
Susceptibility to Clotrimazole of Candida spp. Isolated from the Genitourinary System—A Single Center Study

 ,
,
Abstract
:1. Introduction
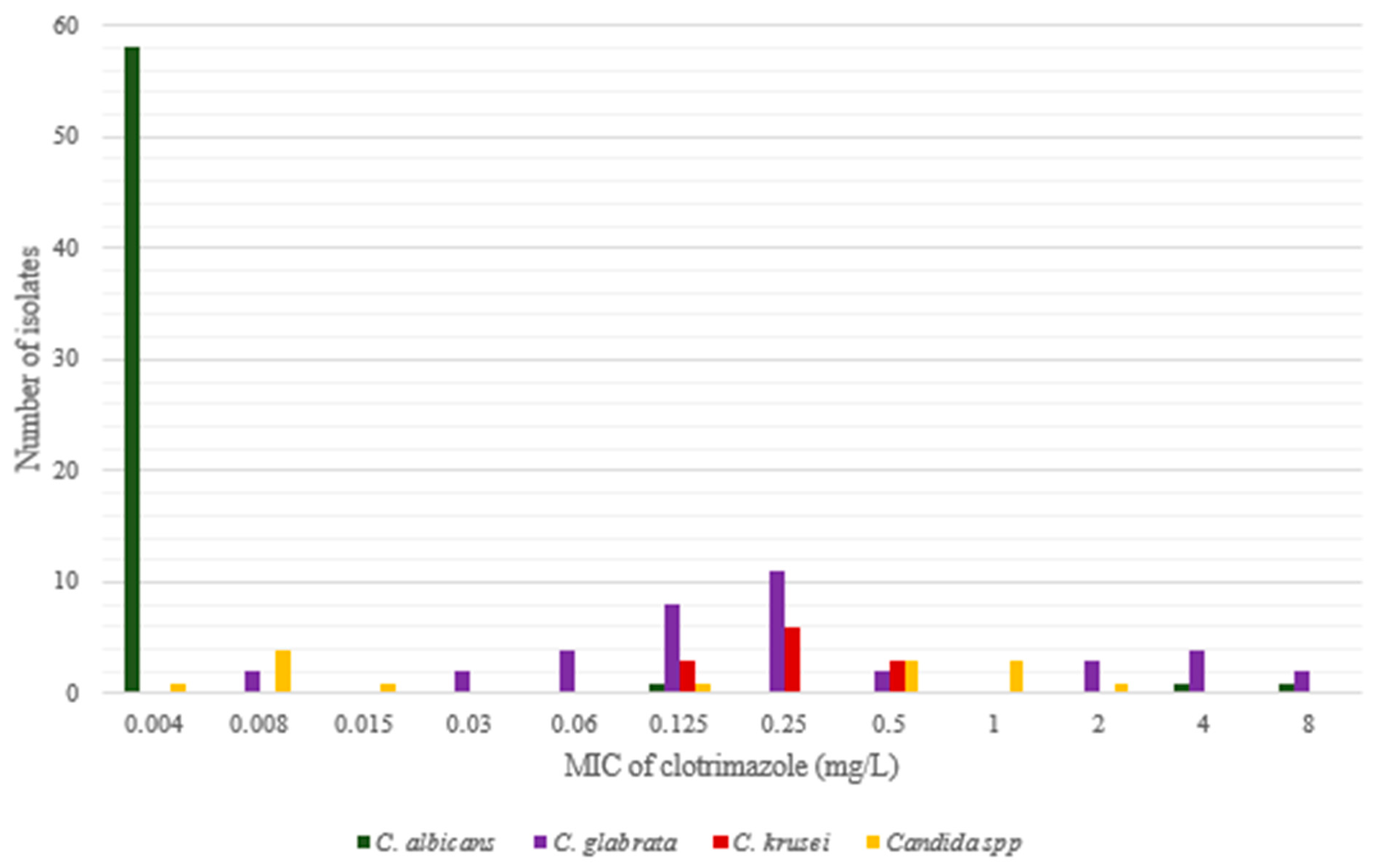
2. Results
Susceptibility to Clotrimazole and Fluconazole

{kind=link}
| Species (Number of Isolates) | Number of Isolates at MIC [mg/L] | MIC50 | MIC90 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| <0.008 | 0.008 | 0.015 | 0.03 | 0.06 | 0.125 | 0.25 | 0.5 | 1 | 2 | 4 | 8 | |||
| C. albicans (61) | 58 | 1 | 1 | 1 | <0.008 | <0.008 | ||||||||
| C. albicans (420); Richter et al. [5] | 9 | 92 | 252 | 65 | 2 | 0.03 | 0.06 | |||||||
| C. glabrata (38) | 2 | 2 | 4 | 8 | 11 | 2 | 3 | 4 | 2 | 0.25 | 4 | |||
| C. glabrata (250) Richter et al. [5], Costa et al. [6]; | 1 | 7 | 15 | 21 | 21 | 53 | 45 | 36 | 21 | |||||
| C. krusei (12) | 3 | 6 | 3 | 0.25 | 0.5 | |||||||||
| C. krusei (12) Richter et al. [5] | 2 | 5 | 4 | 1 | 0.25 | 0.5 | ||||||||
| C. inconspicua (3) | 1 | 2 | ||||||||||||
| C. guilliermondii (3) | 2 | 1 | ||||||||||||
| C. parapsilosis (2) | 1 | 1 | ||||||||||||
| C. tropicalis (2) | 1 | 1 | ||||||||||||
| C. dubliniensis (1) | 1 | |||||||||||||
| C. lusitaniae (1) | 1 | |||||||||||||
| C. pararugosa (1) | 1 | |||||||||||||
| C. melibiosica (1) | 1 | |||||||||||||
| non-albicans. (64) | 1 | 6 | 1 | 2 | 4 | 12 | 17 | 8 | 3 | 4 | 4 | 2 | 0.25 | 2 |
| Total (125) | 59 | 6 | 1 | 2 | 4 | 13 | 17 | 8 | 3 | 4 | 5 | 3 | 0.008 | 1 |
3. Discussion
4. Materials and Methods
4.1. Strains
4.2. Culture and Re-Identification of the Strains
4.3. Determination of Susceptibility to Antifungals/Clotrimazole
4.4. Determination of MFC, the Minimal Fungicidal Concentration of Clotrimazole
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yapar, N. Epidemiology and risk factors for invasive candidiasis. Ther. Clin. Risk Manag. 2014, 10, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Sardi, J.; Scorzoni, L.; Bernardi, T.; Fusco-Almeida, A.M.; Mendes Giannini, M. Candida species: Current epidemiology, pathogenicity, biofilm formation, natural antifungal products and new therapeutic options. J. Med. Microbiol. 2013, 62, 10–24. [Google Scholar] [CrossRef]
- Gonçalves, B.; Ferreira, C.; Alves, C.T.; Henriques, M.; Azeredo, J.; Silva, S. Vulvovaginal candidiasis: Epidemiology, microbiology and risk factors. Crit. Rev. Microbiol. 2016, 42, 905–927. [Google Scholar] [CrossRef] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Overview of Antifungal ECOFFs and Clinical Breakpoints for Yeasts, Moulds and Dermatophytes Using the EUCAST E.Def 7.3, E.Def 9.3 and E.Def 11.0 Procedures. Version 2. 2020. Available online: http://www.eucast.org. (accessed on 19 October 2020).
- Richter, S.S.; Galask, R.P.; Messer, S.A.; Hollis, R.J.; Diekema, D.J.; Pfaller, M.A. Antifungal susceptibilities of Candida species causing vulvovaginitis and epidemiology of recurrent cases. J. Clin. Microbiol. 2005, 43, 2155–2162. [Google Scholar] [CrossRef] [Green Version]
- Costa, C.; Ribeiro, J.; Miranda, I.M.; Silva-Dias, A.; Cavalheiro, M.; Costa-de-Oliveira, S.; Rodrigues, A.G.; Teixeira, M.C. Clotrimazole drug resistance in Candida glabrata clinical isolates correlates with increased expression of the drug: H (+) antiporters CgAqr1, CgTpo1_1, CgTpo3, and CgQdr2. Front. Microbiol. 2016, 7, 526. [Google Scholar] [CrossRef]
- Shi, Y.; Zhu, Y.; Fan, S.; Liu, X.; Liang, Y.; Shan, Y. Molecular identification and antifungal susceptibility profile of yeast from vulvovaginal candidiasis. BMC Infect. Dis. 2020, 20, 287. [Google Scholar] [CrossRef] [PubMed]
- Theill, L.; Dudiuk, C.; Morano, S.; Gamarra, S.; Nardin, M.E.; Méndez, E.; Garcia-Effron, G. Prevalence and antifungal susceptibility of Candida albicans and its related species Candida dubliniensis and Candida africana isolated from vulvovaginal samples in a hospital of Argentina. Rev. Argent. Microbiol. 2016, 48, 43–49. [Google Scholar]
- Zhou, X.; Li, T.; Fan, S.; Zhu, Y.; Liu, X.; Guo, X.; Liang, Y. The efficacy and safety of clotrimazole vaginal tablet vs. oral fluconazole in treating severe vulvovaginal candidiasis. Mycoses 2016, 59, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Diaz, M.C.; Camponovo, R.; Araya, I.; Cerda, A.; Santander, M.P.; Carrillo-Muñoz, A.J. Identificación y sensibilidad antifúngica in vitro de Candida spp. de origen vaginal a fluconazol, clotrimazol y nistatina [Identification and in vitro antifungal susceptibility of vaginal Candida spp. isolates to fluconazole, clotrimazole and nystatin]. Rev. Esp. Quimioter. 2016, 29, 151–154. [Google Scholar]
- Choukri, F.; Benderdouche, M.; Sednaoui, P. In vitro susceptibility profile of 200 recent clinical isolates of Candida spp. to topical antifungal treatments of vulvovaginal candidiasis, the imidazoles and nystatin agents. J. Mycol. Med. 2014, 24, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, R.; Peter, J.; Antin, C.; Gonzalez, C.; Wood, L.; Walsh, T.J. Emergence of resistance of Candida albicans to clotrimazole in human immunodeficiency virus-infected children: In vitro and clinical correlations. J. Clin. Microbiol. 2000, 38, 1563–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hacioglu, M.; Guzel, C.B.; Savage, P.B.; Tan, A. Antifungal susceptibilities, in vitro production of virulence factors and activities of ceragenins against Candida spp. isolated from vulvovaginal candidiasis. Med. Mycol. 2019, 57, 291–299. [Google Scholar] [CrossRef]
- Nelson, M.; Wanjiru, W.; Margaret, M. Identification and susceptibility profile of vaginal Candida species to antifungal agents among pregnant women attending the antenatal clinic of Thika District Hospital, Kenya. Open J. Med. Microbiol. 2013, 3, 239–247. [Google Scholar] [CrossRef] [Green Version]
- Mesquida, A.; Vicente, T.; Reigadas, E.; Palomo, M.; Sánchez-Carrillo, C.; Muñoz, P.; Guinea, J.; Escribano, P. In vitro activity of ibrexafungerp and comparators against Candida albicans genotypes from vaginal samples and blood cultures. Clin. Microbiol. Infect. 2021, 27, e5–e915. [Google Scholar] [CrossRef]
- Rezaei-Matehkolaei, A.; Shafiei, S.; Zarei-Mahmoudabadi, A. Isolation, molecular identification, and antifungal susceptibility profiles of vaginal isolates of Candida species. Iran. J. Microbiol. 2016, 8, 410–417. [Google Scholar]
- Kiakojuri, K.; Mahdavi Omran, S.; Roodgari, S.; Taghizadeh Armaki, M.; Hedayati, M.T.; Shokohi, T.; Haghani, I.; Javidnia, J.; Kermani, F.; Badali, H.; et al. Molecular identification and antifungal susceptibility of yeasts and molds isolated from patients with otomycosis. Mycopathologia 2021, 186, 245–257. [Google Scholar] [CrossRef] [PubMed]
- Farahyar, S.; Izadi, S.; Razmjou, E.; Falahati, M.; Roudbary, M.; Ashrafi-Khozani, M.; Ansari, S.; Fattahi, A.; Ghahri-Mobaser, Z.; Rahimi, M. Low prevalence of antifungal resistant Candida africana, in the C. albicans complex causing vulvovaginal candidiasis. Heliyon 2020, 6, e03619. [Google Scholar] [CrossRef]
- Lotfalikhani, A.; Khosravi, Y.; Sabet, N.S.; Na, S.L.; Ng, K.P.; Tay, S.T. Genetic diversity, antifungal susceptibility and enzymatic characterisation of Malaysian clinical isolates of Candida glabrata. Trop. Biomed. 2018, 35, 1123–1130. [Google Scholar] [PubMed]
- Singh, S.; Sobel, J.D.; Bhargava, P.; Boikov, D.; Vazquez, J.A. Vaginitis due to Candida krusei: Epidemiology, clinical aspects, and therapy. Clin. Infect. Dis. 2002, 35, 1066–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendling, W.; Atef El Shazly, M.; Zhang, L. Clotrimazole for vulvovaginal candidosis: More than 45 years of clinical experience. Pharmaceuticals 2020, 13, 274. [Google Scholar] [CrossRef]
- Marchaim, D.; Lemanek, L.; Bheemreddy, S.; Kaye, K.S.; Sobel, J.D. Fluconazole-resistant Candida albicans vulvovaginitis. Obstet. Gynecol. 2012, 120, 1407–1414. [Google Scholar] [CrossRef] [Green Version]
- Khadka, S.; Sherchand, J.B.; Pokhrel, B.M.; Parajuli, K.; Mishra, S.K.; Sharma, S.; Shah, N.; Kattel, H.P.; Dhital, S.; Khatiwada, S.; et al. Isolation, speciation and antifungal susceptibility testing of Candida isolates from various clinical specimens at a tertiary care hospital, Nepal. BMC Res. Notes 2017, 10, 218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cross, E.W.; Park, S.; Perlin, D.S. Cross-resistance of clinical isolates of Candida albicans and Candida glabrata to over-the-counter azoles used in the treatment of vaginitis. Microb. Drug Resist. 2000, 6, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Makanjuola, O.; Bongomin, F.; Fayemiwo, S.A. An update on the roles of non-albicans Candida species in vulvovaginitis. J. Fungi 2018, 4, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimling, B.; Karolewicz, B.; Nawrot, U.; Włodarczyk, K.; Górniak, A. Physicochemical and antifungal properties of clotrimazole in combination with high-molecular weight chitosan as a multifunctional excipient. Mar. Drugs 2020, 18, 591. [Google Scholar] [CrossRef]
- Spitzer, M.; Wiederhold, N.P. Reduced antifungal susceptibility of vulvovaginal Candida species at normal vaginal pH levels: Clinical implications. J. Low. Genit. Tract Dis. 2018, 22, 152–158. [Google Scholar] [CrossRef]
- Tiboni, M.; Campana, R.; Frangipani, E.; Casettari, L. 3D printed clotrimazole intravaginal ring for the treatment of recurrent vaginal candidiasis. Int. J. Pharm. 2021, 596, 120290. [Google Scholar] [CrossRef]
- Catenacci, L.; Marrubini, G.; Sorrenti, M.; Rossi, S.; Sandri, G.; Ferrari, F.; Fagnani, V.; Valentino, C.; Bonferoni, M.C. Design of experiments-assisted development of clotrimazole-loaded ionic polymeric micelles based on hyaluronic acid. Nanomaterials 2020, 10, 635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arendrup, M.C.; Meletiadis, J.; Mouton, J.W.; the Subcommittee on Antifungal Susceptibility Testing (AFST) of the ESCMID European Committee for Antimicrobial Susceptibility Testing (EUCAST). Method for the Determination of Broth Dilution Minimum Inhibitory Concentrations of Antifungal Agents for Yeasts. Eucast Definitive Document E.Def. 7.3.1 April 2020. Available online: https://www.eucast.org/ (accessed on 19 October 2020).

| No. | Strain Number | Species | MIC [mg/L] | |
|---|---|---|---|---|
| Clotrimazole | Fluconazole | |||
| 1. | 488 | C. albicans | 0.125 | 4 (I) |
| 2. | 1050 | C. albicans | 4 | 64 (R) |
| 3. | 1342 | C. albicans | 8 | >64 (R) |
| 4. | 239 | C. glabrata | 2 | 4 (I) |
| 5. | 2445 | C. glabrata | 2 | 2 (I) |
| 6. | 984 | C. glabrata | 4 | 4 (I) |
| 7. | 136 | C. glabrata | 4 | 32 (R) |
| 8. | 2586 | C. glabrata | 4 | 64 (R) |
| 9. | 2922 | C. glabrata | 4 | >64 (R) |
| 10. | 196 | C. glabrata | 8 | 64 (R) |
| 11. | 772 | C. glabrata | 8 | 64 (R) |
| 12. | 630 | C. guillermondii | 2 | 4 * |
| 13. | 678 | C. guillermondii | 1 | 4 * |
| 14. | 2933 | C. guillermondii | 1 | 4 * |
| 15. | 2408 | C. tropicalis | 1 | 4 (I) |
| Reference | Method | Sample | Number of Strains Tested | Clotrimazole MIC mg/L | % of Non-WT | |||
|---|---|---|---|---|---|---|---|---|
| Range | GM | MIC50 | MIC90 | |||||
| C. albicans | ||||||||
| Shi et al., 2020 [7] | CLSI, M27-A3 | Vaginal | 1272 | 0.015–32 | 0.05 | - | 0.25 | ND |
| Rhichter et al., 2005 [5] | CLSI, M27A | Vaginal | 420 | 0.008–0.125 | 0.03 | 0.06 | 0 | |
| Theill et al., 2016 [8] | CLSI, M27-A3 | Vaginal | 282 | 0.015–0.12 | 0.02 | 0.03 | 0 | |
| Zhou et al., 2016 [9] | CLSI, M27A | Vaginal | 216 | 0.03–4 | 0.046 | <0.03 | 0.25 | ND |
| Diaz et al., 2016 [10] | CLSI, M27-A3 | Vaginal | 126 | 0.03–0.5 | 0.03 | 0.06 | 0 | |
| Choukri et al., 2014 [11] | CLSI, M27-A3 | Vaginal | 113 | 0.015–4 | - | 0.03 | 0.06 | ND |
| Pelletier et al., 2000 [12] | CLSI, M27A | Oral (HIV+) | 87 | <0.06–8 | - | <0.06 | 0.5 | 15 (17%) |
| Hacioglu et al., 2019 [13] | CLSI, M27-A3 | Vaginal | 84 | 0.01–2 | - | 0.007 | 0.25 | ND |
| Nelson et al., 2013 [14] | CLSI, M27 A2 | Vaginal | 60 | 0.03–16 | - | 0.25 | 16 | 36.7% |
| Mesquida et al., 2021 [15] | EUCAST | Vaginal | 72 | 0.004–0.25 | 0.006 | 0.008 | 0.06 | 0 |
| Rezaei-Matehkolaei et al., 2016 [16] | microdilution home method | Vaginal | 30 | 0.25–1 | 0.29 | 0.25 | 0.5 | 5 (16.6%) |
| Kiakojuri et al., 2021 [17] | CLSI | Auricular | 16 | 1–16 | 2.484 | 1.5 | 16 | ND |
| C. dubliniensis | ||||||||
| Theill et al., 2016 [8] | CLSI M27-A3 | Vaginal | 4 | 0.015–0.03 | ND | |||
| Shi et al., 2020 [7] | CLSI, M27-A3 | Vaginal | 1 | 0.015 | ND | |||
| C. africana | ||||||||
| Shi et al., 2020 [7] | CLSI, M27-A3 | Vaginal | 49 | 0.15–4 | - | - | 0.06 | ND |
| Farahyar et al., 2020 [18] | CLSI, M27-S | Vaginal | 3 | 0.06–16 | - | - | 1 | |
| Theill et al., 2016 [8] | CLSI M27-A3 | Vaginal | 1 | 0.03 | - | - | ND | |
| C. glabrata | ||||||||
| Shi et al., 2020 [7] | CLSI, M27-A3 | Vaginal | 267 | 0.015–16 | 0.2 | - | 1 | ND |
| Costa et al., 2016 [6] | CLSI, M27-S4 /EUCAST | Varia | 138 | 0.03–8 | - | 1 | 8 | 89 (64%) |
| Rhichter et al., 2005 [5] | CLSI, M27A | Vaginal | 112 | 0.06–8 | - | 1 | 4 | ND |
| Choukri et al., 2014 [11] | CLSI, M27-A3 | Vaginal | 54 | 0.25–8 | - | 2 | 4 | ND |
| Lotfalikhani et al., 2018 [19] | CLSI, M27 | Vaginal, blood | 41 | 0.1–4 | - | 0.5 | 4 | 15 (30%) |
| Nelson et al., 2013 [14] | CLSI, M27 A2 | Vaginal | 28 | 0.03–16 | - | 0.125 | 0.25 | 10.7% |
| Diaz et al., 2016 [10] | CLSI, M27-A3 | Vaginal | 16 | 0.03–1 | 0.25 | 1 | ND | |
| Zhou et al., 2016 [9] | CLSI, M27A | Vaginal | 13 | 0.03–2 | 0.2466 | 0.25 | 1 | ND |
| Hacioglu et al., 2019 [13] | CLSI, M27-A3 | Vaginal | 9 | 0.25–2 | 0.5 | 2 | ND | |
| Rezaei-Matehkolaei et al., 2016 [16] | microdilution home method | Vaginal | 3 | 0.25 | 0.06 | 0.125 | 0 | |
| C. nivariensis | ||||||||
| Shi et al., 2020 [7] | CLSI, M27-A3 | Vaginal | 9 | 0.03–0.5 | 0 | |||
| C. bracariensis | ||||||||
| Shi et al., 2020 [7] | CLSI, M27-A3 | Vaginal | 2 | 0.03–0.5 | 0 | |||
| C. krusei | ||||||||
| Shi et al., 2020 [7] | CLSI, M27-A3 | Vaginal | 54 | 0.015–0.5 | 0.08 | - | 0.5 | 0% |
| Singh et al., 2002 [20] | CLSI, M27-A | Vaginal | 26 | 0.03–0.5 | - | 0.125 | 0.25 | 0% |
| Rhichter et al., 2005 [7] | CLSI, M27A | Vaginal | 12 | 0.125–1 | - | 0.25 | 0.5 | 1 (3.5%) |
| Choukri et al., 2014 [11] | CLSI, M27-A3 | Vaginal | 11 | 0.25–0.5 | 0.5 | 0.5 | 0% | |
| Nelson et al., 2013 [14] | CLSI, M27-A2 | Vaginal | 2 | 1–4 | 2 (100%) | |||
| Hacioglu et al., 2019 [13] | CLSI, M27-A3 | Vaginal | 1 | 0.5 | 0% | |||
| C. parapsilosis | ||||||||
| Shi et al., 2020 [6] | CLSI, M27-A3 | Vaginal | 76 | 0.015–1 | 0.04 | - | 0.06 | ND |
| Rhichter et al., 2005 [7] | CLSI, M27A | Vaginal | 30 | 0.03–0.5 | - | 0.06 | 0.25 | 0% |
| Choukri et al., 2014 [11] | CLSI, M27-A3 | Vaginal | 11 | 0.03–0.5 | 0.12 | 0.12 | 0% | |
| Kiakojuri et al., 2021 [17] | CLSI | auricular | 12 | 1–>16 | 3.364 | 2 | 16 | 12 (100%) |
| Diaz et al., 2016 [10] | CLSI, M27-A3 | Vaginal | 2 | 0.03 | 0% | |||
| Nelson et al., 2013 [14] | CLSI, M27 A2 | Vaginal | 1 | 0.125 | 0% | |||
| C. metapsilosis | ||||||||
| Shi et al., 2020 [6] | CLSI, M27-A3 | Vaginal | 20 | 0.03–0.25 | 0.04 | - | 0.06 | 0% |
| C. orthopsilosis | ||||||||
| Kiakojuri et al., 2021 [17] | CLSI | Auricular | 18 | 0.25–>16 | 1.782 | 1 | 16 | |
| Shi et al., 2020 [6] | CLSI, M27-A3 | Vaginal | 6 | 0.03–1 | 1 | |||
| C. tropicalis | ||||||||
| Shi et al., 2020 [6] | CLSI, M27-A3 | Vaginal | 61 | 0.015–0.25 | 0.05 | - | 0.05 | 0 |
| Choukri et al., 2014 [11] | CLSI, M27-A3 | Vaginal | 11 | 0.12–0.25 | - | 0.12 | 0.25 | 0 |
| Rhichter et al., 2005 [7] | CLSI, M27A | Vaginal | 8 | 0.03–0.25 | - | 0 | ||
| Nelson et al., 2013 [14] | CLSI, M27 A2 | Vaginal | 3 | 0.125–2 | 1 (33.3%) | |||
| Hacioglu et al., 2019 [13] | CLSI, M27-A3 | Vaginal | 2 | 0.007–0.015 | 0 | |||
| Kiakojuri et al., 2021 [17] | CLSI | Auricular | 1 | 4 | 1 (100%) | |||
| Diaz et al., 2016 [10] | CLSI, M27-A3 | Vaginal | 1 | 1 | 1(100%) | |||
| C. kefyr | ||||||||
| Hacioglu et al., 2019 [13] | CLSI, M27-A3 | Vaginal | 2 | 0.007–0.5 | ||||
| Rezaei-Matehkolaei et al., 2016 [16] | microdilution home method | Vaginal | 1 | 0.25 | ||||
| C. auris | ||||||||
| Kiakojuri et al., 2021 [17] | CLSI | auricular | 1 | 8 | ||||
| C. lusitniae | ||||||||
| Rhichter et al., 2005 [7] | CLSI, M27A | Vaginal | 1 | 0.06 | ||||
| Hacioglu et al., 2019 [13] | CLSI, M27-A3 | Vaginal | 1 | 0.5 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frej-Mądrzak, M.; Golec, S.; Włodarczyk, K.; Choroszy-Król, I.; Nawrot, U. Susceptibility to Clotrimazole of Candida spp. Isolated from the Genitourinary System—A Single Center Study. Pathogens 2021, 10, 1142. https://doi.org/10.3390/pathogens10091142
Frej-Mądrzak M, Golec S, Włodarczyk K, Choroszy-Król I, Nawrot U. Susceptibility to Clotrimazole of Candida spp. Isolated from the Genitourinary System—A Single Center Study. Pathogens. 2021; 10(9):1142. https://doi.org/10.3390/pathogens10091142
Chicago/Turabian StyleFrej-Mądrzak, Magdalena, Sabina Golec, Katarzyna Włodarczyk, Irena Choroszy-Król, and Urszula Nawrot. 2021. "Susceptibility to Clotrimazole of Candida spp. Isolated from the Genitourinary System—A Single Center Study" Pathogens 10, no. 9: 1142. https://doi.org/10.3390/pathogens10091142
APA StyleFrej-Mądrzak, M., Golec, S., Włodarczyk, K., Choroszy-Król, I., & Nawrot, U. (2021). Susceptibility to Clotrimazole of Candida spp. Isolated from the Genitourinary System—A Single Center Study. Pathogens, 10(9), 1142. https://doi.org/10.3390/pathogens10091142