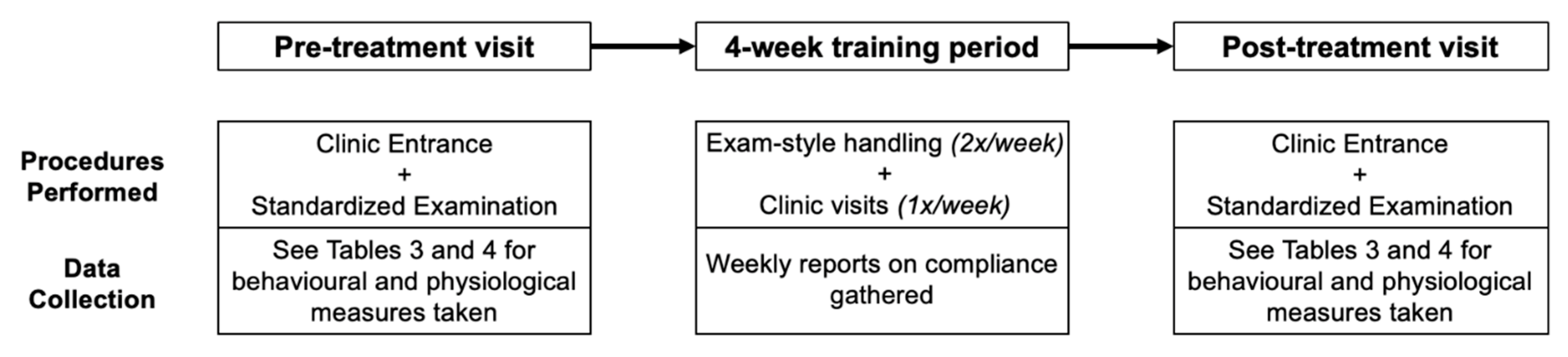
2.1. Stages of Testing
2.2. Desensitization and Counter-Conditioning Training
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Clinic Entrance
3.1.1. The First Visit
3.1.2. Efficacy of Training during the Second Visit
3.1.3. Subjective Fear Scores
3.2. Examination
3.2.1. The First Visit
3.2.2. Efficacy of Training during Second Visit
3.2.3. Phase of Exam
3.2.4. Subjective Fear Scores
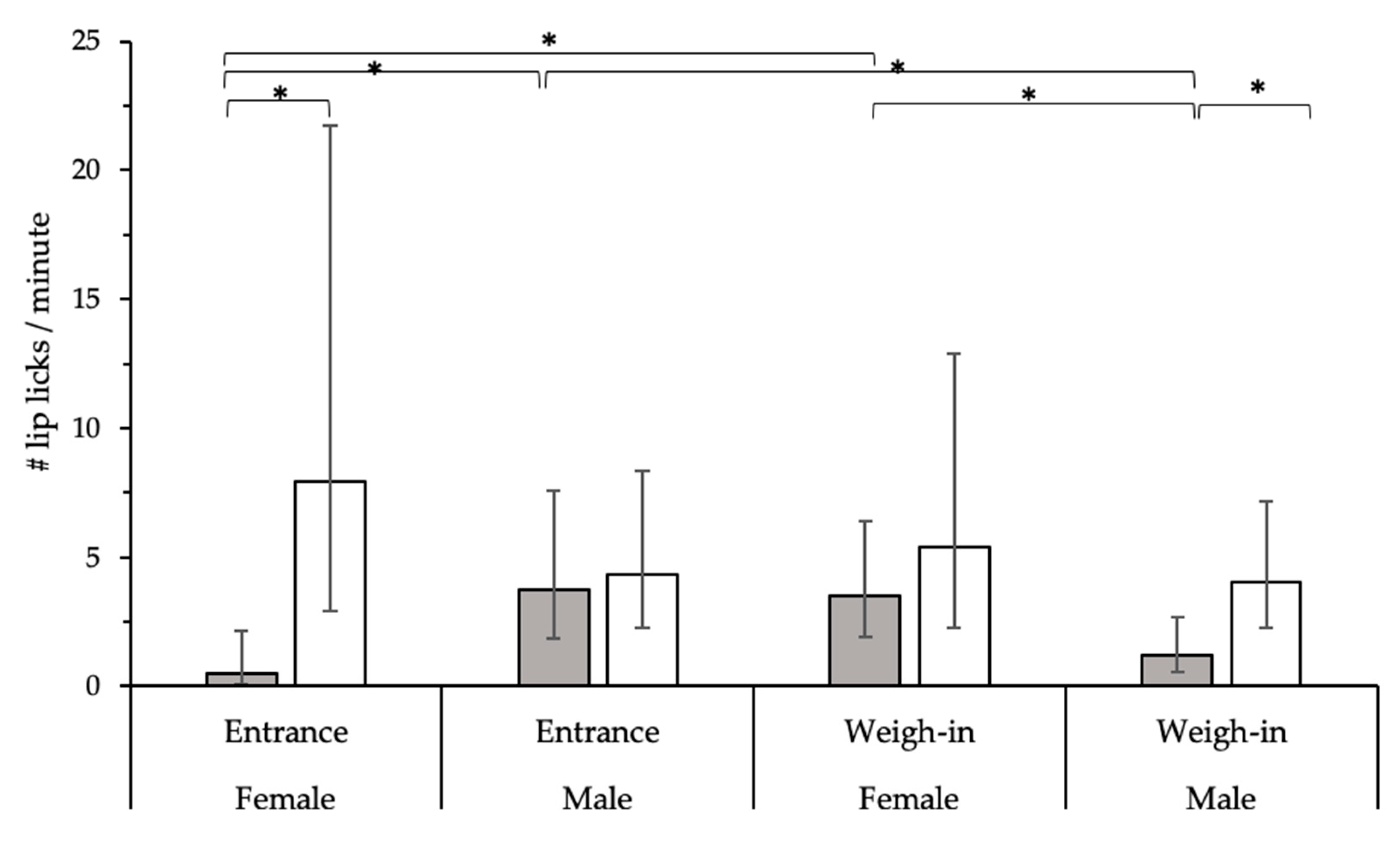
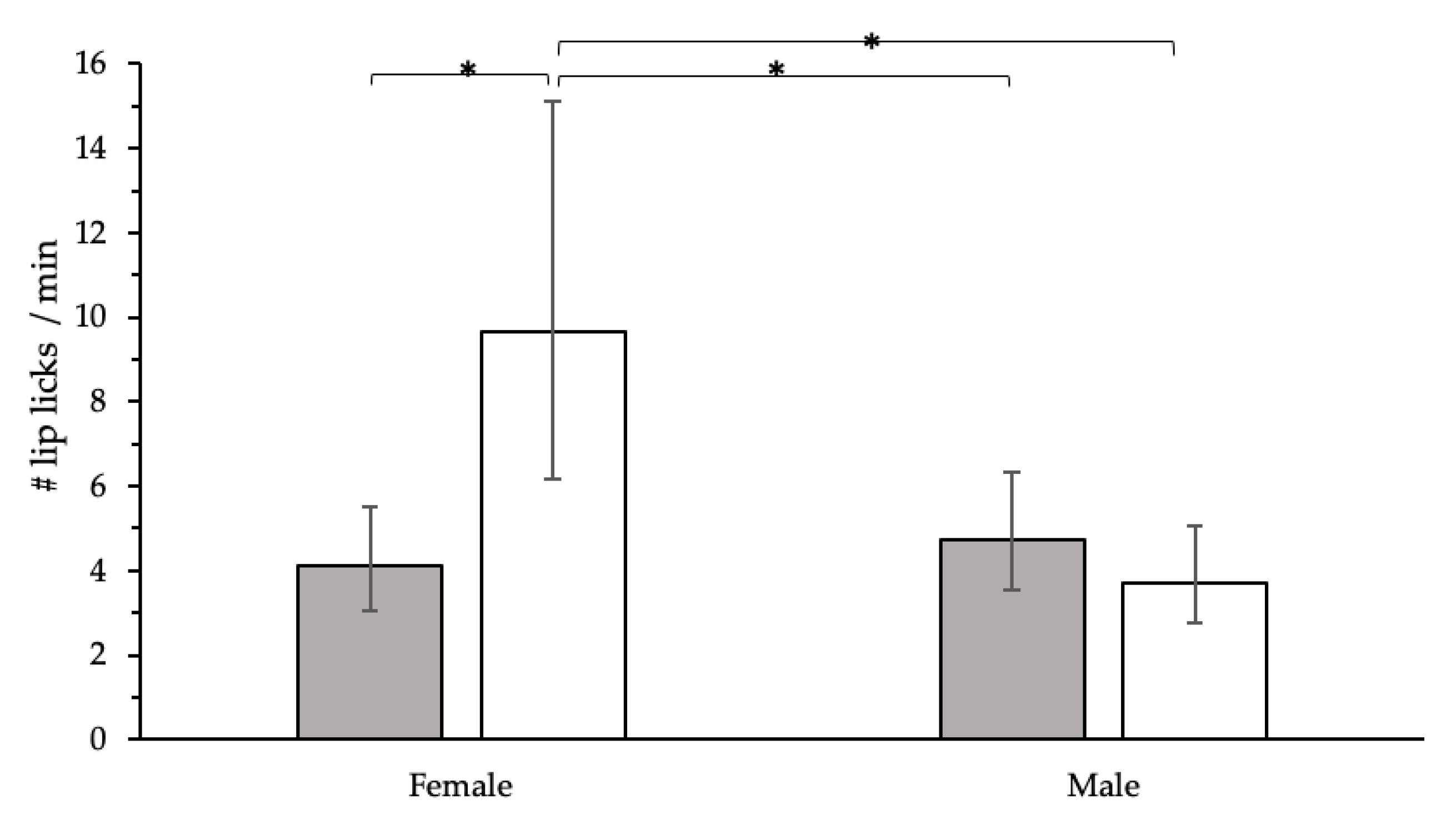
3.3. Age and Sex Effects
4. Discussion
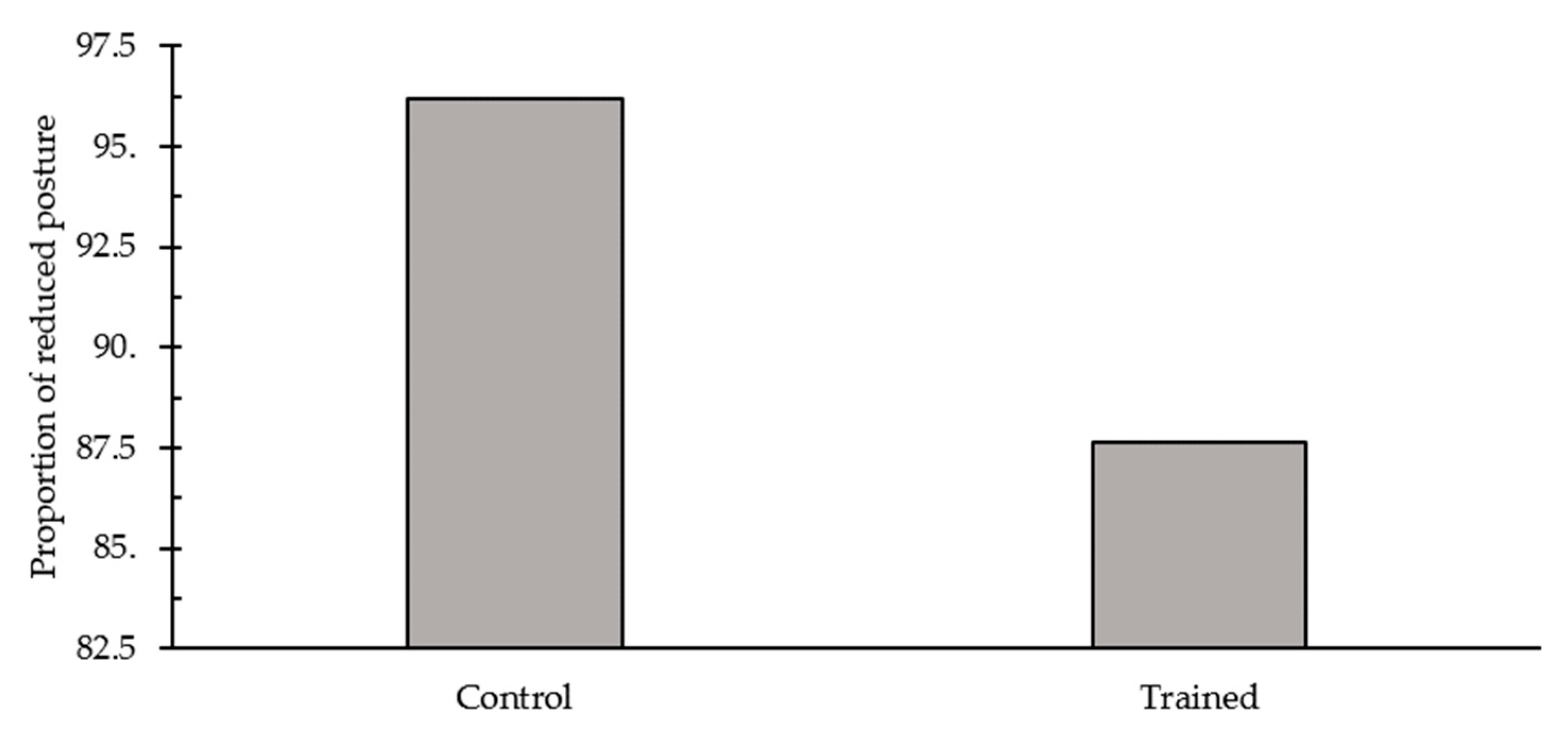
4.1. Effect of Desensitization and Counter-Conditioning Training
4.2. Age and Sex Effects
4.3. Phase Effects
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mariti, C.; Raspanti, E.; Zilocchi, M.; Carlone, B.; Gazzano, A. The assessment of dog welfare in the waiting room of a veterinary clinic. Anim. Welf. 2015, 24, 299–305. [Google Scholar] [CrossRef]
- Döring, D.; Roscher, A.; Scheipl, F.; Küchenhoff, H.; Erhard, M.H. Fear-related behaviour of dogs in veterinary practice. Vet. J. 2009, 182, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Volk, J.O.; Felsted, K.E.; Thomas, J.G.; Siren, C.W. Executive summary of the Bayer veterinary care usage study. J. Am. Vet. Med. Assoc. 2011, 238, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Glardon, O.J.; Hartnack, S.; Horisberger, L. Analysis of dogs and cats behaviour during the physical examination in veterinary practice. Schweiz Arch. Tierheilk 2010, 152, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Bragg, R.F.; Bennett, J.S.; Cummings, A.; Quimby, J.M. Evaluation of the effects of hospital visit stress on physiological variables in dogs. J. Am. Vet. Med. Assoc. 2015, 246, 212–215. [Google Scholar] [CrossRef]
- van Vonderen, I.K.; Kooistra, H.S.; Rijnberk, A. Influence of veterinary care on the urinary corticoid: Creatinine ratio in dogs. J. Vet. Intern. Med. 1998, 12, 431–435. [Google Scholar] [CrossRef] [PubMed]
- August, J.R. Dog and cat bites. J. Am. Vet. Med. Assoc. 1988, 193, 1394–1398. [Google Scholar] [PubMed]
- Stellato, A.; Hoffman, H.; Gowland, S.; Dewey, C.; Widowski, T.; Niel, L. Effect of background noise on dog responses to a routine physical examination in a veterinary setting. Appl. Anim. Behav. Sci. 2019, 214, 64–71. [Google Scholar] [CrossRef]
- Csoltova, E.; Martineau, M.; Boissy, A.; Gilbert, C. Behavioral and physiological reactions in dogs to a veterinary examination: Owner-dog interactions improve canine well-being. Physiol. Behav. 2017, 177, 270–281. [Google Scholar] [CrossRef]
- Lind, A.; Hydbring-Sandberg, E.; Forkman, B.; Keeling, L.J. Assessing stress in dogs during a visit to the veterinary clinic: Correlations between dog behavior in standardized tests and assessments by veterinary staff and owners. J. Vet. Behav. 2017, 17, 24–31. [Google Scholar] [CrossRef]
- Stellato, A.; Dewey, C.; Widowski, T.; Niel, L. Effect of owner presence on dog responses to a routine physical exam in a veterinary setting. J. Am. Vet. Med. Assoc. In Press.
- Herron, M.E.; Shreyer, T. The pet-friendly veterinary practice: A guide for practitioners. Vet. Clin. Small Anim. 2014, 44, 451–481. [Google Scholar] [CrossRef] [PubMed]
- Martin, K.M.; Martin, D.; Shaw, J.K. Small animal behavioral triage: A guide for practitioners. Vet. Clin. Small Anim. Pract. 2014, 44, 379–399. [Google Scholar] [CrossRef] [PubMed]
- Moffat, K. Addressing canine and feline aggression in the veterinary clinic. Vet. Clin. Small Anim. Pract. 2008, 38, 983–1003. [Google Scholar] [CrossRef] [PubMed]
- Yin, S. Low Stress Handling, Restraint and Behavior Modification of Dogs and Cats: Techniques for Developing Patients Who Love Their Visits; Cattle Dog Publishing: Davis, CA, USA, 2009. [Google Scholar]
- Gilbert-Gregory, S.E.; Stull, J.W.; Rico, M.R.; Herron, M.E. Effects of trazodone on behavioral signs of stress in hospitalized dogs. J. Am. Vet. Med. Assoc. 2016, 249, 1281–1291. [Google Scholar] [CrossRef]
- Westlund, K. To feed or not to feed: Counterconditioning in the veterinary clinic. J. Vet. Behav. 2015, 10, 433–437. [Google Scholar] [CrossRef]
- de Jong, P.J.; Vorage, I.; van den Hout, M.A. Counterconditioning in the treatment of spider phobia: Effects on disgust, fear and valence. Behav. Res. Ther. 2000, 28, 1055–1069. [Google Scholar] [CrossRef]
- Thomas, B.L.; Cutler, M.; Cherly, N. A modified counterconditioning procedure prevents the renewal of conditioned fear in rats. Learn Motiv. 2012, 23, 24–34. [Google Scholar] [CrossRef]
- Christensen, J.W.; Rundgren, M.; Olsson, K. Training methods for horses: Habituation to a frightening stimulus. Equine Vet. J. 2006, 38, 429–443. [Google Scholar] [CrossRef]
- Kakuma, Y.; Kinoshita, N. An experimental case study of two aggressive dogs: The effectiveness of a behavioural modification program using systematic desensitization and counter-conditioning. J. Vet. Behav. Clin. Appl. Res. 2010, 5, 29. [Google Scholar] [CrossRef]
- Savage, K.E. A Comparison of Classical Counterconditioning and Differential Reinforcement of Alternative Behaviour on Aggressive Behaviour in Dogs. Master’s Thesis, University of Kansas, Lawrence, KS, USA, 2010. [Google Scholar]
- Crowell-Davis, S.; Sibert, L.M.; Sung, W.; Parthasarathy, V.; Curtis, T.M. Use of clomipramine, alprazolam, and behaviour modification for treatment of storm phobia in dogs. J. Am. Vet. Med. Assoc. 2003, 222, 744–748. [Google Scholar] [CrossRef] [PubMed]
- Levine, E.D.; Ramos, D.; Mills, D.S. A prospective study of two self-help CD based desensitization and counter-conditioning programmes with the use of Dog Appeasing Pheromone for the treatment of firework fears in dogs (Canis familiaris). Appl. Anim. Behav. Sci. 2007, 105, 311–329. [Google Scholar] [CrossRef]
- Garnier, F.; Benoit, E.; Virta, M.; Ochoa, R.; Delatour, P. Adrenal cortisol response in clinically normal dogs before and after adaption to a housing environment. Lab. Anim. 1990, 24, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Vas, J.; Topál, J.; Gácsi, M.; Miklósi, Á.; Csányi, V. A friend or an enemy? Dogs’ reaction to an unfamiliar person showing behavioural cues of threat and friendliness at different times. Appl. Anim. Behav. Sci. 2005, 94, 99–115. [Google Scholar] [CrossRef]
- Kuhne, F.; Hößler, J.; Struwe, R. Affective behavioral responses by dogs to tactile human-dog interactions. Berl. Münch Tierärztl 2012, 125, 371–378. [Google Scholar]
- Kuhne, F.; Hößler, J.; Struwe, R. Effects of human-dog familiarity on dogs’ behavioral responses to petting. Appl. Anim. Behav. Sci. 2012, 142, 176–181. [Google Scholar] [CrossRef]
- Blackwell, E.J.; Bradshaw, J.W.; Case, R.A. Fear responses to noises in domestic dogs: Prevalence, rick factors and co-occurrence with other fear related behaviour. Appl. Anim. Behav. Sci. 2013, 145, 15–25. [Google Scholar] [CrossRef]
- Mazur, J.E. Basic principle of classical conditioning. In Learning and Behavior, 6th ed.; Pearson Education: Upper Saddle River, NJ, USA, 2006; pp. 76–81. [Google Scholar]
- Demant, H.; Ladewig, J.; Balsby, T.J.S.; Dabelsteen, T. The effect of frequency and duration of training sessions on acquisition and long-term memory in dogs. Appl. Anim. Behav. Sci. 2011, 133, 228–234. [Google Scholar] [CrossRef]
- Meyer, I.; Ladewig, J. The relationship between number of training sessions per week and learning dogs. Appl. Anim. Behav. Sci. 2008, 111, 311–320. [Google Scholar] [CrossRef]
- Beerda, B.; Schilder, M.B.H.; van Hooff, J.A.R.A.M.; de Vries, H.W.; Mol, J.A. Behavioural, saliva cortisol and heart rate responses to different types of stimuli in dogs. Appl. Anim. Behav. Sci. 1998, 58, 365–381. [Google Scholar] [CrossRef]
- Döring, D.; Haberland, B.A.; Ossig, A.; Küchenhoff, H.; Dobenecker, B.; Hack, R.; Schmidt, J.; Erhard, M.H. Behavior of laboratory beagles: Assessment in a standardized behavior test using novel stimuli and situations. J. Vet. Behav. 2016, 11, 18–25. [Google Scholar] [CrossRef]
- Beerda, B.; Schilder, M.B.H. Manifestations of chronic and acute stress in dogs. Appl. Anim. Behav. Sci. 1997, 52, 307–319. [Google Scholar] [CrossRef]
- Beerda, B.; Schilder, M.B.H.; Bernadina, W.; van Hooff, J.A.R.A.M.; de Vries, H.W.; Mol, J.A. Chronic stress in dogs subjected to social and spatial restriction. I. Behavioural responses. Physiol. Behav. 1999, 66, 233–242. [Google Scholar] [CrossRef]
- Bondariu, A. Indicators of stress and stress assessment in dogs. Lucari Stinifice Med. Vet. 2008, 41, 20–26. [Google Scholar]
- Cooper, J.J.; Cracknell, N.; Hardiman, J.; Wright, H.; Mills, D. The welfare consequences and efficacy of training pet dogs with remote electronic training collars in comparison to reward based training. PLoS ONE 2014, 9, e102722. [Google Scholar] [CrossRef] [PubMed]
- Firnkes, A.; Bartels, A.; Bidoli, E.; Erhard, M. Appeasement signals used by dogs during dog-human communication. J. Vet. Behav. 2017, 19, 35–44. [Google Scholar] [CrossRef]
- Döring, D.; Haberland, B.A.; Ossig, A.; Küchenhoff, H.; Dobenecker, B.; Hack, R.; Schmidt, J.; Erhard, M.H. Behavior of laboratory beagles towards humans: Assessment in an encounter test and a simulation of experimental situations. J. Vet. Behav. 2014, 9, 295–303. [Google Scholar] [CrossRef]
- Commins, S.; Cunningham, L.; Harvey, D.; Walsh, D. Massed but not spaced training impairs spatial memory. Behav. Brain Res. 2003, 139, 215–223. [Google Scholar] [CrossRef]
- Spreng, M.; Rossier, J.; Schenk, F. Spaced training facilitates long-term retention of place navigation in adult but not in adolescent rats. Behav. Brain Res. 2002, 128, 103–108. [Google Scholar] [CrossRef]
- Rubin, L.; Oppegard, C.; Hintz, H.F. The effect of varying the temporal distribution of conditioning trials on equine learning behavior. J. Anim. Sci. 1980, 50, 1184–1187. [Google Scholar] [CrossRef]
- Hall, L.E.; Robinson, S.; Buchanan-Smith, H.M. Refining dosing by oral gavage in the dog: A protocol to harmonise welfare. J. Pharmacol. Toxicol. Method 2015, 72, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Rohlf, V.I.; Benett, P.C.; Toukhsati, S.; Coleman, G. Why do even committed dog owners fail to comply with some responsible ownership practices? Anthrozoos 2010, 23, 143–155. [Google Scholar] [CrossRef]
- Huber, A.; Barber, A.L.A.; Faragó, T.; Müller, C.A.; Huber, L. Investigating emotional contagion in dogs (Canis familiaris) to emotional sounds of humans and conspecifics. Anim. Cogn. 2017, 20, 703–715. [Google Scholar] [CrossRef] [PubMed]
- Flint, H.E.; Coe, J.B.; Pearl, D.L.; Serpell, J.A.; Niel, L. Effect of training for dog fear identification on dog owner ratings of fear in familiar and unfamiliar dogs. Appl. Anim. Behav. Sci. 2018, 208, 66–74. [Google Scholar] [CrossRef]
- Soszyński, D.; Fizjologii, Z.; Medycznej im, A.; w Bydgoszczy, L.R. Stressful increase in body temperature-hyperthermia or fever. Postepy Hig. Med. Dosw. 1999, 53, 855–870. [Google Scholar] [PubMed]
- Petherick, J.C.; Doogan, V.J.; Venus, B.K.; Holroyd, R.G.; Olsson, P. Quality of handling and holding yard environment and beef cattle temperament, consequences for stress and productivity. Aust. J. Exper. Agric. 2009, 42, 389–398. [Google Scholar] [CrossRef]
- Humphreys, A.P.; Einon, D.F. Play as a reinforcer for maze-learning in juvenile rats. Anim. Behav. 1981, 29, 259–270. [Google Scholar] [CrossRef]
- Affenzeller, N.; Palme, R.; Zulch, H. Playful activity post-learning improves training performance in Labrador Retriever dogs (Canis lupus familiaris). Physiol. Behav. 2017, 168, 62–73. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dog | Breed | Age (Years) | Sex | Training/Control |
|---|---|---|---|---|
| Avery | Yorkshire Terrier | 3 | F | Training |
| Bear | Mixed Breed | 3 | M | Training |
| Bugsly | Mixed Breed | 9 | M | Training |
| Dobby | Mixed Breed | 3 | M | Training |
| Finn | Mixed Breed | 2 | M | Training |
| Ivy | Mixed Breed | 2 | F | Training |
| Midori | Mixed Breed | 5 | F | Training |
| Monty | Greyhound | 7 | M | Training |
| Prince | Mixed Breed | 9 | M | Training |
| Rose | Mixed Breed | 3 | F | Training |
| Solo | Mixed Breed | 1 | M | Training |
| Tanner | Retriever (Golden) | 3 | M | Training |
| Tucker | Other | 6 | M | Training |
| Waldo | Mixed Breed | 7 | M | Training |
| Zappa | Miniature Pinscher | 11 | M | Training |
| Addison | Collie (Rough) | 7 | F | Control |
| Basil | Beagle | 2 | M | Control |
| Calista | Mixed Breed | 2 | F | Control |
| Carter | Mixed Breed | 3 | M | Control |
| Daisy | Mixed Breed | 4 | F | Control |
| Duncan | Mixed Breed | 7 | M | Control |
| Dusty | Mixed Breed | 8 | M | Control |
| Essie | Mixed Breed | 1 | F | Control |
| Freya | Bulldog | 1 | F | Control |
| Hunter | Spaniel (English Springer) | 7 | M | Control |
| Kalaylee | Havanese | 3 | F | Control |
| Lucy | Mixed Breed | 2 | F | Control |
| Luis | Dachshund | 13.5 | M | Control |
| Maggie | Other | 3 | F | Control |
| Milo | Mixed Breed | 9 | M | Control |
| Oliver | Mixed Breed | 2 | M | Control |
| Penny | Labradoodle | 6 | F | Control |
| Pepper | Mixed Breed | 11 | F | Control |
| Reggie | Mixed Breed | 6 | M | Control |
| Roo | Mixed Breed | 3 | F | Control |
| Wrangler | German Shepherd Dog | 7 | M | Control |
| Zeus | Mixed Breed | 1 | M | Control |
| Body Part | Progressions |
|---|---|
| Paws |
|
| Mouth |
|
| Ears |
|
| Body |
|
| Testing Phase | Behaviours | Description |
|---|---|---|
| All phases | Head position | |
| i. Neutral | Head neutral or high | |
| ii. Reduced | Head low | |
| Tail position | ||
| i. Neutral | Tail high or breed specific position | |
| ii. Reduced | Tail lowered either still or wagging, or tucked between bent hind legs | |
| iii. Dog tail out of view | Cannot determine tail position | |
| Ear position | ||
| i. Neutral | Ears forward | |
| ii. Reduced | Ears sideways, down, or pinned back | |
| iii. Dog ears out of view | Cannot determine ear position | |
| Other behaviours | ||
| Body shaking | Lateral, side to side rotation of the body about the central axis, with shaking of the fur | |
| Lip/Snout licking | Portion of the tongue moves along the upper lip | |
| Yawning | Wide opening of mouth | |
| Vocalizing | Barking, growling, whining, yelping | |
| Clinic Entrance | Avoidance | Moving/manipulating body away, refusing to move forward, or successfully placing at least one paw off the scale |
| Encouragement to step on scale | Number of times the owner needed to encourage them onto the scale | |
| Willingness to step on scale | Forced on by pulling on leash, or physically moving them | |
| Examination | Trembling | Obvious shivering of the body |
| Avoidance | Moving/manipulating head or body away from the investigator or handling device | |
| Escape | All four paws off the mat | |
| Score | Behaviour Description | |
|---|---|---|
| 0 | Posture: Head normal or high, ears forward, tail high or breed specific position Avoidance: No escape attempts Subtle behaviours a: None |  |
| 1 | Posture: Head normal or high, ears forward or slightly back from neutral, tail body-height or slightly lowered Avoidance: No escape attempts Subtle behaviours a: 1-2 displayed |  |
| 2 | Posture: Head normal or low, ears sideways, tail lowered and either still or wagging Avoidance: Minor attempts to escape, retreat or hide; few steps made backwards/away Subtle behaviours a: Several behaviours displayed |  |
| 3 | Posture: Head somewhat low, ears down or slightly back, tail tucked between legs Avoidance: Moderate attempts to escape, retreat or hide; more than a few steps made backwards/away Subtle behaviours a: Several behaviours displayed |  |
| 4 | Posture: Head exaggeratedly low, ears down and pinned back, tail fully tucked between bent hind legs Avoidance: Vigorous/constant attempts to escape, retreat or hide Subtle behaviours a: Several behaviours displayed |  |
| Exam-Style Handling | Total | |||
|---|---|---|---|---|
| Yes | No | |||
| Clinic Visits | Yes | 15 | 0 | 15 |
| No | 4 | 8 | 12 | |
| Total | 19 | 8 | 27 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stellato, A.; Jajou, S.; Dewey, C.E.; Widowski, T.M.; Niel, L. Effect of a Standardized Four-Week Desensitization and Counter-Conditioning Training Program on Pre-Existing Veterinary Fear in Companion Dogs. Animals 2019, 9, 767. https://doi.org/10.3390/ani9100767
Stellato A, Jajou S, Dewey CE, Widowski TM, Niel L. Effect of a Standardized Four-Week Desensitization and Counter-Conditioning Training Program on Pre-Existing Veterinary Fear in Companion Dogs. Animals. 2019; 9(10):767. https://doi.org/10.3390/ani9100767
Chicago/Turabian StyleStellato, Anastasia, Sarah Jajou, Cate E. Dewey, Tina M. Widowski, and Lee Niel. 2019. "Effect of a Standardized Four-Week Desensitization and Counter-Conditioning Training Program on Pre-Existing Veterinary Fear in Companion Dogs" Animals 9, no. 10: 767. https://doi.org/10.3390/ani9100767
APA StyleStellato, A., Jajou, S., Dewey, C. E., Widowski, T. M., & Niel, L. (2019). Effect of a Standardized Four-Week Desensitization and Counter-Conditioning Training Program on Pre-Existing Veterinary Fear in Companion Dogs. Animals, 9(10), 767. https://doi.org/10.3390/ani9100767