
Change of Optical Coherence Tomography Morphology and Associated Structural Outcome in Diabetic Macular Edema after Ranibizumab Treatment

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subject Selection
2.2. Data Collection
2.3. Morphology Measurement
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Treatment Outcome
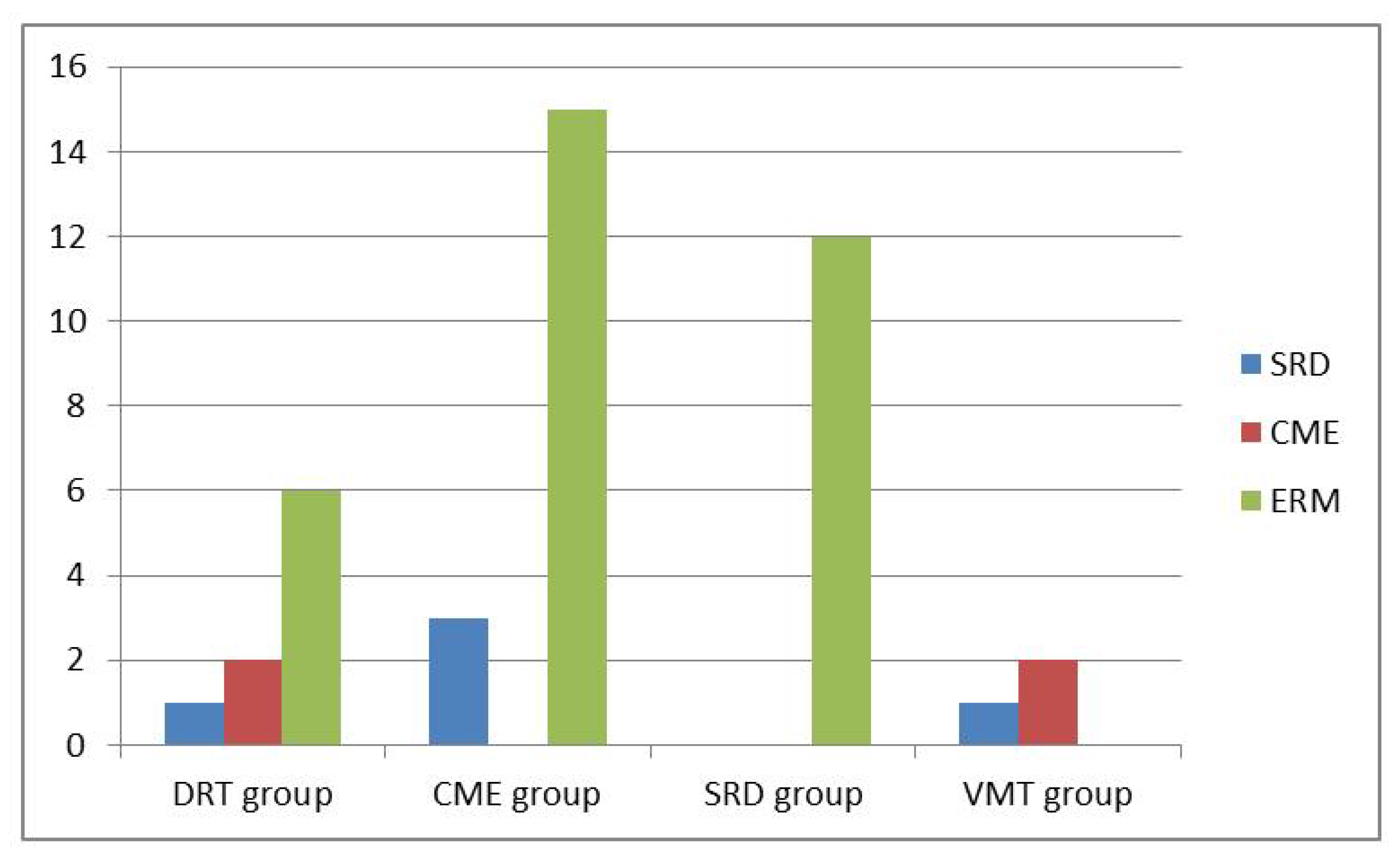
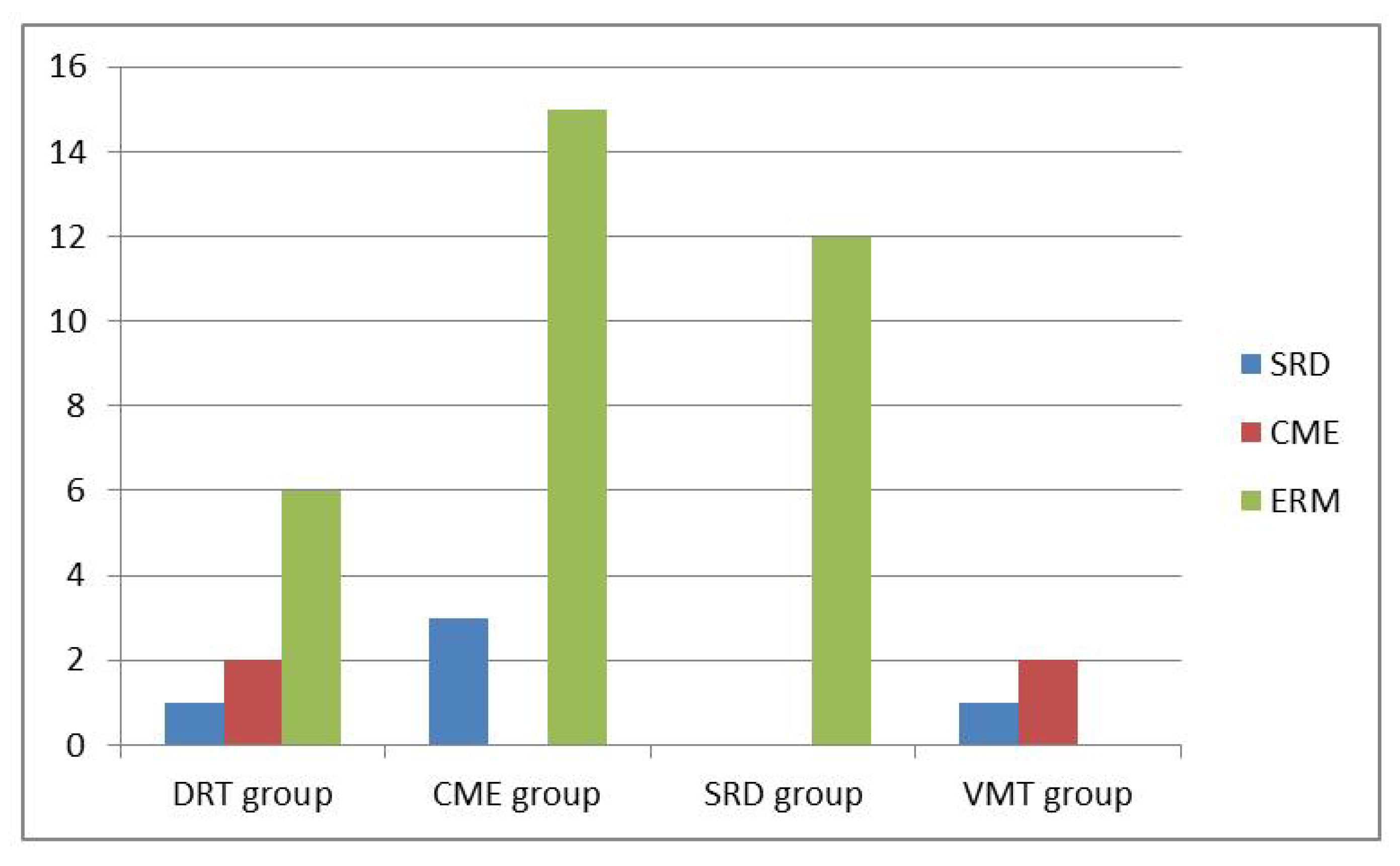
3.2. Subgroup Analysis for Morphological Changes
3.3. Correlation between Systemic Parameters and Morphology
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baskin, D.E. Optical coherence tomography in diabetic macular edema. Curr. Opin. Ophthalmol. 2010, 21, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.Y.; Smith, S.D.; Kaiser, P.K. Optical coherence tomographic patterns of diabetic macular edema. Am. J. Ophthalmol. 2006, 142, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.J.; Lee, D.H.; Kim, M. Optical coherence tomography findings predictive of response to treatment in diabetic macular edema. J. Int. Med. Res. 2018, 46, 4455–4464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buabbud, J.C.; Al-latayfeh, M.M.; Sun, J.K. Optical coherence tomography imaging for diabetic retinopathy and macular edema. Curr. Diab. Rep. 2010, 10, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Itoh, Y.; Petkovsek, D.; Kaiser, P.K.; Singh, R.P.; Ehlers, J.P. Optical coherence tomography features in diabetic macular edema and the impact on anti-vegf response. Ophthalmic. Surg. Lasers Imaging Retin. 2016, 47, 908–913. [Google Scholar] [CrossRef] [Green Version]
- Cheema, H.R.; Al Habash, A.; Al-Askar, E. Improvement of visual acuity based on optical coherence tomography patterns following intravitreal bevacizumab treatment in patients with diabetic macular edema. Int. J. Ophthalmol. 2014, 7, 251–255. [Google Scholar]
- Wu, P.C.; Lai, C.H.; Chen, C.L.; Kuo, C.N. Optical coherence tomographic patterns in diabetic macula edema can predict the effects of intravitreal bevacizumab injection as primary treatment. J. Ocul. Pharmacol. Ther. 2012, 28, 59–64. [Google Scholar] [CrossRef]
- Alkuraya, H.; Kangave, D.; Abu El-Asrar, A.M. The correlation between optical coherence tomographic features and severity of retinopathy, macular thickness and visual acuity in diabetic macular edema. Int. Ophthalmol. 2005, 26, 93–99. [Google Scholar] [CrossRef]
- Bressler, S.B.; Glassman, A.R.; Almukhtar, T.; Bressler, N.M.; Ferris, F.L.; Googe, J.M., Jr.; Gupta, S.K.; Jampol, L.M.; Melia, M.; Wells, J.A., 3rd; et al. Five-year outcomes of ranibizumab with prompt or deferred laser versus laser or triamcinolone plus deferred ranibizumab for diabetic macular edema. Am. J. Ophthalmol. 2016, 164, 57–68. [Google Scholar] [CrossRef] [Green Version]
- Heier, J.S.; Korobelnik, J.F.; Brown, D.M.; Schmidt-Erfurth, U.; Do, D.V.; Midena, E.; Boyer, D.S.; Terasaki, H.; Kaiser, P.K.; Marcus, D.M.; et al. Intravitreal aflibercept for diabetic macular edema: 148-week results from the vista and vivid studies. Ophthalmology 2016, 123, 2376–2385. [Google Scholar] [CrossRef]
- Sheu, S.J.; Lee, Y.Y.; Horng, Y.H.; Lin, H.S.; Lai, W.Y.; Tsen, C.L. Characteristics of diabetic macular edema on optical coherence tomography may change over time or after treatment. Clin. Ophthalmol. 2018, 12, 1887–1893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, C.K.; Cheng, C.K.; Peng, C.H. The incidence and risk factors for the development of vitreomacular interface abnormality in diabetic macular edema treated with intravitreal injection of anti-vegf. Eye 2017, 31, 762–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, N.-N.; Chen, W.-D.; Lai, C.-H.; Kuo, C.-N.; Chen, C.-L.; Huang, J.-C.; Wu, P.-C.; Wu, P.-L.; Chen, C.-Y. Optical coherence tomographic patterns as predictors of structural outcome after intravitreal ranibizumab in diabetic macula edema. Clin. Ophthalmol. 2020, 14, 4023–4030. [Google Scholar] [CrossRef]
- Romero-Aroca, P.; Baget-Bernaldiz, M.; Pareja-Rios, A.; Lopez-Galvez, M.; Navarro-Gil, R.; Verges, R. Diabetic macular edema pathophysiology: Vasogenic versus inflammatory. J. Diabetes Res. 2016, 2016, 2156273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otani, T.; Kishi, S.; Maruyama, Y. Patterns of diabetic macular edema with optical coherence tomography. Am. J. Ophthalmol. 1999, 127, 688–693. [Google Scholar] [CrossRef]
- Radovanova, K.T. Optical coherence tomography patterns in diabetic macular edema can predict the effectiveness of intravitreal bevacizumab combined with macular photocoagulation. J. Clin. Exp. Ophthalmol. 2014, 5. [Google Scholar] [CrossRef] [Green Version]
- Hoon Seo, K.; Yu, S.-Y.; Kim, M.; Woo Kwak, H. Visual and morphologic outcomes of intravitreal ranibizumab for diabetic macular edema based on optical coherence tomography patterns. Retina 2016, 36, 588–595. [Google Scholar]
- Kim, M.; Lee, P.; Kim, Y.; Yu, S.Y.; Kwak, H.W. Effect of intravitreal bevacizumab based on optical coherence tomography patterns of diabetic macular edema. Ophthalmologica 2011, 226, 138–144. [Google Scholar] [CrossRef]
- Koytak, A.; Altinisik, M.; Sogutlu Sari, E.; Artunay, O.; Umurhan Akkan, J.C.; Tuncer, K. Effect of a single intravitreal bevacizumab injection on different optical coherence tomographic patterns of diabetic macular oedema. Eye 2013, 27, 716–721. [Google Scholar] [CrossRef] [Green Version]
- Roh, M.I.; Kim, J.H.; Kwon, O.W. Features of optical coherence tomography are predictive of visual outcomes after intravitreal bevacizumab injection for diabetic macular edema. Ophthalmologica 2010, 224, 374–380. [Google Scholar] [CrossRef]
- Horii, T.; Murakami, T.; Nishijima, K.; Sakamoto, A.; Ota, M.; Yoshimura, N. Optical coherence tomographic characteristics of microaneurysms in diabetic retinopathy. Am. J. Ophthalmol. 2010, 150, 840–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joshi, L.; Bar, A.; Tomkins-Netzer, O.; Yaganti, S.; Morarji, J.; Vouzounis, P.; Seguin-Greenstein, S.; Taylor, S.R.; Lightman, S. Intravitreal bevacizumab injections for diabetic macular edema—Predictors of response: A retrospective study. Clin Ophthalmol. 2016, 10, 2093–2098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnin, S.; Sandali, O.; Bonnel, S.; Monin, C.; El Sanharawi, M. Vitrectomy with internal limiting membrane peeling for tractional and nontractional diabetic macular edema: Long-term results of a comparative study. Retina 2015, 35, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Cetin, E.N.; Demirtas, O.; Ozbakis, N.C.; Pekel, G. Quantitative assessment of macular contraction and vitreoretinal interface alterations in diabetic macular edema treated with intravitreal anti-vegf injections. Graefes Arch. Clin. Exp. Ophthalmol. 2018, 256, 1801–1806. [Google Scholar] [CrossRef]
- Zhang, X.; Zeng, H.; Bao, S.; Wang, N.; Gillies, M.C. Diabetic macular edema: New concepts in patho-physiology and treatment. Cell Biosci. 2014, 4, 27. [Google Scholar] [CrossRef] [Green Version]
- Hagenau, F.; Vogt, D.; Ziada, J.; Guenther, S.R.; Haritoglou, C.; Wolf, A.; Priglinger, S.G.; Schumann, R.G. Vitrectomy for diabetic macular edema: Optical coherence tomography criteria and pathology of the vitreomacular interface. Am. J. Ophthalmol. 2019, 200, 34–46. [Google Scholar] [CrossRef]
- Desjardins, D.M.; Yates, P.W.; Dahrouj, M.; Liu, Y.; Crosson, C.E.; Ablonczy, Z. Progressive early breakdown of retinal pigment epithelium function in hyperglycemic rats. Investig. Ophthalmol. Vis. Sci. 2016, 57, 2706–2713. [Google Scholar] [CrossRef] [Green Version]
- Daruich, A.; Matet, A.; Moulin, A.; Kowalczuk, L.; Nicolas, M.; Sellam, A.; Rothschild, P.R.; Omri, S.; Gelize, E.; Jonet, L.; et al. Mechanisms of macular edema: Beyond the surface. Prog. Retin. Eye Res. 2018, 63, 20–68. [Google Scholar] [CrossRef]
- Sophie, R.; Lu, N.; Campochiaro, P.A. Predictors of functional and anatomic outcomes in patients with diabetic macular edema treated with ranibizumab. Ophthalmology 2015, 122, 1395–1401. [Google Scholar] [CrossRef] [Green Version]
- Xie, J.; Ikram, M.K.; Cotch, M.F.; Klein, B.; Varma, R.; Shaw, J.E.; Klein, R.; Mitchell, P.; Lamoureux, E.L.; Wong, T.Y. Association of diabetic macular edema and proliferative diabetic retinopathy with cardiovascular disease: A systematic review and meta-analysis. JAMA Ophthalmol. 2017, 135, 586–593. [Google Scholar] [CrossRef]
- Wu, Y.; Zhu, W.; Li, Y.H.; Yu, J. Aspirin and age related macular degeneration; the possible relationship. Med. Hypothesis Discov. Innov. Ophthalmol. J. 2013, 2, 59. [Google Scholar]

{kind=link}
{kind=link}
| Description | Group 1 | Group 2 | p-Value |
|---|---|---|---|
| No. of eyes | 42 | 186 | |
| Male/Female | 19/14 | 76/41 | 0.437 |
| Age, years | 66.30 ± 9.47 | 65.66 ± 9.01 | 0.720 |
| Baseline BCVA (logMAR) | 0.84 ± 0.39 | 0.71 ± 0.36 | 0.035 |
| 2nd year BCVA (logMAR) | 0.99 ± 0.44 | 0.67 ± 0.30 | 0.001 |
| Baseline CMT | 422.07 ± 151.11 | 412.16 ± 109.67 | 0.690 |
| 2nd year CMT | 354.21 ± 89.02 | 305.33 ± 83.05 | 0.001 |
| 1 year dosage | 4.40 ± 1.13 | 4.30 ± 1.31 | 0.618 |
| 2 years dosage | 5.43 ± 1.71 | 5.31 ± 1.95 | 0.709 |
| HbA1c | 7.56 ± 1.09 | 7.56 ± 1.19 | 0.993 |
| NPDR/PDR | 26/16 | 114/72 | 0.941 |
| PRP | 33 | 130 | 0.260 |
| Pseudophakia | 9 | 51 | 0.426 |
| High Myopia | 2 | 5 | 0.616 |
| Smoking | 1 | 6 | 1.000 |
| Hypertension | 23 | 70 | 0.302 |
| Hyperlipidemia | 4 | 23 | 0.320 |
| Coronary artery disease | 2 | 7 | 1.000 |
| Stroke | 4 | 5 | 0.108 |
| Chronic kidney disease | 9 | 21 | 0.237 |
| Thyroid disease | 0 | 1 | 1.000 |
| Cancer | 2 | 4 | 0.613 |
| OCT Patterns | All No. (%) | No. of Changes over Time Period of 2 Years (%) |
|---|---|---|
| DRT group | ||
| DRT alone | 38 (16.67%) | 9 (23.7%) |
| Combined pattern | 0 (0%) | 0 (0%) |
| Total | 38 (16.67%) | 9 (23.7%) |
| CME group | ||
| CME alone | 20 (8.77%) | 3 (15.0%) |
| Combined pattern | 60 (26.3%) | 14 (23.3%) |
| Total | 80 (35.09%) | 17 (21.3%) |
| SRD group | ||
| SRD alone | 7 (3.07%) | 0 (0%) |
| Combined pattern | 38 (16.67%) | 11 (28.95%) |
| Total | 45 (19.7%) | 11(24.44%) |
| VMIA group | ||
| ERM alone | 13 (5.70%) | 1 (7.7%) |
| Combined pattern | 52 (22.80%) | 3 (5.77%) |
| Total | 65 (28.5%) | 4 (6.15%) |
| Variable | S.E | OR (95% CI) | p-Value |
|---|---|---|---|
| Intercept | 1.614 | 0.117 | |
| Age | 0.024 | 1.012 (0.966, 1.060) | 0.615 |
| Gender | 0.440 | 1.425 (0.602, 3.375) | 0.421 |
| Smoking | 1.242 | 0.487 (0.043, 5.555) | 0.563 |
| Alcohol | 0.963 | 1.743 (0.264, 11.500) | 0.564 |
| HbA1c | 0.186 | 1.061 (0.737, 1.526) | 0.750 |
| Hypertension | 0.460 | 1.459 (0.593, 3.593) | 0.411 |
| CAD | 0.933 | 0.631 (0.101, 3.925) | 0.622 |
| Stroke | 0.892 | 6.381 (1.112, 36.623) | 0.038 |
| CKD | 0.525 | 2.316 (0.828, 6.476) | 0.109 |
| Cancer | 0.931 | 1.085 (0.175, 6.733) | 0.930 |
| Hyperlipidemia | 0.728 | 0.258 (0.062, 1.075) | 0.063 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, N.-N.; Lai, C.-H.; Lee, C.-Y.; Kuo, C.-N.; Chen, C.-L.; Huang, J.-C.; Wu, P.-C.; Wu, P.-L.; Chen, C.-Y. Change of Optical Coherence Tomography Morphology and Associated Structural Outcome in Diabetic Macular Edema after Ranibizumab Treatment. J. Pers. Med. 2022, 12, 611. https://doi.org/10.3390/jpm12040611
Chen N-N, Lai C-H, Lee C-Y, Kuo C-N, Chen C-L, Huang J-C, Wu P-C, Wu P-L, Chen C-Y. Change of Optical Coherence Tomography Morphology and Associated Structural Outcome in Diabetic Macular Edema after Ranibizumab Treatment. Journal of Personalized Medicine. 2022; 12(4):611. https://doi.org/10.3390/jpm12040611
Chicago/Turabian StyleChen, Nan-Ni, Chien-Hsiung Lai, Chai-Yi Lee, Chien-Neng Kuo, Ching-Lung Chen, Jou-Chen Huang, Pei-Chen Wu, Pei-Lun Wu, and Chau-Yin Chen. 2022. "Change of Optical Coherence Tomography Morphology and Associated Structural Outcome in Diabetic Macular Edema after Ranibizumab Treatment" Journal of Personalized Medicine 12, no. 4: 611. https://doi.org/10.3390/jpm12040611
APA StyleChen, N.-N., Lai, C.-H., Lee, C.-Y., Kuo, C.-N., Chen, C.-L., Huang, J.-C., Wu, P.-C., Wu, P.-L., & Chen, C.-Y. (2022). Change of Optical Coherence Tomography Morphology and Associated Structural Outcome in Diabetic Macular Edema after Ranibizumab Treatment. Journal of Personalized Medicine, 12(4), 611. https://doi.org/10.3390/jpm12040611