
Impact of Psychopathology and Gut Microbiota on Disease Progression in Ulcerative Colitis: A Five-Year Follow-Up Study

 , , , , , ,
, , , , , ,  , ,
, ,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Procedures and Questionnaires
2.3. 16S rRNA-Targeted Metagenomics of Fecal Microbiota
2.4. Biocomputational and Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Demographical, Clinical, Psychometric, and Gut Microbiota Data at Baseline
3.2. Assessment of UC Adverse Outcomes
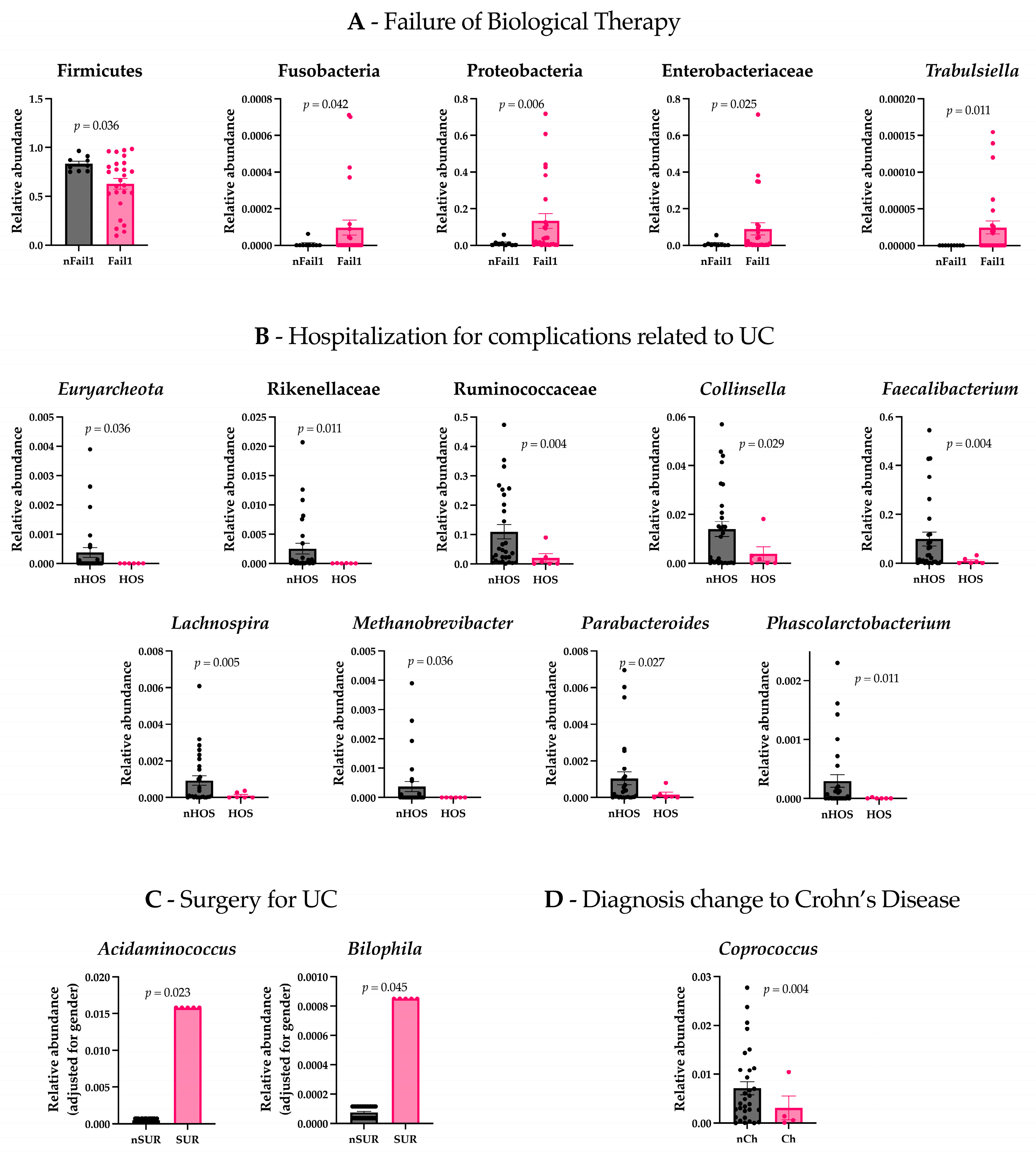
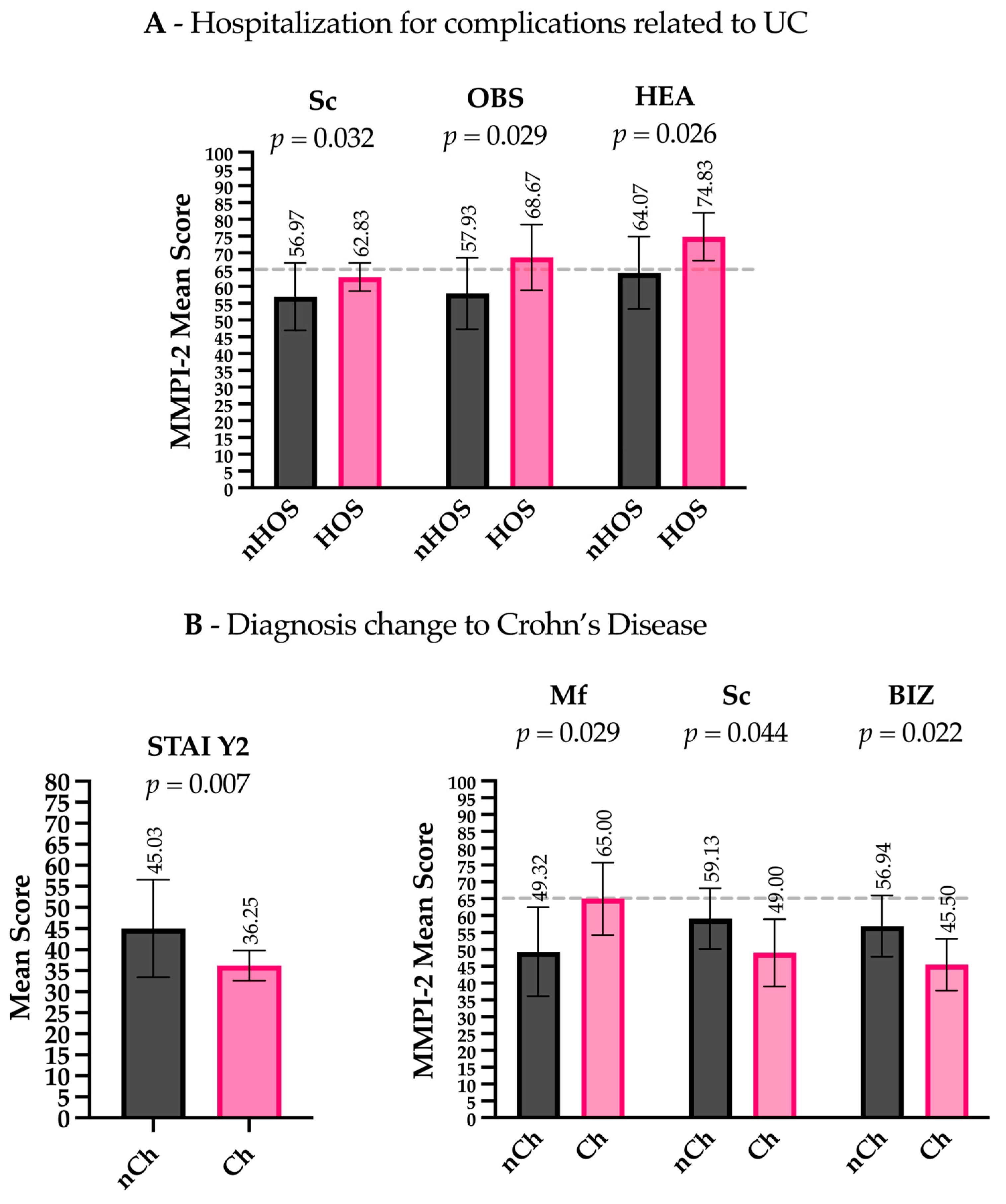
3.3. Psychopathological and Gut Microbiota Characteristics of Patients with UC Progression
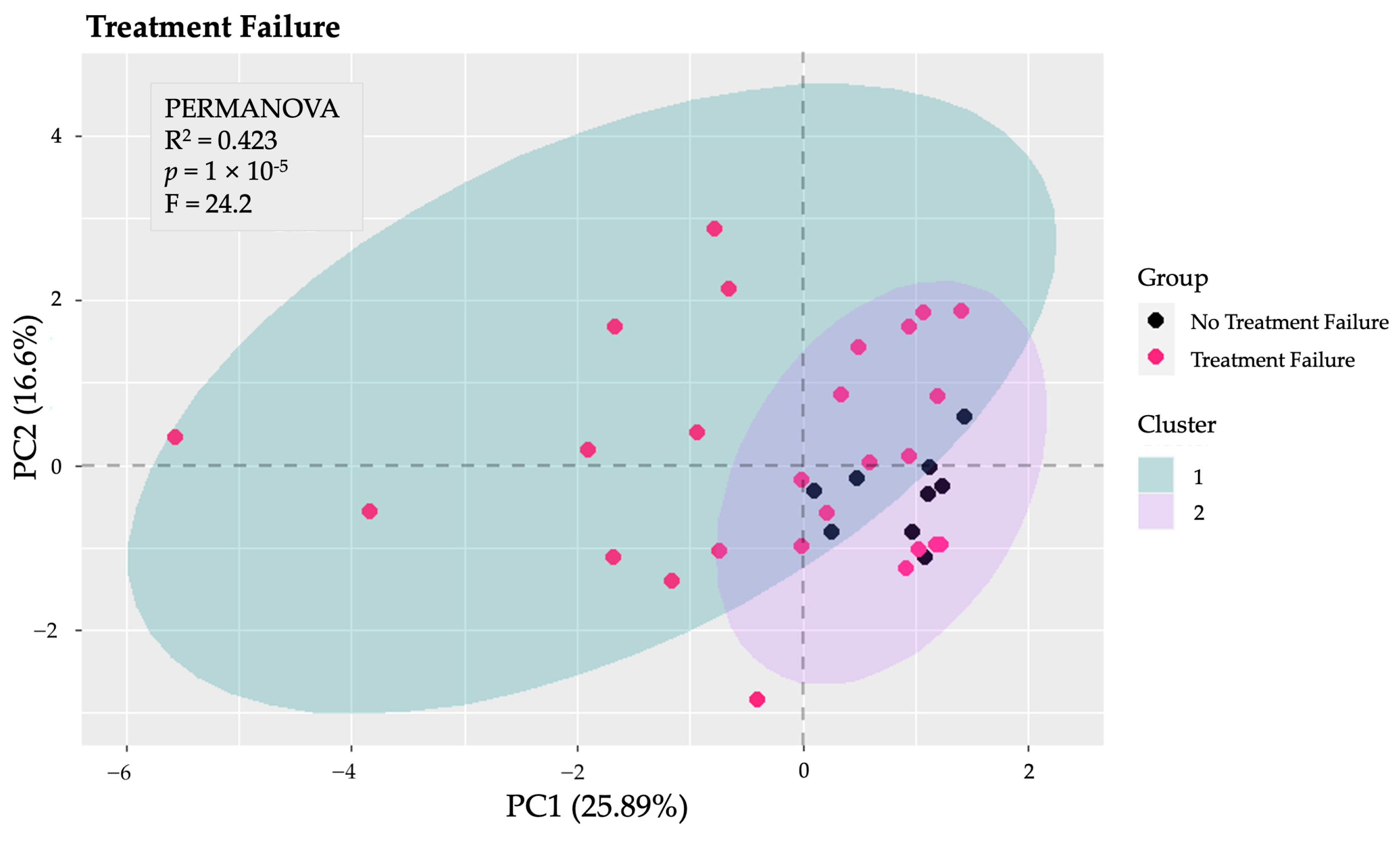
3.4. Psychopathological and Gut Microbiota Features as Predictive Factors
4. Discussion
5. Limitations
6. Conclusions and Future Perspectives
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 16S rRNA | 16S Ribosomal Ribonucleic Acid |
| AMPure XP | Agencourt AMPure XP Beads |
| ANCOVA | Analysis of Covariance |
| BIZ | Bizarre Mentation (MMPI-2 content scale) |
| CD | Crohn’s Disease |
| CD-RISC | Connor–Davidson Resilience Scale |
| CEMAD | Center for Digestive Disease |
| CO2 | Carbon Dioxide |
| DDS | Dextran Sulfate Sodium |
| DESeq2 | Differential Expression Analysis Using Shrinkage Estimation |
| DNA | Deoxyribonucleic Acid |
| FDR | False Discovery Rate |
| GSES | General Self-Efficacy Scale |
| H2 | Hydrogen Gas |
| H2S | Hydrogen Sulfide |
| HADS | Hospital Anxiety and Depression Scale |
| HEA | Health Concerns (MMPI-2 Content Scale) |
| Hy | Hysteria (MMPI-2 Clinical Scale) |
| IBD | Inflammatory Bowel Disease |
| IRCCS | Istituto di Ricovero e Cura a Carattere Scientifico (Scientific Institute for Research, Hospitalization, and Healthcare) |
| Mf | Masculinity–Femininity (MMPI-2 clinical scale) |
| MMPI-2 | Minnesota Multiphasic Personality Inventory, Second Edition |
| MAM | Microbial Anti-Inflammatory Molecule |
| OBS | Obsessivity (MMPI-2 content scale) |
| OTU | Operational Taxonomic Unit |
| Pa | Paranoia (MMPI-2 clinical scale) |
| PCA | Principal Component Analysis |
| Pd | Psychopathic Deviance (MMPI-2 clinical scale) |
| PERMANOVA | Permutational Multivariate Analysis of Variance |
| PSY-5 | Personality Psychopathology Five (subscale group in MMPI-2) |
| Pt | Psychasthenia (MMPI-2 clinical scale) |
| qPCR | Quantitative Polymerase Chain Reaction |
| R2 (Nagelkerke) | Nagelkerke’s R-Squared (Measure of Model Fit in Regression) |
| RNA | Ribonucleic Acid |
| SC | Schizophrenia (MMPI-2 clinical scale) |
| SCFA | Short-Chain Fatty Acid |
| STAI-Y1 | State-Trait Anxiety Inventory—Form Y1 (State Anxiety) |
| STAI-Y2 | State-Trait Anxiety Inventory—Form Y2 (Trait Anxiety) |
| TAS-20 | Toronto Alexithymia Scale—20 Items |
| UC | Ulcerative Colitis |
References
- Bonaz, B.; Sinniger, V.; Pellissier, S. Vagus Nerve Stimulation at the Interface of Brain–Gut Interactions. Cold Spring Harb. Perspect. Med. 2019, 9, a034199. [Google Scholar] [CrossRef] [PubMed]
- Sudo, N.; Chida, Y.; Aiba, Y.; Sonoda, J.; Oyama, N.; Yu, X.; Kubo, C.; Koga, Y. Postnatal microbial colonization programs the hypothalamic–pituitary–adrenal system for stress response in mice. J. Physiol. 2004, 558, 263–275. [Google Scholar] [CrossRef]
- Ahmed, H.; Leyrolle, Q.; Koistinen, V.; Kärkkäinen, O.; Layé, S.; Delzenne, N.; Hanhineva, K. Microbiota-derived metabolites as drivers of gut–brain communication. Gut Microbes 2022, 14, 2102878. [Google Scholar] [CrossRef]
- Gunawardene, A.R.; Corfe, B.M.; Staton, C.A. Classification and functions of enteroendocrine cells of the lower gastrointestinal tract: Classification and functions of colorectal enteroendocrine cells. Int. J. Exp. Pathol. 2011, 92, 219–231. [Google Scholar] [CrossRef]
- Appleton, J. The Gut-Brain Axis: Influence of Microbiota on Mood and Mental Health. Integr. Med. 2018, 17, 28–32. [Google Scholar]
- Bonaz, B.; Bazin, T.; Pellissier, S. The Vagus Nerve at the Interface of the Microbiota-Gut-Brain Axis. Front. Neurosci. 2018, 12, 49. [Google Scholar] [CrossRef]
- Rusch, J.A.; Layden, B.T.; Dugas, L.R. Signalling cognition: The gut microbiota and hypothalamic-pituitary-adrenal axis. Front. Endocrinol. 2023, 14, 1130689. [Google Scholar] [CrossRef] [PubMed]
- Sterling, K.G.; Dodd, G.K.; Alhamdi, S.; Asimenios, P.G.; Dagda, R.K.; De Meirleir, K.L.; Hudig, D.; Lombardi, V.C. Mucosal Immunity and the Gut-Microbiota-Brain-Axis in Neuroimmune Disease. Int. J. Mol. Sci. 2022, 23, 13328. [Google Scholar] [CrossRef] [PubMed]
- Masse, K.E.; Lu, V.B. Short-chain fatty acids, secondary bile acids and indoles: Gut microbial metabolites with effects on enteroendocrine cell function and their potential as therapies for metabolic disease. Front. Endocrinol. 2023, 14, 1169624. [Google Scholar] [CrossRef]
- Fairbrass, K.M.; Lovatt, J.; Barberio, B.; Yuan, Y.; Gracie, D.J.; Ford, A.C. Bidirectional brain–gut axis effects influence mood and prognosis in IBD: A systematic review and meta-analysis. Gut 2022, 71, 1773–1780. [Google Scholar] [CrossRef]
- Peppas, S.; Pansieri, C.; Piovani, D.; Danese, S.; Peyrin-Biroulet, L.; Tsantes, A.G.; Brunetta, E.; Tsantes, A.E.; Bonovas, S. The Brain-Gut Axis: Psychological Functioning and Inflammatory Bowel Diseases. J. Clin. Med. 2021, 10, 377. [Google Scholar] [CrossRef] [PubMed]
- Zakerska-Banaszak, O.; Tomczak, H.; Gabryel, M.; Baturo, A.; Wolko, L.; Michalak, M.; Malinska, N.; Mankowska-Wierzbicka, D.; Eder, P.; Dobrowolska, A.; et al. Dysbiosis of gut microbiota in Polish patients with ulcerative colitis: A pilot study. Sci. Rep. 2021, 11, 2166. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Xu, Z.Z.; He, Y.; Yang, Y.; Liu, L.; Lin, Q.; Nie, Y.; Li, M.; Zhi, F.; Liu, S.; et al. Gut Microbiota Offers Universal Biomarkers across Ethnicity in Inflammatory Bowel Disease Diagnosis and Infliximab Response Prediction. mSystems 2018, 3, e00188-17. [Google Scholar] [CrossRef]
- Barberio, B.; Zamani, M.; Black, C.J.; Savarino, E.V.; Ford, A.C. Prevalence of symptoms of anxiety and depression in patients with inflammatory bowel disease: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 6, 359–370. [Google Scholar] [CrossRef]
- Porcelli, P.; Leoci, C.; Guerra, V.; Taylor, G.J.; Bagby, R.M. A longitudinal study of alexithymia and psychological distress in inflammatory bowel disease. J. Psychosom. Res. 1996, 41, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Viganò, C.A.; Beltrami, M.M.; Bosi, M.F.; Zanello, R.; Valtorta, M.; Maconi, G. Alexithymia and Psychopathology in Patients Suffering From Inflammatory Bowel Disease: Arising Differences and Correlations to Tailoring Therapeutic Strategies. Front. Psychiatry 2018, 9, 324. [Google Scholar] [CrossRef]
- Scaldaferri, F.; D’Onofrio, A.M.; Calia, R.; Di Vincenzo, F.; Ferrajoli, G.F.; Petito, V.; Maggio, E.; Pafundi, P.C.; Napolitano, D.; Masi, L.; et al. Gut Microbiota Signatures Are Associated With Psychopathological Profiles in Patients With Ulcerative Colitis: Results From an Italian Tertiary IBD Center. Inflamm. Bowel Dis. 2023, 29, 1805–1818. [Google Scholar] [CrossRef]
- Caenepeel, C.; Falony, G.; Machiels, K.; Verstockt, B.; Goncalves, P.J.; Ferrante, M.; Sabino, J.; Raes, J.; Vieira-Silva, S.; Vermeire, S. Dysbiosis and Associated Stool Features Improve Prediction of Response to Biological Therapy in Inflammatory Bowel Disease. Gastroenterology 2024, 166, 483–495. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N.; Luo, C.; Yajnik, V.; Khalili, H.; Garber, J.J.; Stevens, B.W.; Cleland, T.; Xavier, R.J. Gut Microbiome Function Predicts Response to Anti-integrin Biologic Therapy in Inflammatory Bowel Diseases. Cell Host Microbe 2017, 21, 603–610.e3. [Google Scholar] [CrossRef]
- Magro, F.; Gionchetti, P.; Eliakim, R.; Ardizzone, S.; Armuzzi, A.; Barreiro-de Acosta, M.; Burisch, J.; Gecse, K.B.; Hart, A.L.; Hindryckx, P.; et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. J. Crohn’s Colitis 2017, 11, 649–670. [Google Scholar] [CrossRef]
- Drayton, M. The Minnesota Multiphasic Personality Inventory-2 (MMPI-2). Occup. Med. 2009, 59, 135–136. [Google Scholar] [CrossRef] [PubMed]
- Friedman, A.F.; Bolinskey, P.K.; Levak, R.W.; Nichols, D.S. Psychological Assessment with the MMPI-2/MMPI-2-RF, 3rd ed.; Routledge: London, UK, 2014. [Google Scholar] [CrossRef]
- Vigneau, F.; Cormier, S. The Factor Structure of the State-Trait Anxiety Inventory: An Alternative View. J. Personal. Assess. 2008, 90, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Newham, J.J.; Westwood, M.; Aplin, J.D.; Wittkowski, A. State–trait anxiety inventory (STAI) scores during pregnancy following intervention with complementary therapies. J. Affect. Disord. 2012, 142, 22–30. [Google Scholar] [CrossRef]
- Opheim, R.; Moum, B.; Grimstad, B.T.; Jahnsen, J.; Prytz Berset, I.; Hovde, Ø.; Huppertz-Hauss, G.; Bernklev, T.; Jelsness-Jørgensen, L.-P. Self-esteem in patients with inflammatory bowel disease. Qual. Life Res. 2020, 29, 1839–1846. [Google Scholar] [CrossRef] [PubMed]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Craparo, G.; Faraci, P.; Gori, A. Psychometric Properties of the 20-Item Toronto Alexithymia Scale in a Group of Italian Younger Adolescents. Psychiatry Investig. 2015, 12, 500. [Google Scholar] [CrossRef]
- Lin, S.; Zhang, X.; Zhu, X.; Jiao, J.; Wu, Y.; Li, Y.; Zhao, L. Fusobacterium nucleatum aggravates ulcerative colitis through promoting gut microbiota dysbiosis and dysmetabolism. J. Periodontol. 2023, 94, 405–418. [Google Scholar] [CrossRef]
- Yang, X.; Yang, L.; Zhang, T.; Zhang, H.; Chen, H.; Zuo, X. Causal atlas between inflammatory bowel disease and mental disorders: A bi-directional 2-sample Mendelian randomization study. Front. Immunol. 2023, 14, 1267834. [Google Scholar] [CrossRef]
- Janati, A.I.; Karp, I.; Laprise, C.; Sabri, H.; Emami, E. Detection of Fusobacterium nucleatum in feces and colorectal mucosa as a risk factor for colorectal cancer: A systematic review and meta-analysis. Syst. Rev. 2020, 9, 276. [Google Scholar] [CrossRef]
- Lucafò, M.; Curci, D.; Franzin, M.; Decorti, G.; Stocco, G. Inflammatory Bowel Disease and Risk of Colorectal Cancer: An Overview From Pathophysiology to Pharmacological Prevention. Front. Pharmacol. 2021, 12, 772101. [Google Scholar] [CrossRef]
- Ohkusa, T. Induction of experimental ulcerative colitis by Fusobacterium varium isolated from colonic mucosa of patients with ulcerative colitis. Gut 2003, 52, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Rizzatti, G.; Lopetuso, L.R.; Gibiino, G.; Binda, C.; Gasbarrini, A. Proteobacteria: A Common Factor in Human Diseases. BioMed Res. Int. 2017, 2017, 9351507. [Google Scholar] [CrossRef] [PubMed]
- Winter, S.E.; Winter, M.G.; Xavier, M.N.; Thiennimitr, P.; Poon, V.; Keestra, A.M.; Laughlin, R.C.; Gomez, G.; Wu, J.; Lawhon, S.D.; et al. Host-Derived Nitrate Boosts Growth of E. coli in the Inflamed Gut. Science 2013, 339, 708–711. [Google Scholar] [CrossRef]
- Sokol, H.; Pigneur, B.; Watterlot, L.; Lakhdari, O.; Bermúdez-Humarán, L.G.; Gratadoux, J.-J.; Blugeon, S.; Bridonneau, C.; Furet, J.-P.; Corthier, G.; et al. Faecalibacterium prausnitzii is an anti-inflammatory commensal bacterium identified by gut microbiota analysis of Crohn disease patients. Proc. Natl. Acad. Sci. USA 2008, 105, 16731–16736. [Google Scholar] [CrossRef]
- Lenoir, M.; Martín, R.; Torres-Maravilla, E.; Chadi, S.; González-Dávila, P.; Sokol, H.; Langella, P.; Chain, F.; Bermúdez-Humarán, L.G. Butyrate mediates anti-inflammatory effects of Faecalibacterium prausnitzii in intestinal epithelial cells through Dact3. Gut Microbes 2020, 12, 1826748. [Google Scholar] [CrossRef]
- Miquel, S.; Leclerc, M.; Martin, R.; Chain, F.; Lenoir, M.; Raguideau, S.; Hudault, S.; Bridonneau, C.; Northen, T.; Bowen, B.; et al. Identification of Metabolic Signatures Linked to Anti-Inflammatory Effects of Faecalibacterium prausnitzii. mBio 2015, 6, e00300-15. [Google Scholar] [CrossRef]
- Quévrain, E.; Maubert, M.A.; Michon, C.; Chain, F.; Marquant, R.; Tailhades, J.; Miquel, S.; Carlier, L.; Bermúdez-Humarán, L.G.; Pigneur, B.; et al. Identification of an anti-inflammatory protein from Faecalibacterium prausnitzii, a commensal bacterium deficient in Crohn’s disease. Gut 2016, 65, 415–425. [Google Scholar] [CrossRef]
- Di Vincenzo, F.; Del Gaudio, A.; Petito, V.; Lopetuso, L.R.; Scaldaferri, F. Gut microbiota, intestinal permeability, and systemic inflammation: A narrative review. Intern. Emerg. Med. 2024, 19, 275–293. [Google Scholar] [CrossRef] [PubMed]
- Bajer, L.; Kverka, M.; Kostovcik, M.; Macinga, P.; Dvorak, J.; Stehlikova, Z.; Brezina, J.; Wohl, P.; Spicak, J.; Drastich, P. Distinct gut microbiota profiles in patients with primary sclerosing cholangitis and ulcerative colitis. WJG 2017, 23, 4548. [Google Scholar] [CrossRef]
- Zhuang, X.; Liu, C.; Zhan, S.; Tian, Z.; Li, N.; Mao, R.; Zeng, Z.; Chen, M. Gut Microbiota Profile in Pediatric Patients With Inflammatory Bowel Disease: A Systematic Review. Front. Pediatr. 2021, 9, 626232. [Google Scholar] [CrossRef]
- Firoozi, D.; Masoumi, S.J.; Mohammad-Kazem Hosseini Asl, S.; Labbe, A.; Razeghian-Jahromi, I.; Fararouei, M.; Lankarani, K.B.; Dara, M. Effects of short-chain fatty acid-butyrate supplementation on expression of circadian-clock genes, sleep quality, and inflammation in patients with active ulcerative colitis: A double-blind randomized controlled trial. Lipids Health Dis. 2024, 23, 216. [Google Scholar] [CrossRef] [PubMed]
- Scanu, M.; Toto, F.; Petito, V.; Masi, L.; Fidaleo, M.; Puca, P.; Baldelli, V.; Reddel, S.; Vernocchi, P.; Pani, G.; et al. An integrative multi-omic analysis defines gut microbiota, mycobiota, and metabolic fingerprints in ulcerative colitis patients. Front. Cell. Infect. Microbiol. 2024, 14, 1366192. [Google Scholar] [CrossRef] [PubMed]
- Ghavami, S.B.; Rostami, E.; Sephay, A.A.; Shahrokh, S.; Balaii, H.; Aghdaei, H.A.; Zali, M.R. Alterations of the human gut Methanobrevibacter smithii as a biomarker for inflammatory bowel diseases. Microb. Pathog. 2018, 117, 285–289. [Google Scholar] [CrossRef]
- Feng, Y.; Stams, A.J.M.; De Vos, W.M.; Sánchez-Andrea, I. Enrichment of sulfidogenic bacteria from the human intestinal tract. FEMS Microbiol. Lett. 2017, 364, fnx028. [Google Scholar] [CrossRef]
- Pitcher, M.C.L. The contribution of sulphate reducing bacteria and 5-aminosalicylic acid to faecal sulphide in patients with ulcerative colitis. Gut 2000, 46, 64–72. [Google Scholar] [CrossRef]
- Mottawea, W.; Chiang, C.-K.; Mühlbauer, M.; Starr, A.E.; Butcher, J.; Abujamel, T.; Deeke, S.A.; Brandel, A.; Zhou, H.; Shokralla, S.; et al. Altered intestinal microbiota–host mitochondria crosstalk in new onset Crohn’s disease. Nat. Commun. 2016, 7, 13419. [Google Scholar] [CrossRef]
- Stummer, N.; Feichtinger, R.G.; Weghuber, D.; Kofler, B.; Schneider, A.M. Role of Hydrogen Sulfide in Inflammatory Bowel Disease. Antioxidants 2023, 12, 1570. [Google Scholar] [CrossRef] [PubMed]
- Motta, J.-P.; Flannigan, K.L.; Agbor, T.A.; Beatty, J.K.; Blackler, R.W.; Workentine, M.L.; Da Silva, G.J.; Wang, R.; Buret, A.G.; Wallace, J.L. Hydrogen Sulfide Protects from Colitis and Restores Intestinal Microbiota Biofilm and Mucus Production. Inflamm. Bowel Dis. 2015, 21, 1006–1017. [Google Scholar] [CrossRef]
- Altomare, A.; Putignani, L.; Del Chierico, F.; Cocca, S.; Angeletti, S.; Ciccozzi, M.; Tripiciano, C.; Dalla Piccola, B.; Cicala, M.; Guarino, M.P.L. Gut mucosal-associated microbiota better discloses inflammatory bowel disease differential patterns than faecal microbiota. Dig. Liver Dis. 2019, 51, 648–656. [Google Scholar] [CrossRef]
- Härtel, U.; Buckel, W. Sodium ion-dependent hydrogen production in Acidaminococcus fermentans. Arch. Microbiol. 1996, 166, 350–356. [Google Scholar] [CrossRef]
- Zheng, J.; Hoffman, K.L.; Chen, J.-S.; Shivappa, N.; Sood, A.; Browman, G.J.; Dirba, D.D.; Hanash, S.; Wei, P.; Hebert, J.R.; et al. Dietary inflammatory potential in relation to the gut microbiome: Results from a cross-sectional study. Br. J. Nutr. 2020, 124, 931–942. [Google Scholar] [CrossRef]
- Liu, B.; Ye, D.; Yang, H.; Song, J.; Sun, X.; Mao, Y.; He, Z. Two-Sample Mendelian Randomization Analysis Investigates Causal Associations Between Gut Microbial Genera and Inflammatory Bowel Disease, and Specificity Causal Associations in Ulcerative Colitis or Crohn’s Disease. Front. Immunol. 2022, 13, 921546. [Google Scholar] [CrossRef] [PubMed]
- Haac, B.E.; Palmateer, N.C.; Seaton, M.E.; VanYPeren, R.; Fraser, C.M.; Bafford, A.C. A Distinct Gut Microbiota Exists Within Crohn’s Disease–Related Perianal Fistulae. J. Surg. Res. 2019, 242, 118–128. [Google Scholar] [CrossRef] [PubMed]
- Breton, J.; Tanes, C.; Tu, V.; Albenberg, L.; Rowley, S.; Devas, N.; Hwang, R.; Kachelries, K.; Wu, G.D.; Baldassano, R.N.; et al. A Microbial Signature for Paediatric Perianal Crohn’s Disease. J. Crohn’s Colitis 2022, 16, 1281–1292. [Google Scholar] [CrossRef]
- Jouvent, R.; Bungener, C.; Morand, P.; Millet, V.; Lancrenon, S.; Ferreri, M. Distinction between anxiety state/trait in general practice: A descriptive study. Encephale 1999, 25, 44–49. [Google Scholar]
- Filipovic, B.R. Psychiatric comorbidity in the treatment of patients with inflammatory bowel disease. WJG 2014, 20, 3552. [Google Scholar] [CrossRef] [PubMed]
- Rau, M.; Rehman, A.; Dittrich, M.; Groen, A.K.; Hermanns, H.M.; Seyfried, F.; Beyersdorf, N.; Dandekar, T.; Rosenstiel, P.; Geier, A. Fecal SCFAs and SCFA-producing bacteria in gut microbiome of human NAFLD as a putative link to systemic T-cell activation and advanced disease. UEG J. 2018, 6, 1496–1507. [Google Scholar] [CrossRef]
- Ratajczak, W.; Rył, A.; Mizerski, A.; Walczakiewicz, K.; Sipak, O.; Laszczyńska, M. Immunomodulatory potential of gut microbiome-derived short-chain fatty acids (SCFAs). Acta Biochim. Pol. 2019, 66, 1–12. [Google Scholar] [CrossRef]
- Levak, R.; Siegel, L.; Nichols, D.S.; Stolberg, R. Therapeutic Feedback with the MMPI-2: A Positive Psychology Approach; Routledge, Taylor & Francis Group: New York, NY, USA, 2011. [Google Scholar]
- Alexakis, C.; Kumar, S.; Saxena, S.; Pollok, R. Systematic review with meta-analysis: The impact of a depressive state on disease course in adult inflammatory bowel disease. Aliment. Pharmacol. Ther. 2017, 46, 225–235. [Google Scholar] [CrossRef]
- Mittermaier, C.; Dejaco, C.; Waldhoer, T.; Oefferlbauer-Ernst, A.; Miehsler, W.; Beier, M.; Tillinger, W.; Gangl, A.; Moser, G. Impact of Depressive Mood on Relapse in Patients With Inflammatory Bowel Disease: A Prospective 18-Month Follow-Up Study. Psychosom. Med. 2004, 66, 79–84. [Google Scholar] [CrossRef]
- Levenstein, S.; Prantera, C.; Varvo, V.; Scribano, M.L.; Andreoli, A.; Luzi, C.; Arcà, M.; Berto, E.; Milite, G.; Marcheggiano, A. Stress and Exacerbation in Ulcerative Colitis: A Prospective Study of Patients Enrolled in Remission. Am. J. Gastroenterol. 2000, 95, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Jordi, S.B.U.; Lang, B.M.; Wyss, J.; Auschra, B.; Yilmaz, B.; Krupka, N.; Greuter, T.; Schreiner, P.; Biedermann, L.; Preisig, M.; et al. The personality traits activity, self-reproach, and negative affect jointly predict clinical recurrence, depressive symptoms, and low quality of life in inflammatory bowel disease patients. J. Gastroenterol. 2022, 57, 848–866. [Google Scholar] [CrossRef] [PubMed]
- Schoefs, E.; Vermeire, S.; Ferrante, M.; Sabino, J.; Lambrechts, T.; Avedano, L.; Haaf, I.; De Rocchis, M.S.; Broggi, A.; Sajak-Szczerba, M.; et al. What are the Unmet Needs and Most Relevant Treatment Outcomes According to Patients with Inflammatory Bowel Disease? A Qualitative Patient Preference Study. J. Crohn’s Colitis 2023, 17, 379–388. [Google Scholar] [CrossRef]
- Chew, D.; Zhiqin, W.; Ibrahim, N.; Ali, R.A.R. Optimizing the multidimensional aspects of the patient-physician relationship in the management of inflammatory bowel disease. Intest. Res. 2018, 16, 509–521. [Google Scholar] [CrossRef] [PubMed]
- Hollander, E.; Kwon, J.H.; Stein, D.J.; Broatch, J.; Rowland, C.T.; Himelein, C.A. Obsessive-compulsive and spectrum disorders: Overview and quality of life issues. J. Clin. Psychiatry 1996, 57 (Suppl. 8), 3–6. [Google Scholar]
- Sauk, J.S.; Ryu, H.J.; Labus, J.S.; Khandadash, A.; Ahdoot, A.I.; Lagishetty, V.; Katzka, W.; Wang, H.; Naliboff, B.; Jacobs, J.P.; et al. High Perceived Stress is Associated With Increased Risk of Ulcerative Colitis Clinical Flares. Clin. Gastroenterol. Hepatol. 2023, 21, 741–749.e3. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Therapy failure (n, %) | No (9, 25.7%) |
| Yes (26, 74.3%) | |
| Therapy multifailure (>3) (n, %) | No (23, 65.8%) |
| Yes (12, 34.2%) | |
| Surgery (UC-related) (n, %) | No (30, 85.7%) |
| Yes (5, 14.3%) | |
| Hospitalization (UC-related) (n, %) | No (29, 82.9%) |
| Yes (6, 17.1%) | |
| Variation in diagnosis (CD) (n, %) | No (31, 88.6%) |
| Yes (4, 11.4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scaldaferri, F.; D’Onofrio, A.M.; Chiera, E.; Gomez-Nguyen, A.; Ferrajoli, G.F.; Di Vincenzo, F.; Petito, V.; Laterza, L.; Pugliese, D.; Napolitano, D.; et al. Impact of Psychopathology and Gut Microbiota on Disease Progression in Ulcerative Colitis: A Five-Year Follow-Up Study. Microorganisms 2025, 13, 1208. https://doi.org/10.3390/microorganisms13061208
Scaldaferri F, D’Onofrio AM, Chiera E, Gomez-Nguyen A, Ferrajoli GF, Di Vincenzo F, Petito V, Laterza L, Pugliese D, Napolitano D, et al. Impact of Psychopathology and Gut Microbiota on Disease Progression in Ulcerative Colitis: A Five-Year Follow-Up Study. Microorganisms. 2025; 13(6):1208. https://doi.org/10.3390/microorganisms13061208
Chicago/Turabian StyleScaldaferri, Franco, Antonio Maria D’Onofrio, Elena Chiera, Adrian Gomez-Nguyen, Gaspare Filippo Ferrajoli, Federica Di Vincenzo, Valentina Petito, Lucrezia Laterza, Daniela Pugliese, Daniele Napolitano, and et al. 2025. "Impact of Psychopathology and Gut Microbiota on Disease Progression in Ulcerative Colitis: A Five-Year Follow-Up Study" Microorganisms 13, no. 6: 1208. https://doi.org/10.3390/microorganisms13061208
APA StyleScaldaferri, F., D’Onofrio, A. M., Chiera, E., Gomez-Nguyen, A., Ferrajoli, G. F., Di Vincenzo, F., Petito, V., Laterza, L., Pugliese, D., Napolitano, D., Schiavoni, E., Spagnolo, G., Ferrarese, D., Putignani, L., Lopetuso, L. R., Cammarota, G., Cominelli, F., Gasbarrini, A., Sani, G., & Camardese, G. (2025). Impact of Psychopathology and Gut Microbiota on Disease Progression in Ulcerative Colitis: A Five-Year Follow-Up Study. Microorganisms, 13(6), 1208. https://doi.org/10.3390/microorganisms13061208