
Evaluation of Direct Antimicrobial Susceptibility Testing of Gram-Negative Bacilli and Staphylococcus aureus from Positive Pediatric Blood Culture Bottles Using BD Phoenix M50

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
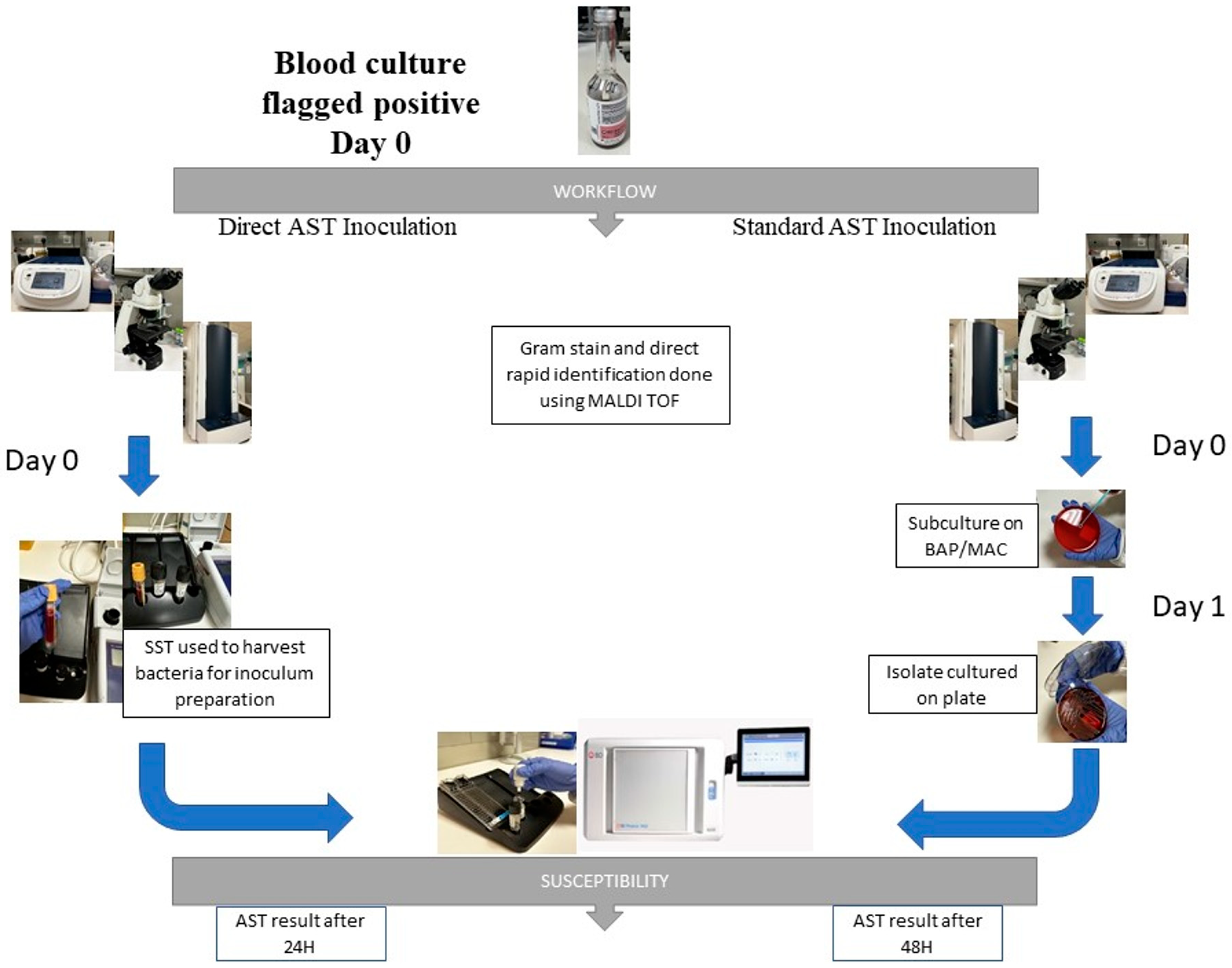
2.1. Study Design, Sample Collection, and Blood Culture Specimen Processing
2.2. AST Using the Standard Method
2.3. AST Using Direct Inoculation
2.4. Conflict Resolution and Statistical Analysis
3. Results
3.1. Samples Tested
3.2. AST Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bearman, G.M.L.; Wenzel, R.P. Bacteremias: A Leading Cause of Death. Arch. Med. Res. 2005, 36, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Lupetti, A.; Barnini, S.; Castagna, B.; Nibbering, P.H.; Campa, M. Rapid Identification and Antimicrobial Susceptibility Testing of Gram-Positive Cocci in Blood Cultures by Direct Inoculation into the BD Phoenix System. Clin. Microbiol. Infect. 2010, 16, 986–991. [Google Scholar] [CrossRef] [PubMed]
- Doern, G.V.; Vautour, R.; Gaudet, M.; Levy, B. Clinical Impact of Rapid In Vitro Susceptibility Testing and Bacterial Identification. J. Clin. Microbiol. 1994, 32, 1757–1762. [Google Scholar] [CrossRef] [PubMed]
- Putnam, L.R.; Howard, W.J.; Pfaller, M.A.; Koontz, F.P.; Jones, R.N. Accuracy of the Vitek System for Antimicrobial Susceptibility Testing Enterobacteriaceae Bloodstream Infection Isolates: Use of “Direct” Inoculation from Bactec 9240 Blood Culture Bottles. Diagn. Microbiol. Infect. Dis. 1997, 28, 101–104. [Google Scholar] [CrossRef] [PubMed]
- Funke, G.; Funke-Kissling, P. Use of the BD PHOENIX Automated Microbiology System for Direct Identification and Susceptibility Testing of Gram-Negative Rods from Positive Blood Cultures in a Three-Phase Trial. J. Clin. Microbiol. 2004, 42, 1466–1470. [Google Scholar] [CrossRef] [PubMed]
- Beuving, J.; van der Donk, C.F.; Linssen, C.F.; Wolffs, P.F.; Verbon, A. Evaluation of Direct Inoculation of the BD PHOENIX System from Positive BACTEC Blood Cultures for Both Gram-Positive Cocci and Gram-Negative Rods. BMC Microbiol. 2011, 11, 156. [Google Scholar] [CrossRef] [PubMed]
- Anton-Vazquez, V.; Adjepong, S.; Suarez, C.; Planche, T. Evaluation of a New Rapid Antimicrobial Susceptibility System for Gram-Negative and Gram-Positive Bloodstream Infections: Speed and Accuracy of Alfred 60AST. BMC Microbiol. 2019, 19, 268. [Google Scholar] [CrossRef]
- Bruins, M.J.; Bloembergen, P.; Ruijs, G.J.H.M.; Wolfhagen, M.J.H.M. Identification and Susceptibility Testing of Enterobacteriaceae and Pseudomonas aeruginosa by Direct Inoculation from Positive BACTEC Blood Culture Bottles into Vitek 2. J. Clin. Microbiol. 2004, 42, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Waites, K.B.; Brookings, E.S.; Moser, S.A.; Zimmer, B.L. Direct Susceptibility Testing with Positive BacT/Alert Blood Cultures by Using MicroScan Overnight and Rapid Panels. J. Clin. Microbiol. 1998, 36, 2052–2056. [Google Scholar] [CrossRef]
- De Cueto, M.; Ceballos, E.; Martinez-Martinez, L.; Perea, E.J.; Pascual, A. Use of Positive Blood Cultures for Direct Identification and Susceptibility Testing with the Vitek 2 System. J. Clin. Microbiol. 2004, 42, 3734–3738. [Google Scholar] [CrossRef] [PubMed]
- Pérez-López, A.; Elamin, N.; Nabor, R.; Dumindin, S.; Roscoe, D.; Hasan, M.R.; Suleiman, M.; Tang, P. Performance and Impact on Initial Antibiotic Choice of Direct Identification of Pathogens from Pediatric Blood Culture Bottles Using an In-House MALDI-TOF MS Protocol. Microbiol. Spectr. 2021, 9, e01905-21. [Google Scholar] [CrossRef]
- Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing: CLSI Supplement M100, 33rd ed.; Clinical and Laboratory Standards Institute (CLSI): Wayne, PA, USA, 2024. [Google Scholar]
- Khan, S.; Das, A.; Mishra, A.; Vidyarthi, A.J.; Nandal, M.; Yadav, H.; Roy, S.; Singh, M. Evaluation of Three Protocols for Direct Susceptibility Testing for Gram-Negative Rods from Flagged Positive Blood Culture Bottles. Microbiol. Spectr. 2024, 12, e03081-23. [Google Scholar] [CrossRef]
- Hogan, C.; Watz, N.; Budvytiene, I.; Banaei, N. Rapid Antimicrobial Susceptibility Testing by VITEK®2 Directly from Blood Cultures in Patients with Gram-Negative Rod Bacteremia. Diagn. Microbiol. Infect. Dis. 2019, 94, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Paluch, M.; Lleres-Vadeboin, M.; Poupet, H.; Chanard, E.; Wilhelm, N.; Nadji, S.; Prots, L.; Bala, Y.; Zambardi, G.; Cattoen, C. Multicenter Evaluation of Rapid Antimicrobial Susceptibility Testing by VITEK®2 Directly from Positive Blood Culture. Diagn. Microbiol. Infect. Dis. 2023, 106, 115950. [Google Scholar] [CrossRef] [PubMed]
- Kwiecinski, J.M.; Horswill, A.R. Staphylococcus aureus Bloodstream Infections: Pathogenesis and Regulatory Mechanisms. Curr. Opin. Microbiol. 2020, 53, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Squadrito, F.J.; del Portal, D. Nitrofurantoin. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]

{kind=link}
| Bacterial Isolates (n) | Total Tested | %EA | %CA | mE (%) | ME (%) | VME (%) |
|---|---|---|---|---|---|---|
| Gram-negative Enterobacterales | ||||||
| Klebsiella pneumoniae (28) | 728 | 99.3 | 98.9 | 3 (0.4%) | 3 (0.4%) | 2 (0.3%) |
| Klebsiella oxytoca (1) | 26 | 100 | 100 | 0 | 0 | 0 |
| Klebsiella aerogenes (1) | 26 | 100 | 100 | 0 | 0 | 0 |
| Escherichia coli (15) | 390 | 100 | 99.4 | 2 (0.5%) | 0 | 0 |
| Enterobacter spp. (5) | 130 | 100 | 99.2 | 1 (0.8%) | 0 | 0 |
| Salmonella spp. (9) | 234 | 100 | 99.1 | 2 (0.8%) | 0 | 0 |
| Citrobacter spp. (1) | 26 | 100 | 100 | 0 | 0 | 0 |
| Serratia marcescens (5) | 130 | 100 | 100 | 0 | 0 | 0 |
| Gram-negative non-fermenters | ||||||
| Pseudomonas aeruginosa (13) | 338 | 100 | 100 | 0 | 0 | 0 |
| Acinetobacter spp. (8) | 208 | 100 | 100 | 0 | 0 | 0 |
| Gram-positive | ||||||
| Staphylococcus aureus (46) | 1058 | 99.9 | 99.9 | 0 | 0 | 1 (0.09%) |
| Total (132) | 3294 | 99.8 | 99.6 | 8 (0.20%) | 3 (0.09%) | 3 (0.09%) |
| Antimicrobial Agents | (n) | %EA | %CA | mE (%) | ME (%) | VME (%) |
|---|---|---|---|---|---|---|
| Amikacin | 86 | 100 | 100 | 0 | 0 | 0 |
| Ampicillin | 132 | 100 | 100 | 0 | 0 | 0 |
| Ampicillin–Sulbactam | 86 | 100 | 98.8 | 1 (1.2%) | 0 | 0 |
| Azteronam | 86 | 100 | 100 | 0 | 0 | 0 |
| Ceftaroline | 46 | 100 | 100 | 0 | 0 | 0 |
| Cefotaxime | 46 | 100 | 100 | 0 | 0 | 0 |
| Cefazolin | 86 | 100 | 98.8 | 1 (1.2%) | 0 | 0 |
| Cefepime | 86 | 100 | 100 | 0 | 0 | 0 |
| Cefoxitin | 132 | 100 | 100 | 0 | 0 | 0 |
| Ceftazidime | 86 | 100 | 100 | 0 | 0 | 0 |
| Ceftazidime–Avibactam | 86 | 100 | 100 | 0 | 0 | 0 |
| Ceftolozane–Tazobactam | 86 | 100 | 100 | 0 | 0 | 0 |
| Ceftriaxone | 86 | 100 | 98.8 | 1 (1.2%) | 0 | 0 |
| Cefuroxime | 86 | 100 | 97.7 | 2 (2.3%) | 0 | 0 |
| Ciprofloxacin | 132 | 100 | 99.2 | 1 (1.2%) | 0 | 0 |
| Clindamycin | 46 | 100 | 100 | 0 | 0 | 0 |
| Colistin | 86 | 100 | 100 | 0 | 0 | 0 |
| Daptomycin | 46 | 100 | 100 | 0 | 0 | 0 |
| Erythromycin | 46 | 100 | 100 | 0 | 0 | 0 |
| Ertapenem | 86 | 98.8 | 98.8 | 0 | 1 (1.2%) | 0 |
| Fosfomycin | 86 | 98.8 | 98.8 | 0 | 1 (1.2%) | 0 |
| Gentamicin | 132 | 100 | 100 | 0 | 0 | 0 |
| Gentamycin-synergy | 46 | 100 | 100 | 0 | 0 | 0 |
| Imipenem | 86 | 100 | 100 | 0 | 0 | 0 |
| Levofloxacin | 132 | 100 | 100 | 0 | 0 | 0 |
| Linezolid | 46 | 100 | 100 | 0 | 0 | 0 |
| Moxifloxacin | 46 | 100 | 100 | 0 | 0 | 0 |
| Mupirocin HL | 46 | 100 | 100 | 0 | 0 | 0 |
| Meropenem | 86 | 100 | 100 | 0 | 0 | 0 |
| Minocycline | 86 | 100 | 100 | 0 | 0 | 0 |
| Nitrofurantoin | 132 | 98.4 | 97.7 | 1 (0.75%) | 0 | 2 (1.5%) |
| Norfloxacin | 86 | 100 | 100 | 0 | 0 | 0 |
| Oxacillin | 46 | 100 | 100 | 0 | 0 | 0 |
| Penicillin | 46 | 100 | 100 | 0 | 0 | 0 |
| Piperacillin–Tazobactam | 86 | 100 | 100 | 0 | 0 | 0 |
| Rifampin | 46 | 100 | 100 | 0 | 0 | 0 |
| Tetracycline | 46 | 100 | 100 | 0 | 0 | 0 |
| Teicoplanin | 46 | 100 | 100 | 0 | 0 | 0 |
| Tigecycline | 132 | 99.2 | 98.4 | 1 (0.75%) | 1 (0.75%) | 0 |
| SXT | 132 | 99.2 | 99.2 | 0 | 0 | 1 (0.9%) |
| Vancomycin | 46 | 100 | 100 | 0 | 0 | 0 |
| Total | 3294 | 99.8 | 99.6 | 8 (0.20%) | 3 (0.09%) | 3 (0.09%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales, P.; Tang, P.; Mariano, E.; Gopalan, A.; Aji, N.; Pérez-López, A.; Suleiman, M. Evaluation of Direct Antimicrobial Susceptibility Testing of Gram-Negative Bacilli and Staphylococcus aureus from Positive Pediatric Blood Culture Bottles Using BD Phoenix M50. Microorganisms 2024, 12, 1704. https://doi.org/10.3390/microorganisms12081704
Morales P, Tang P, Mariano E, Gopalan A, Aji N, Pérez-López A, Suleiman M. Evaluation of Direct Antimicrobial Susceptibility Testing of Gram-Negative Bacilli and Staphylococcus aureus from Positive Pediatric Blood Culture Bottles Using BD Phoenix M50. Microorganisms. 2024; 12(8):1704. https://doi.org/10.3390/microorganisms12081704
Chicago/Turabian StyleMorales, Princess, Patrick Tang, Elaine Mariano, Arun Gopalan, Nisha Aji, Andrés Pérez-López, and Mohammed Suleiman. 2024. "Evaluation of Direct Antimicrobial Susceptibility Testing of Gram-Negative Bacilli and Staphylococcus aureus from Positive Pediatric Blood Culture Bottles Using BD Phoenix M50" Microorganisms 12, no. 8: 1704. https://doi.org/10.3390/microorganisms12081704
APA StyleMorales, P., Tang, P., Mariano, E., Gopalan, A., Aji, N., Pérez-López, A., & Suleiman, M. (2024). Evaluation of Direct Antimicrobial Susceptibility Testing of Gram-Negative Bacilli and Staphylococcus aureus from Positive Pediatric Blood Culture Bottles Using BD Phoenix M50. Microorganisms, 12(8), 1704. https://doi.org/10.3390/microorganisms12081704