Abstract
Extended reality (XR) devices, including virtual and augmented reality head-mounted displays (HMDs), are increasingly utilised within healthcare to provide clinical interventions and education. Currently, XR devices are utilised to assist in reducing pain and improving psychological outcomes for immunocompromised patients in intensive care units, palliative care environments and surgical theatres. However, there is a paucity of research on the risks of infection from such devices in healthcare settings. Identify existing literature providing insights into the infection control risk XR HMDs pose within healthcare facilities and the efficacy of current infection control and cleaning procedures. Three databases (PubMed, Embase and CINAHL) in addition to Google Scholar were systematically searched. A total of seven studies were identified for this review. Microorganisms, including pathogenic bacteria (e.g., Staphylococcus aureus and Pseudomonas aeruginosa), were found to be present on XR HMDs. Published cleaning and infection control protocols designed to disinfect XR HMDs and protect users were heterogeneous in nature. Current cleaning protocols displayed varying levels of efficacy with microbial load affected by multiple factors, including time in use, number of users and XR HMD design features. In healthcare settings, fitting XR HMDs harbouring microorganisms near biological and mucosal entry points presents an infection control risk. An urgent revision of the Spaulding classification is required to ensure flexibility that allows for these devices to be reclassified from ‘Non-critical’ to ‘Semi-Critical’ depending on the healthcare setting and patient population (surgery, immunocompromised, burns, etc.). This review identified evidence supporting the presence of microorganisms on XR HMDs. Due to the potential for HMDs to contact mucosal entry points, devices must be re-considered within the Spaulding classification as ‘Semi-critical’. The existence of microbial contaminated XR HMDs in high-risk medical settings such as operating wards, intensive care units, emergency departments, labour and delivery wards and clinical areas with immunosuppressed patients requires urgent attention. Public health authorities have a duty of care to develop revised guidelines or new recommendations to ensure efficient sanitation of such devices.
1. Introduction
Overview
Extended reality (XR), encompassing virtual, augmented and mixed reality, is increasingly being integrated across various industries from leisure and gaming to education and healthcare. In 2023, there were approximately 171 million virtual reality (VR) users globally, with healthcare anticipated to experience the greatest adoption, increasing from a market value of USD 3.11 billion in 2023, to USD 25.22 billion by 2030 [1,2]. Currently, XR head-mounted displays (HMDs) are rapidly being integrated into healthcare settings, which require strict infection control policies and procedures such as surgery [3,4,5], intensive care units [6,7,8], palliative care [9] and oncology [10,11,12,13] to improve clinical outcomes. As a result, XR equipment meets the current definition of a medical device according to the Food and Drug Administration (FDA) [14] and the Therapeutic Goods Administration (TGA) [15,16]. Hospitals and health care workers currently require clear guidance as to the optimal strategy to ameliorate risks of hospital acquired infections (HAIs) associated with XR equipment.
Fomites are inanimate platforms subject to contact and deposition of droplets from any living organism shedding such infectious agents. Factors such as humidity, moisture, temperature, UV exposure, nature and type of microorganisms collectively influence whether microorganisms will adhere to and survive on a fomite [17,18,19]. XR equipment (1) are frequently exposed to hands, skin and biological secretions; (2) receive nasopharyngeal droplets which contain viruses and bacteria, due to close proximity to the eyes, nose and other areas of the head; (3) undergo temperature fluctuations [20], providing the suitable environmental conditions for growth of pathogens; (4) lack validated and implemented sanitation protocols and; (5) are used in high-risk healthcare settings.
Mobile phones are similar fomites which are widely utilised within the healthcare industry, and in conjunction with XR headsets as part of the visual display, to assist the healthcare provider in controlling and visualizing the XR-related intervention. Metagenomic next-generation sequencing has demonstrated mobile phones from medical staff within a paediatric intensive care, neonatal intensive care and emergency department setting have the potential to act as a reservoir for “ESKAPE” pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumanii, Pseudomonas aeruginosa and Enterobacter spp.) and antimicrobial resistance genes [21,22]. Studies have reported that only a small quantity of microorganisms may be sufficient to infect the host [23]. Together, this research demonstrates the need to further ensure that XR HMDs, and the associated infection control risks, are managed appropriately, especially when used in high-risk patient populations and/or healthcare settings.
The economic burden HAIs represent to already strained public healthcare systems currently represents a major global public health crisis. Worldwide costs associated with HAIs are difficult to quantify, and publicly available estimates differ between countries. In the United States of America (USA) HAIs cost an estimated USD 28–45 billion each year [24], with a recent study estimating the annual economic burden to be in the range of USD 96 billion to USD 147 billion annually, encompassing both direct and indirect costs [25]. The costs associated with HAIs fluctuates due to a series of factors, including patient population, study settings/environments, data obtained from index hospitalization costs, the inclusion of outpatient costs and multi-drug resistant infections [26,27].
This systematic review aims to determine if XR HMDs are potentially hazardous fomites posing a risk to individuals within the healthcare sector, and in particular, within high-risk settings and/or immunocompromised individuals. Additionally, we aim to identify and compare the recommended cleaning protocols used to date to sanitise XR equipment and to determine the efficacies of the cleaning procedures to provide recommendations for future research and to assist in the develop of clinical interventions.
2. Methods
2.1. Search Strategy
A systematic search was developed in line with the following three-step methodological approach outlined by the Johanna Briggs Institute: (a) a preliminary literature search was undertaken in PubMed and Google Scholar, (b) additional search terms were identified and search strategies translated with the assistance of a validated search engine translation software (Polyglot, https://sr-accelerator.com/#/polyglot, accessed on 26 August 2023), (c) execution of final search strategies [28]. The search strategy consisted of: (“virtual reality” OR “augmented reality” OR “mixed reality” OR “extended reality”) AND (microbe OR microbial OR infection OR bacteria OR virus OR pandemic OR fomite) AND (Colony forming unit* OR metagenomic OR sterilis* OR clean OR disinfect* OR sanitis* OR hygiene OR guideline).
2.2. Information Sources and Study Selection
Three databases (PubMed, EMBASE and CINAHL) and Google Scholar were searched on 26 August 2023. All results from the databases and the first 100 Google Scholar results were exported into EndNote X9. Forward–backwards citation searching alongside an additional search for grey literature was performed in an attempt to undertake a thorough evaluation of the literature.
2.3. Data Extraction and Quality Assessment of Sources
Duplicate results were removed within Systematic Review Accelerator’s validated deduplication software utilising the focused algorithm prior to being manually reviewed. Articles were screened first by title and abstract and then by full text by two authors (MO and AG) against predefined inclusion and exclusion criteria within Systematic Review Accelerator’s Screenatron. Articles which were included aimed at investigating and/or analysing the level of microbial contamination or the cleaning procedures employed. Articles were excluded if they were not available in English.
3. Results
Selection of Sources of Evidence
Following the systematic search, 365 articles were identified from the literature, with 39 articles from PubMed, 163 from EMBASE, 63 from CINAHL and 100 from Google Scholar. After duplicates were removed, the remaining 331 articles were screened based on the inclusion criteria. Of these, eight full-text articles were assessed for eligibility, of which one article was excluded for not meeting the inclusion criteria. Finally, seven articles met the criteria for full review and were included in the final analysis. Figure 1 represents the PRISMA flow diagram outlining the selected studies that passed the criteria for full review.
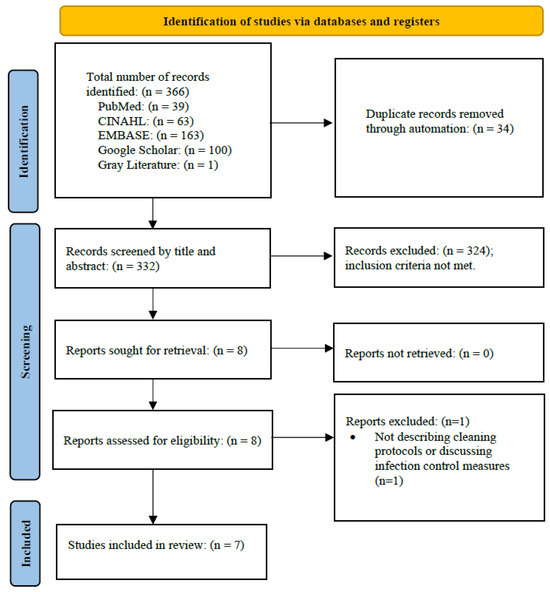
Figure 1.
PRISMA flow diagram of selection protocol for studies included for full review.
No identified article undertook a cleaning validation of XR HMDs within a healthcare setting (Table 1). One study investigated the presence of microorganisms on devices within a university education setting [29]. Two further studies [30,31] investigated the recovery of microorganisms following inoculation of various microbes (Table 2). Two surveys [30,32] and one scoping review [6] investigated the current cleaning and infection control practices within the healthcare industry. The five cleaning protocols [29,30,31,33,34] which were described were heterogeneous, with only one article [30] explicitly advocating for cleaning to be undertaken pre and post at every utilisation of XR (Table 3).

Table 1.
Summary of aims and comments of the articles included in this systematic review.
Table 2.
Studies confirming the presence and recovery of microorganisms from VR headsets.
Table 3.
Cleaning protocols implemented in five articles.
In the study by Creel et al. [29], the most frequently isolated bacteria was Staphylococcus aureus, with 37 colonies reported. Additionally, this study identified antimicrobial resistance to 4 antibiotics from the 37 colonies of Staphylococcus aureus (Erythromycin (27 colonies), Penicillin (22 colonies), Tetracycline (24 colonies) and Gentamycin (2 colonies)) [29]. This study also identified several additional bacteria, including Moraxella osloensis, Micrococcus luteus, Kocuria rosea, Rothia kristinae, Dermacoccus nishinomiyaensis, Moraxella osloensis 2, Corynebacterium ihumii, Staphylococcus argensis and Moraxella osloensis 3 [29].
On the other hand, the study by Roberts et al. [30] performed a disinfection study where laboratory-grown bacteria were inoculated onto VR headsets. From this study, Staphylococcus epidermidis (ATCC 12228), Pseudomonas aeruginosa (laboratory strain PAO1) and Staphylococcus aureus (ATCC 25923) were recovered from VR headsets following disinfection. Similarly, Daniel et al. [31] performed a sterilisation study with dry chlorine dioxide (dClO2) with laboratory-grown bacteria inoculated onto VR headsets. From this study, Staphylococcus aureus, Pseudomonas aeruginosa, Burkholderia multivorans, Acinetobacter baumanni, Mycobacteroides chelonae and Candida albicans were inoculated, recovered and cultured from HMDs post disinfection [31].
4. Discussion
Overview
This systematic review demonstrates that little research has been undertaken to date regarding the microbial contamination of XR devices and associated infection control procedures [6]. A wide variety of hardware devices are currently used with varying design features utilising both porous and non-porous materials [6,30,32,35]. No current “gold standard” cleaning procedures and protocols have been developed. Currently implemented cleaning strategies involve the use chemical cleaning wipes, UV-C technology, chlorine dioxide gas (dClO2) and reusable or disposable covers for the facial interface. In addition, no cleaning validation studies undertaken in healthcare facilities have been reported, demonstrating that XR HMDs are entirely and efficiently disinfected through robust infection control procedures. As a result, this systematic review has identified XR-HMDs as important fomites that require attention from an infection control perspective to ensure they are able to be sanitised efficiently. Our review also demonstrates a lack of scientific literature evaluating the risk current XR HMDs pose to immunocompromised individuals in health care settings.
In medical settings, XR HMDs are classified as “non-critical” medical equipment under the Spaulding classification as the device is intended to come in contact with intact skin only [33]. As a result, XR equipment is assumed to require low to intermediate levels of disinfection between patients [36]. This ‘non-critical’ classification suggests that XR devices are at low risk of infection transmission. However, this current Spaulding classification fails to consider three major points. Firstly, HMDs might not be optimally sanitised/sterilised as cleaning protocols associated with low or intermediate recommended levels of disinfection do not eliminate all non-enveloped viruses, fungi and spores, and the design of current HMDs provides significant challenges to disinfection [37]. When XR HMDs are used by patients or medical staff, the user’s flora or pathogens might be deposited on these devices’ external surfaces, crevices and optic projection areas. Liquids from microbial-laden nasopharyngeal droplets during breathing or sneezing or salivary droplets when talking or coughing are inadvertently expulsed towards the crevices, narrow fissures and adjustment-openings and will penetrate any porous surfaces on the HMDs. Additionally, XR HMDs have internal components (e.g., fans) that may become niches for pathogenic microorganisms providing additional challenges to achieving adequate levels of disinfection. Of particular interest, the study by Creel et al. [29] swabbed two HTC VIVE VR devices that were used for an Immersive Media course in the University of Mississippi. The authors showed the growth of viable microorganisms cultured in three different media with the number of colony-forming units, sourced from swabbing headsets, increasing over the course of their seven-week study [29].
Secondly, the classification fails to adequately consider the proximity of HMDs to the mucosal points of entry of the user’s exposed face as a possible means by which pathogenic microorganisms can contaminate the user via various routes. For example, during the donning and doffing of some devices, direct contact is common between the facial interface and users’ eyelids and eyelashes, structures that interface with mucous membranes of the eyes [38]. The dynamic manner in which XR HMDs are designed to be utilised may also result in microorganisms translocating from the device to various mucous membranes. Of particular consideration for healthcare settings is the manner in which XR HMDs may act as a fomite which negates hand hygiene. Only one of five cleaning protocols reported in this systematic review commented on the necessity for patients and healthcare providers to undertake hand hygiene both prior to and following XR use [30]. The adjustment and usage of suboptimally decontaminated XR HMDs by either the patient or healthcare worker negates hand hygiene procedures increasing the risk of HAIs and impact on the health of the XR users. Infections such as acute haemorrhagic conjunctivitis may result from users rubbing their eyes or face following removal of the equipment [39]. In this way, XR devices may act as ‘trojan horses’ for microbial contamination and infection spread.
Thirdly, XR devices are increasingly being utilised within high-risk settings such as operating theatres and intensive care units as well as with immunocompromised patients (Figure 2). For example, XR headsets have been shown to have great utility and are currently utilised by both surgeons to assist in providing virtual displays and for patients to assist with pain management and anxiety during surgery. The high risks of fomite-based transmission in these settings emphasise the need for sophisticated infection control protocols and sanitisation policies to ensure these devices do not present the risks of a hazardous fomite.
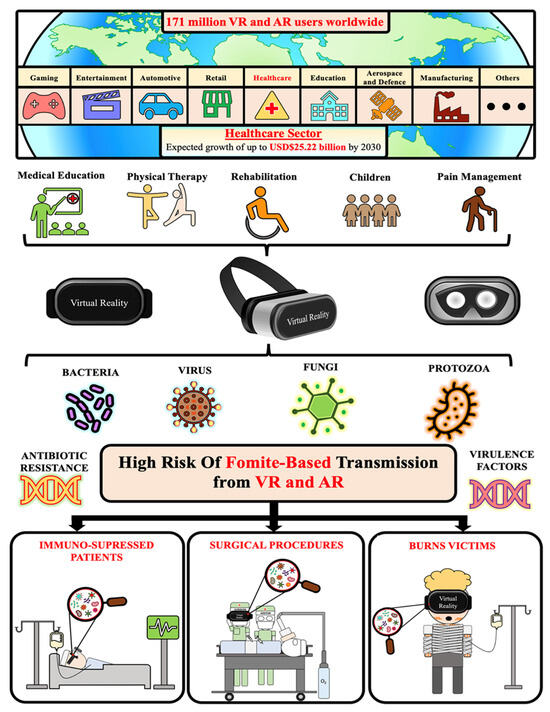
Figure 2.
Overview of extended reality devices and their role as potential fomites in high-risk healthcare environments with implications for immune suppressed and immune-compromised individuals.
Daniel et al. [31] utilised dry chlorine gas to disinfect VR HMDs. This technique may assist in disinfecting crevices and other areas that are hard to clean via other manual methods effectively. However, previous research has demonstrated dry chlorine gas to be less effective at disinfecting porous surfaces raising concern regarding the method’s efficacy at sterilising the porous surfaces associated with some facial interfaces and head straps [40]. Roberts et al. [30] also demonstrated that porous materials from such headsets were more difficult to disinfect than non-porous parts of the VR headsets. In their study, the authors investigated the efficacy of two different disinfectants (Isopropanol and quaternary ammonium) on two popular VR headsets (Oculus Quest and Oculus Quest 2). Samples were swabbed on high-touch porous and non-porous surface areas of the VR sets to monitor the survivability of three bacteria. Whilst physical barriers, both disposable and cleanable, are commonly utilised to cover the porous facial interface, no data was identified to assist in understanding if this measure is effective at preventing this porous surface from becoming a reservoir for pathogenic microbes.
Of note, recommendations currently outlined in the draft of the international standards organisation suggest that UV-C when properly utilised is an effective cleaning tool for HMDs including their associated facial interfaces and controllers. In contrast Roberts et al. [30] describe UV-C to be an ineffective sanitisation tool for VR equipment, but details regarding devices, methodology, data and results were not disclosed. Major advantages of the use of UV-C sanitisation include the removal of human variance in cleaning efficacy as well as the ability to incorporate mechanisms to electronically record data regarding the time and date specific devices were sanitised for recordkeeping purposes. Conversely, the rapid manner in which HMDs with vastly different profiles and designs are being developed, provides challenges to the design of UV-C sanitisation devices as the light emitting diodes (LEDs) are likely required to be in close proximity to the device to be of sufficient germicidal efficacy. Further research is warranted to validate current commercially available UV-C devices as an effective sanitisation method and to facilitate the development of more effective and robust XR UV-C technology in the future.
5. Study Limitations
As a result of the limited literature to date which has been published investigating the microbial contamination of XR HMDs, this review is currently unable to provide strong recommendations as to the optimal strategy which should be utilised to sanitise XR HMDs. Additionally, as research investigating this important issue is published, it will likely necessitate a re-evaluation of the literature.
6. Author’s Recommendations
To date, very little evidence has been published describing the extent to which XR-HMDs are contaminated with pathogenic microbes. Additionally, no robust solutions are in place to mitigate these risks despite the use of XR devices in high-risk healthcare settings. Infographic 2 illustrates our recommendation for reclassifying XR equipment within the Spaulding’s classification (Figure 3). The first step to understanding the risk posed by XR equipment includes defining the microbial load and spectrum present on such devices. The characterisation of the microbial virulence and potential antimicrobial resistance present on XR equipment would further demonstrate the clinical importance of decontaminating these important fomites. The second stage involves undertaking cleaning validation studies of various cleaning protocols to validate sanitation protocols that can be effectively implemented in healthcare settings. Finally, a review of policy is required to ensure sanitisation procedures are correctly undertaken, which may also include an elaboration of Spaulding’s classification to allow for flexibility of medical devices such as XR from “non-critical” to “semi-critical” when used in high-risk environments or within various high-risk patient populations. Overall, the utility of XR devices and their benefits in the healthcare sector are paramount and the risks associated with their use from an infection control perspective must be taken seriously.
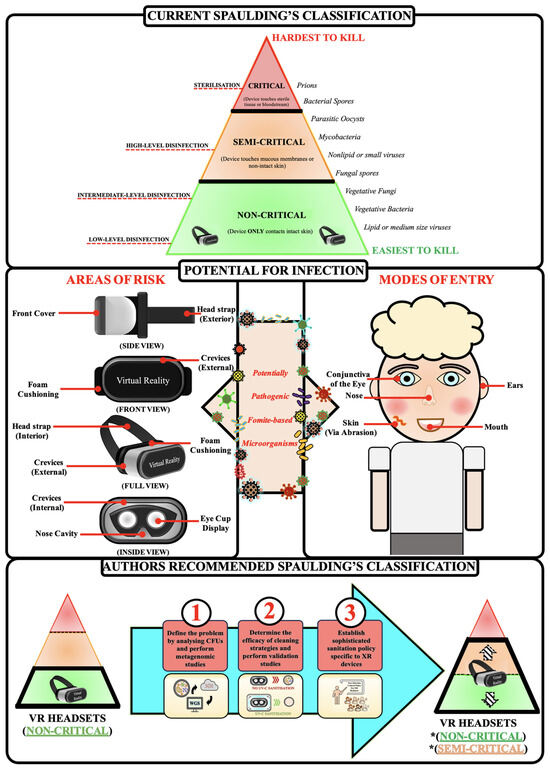
Figure 3.
Strategic plan for further research and potential solutions to XR headset fomites. * Classification dependent on factors such as environment and patient population. For example, in physiotherapy, XR HMDs within musculoskeletal private practice should be classified as non-critical. However, when XR-HMDs are utilised in conjunction with immunocompromised individuals, they could be classified as semi-critical.
7. Conclusions
The utilisation of sophisticated XR devices within the healthcare sector is becoming increasingly adopted, yet the potential for microbial dissemination from these devices is currently overlooked. HMDs are fomites, and the current application of disinfection strategies to sanitise these devices is likely to be suboptimal given the current classification as ‘non-critical’ medical devices under the Spaulding classification. The current use of HMDs within healthcare settings, especially high-risk settings such as operating theatres and with immune-compromised individuals may be exposing users to pathogenic microbes resulting in adverse patient outcomes and higher morbidity and mortality. Considering the rapid development of immersive XR HMD technology in healthcare settings and the likely fact that these devices are important fomites, based on our knowledge of other mobile devices, it is necessary to consider the re-classification of HMDs to semi-critical devices in these settings. Implementing stringent sanitisation protocols is imperative to establish effective XR infection control measures, ensuring that XR devices can continue to enhance patient outcomes within a safe patient care workflow.
Funding
This research received no external funding.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fortune Business Insights. Virtual Reality (VR in Healthcare Market Size, Share & COVID-19 Impact Analysis, by Component (Hardware, Software, and Content), by Application (Pain Management, Education & Training, Surgery, Paitient Care Management, Rehabilitation & Therapy Procedures, and Post-Traumatic Stress Disorder (PTSD), and Regional Forecast, 2023–2020; Fortune Business Insights: Pune, India, 2022. [Google Scholar]
- Perkins Coie LLP. Augmented and Virtual Reality Survey Report; Perkins Coie LLP: Washington, DC, USA, 2020. [Google Scholar]
- Barcali, E.; Iadanza, E.; Manetti, L.; Francia, P.; Nardi, C.; Bocchi, L. Augmented reality in surgery: A scoping review. Appl. Sci. 2022, 12, 6890. [Google Scholar] [CrossRef]
- Eves, J.; Sudarsanam, A.; Shalhoub, J.; Amiras, D. Augmented reality in vascular and endovascular surgery: Scoping review. JMIR Serious Games 2022, 10, e34501. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, V.; Khanduja, V. The impact of extended reality on surgery: A scoping review. Int. Orthop. 2023, 47, 611–621. [Google Scholar] [CrossRef]
- Goldsworthy, A.; Chawla, J.; Baumann, O.; Birt, J.; Gough, S. Extended Reality Use in Paediatric Intensive Care: A Scoping Review. J. Intensive Care Med. 2023, 38, 856–877. [Google Scholar] [CrossRef]
- Hill, J.E.; Twamley, J.; Breed, H.; Kenyon, R.; Casey, R.; Zhang, J.; Clegg, A. Scoping review of the use of virtual reality in intensive care units. Nurs. Crit. Care 2022, 27, 756–771. [Google Scholar] [CrossRef]
- Bruno, R.R.; Bruining, N.; Jung, C.; VR-ICU Study group Kelm Malte Wolff Georg Wernly Bernhard. Virtual reality in intensive care. Intensive Care Med. 2022, 48, 1227–1229. [Google Scholar] [CrossRef]
- Mo, J.; Vickerstaff, V.; Minton, O.; Tavabie, S.; Taubert, M.; Stone, P.; White, N. How effective is virtual reality technology in palliative care? A systematic review and meta-analysis. Palliat. Med. 2022, 36, 1047–1058. [Google Scholar] [CrossRef]
- Chirico, A.; Lucidi, F.; De Laurentiis, M.; Milanese, C.; Napoli, A.; Giordano, A. Virtual reality in health system: Beyond entertainment. A mini-review on the efficacy of VR during cancer treatment. J. Cell. Physiol. 2016, 231, 275–287. [Google Scholar] [CrossRef]
- Yap, K.Y.-L.; Koh, D.W.H.; Lee, V.S.J.; Wong, L.L. Use of virtual reality in the supportive care management of paediatric patients with cancer. Lancet Child Adolesc. Health 2020, 4, 899–908. [Google Scholar] [CrossRef]
- Zeng, Y.; Zhang, J.-E.; Cheng, A.S.; Cheng, H.; Wefel, J.S. Meta-analysis of the efficacy of virtual reality-based interventions in cancer-related symptom management. Integr. Cancer Ther. 2019, 18, 1534735419871108. [Google Scholar] [CrossRef]
- Pittara, M.; Matsangidou, M.; Stylianides, K.; Petkov, N.; Pattichis, C.S. Virtual reality for pain management in cancer: A comprehensive review. IEEE Access 2020, 8, 225475–225489. [Google Scholar] [CrossRef]
- Sutton, B. 2011 01/04/2018. Available online: https://www.fda.gov/training-and-continuing-education/cdrh-learn/overview-regulatory-requirements-medical-devices-transcript#:~:text=It%20can%20be%20found%20in,%2C%20diagnose%20disease%20in%20man%E2%80%9D (accessed on 27 August 2023).
- Medical Devices Overview 2023. 13 April 2023. Available online: https://www.tga.gov.au/products/medical-devices/medical-devices-overview (accessed on 27 August 2023).
- Is My Product a Medical Device? Available online: https://www.tga.gov.au/resources/my-product-medical-device (accessed on 27 August 2023).
- Bright, K.R.; Boone, S.A.; Gerba, C.P. Occurrence of bacteria and viruses on elementary classroom surfaces and the potential role of classroom hygiene in the spread of infectious diseases. J. Sch. Nurs. 2010, 26, 33–41. [Google Scholar] [CrossRef]
- Vasickova, P.; Pavlik, I.; Verani, M.; Carducci, A. Issues concerning survival of viruses on surfaces. Food Environ. Virol. 2010, 2, 24–34. [Google Scholar] [CrossRef]
- Kramer, A.; Assadian, O. Survival of microorganisms on inanimate surfaces. Use Biocidal Surf. Reduct. Healthc. Acquir. Infect. 2014, 7–26. [Google Scholar] [CrossRef]
- Wang, Z.; He, R.; Chen, K. Thermal comfort and virtual reality headsets. Appl. Ergon. 2020, 85, 103066. [Google Scholar] [CrossRef]
- Xu, X.; Kilroy, D.; Mangina, E.; Campbell, A.G. Work-in-progress—Adapting a virtual reality anatomy teaching tool for mobility: Pilot study. In Proceedings of the 2020 6th International Conference of the Immersive Learning Research Network (iLRN), San Luis Obispo, CA, USA, 21–25 June 2020; pp. 328–331. [Google Scholar]
- Tajouri, L.; Campos, M.; Olsen, M.; Lohning, A.; Jones, P.; Moloney, S.; Grimwood, K.; Ugail, H.; Mahboub, B.; Alawar, H. The role of mobile phones as a possible pathway for pathogen movement, a cross-sectional microbial analysis. Travel Med. Infect. Dis. 2021, 43, 102095. [Google Scholar] [CrossRef]
- Doron, S.; Gorbach, S.L. Bacterial infections: Overview. Int. Encycl. Public Health 2008, 273–282. [Google Scholar] [CrossRef]
- Stone, P.W. Economic burden of healthcare-associated infections: An American perspective. Expert Rev. Pharmacoecon. Outcomes Res. 2009, 9, 417–422. [Google Scholar] [CrossRef]
- Marchetti, A.; Rossiter, R. Economic burden of healthcare-associated infection in US acute care hospitals: Societal perspective. J. Med. Econ. 2013, 16, 1399–1404. [Google Scholar] [CrossRef]
- Chow, E.J.; Mermel, L.A. Hospital-acquired respiratory viral infections: Incidence, morbidity, and mortality in pediatric and adult patients. In Open Forum Infectious Diseases; Oxford University Press: Cary, NC, USA, 2017; p. ofx006. [Google Scholar]
- Zingg, W.; Hopkins, S.; Gayet-Ageron, A.; Holmes, A.; Sharland, M.; Suetens, C.; Almeida, M.; Asembergiene, J.; Borg, M.A.; Budimir, A. Health-care-associated infections in neonates, children, and adolescents: An analysis of paediatric data from the European Centre for Disease Prevention and Control point-prevalence survey. Lancet Infect. Dis. 2017, 17, 381–389. [Google Scholar] [CrossRef]
- Peters, M.D.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Creel, B. Bacterial Load in Virtual Reality Headsets. In Proceedings of the 26th ACM Symposium on Virtual Reality Software and Technology, Virtual, 1–4 November 2020. [Google Scholar]
- Roberts, S.C.; Havill, N.L.; Flores, R.M.; Hendrix II, C.A.; Williams, M.J.; Feinn, R.S.; Choi, S.J.; Martinello, R.A.; Marks, A.M.; Murray, T.S. Disinfection of Virtual Reality Devices in Health Care Settings: In Vitro Assessment and Survey Study. J. Med. Internet Res. 2022, 24, e42332. [Google Scholar] [CrossRef]
- Daniel, V.; Jones, R.; Dhillon, R.; Duckers, J.; Rattenbury, S. EPS9. 09 Pilot study to evaluate the use of dry chlorine dioxide gas for sterilisation of virtual reality headsets. J. Cyst. Fibros. 2023, 22, S63. [Google Scholar] [CrossRef]
- Høeg, E.R.; Lange, B. A Survey of Virtual Reality Hygiene Practices. In Proceedings of the International Conference on Disability, Virtual Reality & Associated Technologies, Ponta Delgada, Portugal, 6–8 September 2022. [Google Scholar]
- Moore, N.; Dempsey, K.; Hockey, P.; Jain, S.; Poronnik, P.; Shaban, R.Z.; Ahmadpour, N. Innovation during a pandemic: Developing a guideline for infection prevention and control to support education through virtual reality. Front. Digit. Health 2021, 3, 628452. [Google Scholar] [CrossRef]
- International Standards Organisation. Augmented and Virtual Reality Safety–Guidance on Safe Immersion, Set Up and Usage; International Standards Organisation: Geneva, Switzerland, 2024; pp. 1–27. [Google Scholar]
- Goldsworthy, A.; Chawla, J.; Birt, J.; Baumann, O.; Gough, S. Use of extended reality in sleep health, medicine, and research: A scoping review. Sleep 2023, 46, zsad201. [Google Scholar] [CrossRef]
- McDonnell, G.; Burke, P. Disinfection: Is it time to reconsider Spaulding? J. Hosp. Infect. 2011, 78, 163–170. [Google Scholar] [CrossRef]
- Rutala, W.A.; Weber, D.J. Disinfection and sterilization in health care facilities: An overview and current issues. Infect. Dis. Clin. 2016, 30, 609–637. [Google Scholar] [CrossRef]
- Burt, M. Theme Parks Employ Virtual Reality as Part of the Entertainment Mix—But What Do Audiences Think? 2023. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4475874 (accessed on 10 April 2024).
- Azari, A.A.; Arabi, A. Conjunctivitis: A systematic review. J. Ophthalmic Vis. Res. 2020, 15, 372. [Google Scholar] [CrossRef]
- Gallandat, K.; Kolus, R.C.; Julian, T.R.; Lantagne, D.S. A systematic review of chlorine-based surface disinfection efficacy to inform recommendations for low-resource outbreak settings. Am. J. Infect. Control 2021, 49, 90–103. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).