
Leaving No One Behind: A Photovoice Case Study on Vulnerability and Wellbeing of Children Heading Households in Two Informal Settlements in Nairobi

 ,
,
Abstract
1. Introduction
1.1. Urban Informality and Vulnerability
1.2. Wellbeing as a Development Concept
1.3. Wellbeing and Vulnerabilities of Child-Headed Households
2. Materials and Methods
Study Participants
3. Results
3.1. Participant Characteristics
3.2. Material Aspects of Wellbeing
“Like at the bridge. When the bridge was removed there were some wires that were there on the wall. A woman went to pass, she touched a wire and she was electrocuted. So people are even afraid to pass through that road because of the wires…They [electricity gangs] hook electricity on your roof. So, when you touch the roof, you are shocked [electrocuted].”(Mwangaza, 17-year-old girl, Viwandani)
“During floods, the house owner may shock [electrocute] you so that you don’t touch his roof while crossing the floods. That is the electricity challenge here. Someone puts current so that you don’t touch his roof while you cross. They think you will lean on it [the roof] and bend it. So they put a current there.”(Mwangaza, 17-year-old girl, Viwandani)
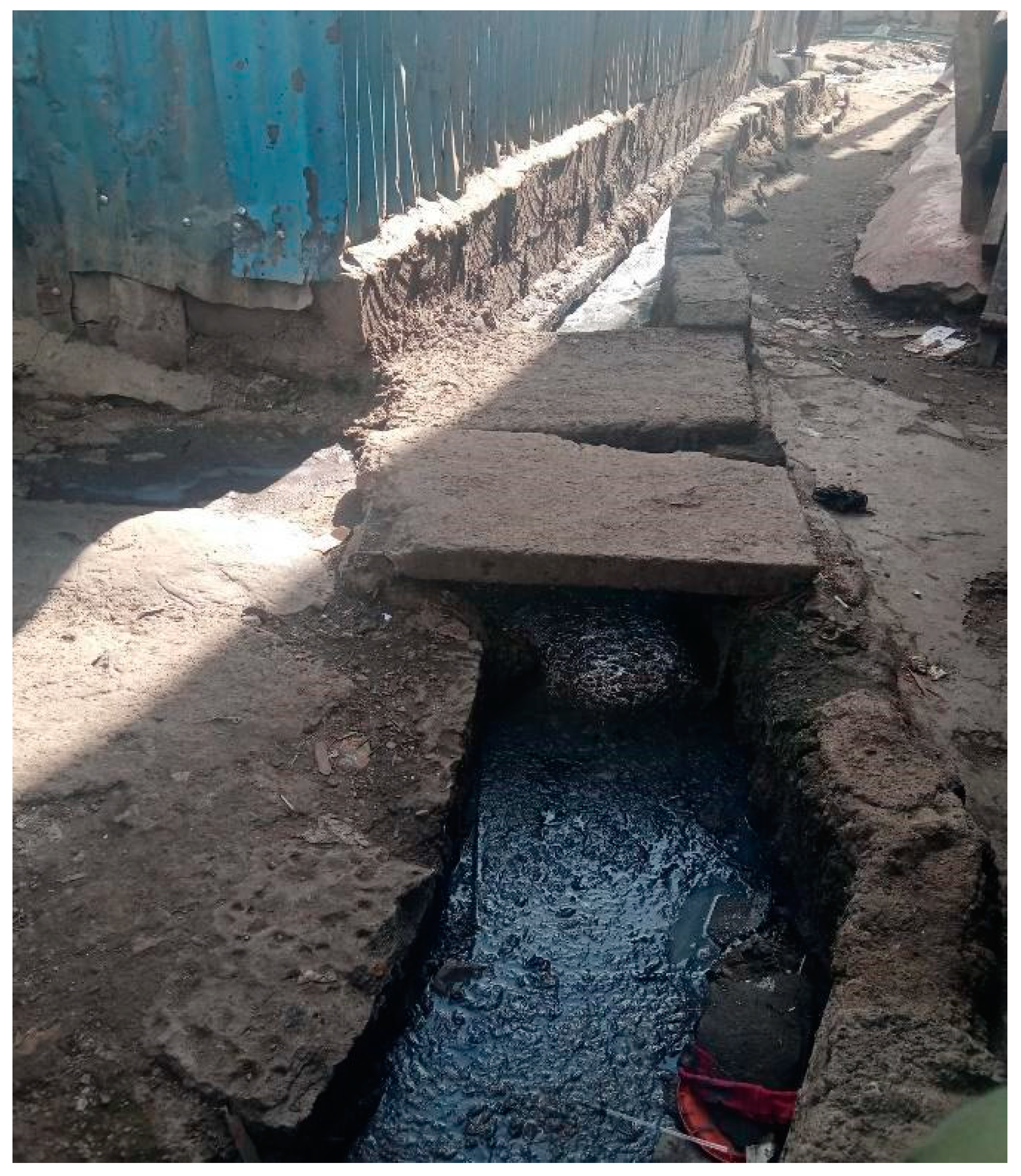
“Those who are living in other areas like for example in Civo (nearby middle-class estate). They usually have garbage collection but here in Korogocho there is no garbage collection, you just throw the garbage into the river. Others even do flying toilets…. Someone goes for a long call (defecates) then puts the human waste in a plastic bag and throws it away. Sometimes it can even land into your food and they won’t be bothered. For them, wherever it goes, let it go it’s okay, but in the estates you cannot find such things.”(Violet, 17-year-old girl, Korogocho)
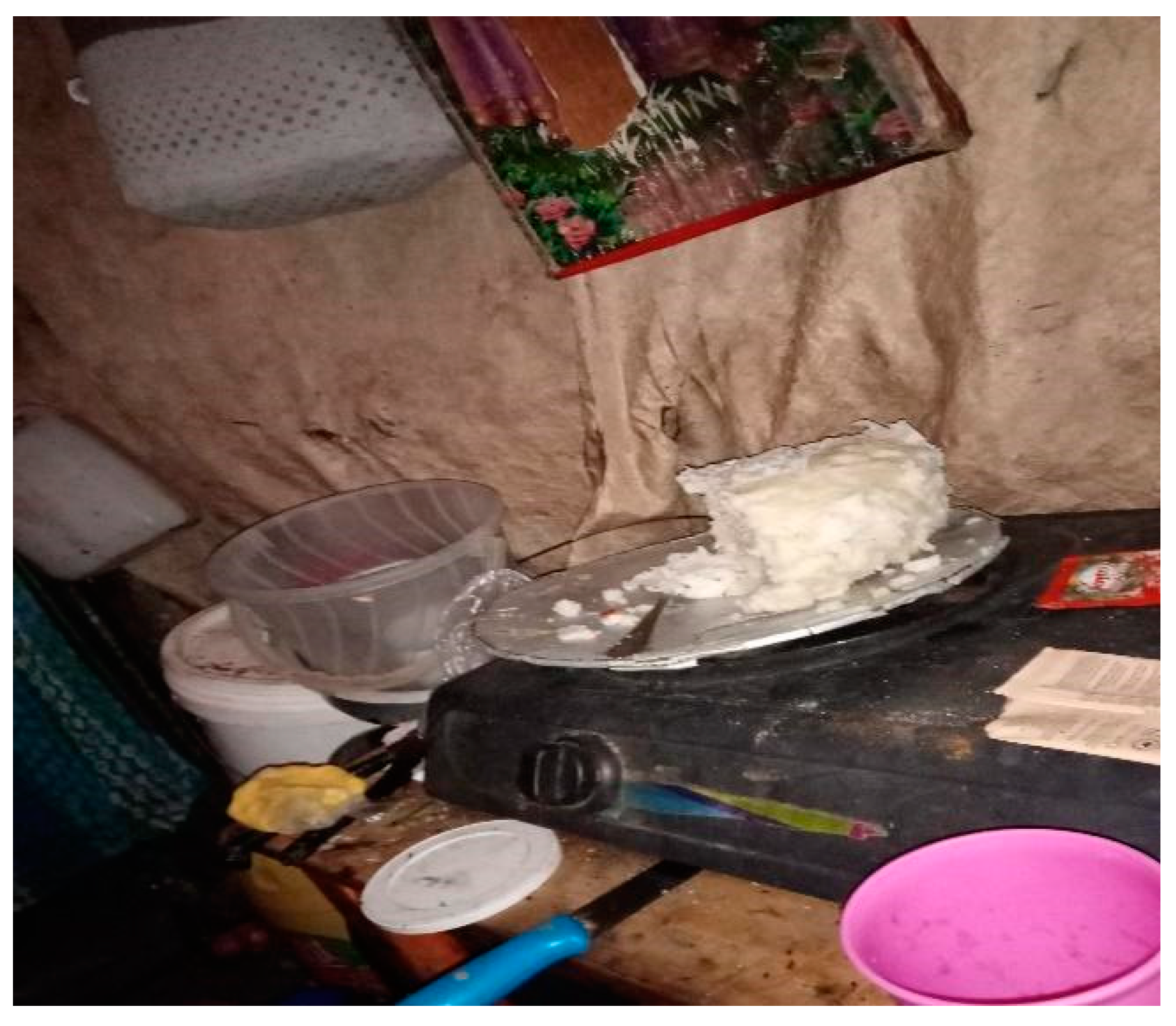
“I get laundry work to do…. There are sometimes I don’t get [any] at all and sometimes I get—it depends. … When I don’t get, we sleep like that… We sleep hungry.”(Paula, 17-year-old girl, Viwandani)
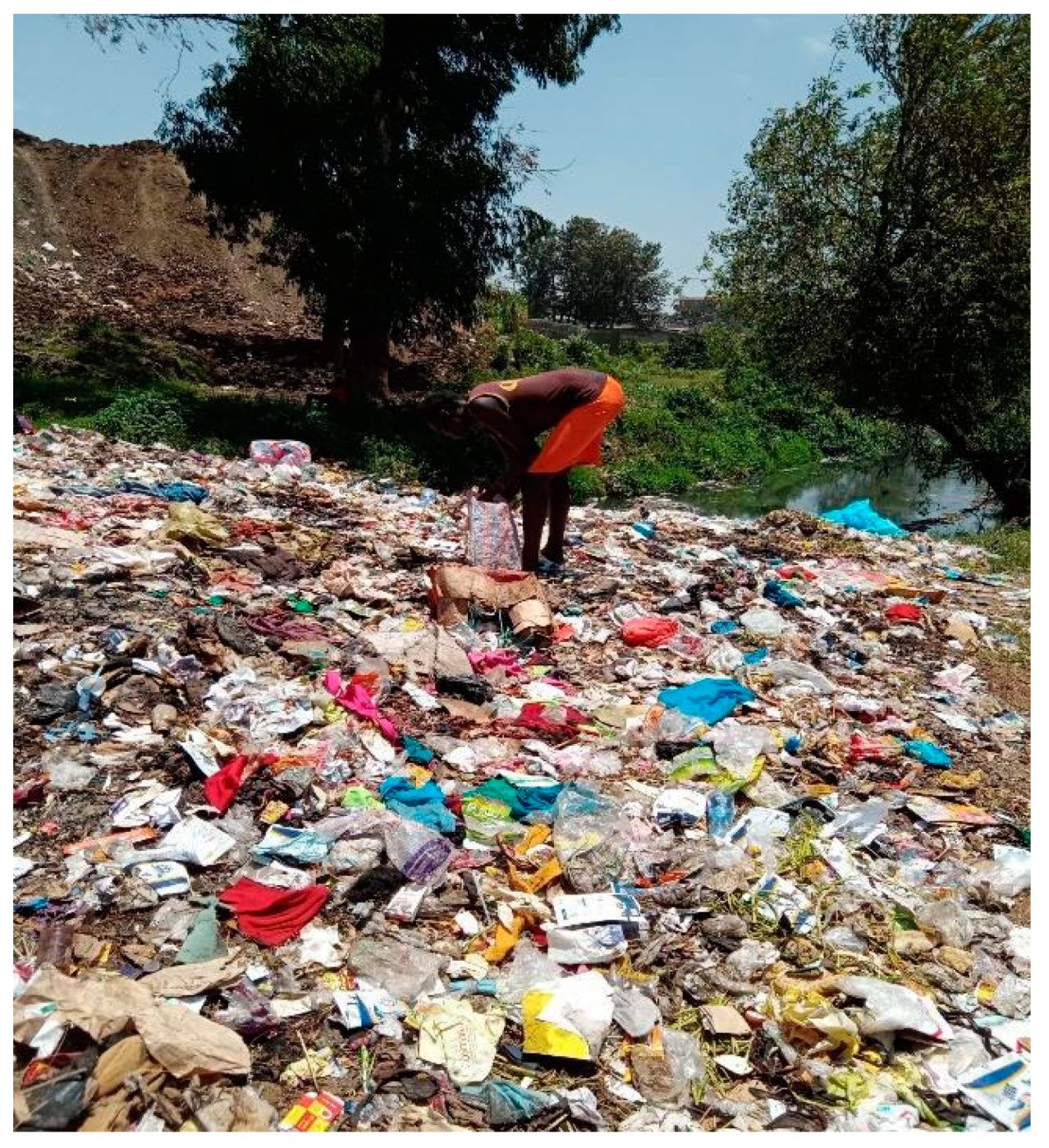
“I have been living as a street child, getting my earning from the garbage scavenging. Whatever I get, I go and sell and get money to go and buy food or sometimes [I] ask for some work from those who brew alcohol. Those who brew alcohol tell us to go to Boma and bring to them those things used to brew alcohol and when there is water shortage we go and fetch water for them… such things.”(Job, 17-year-old boy, Korogocho)
“With my kind of work and having to collect garbage and over-ripe bananas, I am bound to get dirty. My peers (living in same settlement) tell me that I resemble a Chokora (homeless street child). They make fun that I eat food from the garbage river. They go to the extent of saying that I might infect them with COVID-19 just by virtue of being dirty.”(Robert, 17-year-old boy, Korogocho)
“Last year were it not for COVID, I was struggling…. COVID started in March. Before COVID started I never used to go to school. So to some extent COVID has helped me because all those months I could have missed school since there was nobody at home who could have been left to take care of mum. And my sister has to go to work so that she can get the money for my mother’s medication.”(Violet, 17-year-old girl, Korogocho)
3.3. Social Relational Aspects of Wellbeing
“As I was doing casual jobs of washing clothes and utensils, there was a boy who wooed me, impregnated me. We lived together for like 6 months after I delivered. But he started beating me. I got pregnant, the second time. The guy was still abusive, he threated to stab me and kill the baby. I have even been strangled using electricity wires.”(Sandra, 16-year-old girl, Korogocho)
“We need to be given a chance to speak out. You find someone like me needs to be given a chance for us to air grievances or they take us to go and do a course or they offer us jobs.”(Shadrack, 17-year-old boy, Viwandani)
“During that period for COVID, I heard that there was money that used to be sent but I never got to receive any money and even my name was never registered anywhere. I just used to struggle on my own—I go to hassle (slang for work) and then come back I used to hear that people were being sent money …KES 7000 (Approximately USD 70) from the Chief’s Office…but I never received any… I don’t know why I didn’t get it.”(Meshack, 17-year-old boy, Viwandani)
- R:
- I feel very bad because sometimes the teacher does not care about our situation and thinks one is strong just by their outward looks, but little does he know how much suffering there is on the inside. He sometimes uses harsh and spiteful words while sending us away. He once said, ‘Go and take your mother to town and beg for money’…this is something that we do not want to do. He tries to pressure us into it as long as he gets something to fill his pockets.
- I:
- When you are sent away and there is still learning ongoing, how does this make you feel?
“I feel terrible because everything that will be taught in my absence will not be repeated and this affects my performance in school and my grades as well. In secondary school, the teachers do not repeat what has once been taught even for students who do not understand. To them, it is just a job that will pay them after all and they even result to using rude language when questioned. My classmates are also selfish at times and will not share notes taken in my absence. They, however, tease and insult me citing my situation and poor state. This stresses me.”
3.4. Human Aspects of Wellbeing
“[Other relatives] are there but you cannot depend on them every day like for example today you go to them and borrow. Same situation again tomorrow they will tell you to also go out and work… I know you are aware how bad the relatives usually talk so you are forced to just depend on yourself. Sometimes they can even call to form a committee but the committee is not for helping it is just for gossip. So, you are forced to just solve your problems within your house.”(Violet, CHH, 17-year-old girl, Korogocho)
“I usually wake up at 4.30 a.m. take a bath then prepare by 5.30 I make sure that even the other children have prepared and gone to school. Then I go to school and come back in the house around 6.20 or 6.30 p.m. there about. Upon arriving home I check with my sister—if there is work that she hasn’t done, I do it, then check up on my mum to see if she has had her porridge or not. After that I go to the market shop for vegetables, then come and prepare them, then cook, after which I feed my mum… I serve food to the small ones first then give to my mum. I usually go to bed at around 9.30 p.m.”(Tumaini, 17-year-old girl, Korogocho)
“Yes, it is at the market where I work. There is a place where there’s sewage belonging to Nairobi water, but it smells so bad so whenever I come to dispose the ‘’mahuti’’ (onion waste)…the stench from the sewage comes with a lot of pressure and the poison from those chemicals spoils my clothes—it also affects my chest and also there is a lot of dirt like from avocados and other garbage, but that is the same place that I try to look for something while I use my bare hands when looking for something or sweeping. It affects my clothes—for example you can see this sack that I usually use to carry the garbage is dirty and it also spoils my clothes. And also, the stench of that garbage and carrying the garbage on my back which affects my skin and makes it start peeling off.”(Robert, 17 year-old boy, Korogocho)
3.5. Subjective Perceptions of Wellbeing
“I feel bad that my friends are living comfortably while I’m suffering…When my friends call me to hang out, I cannot because most of the time, my mind is thinking of home. My friends sometimes advise and encouraged me to stop thinking about home and my family, but I cannot because I am the one who has to sustain it. Some of my peers who live with disabled parents have rejected their situations and abandoned responsibility and they even encourage me to do so but I cannot because even though my mother is blind, I still value her advice and respect her. This does not go down well with my peers who make me feel isolated and alone.”(Musa, 17-year-old boy, Korogocho)
- I:
- What made you feel that these pictures are important?
- R:
- “These pictures are important because one day I believe ‘nitaomoka’ (I will become rich). So when I’ll look back at these photos, they will be reminding me of where I came from, so that is why I was taking them” (Violet, 17-year-old, Korogocho).
- R:
- When I see my friends going out, I question God about my situation. Some of them are also realising and utilising their talents while I do not get the chance to do so myself. I ask God why he made my situation to be like this.
- I:
- What is your talent?
- R:
- I have three. One is dancing another is drawing… actually, I have three, and acting.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ardrey, Jane, Kate Jehan, Kate Desmond, Caroline Kumbuyo, Kumbuyo Mortimer, and Rachel Tolhurst. 2021. ‘Cooking Is for Everyone?’: Exploring the Complexity of Gendered Dynamics in a Cookstove Intervention Study in Rural Malawi. Global Health Action 14: 2006425. [Google Scholar] [CrossRef] [PubMed]
- ARISE. 2022. Accountability and Responsiveness in Informal Settlements for Equity (Arise). Available online: https://www.ariseconsortium.org/ (accessed on 5 July 2021).
- Awino, Dorcus. 2010. Life in a Child/Adolescent Headed Household. A Qualitative Study on Everyday Life Experience of Children Living in Child/Adolescent Headed Households in Western Kenya Region. Umeå: Umeå University. [Google Scholar]
- Bates, Maya Jane, Jane Ardrey, Treza Mphwatiwa, Squire Bertel Squire, and Louis Willem Niessen. 2018. Enhanced Patient Research Participation: A Photovoice Study in Blantyre Malawi. BMJ Support Palliat Care 8: 171–74. [Google Scholar] [CrossRef] [PubMed]
- Beguy, Donatien, Patricia Elung’ata, Blessing Mberu, Clement Oduor, Marylene Wamukoya, Bonface Nganyi, and Alex Ezeh. 2015. Health & Demographic Surveillance System Profile: The Nairobi Urban Health and Demographic Surveillance System (Nuhdss). International Journal of Epidemiology 44: 462–71. [Google Scholar] [CrossRef] [PubMed]
- Bisung, Elijah, Susan Elliott, Bernard Abudho, Diana Karanja, and Corrine Schuster-Wallace. 2015. Using Photovoice As a Community Based Participatory Research Tool for Changing Water, Sanitation, and Hygiene Behaviours in Usoma, Kenya. BioMed Research International 2015: 903025. [Google Scholar] [CrossRef] [PubMed]
- Budig, Kirsten, Julia Diez, Paloma Conde, Marta Sastre, Mariano Hernán, and Manuel Franco. 2018. Photovoice and Empowerment: Evaluating the Transformative Potential of A Participatory Action Research Project. BMC Public Health 18: 432. [Google Scholar] [CrossRef] [PubMed]
- Caserta, Tehetna Alemu, Anna Maija, Pirttilä Backman, and Raija-Leena Punamäki. 2017. The Association between Psychosocial Well-Being and Living Environments: A Case of Orphans in Rwanda. Child & Family Social Work 22: 881–91. [Google Scholar]
- Catalani, Caricia, and Minkler Minkler. 2010. Photovoice: A Review of the Literature in Health and Public Health. Health Education & Behavior 37: 424–51. [Google Scholar] [CrossRef]
- Chademana, Kudzai, and Brian Van Wyk. 2021. Life in a Child-Headed Household: Exploring the Quality of Life of Orphans Living in Child-Headed Households in Zimbabwe. African Journal of AIDS Research 20: 172–80. [Google Scholar] [CrossRef]
- Chidziva, Verna, and Prem Jotham Heeralal. 2016. Circumstances Leading to the Establishment of Child-Headed Households. International Journal for Innovation Education and Research 4: 91–102. [Google Scholar] [CrossRef]
- Chloe, Ilagan, Akbari Zahra, Sethi Bharati, and Williams Allison. 2020. Use of Photovoice Methods in Research on Informal Caring: A Scoping Review of the Literature. Journal of Human Health Research 1: 1–14. [Google Scholar]
- Collins, Lisa, Matthew Ellis, Matthew Pritchard, Christopher Jenkins, Ingrid Hoeritzauer, Adam Farquhar, Orla Laverty, Vincent Murray, and Brett D. Nelson. 2016. Child-Headed Households in Rakai District, Uganda: A Mixed-Methods Study. Paediatrics and International Child Health 36: 58–63. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Daniel, Marguerite, and Angela Mathias. 2012. Challenges and coping strategies of orphaned children in Tanzania who are not adequately cared for by adults. African Journal of AIDS Research 11: 191–201. [Google Scholar] [CrossRef]
- De Vita, Maria Vittoria, Carlo Scolfaro, Bruna Santini, Antonella Lezo, Federico Gobbi, Dora Buonfrate, Elizabeth W. Kimani-Murage, T. Macharia, M. Wanjohi, J. M. Rovarini, and et al. 2019. Malnutrition, Morbidity and Infection in the Informal Settlements of Nairobi, Kenya: An Epidemiological Study. Italian Journal of Pediatrics 45: 12. [Google Scholar] [CrossRef] [PubMed]
- Donald, David, and Glynis Clacherty. 2005. Developmental Vulnerabilities and Strengths of Children Living in Child-Headed Households: A Comparison with Children in Adult-Headed Households in Equivalent Impoverished Communities. African Journal of AIDS Research 4: 21–28. [Google Scholar] [CrossRef] [PubMed]
- Elsey, Helen, D. R. Thomson, R. Y. Lin, Uden Maharjan, Siddharth Agarwal, and James Newell. 2016. Addressing Inequities in Urban Health: Do Decision-Makers Have the Data They Need? Report from the Urban Health Data Special Session at International Conference on Urban Health Dhaka 2015. Journal of Urban Health 93: 526–37. [Google Scholar] [CrossRef]
- Emina, Jacques, Donatien Beguy, Muindi Zulu Eliya, Alex Ezeh, Kanyiva Muindi, Patricia Elung’ata, John Otsola, and Y. Yé. 2011. Monitoring of Health and Demographic Outcomes in Poor Urban Settlements: Evidence from the Nairobi Urban Health and Demographic Surveillance System. Journal of Heredity 88: S200–S218. [Google Scholar] [CrossRef]
- Evans, Ruth. 2005. Social Networks, Migration, And Care in Tanzania. Journal of Children And Poverty 11: 111–29. [Google Scholar] [CrossRef]
- Ezeh, Alex, Oyinlola Oyebode, David Satterthwaite, Yen-Fu Chen, Robert Ndugwa, Jo Sartori, Blessing Mberu, G. J. Melendez-Torres, Tilahun Haregu, Samuel Watson, and et al. 2017. The History, Geography, and Sociology of Slums and the Health Problems of People Who Live in Slums. The Lancet 389: 547–58. [Google Scholar] [CrossRef]
- Fairey, Tiffany. 2018. Whose Photo? Whose Voice? Who Listens? ‘Giving’, Silencing and Listening to Voice in Participatory Visual Projects. Visual Studies 33: 111–26. [Google Scholar] [CrossRef]
- Francis-Chizororo, Monica. 2010. Growing up without Parents: Socialisation and Gender Relations in Orphaned-Child-Headed Households in Rural Zimbabwe. Journal of Southern African Studie 36: 711–27. [Google Scholar] [CrossRef]
- Gaciuki, Perpetua. 2010. Child Headed Households, The Emerging Phenomenon in Urban Informal Settlements: A Case Study of Kibera Slum Nairobi-Kenya. Master’s thesis, University of Nairobi, Nairobi, Kenya. [Google Scholar]
- Gale, Nicola, Gemma Heath, Elaine Cameron, Sabina Rashid, and Sabi Redwood. 2013. Using the Framework Method for the Analysis of Qualitative Data in Multi-Disciplinary Health Research. BMC Medical Research Methodology 13: 117. [Google Scholar] [CrossRef] [PubMed]
- Government of Kenya. 2011. Kenya National Social Protection Policy. Nairobi: Government of Kenya. [Google Scholar]
- Government of Kenya. 2017. Kenya Social Protection Sector Review. Nairobi: Government of Kenya. [Google Scholar]
- Hughes, Robort, Patrical Kitsao-Wekulo, Sunil Bhopal, Elizabeth W. Kimani-Murage, Hill Zelee, and B. R. Kirkwood. 2020. Nairobi Early Childcare in Slums (Necs) Study Protocol: A Mixed-Methods Exploration of Paid Early Childcare in Mukuru Slum, Nairobi. BMJ Paediatrics Open 4: E000822. [Google Scholar] [CrossRef] [PubMed]
- Kakulu, Stephen. 2008. Challenges Facing Orphaned and Vulnerable Children in Accessing Free Primary Education in Kenya: A Case of Embakasi Division. Nairobi: University of Nairobi. [Google Scholar]
- Kanyi, Nancy. 2019. Social and Economic Constrains Affecting the Welfare of Households Headed by Children. In Mathare Slums, Nairobi City County. Nairobi: Kenya University of Nairobi. [Google Scholar]
- Kenya National Bureau of Statistics. 2021. Kenya Integrated Household Budget Survey 2015–2016. Nairobi: KNBS. [Google Scholar]
- King, Megan, Vivian Renó, and Evlyn Novo. 2014. The Concept, Dimensions and Methods of Assessment of Human Well-Being within a Socioecological Context: A Literature Review. Social Indicators Research 116: 681–98. [Google Scholar] [CrossRef]
- Kurebwa, Jeffrey, and Nyasha Kurebwa. 2014. Coping Strategies of Child-Headed Households in Bindura Urban Zimbabwe. International Journal of Innovative Research and Development 3: 236–49. [Google Scholar]
- Le, Trang Mai, and Nilan Yu. 2021. Sexual and Reproductive Health Challenges Facing Minority Ethnic Girls in Vietnam: A Photovoice Study. Culture, Health & Sexuality 23: 1015–33. [Google Scholar] [CrossRef]
- Le Roux-Kemp, Andra. 2013. Child Headed Households in South Africa: The Legal and Ethical Dilemmas When Children Are the Primary Caregivers in a Therapeutic Relationship. In People Being Patients: International, Interdisciplinary Perspectives. Edited by Peter Bray and Diana Mak. London: Inter-Disciplinary Press. [Google Scholar]
- Lee, Veronica C., Patrick Muriithi, Ulrike Gilbert-Nandra, Andrea A. Kim, Mary E. Schmitz, James Odek, Rose Mokaya, Jennifer S. Galbraith, and KAIS Study Group. 2014. Orphans and Vulnerable Children in Kenya: Results from a Nationally Representative Population-Based Survey. JAIDS Journal of Acquired Immune Deficiency Syndromes 66: S89–S97. [Google Scholar] [CrossRef]
- Lindhout, Partick, Truus Teunissen, and Genserik Reniers. 2021. What about Using Photovoice for Health and Safety? International Journal of Environmental Research and Public Health 18: 11985. [Google Scholar] [CrossRef]
- Loewenson, Rene, and Marie Masotya. 2018. Pathways to Urban Health Equity Report of Multi-Method Research in East and Southern Africa. Harare: Civic Forum on Human Development and Lusaka District Health Office. [Google Scholar]
- Makuyana, Abigail, Shingirai P. Mbulayi, and Mbulayi Kangethe Shingirai. 2020. Psychosocial Deficits Underpinning Child Headed Households (Chhs) in Mabvuku and Tafara Suburbs of Harare, Zimbabwe. Children and Youth Services Review 115: 105093. [Google Scholar] [CrossRef]
- McCollum, Rosalind, Sally Theobald, Lilian Otiso, Tim Martineau, Robinson Karuga, E. Barasa, Sassy Molyneux, and M. Taegtmeyer. 2018. Priority Setting for Health in the Context of Devolution in Kenya: Implications for Health Equity and Community-Based Primary Care. Health Policy and Planning 33: 729–42. [Google Scholar] [CrossRef]
- Ministry of Health. 2018. Kenya AIDS Response Progress Report 2018; Saint Vincent and the Grenadines: Ministry of Health.
- Mogotlane, Sophie Mataniele, Chauke Motshedisi, van Rensburg Gisela, Human Sarie, and Kganakga Mokgadi. 2010. A Situational Analysis of Child-Headed Households in South Africa. Curationis 33: 24–32. [Google Scholar] [CrossRef]
- Moyo, Wisdom. 2013. Causes and Effects of Poverty on Academic Achievements of Rural Secondary School Students: Case of Tshazi Secondary School in Insiza District. International Journal of Asian Social Science 3: 2104–13. [Google Scholar]
- National AIDS and STI Control Programme (NASCOP). 2015. Guidelines for Conducting Adolescent Hiv Sexual and Reproductive Health Research in Kenya. Nairobi: National AIDS and STI Control Programme (NASCOP). [Google Scholar]
- Ndeda, Mildred. 2013. The Gendered Face of Orphanhood: The Double Vulnerability of Female Orphans in Child-Headed Households in Kisumu East District. Les Cahiers d’Afrique de l’Est/The East African Review 46: 81–104. [Google Scholar] [CrossRef]
- Nowell, Lorelli S., Jill M. Norris, Deborah E. White, and Nancy J. Moules. 2017. Thematic Analysis:Striving to Meet the Trustworthiness Criteria. International Journal of Qualitative Methods 16: 1609406917733847. [Google Scholar] [CrossRef]
- Nykiforuk, Candace, Vallianatos Helen, and Nieuwendyk Laura. 2011. Photovoice as a Method for Revealing Community Perceptions of the Built and Social Environment. International Journal of Qualitative Methods 10: 103–124. [Google Scholar] [CrossRef]
- Pillay, Jace. 2016. Problematising Child-Headed Households: The Need for Children’s Participation in Early Childhood Interventions. South African Journal of Childhood Education 6: 1–8. [Google Scholar] [CrossRef]
- Pipa, Tony, and Conroy Caroline. 2020. Leave No One Behind Time for Specifics on the Sustainable Development Goals. Washington, DC: Brookings Institution Press. [Google Scholar]
- Ronzi, Sara, Puzzolo Elisa, Hyseni Lirije, Higgerson James, Stanistreet Debbi, Hugo Mbatchou, Bruce Nigel, and Pope Daniel. 2019. Using photovoice methods as a community-based participatory research tool to advance uptake of clean cooking and improve health: The LPG adoption in Cameroon evaluation studies. Social Science & Medicine 228: 30–40. [Google Scholar] [CrossRef]
- Sevelius, Jae, Gutierrez-Mock Luis, Zamudio-Haas Sophia, McCree Breonna, Ngo Azize, Jackson Akira, Clynes Carla, Venegas Luz, Salinas Arianna, Herrera Cinthya, and et al. 2020. Research with Marginalized Communities: Challenges to Continuity During the COVID-19 Pandemic. AIDS and Behavior 24: 2009–2012. [Google Scholar] [CrossRef] [PubMed]
- The Lancet. 2017. Health in Slums: Understanding the Unseen. The Lancet 389: 478. [Google Scholar] [CrossRef]
- Thwala, S’lungile. 2018. Experiences and Coping Strategies of Children From Child-Headed Households in Swaziland. Journal of Education and Training Studies 6: 9. [Google Scholar] [CrossRef]
- Un-Habitat. 2020. World Cities Report 2020: The Value of Sustainable Urbanization. Nairobi: UN-Habitat. [Google Scholar]
- United Nations. 2017. Leaving No-One Behind: Equality and Non-Discrimination at the Heart of Sustainable Development. New York: United Nations. [Google Scholar]
- Van Breda, Adrian D. 2010. The Phenomenon and Concerns of Child-Headed Households in Africa. In Sozialarbeit des Südens, Band III: Kindheiten und Kinderrechte. Edited by Manfred Liebel and Ronald Lutz. Oldenberg: Paolo Freire Verlag, pp. 259–80. [Google Scholar]
- Wang, Caroline. 1999. Photovoice: A participatory action research strategy applied to women’s health. Journal Womens Health 8: 185–192. [Google Scholar] [CrossRef] [PubMed]
- Wang, Caroline, and Cheri Pies. 2004. Family, Maternal, and Child Health through Photovoice. Maternal and Child Health Journal 8: 95–102. [Google Scholar] [CrossRef] [PubMed]
- Wang, Caroline, Burris Mary, and Ann Burris. 1997. Photovoice: Concept, methodology, and use for participatory needs assessment. Health Education & Behavior 24: 369–87. [Google Scholar] [CrossRef] [PubMed]
- Ward, Laura, and Carola Eyber. 2009. Resiliency of Children in Child-Headed Households in Rwanda: Implications for Community Based Psychosocial Interventions. Intervention 7: 17–33. [Google Scholar] [CrossRef]
- White, Sarah. 2009. Analyzing Wellbeing: A Framework for Development Practice. In Wellbeing in Developing Countries. Bath: Bath University. [Google Scholar]
- White, Sarah. 2010. Analysing Wellbeing: A Framework for Development Practice. Development in Practice 20: 158–72. [Google Scholar] [CrossRef]
- Yiftachel, Oren. 2009. Theoretical Notes on ‘Gray Cities’: The Coming of Urban Apartheid? Planning Theory 8: 88–100. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Korogocho | Viwandani | |||||
|---|---|---|---|---|---|---|
| Method | Participants | Age | Sex | Pseudonyms | Age | Sex |
| Photovoice | CHH1-KG | 17 | Female | CHH 1-VIW(Jacinta) | 17 years | Female |
| CHH 2-KG | 17 | Male | CHH-2-VIW(Brian) | 17 years | Male | |
| IDI | CHH 3-KG | 17 | Male | CHH 3-VIW (Kevin) | 17 years | Male |
| CHH 4-KG | 17 | Male | CHH 4-VIW(Shadrack) | 17 years | Male | |
| CHH 5-KG | 17 | Female | CHH 5-VIW (Teresia) | 17 years | Female | |
| CHH 6-KG | 16 | Female | CHH 6-VIW (Imani) | 16 years | Female | |
| Total | 6 | 6 | ||||
| Participant Pseudonyms | Age | Gender | Axis of Inequalities |
|---|---|---|---|
| Korogocho Informal Settlement | |||
| Violet | 17 years | Female | Violet is responsible for taking care of nine family members living in one room. She became the primary caregiver to her family since her mother fell ill in 2020. Her elder brother and sisters have turned to alcohol and drug abuse since her mother became unwell, leaving her to provide for her sisters, nieces and nephews. One of her sisters is disabled. Violet attends school but frequently skips to work for income e.g., washing clothes. Two of her sisters died in the course of the photovoice study. |
| Robert | 17 years | Male | Robert’s mother is blind which has led him to be the primary caregiver of his family with other young dependents—11 and 13-year-old siblings. He attends school when he has the funds and is actively involved in church. He is also taking ARV medication for HIV. |
| Musa | 17 years | Male | Musa lives with his father, who is alcohol-dependent, and a stepmother. Musa’s mother relocated to their rural home. Because his father and stepmother do not provide for the family, he dropped out of school to work and provide for his five siblings and biological mother. |
| Tumaini | 17 years | Female | Tumaini was abandoned by her mother and could not proceed to secondary school. She has no source of income, and she takes care of 2 siblings aged below 10 years. |
| Sandra | 16 years | Female | Sandra was unable to proceed to high school after she was abandoned by her mother. She has no source of income and is responsible for taking care of three younger siblings and her own child. She has a history of experiencing GBV. |
| Job | 17 years | Male | Job is an orphaned child who dropped out of school. He lives on his own in a mud house and has no social support. |
| Viwandani Informal Settlement | |||
| Paula | 17 years | Female | Paula washes people’s clothes for income so as to support the family. She lives in a mud house and is the primary caregiver to two siblings who are in primary school and her infant son. She was abandoned by her mother and had to drop out of school because she became pregnant and so that she could take care of her siblings and her own child. She has no social or financial support. |
| Daniel | 17 years | Male | Daniel’s mother died. He lives with his father who is mentally ill. His father needs full-time care because he occasionally wanders off and has to be sought after. Daniel still attends school and is a primary caregiver to two siblings, a boy, and a girl. He engages himself in casual jobs after school and during weekends to generate income. |
| Meshack | 17 years | Male | Meshack dropped out of primary school to take care of his bedridden mother. To sustain the family, he engages in making illegal electricity and water connections to houses in the slums for a fee. He also works in a nearby market as a carrier. He does not have a birth certificate, which makes it impossible for him to obtain a national identification card when he turns 18 years old. This is a major source of stress for him. |
| Mwangaza | 17 years | Female | Mwangaza was abandoned by both parents and lives in a shack, which occasionally floods with stormwater and sewage. She dropped out of secondary school to take care of her two-year-old child. She does menial jobs such as dishwashing in a nearby food kiosk and is paid with food for herself and her child. |
| Imani | 16 years | Female | Imani lives alone with her infant. The father of her child deserted her. She was chased away from her parents’ home when she became pregnant and lost all her family support. She lives in a semi-permanent shack. She had to drop out of school to generate income by washing clothes. |
| Shadrack | 17 years | Male | Shadrack lives with his mother who has a physical disability. His father relocated to their rural home when he lost employment due to the COVID-19 pandemic. His mother is uncomfortable with being taken care of by a child. He is unable to obtain employment in the surrounding factories because he is underage. He ekes out a living by washing utensils in nearby restaurants. Being out of school is a major source of stress for him because his ambition is to be a doctor when he grows up. Shadrack lives in constant fear of being evicted due to rental arrears. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karuga, R.; Steege, R.; Njoroge, I.; Liani, M.; Wiltgen Georgi, N.; Otiso, L.; Muturi, N.; Okoth, L.A.; Theobald, S.; Tolhurst, R. Leaving No One Behind: A Photovoice Case Study on Vulnerability and Wellbeing of Children Heading Households in Two Informal Settlements in Nairobi. Soc. Sci. 2022, 11, 296. https://doi.org/10.3390/socsci11070296
Karuga R, Steege R, Njoroge I, Liani M, Wiltgen Georgi N, Otiso L, Muturi N, Okoth LA, Theobald S, Tolhurst R. Leaving No One Behind: A Photovoice Case Study on Vulnerability and Wellbeing of Children Heading Households in Two Informal Settlements in Nairobi. Social Sciences. 2022; 11(7):296. https://doi.org/10.3390/socsci11070296
Chicago/Turabian StyleKaruga, Robinson, Rosie Steege, Inviolata Njoroge, Millicent Liani, Neele Wiltgen Georgi, Lilian Otiso, Nelly Muturi, Linet Atieno Okoth, Sally Theobald, and Rachel Tolhurst. 2022. "Leaving No One Behind: A Photovoice Case Study on Vulnerability and Wellbeing of Children Heading Households in Two Informal Settlements in Nairobi" Social Sciences 11, no. 7: 296. https://doi.org/10.3390/socsci11070296
APA StyleKaruga, R., Steege, R., Njoroge, I., Liani, M., Wiltgen Georgi, N., Otiso, L., Muturi, N., Okoth, L. A., Theobald, S., & Tolhurst, R. (2022). Leaving No One Behind: A Photovoice Case Study on Vulnerability and Wellbeing of Children Heading Households in Two Informal Settlements in Nairobi. Social Sciences, 11(7), 296. https://doi.org/10.3390/socsci11070296