
Higher Leg and Trunk Muscle Activation during Balance Control in Copers versus People with Chronic Ankle Instability and Healthy Female Athletes

 ,
,  and
and
Abstract
:Highlights
- Athletes with a history of ankle sprain that do not suffer from ankle instability (copers) exhibit similar balance and neuromuscular control compared to healthy athletes.
- Athletes with chronic ankle instability show a deficit in neuromuscular control and balance, which may increase the risk of subsequent injuries.
- Athletes with chronic ankle instability are advised to use neuromuscular training in their rehabilitation program to improve balance and neuromuscular performance to reduce the risk of injury.
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedure
2.3. Postural Stability
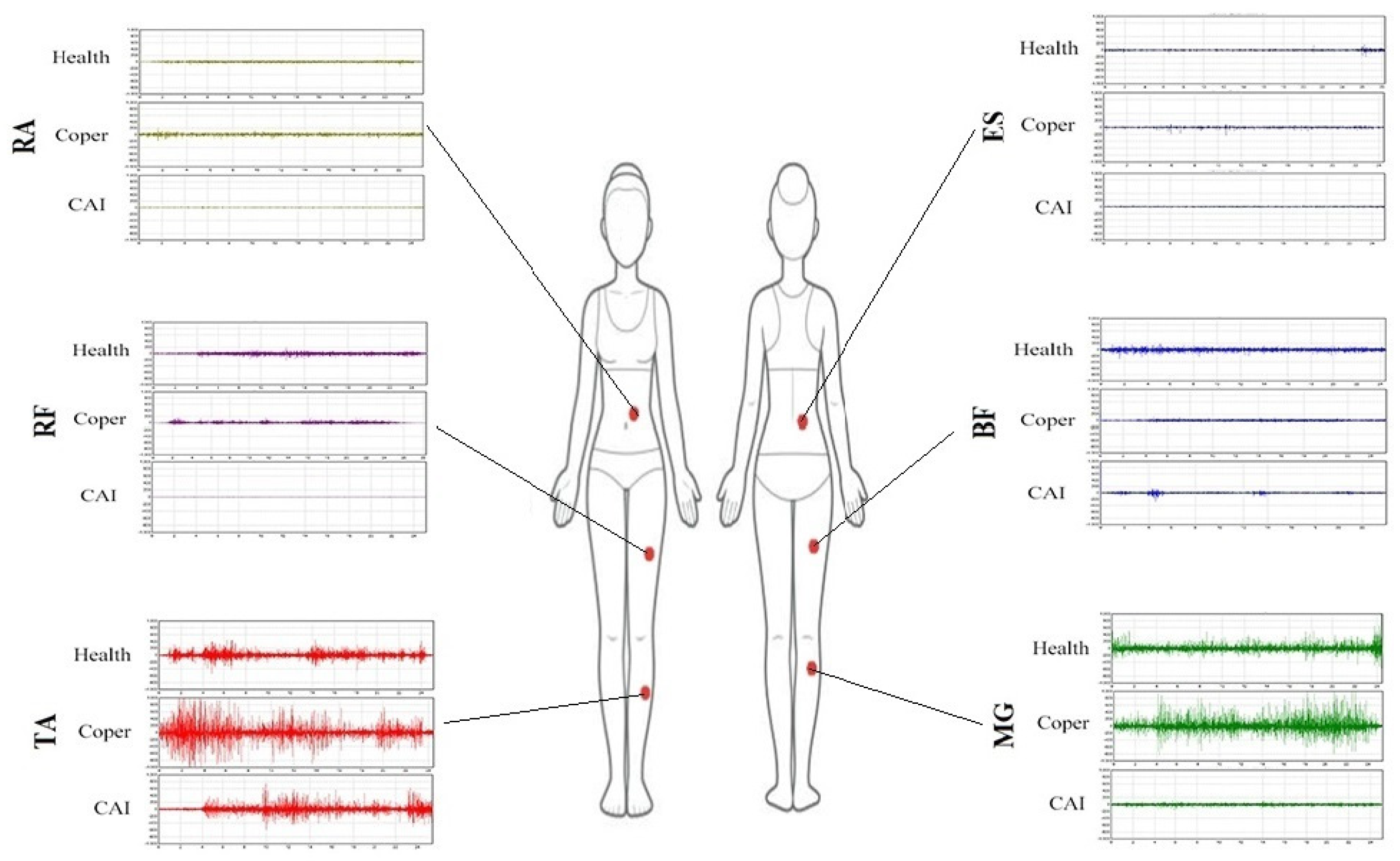
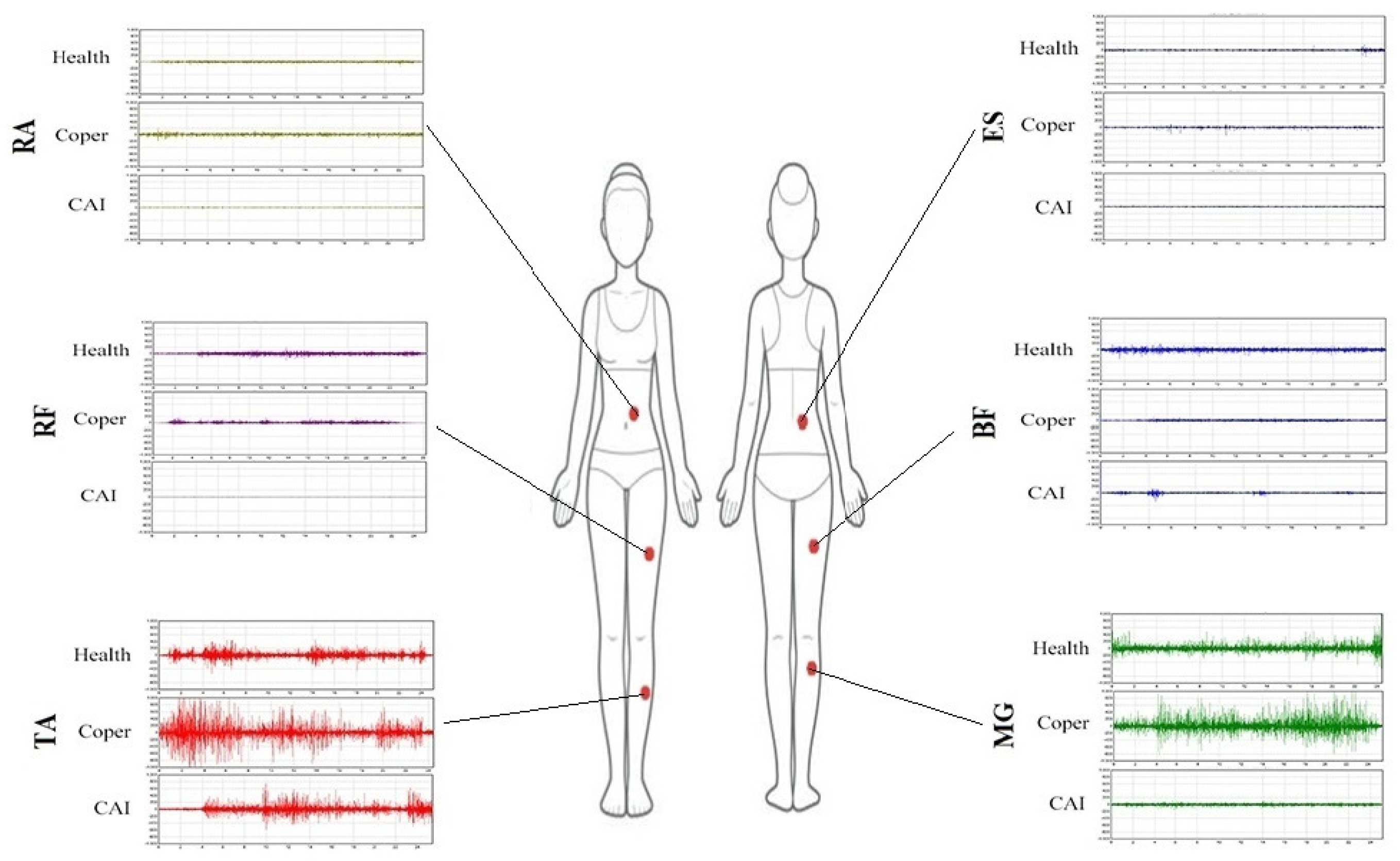
2.4. Electromyography (EMG) Measurement
2.5. Statistical Analysis
3. Results
3.1. EMG Activity during Unstable Condition
3.2. EMG Activity during Stable Condition
3.3. EMG Activity between Stable and Unstable Conditions
3.4. Balance Error Scores during Unstable Condition
3.5. Balance Error Scores during Stable Conditions
3.6. Balance Error Scores between Stable and Unstable Conditions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Waterman, B.R.; Owens, B.D.; Davey, S.; Zacchilli, M.A.; Belmont, P.J., Jr. The epidemiology of ankle sprains in the United States. JBJS 2010, 92, 2279–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gribble, P.A.; Bleakley, C.M.; Caulfield, B.M.; Docherty, C.L.; Fourchet, F.; Fong, D.T.-P.; Hertel, J.; Hiller, C.E.; Kaminski, T.W.; McKeon, P.O. 2016 consensus statement of the International Ankle Consortium: Prevalence, impact and long-term consequences of lateral ankle sprains. Br. J. Sports Med. 2016, 50, 1493–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michelson, J.D.; Hutchins, C. Mechanoreceptors in human ankle ligaments. J. Bone Jt. Surg. Br. Vol. 1995, 77, 219–224. [Google Scholar] [CrossRef]
- McKeon, P.O.; Hertel, J. Systematic review of postural control and lateral ankle instability, part I: Can deficits be detected with instrumented testing? J. Athl. Train. 2008, 43, 293–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldie, P.A.; Evans, O.M.; Bach, T.M. Postural control following inversion injuries of the ankle. Arch. Phys. Med. Rehabil. 1994, 75, 969–975. [Google Scholar] [CrossRef]
- Mattacola, C.G.; Dwyer, M.K. Rehabilitation of the ankle after acute sprain or chronic instability. J. Athl. Train. 2002, 37, 413. [Google Scholar]
- Freeman, M.; Dean, M.; Hanham, I. The etiology and prevention of functional instability of the foot. J. Bone Jt. Surg. Br. Vol. 1965, 47, 678–685. [Google Scholar] [CrossRef]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.; Caulfield, B.; Docherty, C.; Fourchet, F.; Fong, D.; Hertel, J.; Hiller, C.; Kaminski, T. Selection criteria for patients with chronic ankle instability in controlled research: A position statement of the International Ankle Consortium. J. Orthop. Sports Phys. Ther. 2013, 43, 585–591. [Google Scholar] [CrossRef] [Green Version]
- Wikstrom, E.A.; Brown, C.N. Minimum reporting standards for copers in chronic ankle instability research. Sports Med. 2014, 44, 251–268. [Google Scholar] [CrossRef]
- Liu, K.; Dierkes, C.; Blair, L. A new jump-landing protocol identifies differences in healthy, coper, and unstable ankles in collegiate athletes. Sports Biomech. 2016, 15, 245–254. [Google Scholar] [CrossRef]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Sweeney, K.; Patterson, M.R.; Delahunt, E. Lower limb interjoint postural coordination one year after first-time ankle sprain. Med. Sci. Sports Exerc. 2015, 47, 2398–2405. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, R.; Rogers, D.K.; McCloskey, D. Stable human standing with lower-limb muscle afferents providing the only sensory input. J. Physiol. 1994, 480, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Loram, I.D.; Maganaris, C.N.; Lakie, M. Active, non-spring-like muscle movements in human postural sway: How might paradoxical changes in muscle length be produced? J. Physiol. 2005, 564, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Nashner, L.M.; McCollum, G. The organization of human postural movements: A formal basis and experimental synthesis. Behav. Brain Sci. 1985, 8, 135–150. [Google Scholar] [CrossRef]
- Shields, C.A.; Needle, A.R.; Rose, W.C.; Swanik, C.B.; Kaminski, T.W. Effect of Elastic Taping on Postural Control Deficits in Subjects With Healthy Ankles, Copers, and Individuals With Functional Ankle Instability. Foot Ankle Int. 2013, 34, 1427–1435. [Google Scholar] [CrossRef]
- Watabe, T.; Takabayashi, T.; Tokunaga, Y.; Kubo, M. Individuals with chronic ankle instability exhibit altered ankle kinematics and neuromuscular control compared to copers during inversion single-leg landing. Phys. Ther. Sport 2021, 49, 77–82. [Google Scholar] [CrossRef]
- Watabe, T.; Takabayashi, T.; Tokunaga, Y.; Yoshida, T.; Kubo, M. Copers adopt an altered movement pattern compared to individuals with chronic ankle instability and control groups in unexpected single-leg landing and cutting task. J. Electromyogr. Kinesiol. 2021, 57, 102529. [Google Scholar] [CrossRef]
- Kwon, Y.U. Static postural stability in chronic ankle instability, an ankle sprain and healthy ankles. Int. J. Sports Med. 2018, 39, 625–629. [Google Scholar] [CrossRef]
- Jaber, H.; Lohman, E.; Daher, N.; Bains, G.; Nagaraj, A.; Mayekar, P.; Shanbhag, M.; Alameri, M. Neuromuscular control of ankle and hip during performance of the star excursion balance test in subjects with and without chronic ankle instability. PLoS ONE 2018, 13, e0201479. [Google Scholar] [CrossRef] [Green Version]
- Labanca, L.; Mosca, M.; Ghislieri, M.; Agostini, V.; Knaflitz, M.; Benedetti, M.G. Muscle activations during functional tasks in individuals with chronic ankle instability: A systematic review of electromyographical studies. Gait Posture 2021, 90, 340–373. [Google Scholar] [CrossRef]
- Pozzi, F.; Moffat, M.; Gutierrez, G. Neuromuscular control during performance of a dynamic balance task in subjects with and without ankle instability. Int. J. Sports Phys. Ther. 2015, 10, 520. [Google Scholar] [PubMed]
- Feger, M.A.; Donovan, L.; Hart, J.M.; Hertel, J. Lower extremity muscle activation during functional exercises in patients with and without chronic ankle instability. PMR 2014, 6, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Dundas, M.A.; Gutierrez, G.M.; Pozzi, F. Neuromuscular control during stepping down in continuous gait in individuals with and without ankle instability. J. Sports Sci. 2014, 32, 926–933. [Google Scholar] [CrossRef] [PubMed]
- Delahunt, E.; Monaghan, K.; Caulfield, B. Ankle function during hopping in subjects with functional instability of the ankle joint. Scand. J. Med. Sci. Sports 2007, 17, 641–648. [Google Scholar] [CrossRef]
- Wright, C.J.; Arnold, B.L.; Ross, S.E.; Linens, S.W. Recalibration and validation of the Cumberland Ankle Instability Tool cutoff score for individuals with chronic ankle instability. Arch. Phys. Med. Rehabil. 2014, 95, 1853–1859. [Google Scholar] [CrossRef]
- van Melick, N.; Meddeler, B.M.; Hoogeboom, T.J.; Nijhuis-van der Sanden, M.W.; van Cingel, R.E. How to determine leg dominance: The agreement between self-reported and observed performance in healthy adults. PLoS ONE 2017, 12, e0189876. [Google Scholar] [CrossRef] [Green Version]
- Neumann, P.; Gill, V. Pelvic floor and abdominal muscle interaction: EMG activity and intra-abdominal pressure. Int. Urogynecology J. 2002, 13, 125–132. [Google Scholar] [CrossRef]
- Konrad, P. A Practical Introduction to Kinesiological Electromyography, Noraxon INC. 2005. Available online: https://hermanwallace.com/download/The_ABC_of_EMG_by_Peter_Konrad.pdf (accessed on 1 June 2022).
- De Luca, C.J.; Kuznetsov, M.; Gilmore, L.D.; Roy, S.H. Inter-electrode spacing of surface EMG sensors: Reduction of crosstalk contamination during voluntary contractions. J. Biomech. 2012, 45, 555–561. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef]
- Kunugi, S.; Masunari, A.; Yoshida, N.; Miyakawa, S. Postural stability and lower leg muscle activity during a diagonal single-leg landing differs in male collegiate soccer players with and without functional ankle instability. J. Phys. Fit. Sports Med. 2017, 6, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Muehlbauer, T.; Mettler, C.; Roth, R.; Granacher, U. One-leg standing performance and muscle activity: Are there limb differences? J. Appl. Biomech. 2014, 30, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Rosen, A.B.; Yentes, J.M.; McGrath, M.L.; Maerlender, A.C.; Myers, S.A.; Mukherjee, M. Alterations in cortical activation among individuals with chronic ankle instability during single-limb postural control. J. Athl. Train. 2019, 54, 718–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Needle, A.R.; Lepley, A.S.; Grooms, D.R. Central nervous system adaptation after ligamentous injury: A summary of theories, evidence, and clinical interpretation. Sports Med. 2017, 47, 1271–1288. [Google Scholar] [CrossRef] [PubMed]
- Bowker, S.; Terada, M.; Thomas, A.C.; Pietrosimone, B.G.; Hiller, C.E.; Gribble, P.A. Neural excitability and joint laxity in chronic ankle instability, coper, and control groups. J. Athl. Train. 2016, 51, 336–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hertel, J. Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. J. Athl. Train. 2002, 37, 364. [Google Scholar]
- Bullock-Saxton, J.; Janda, V.; Bullock, M. The influence of ankle sprain injury on muscle activation during hip extension. Int. J. Sports Med. 1994, 15, 330–334. [Google Scholar] [CrossRef]
- Florence Tse, Y.Y.; Petrofsky, J.; Berk, L.; Daher, N.; Lohman, E.; Cavalcanti, P.; Laymon, M.; Rodrigues, S.; Lodha, R.; Potnis, P.A. Postural sway and EMG analysis of hip and ankle muscles during balance tasks. Int. J. Ther. Rehabil. 2013, 20, 280–288. [Google Scholar] [CrossRef]
- Horak, F.B.; Nashner, L.M. Central programming of postural movements: Adaptation to altered support-surface configurations. J. Neurophysiol. 1986, 55, 1369–1381. [Google Scholar] [CrossRef]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Dynamic balance deficits in individuals with chronic ankle instability compared to ankle sprain copers 1 year after a first-time lateral ankle sprain injury. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1086–1095. [Google Scholar] [CrossRef] [Green Version]
- Plante, J.E.; Wikstrom, E.A. Differences in clinician-oriented outcomes among controls, copers, and chronic ankle instability groups. Phys. Ther. Sport 2013, 14, 221–226. [Google Scholar] [CrossRef]
- Ross, S.E.; Guskiewicz, K.M. Examination of static and dynamic postural stability in individuals with functionally stable and unstable ankles. Clin. J. Sport Med. 2004, 14, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Son, S.J.; Seeley, M.K.; Hopkins, J.T. Altered movement biomechanics in chronic ankle instability, coper, and control groups: Energy absorption and distribution implications. J. Athl. Train. 2019, 54, 708–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Copers | CAI | Healthy | Sig. | |
|---|---|---|---|---|
| Age (years) | 21.9 ± 1.37 | 22.3 ± 4.21 | 24.5 ± 4.1 | 0.174 |
| Height (cm) | 165.9 ± 4.7 | 166.7 ± 5.8 | 165.7 ± 5.3 | 0.873 |
| Body mass (kg) | 56.2 ± 5.7 | 59 ± 7.4 | 57 ± 6.9 | 0.572 |
| BMI (kg.m−2) | 20.5 ± 2.7 | 21.2 ± 2.6 | 20.7 ± 2.5 | 0.784 |
| Coper | CAI | Healthy | Sig. | Effect Size (r) | |
|---|---|---|---|---|---|
| Medial gastrocnemius (level 3) | 35 ± 22 | 15 ± 4 | 33 ± 19 | 0.015 * 0.005 † | 0.5 ** 0.53 †† |
| Rectus abdominis (level 3) | 9 ± 5 | 5 ± 3 | 6 ± 3 | 0.013 * | 0.51 ** |
| Rectus femoris (level 3) | 10 ± 5 | 6 ± 4.2 | 14 ± 5 | 0.008 † | 0.53 †† |
| Rectus abdominis (level 12) | 8 ± 5 | 5 ± 3 | 6 ± 3 | 0.015 * | 0.5 ** |
| Tibialis anterior (level 12) | 18 ± 13 | 9 ± 4.2 | 9 ± 5 | 0.013 ‡ | 0.53 ‡‡ |
| Rectus femoris (level 12) | 8 ± 5 | 4 ± 4 | 11 ± 5 | 0.001 † | 0.67 †† |
| BBS Level | Coper | CAI | Healthy | Sig. | Effect Size (r) | |
|---|---|---|---|---|---|---|
| Tibialis anterior | 3 | 16 ± 13 | 16 ± 7 | 14 ± 9 | 0.003 * 0.004 † | 0.86 ** 0.85 †† |
| 12 | 18 ± 13 | 9 ± 4 | 9 ± 5 | |||
| Biceps femoris | 3 | 4 ± 3 | 3 ± 2 | 3 ± 2 | 0.015 * | 0.67 ** |
| 12 | 4 ± 3 | 2 ± 2 | 3 ± 2 | |||
| Rectus femoris | 3 | 10 ± 5 | 6 ± 4 | 14 ± 5 | 0.006 * 0.017 ‡ | 0.76 ** 0.75 ‡‡ |
| 12 | 8 ± 5 | 4 ± 4 | 11 ± 5 | |||
| Erector spinae | 3 | 6 ± 4 | 5 ± 3 | 5 ± 3 | 0.011 * 0.041 † | 0.66 ** 0.61 †† |
| 12 | 5 ± 6 | 3 ± 1 | 5 ± 3 | |||
| Rectus abdominis | 3 | 9 ± 5 | 5 ± 3 | 6 ± 3 | 0.018 * 0.025 ‡ | 0.66 ** 0.71 ‡‡ |
| 12 | 8 ± 5 | 5 ± 3 | 6 ± 3 | |||
| Medial gastrocnemius | 3 | 35.35 ± 22.1 | 15.97 ± 4.1 | 32.9 ± 18.56 | NS | NS |
| 12 | 31.56 ± 20.43 | 20.68 ± 13.13 | 32.56 ± 22.9 |
| BBS Difficulty Level | Coper | CAI | Healthy | Sig. | Effect Size (r) | |
|---|---|---|---|---|---|---|
| Medial–lateral | 3 | 2.3 ± 1.6 | 2.1 ± 1.4 | 0.8 ± 0.4 | 0.002 * 0.026 † 0.008 ‡ | 0.84 ** 0.67 †† 0.83 ‡‡ |
| 12 | 0.9 ± 0.4 | 0.9 ± 0.5 | 0.5 ± 0.2 | |||
| Anterior–posterior | 3 | 1.3 ± 0.7 | 1.8 ± 0.7 | 1.1 ± 0.9 | 0.013 * 0.021 ‡ | 0.64 ** 0.73 ‡‡ |
| 12 | 0.9 ± 0.3 | 1.2 ± 0.4 | 0.8 ± 06 | |||
| Overall | 3 | 3 ± 1.3 | 2.9 ± 1.4 | 1.4 ± 0.9 | 0.003 * 0.008 ‡ | 0.82 ** 0.73 ‡‡ |
| 12 | 1.4 ± 0.2 | 1.6 ± 0.4 | 1.1 ± 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karbalaeimahdi, M.; Alizadeh, M.H.; Minoonejad, H.; Behm, D.G.; Alizadeh, S. Higher Leg and Trunk Muscle Activation during Balance Control in Copers versus People with Chronic Ankle Instability and Healthy Female Athletes. Sports 2022, 10, 111. https://doi.org/10.3390/sports10080111
Karbalaeimahdi M, Alizadeh MH, Minoonejad H, Behm DG, Alizadeh S. Higher Leg and Trunk Muscle Activation during Balance Control in Copers versus People with Chronic Ankle Instability and Healthy Female Athletes. Sports. 2022; 10(8):111. https://doi.org/10.3390/sports10080111
Chicago/Turabian StyleKarbalaeimahdi, Mina, Mohammad Hossein Alizadeh, Hooman Minoonejad, David G. Behm, and Shahab Alizadeh. 2022. "Higher Leg and Trunk Muscle Activation during Balance Control in Copers versus People with Chronic Ankle Instability and Healthy Female Athletes" Sports 10, no. 8: 111. https://doi.org/10.3390/sports10080111
APA StyleKarbalaeimahdi, M., Alizadeh, M. H., Minoonejad, H., Behm, D. G., & Alizadeh, S. (2022). Higher Leg and Trunk Muscle Activation during Balance Control in Copers versus People with Chronic Ankle Instability and Healthy Female Athletes. Sports, 10(8), 111. https://doi.org/10.3390/sports10080111