
Association between 3D Printing-Assisted Pelvic or Acetabular Fracture Surgery and the Length of Hospital Stay in Nongeriatric Male Adults


 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
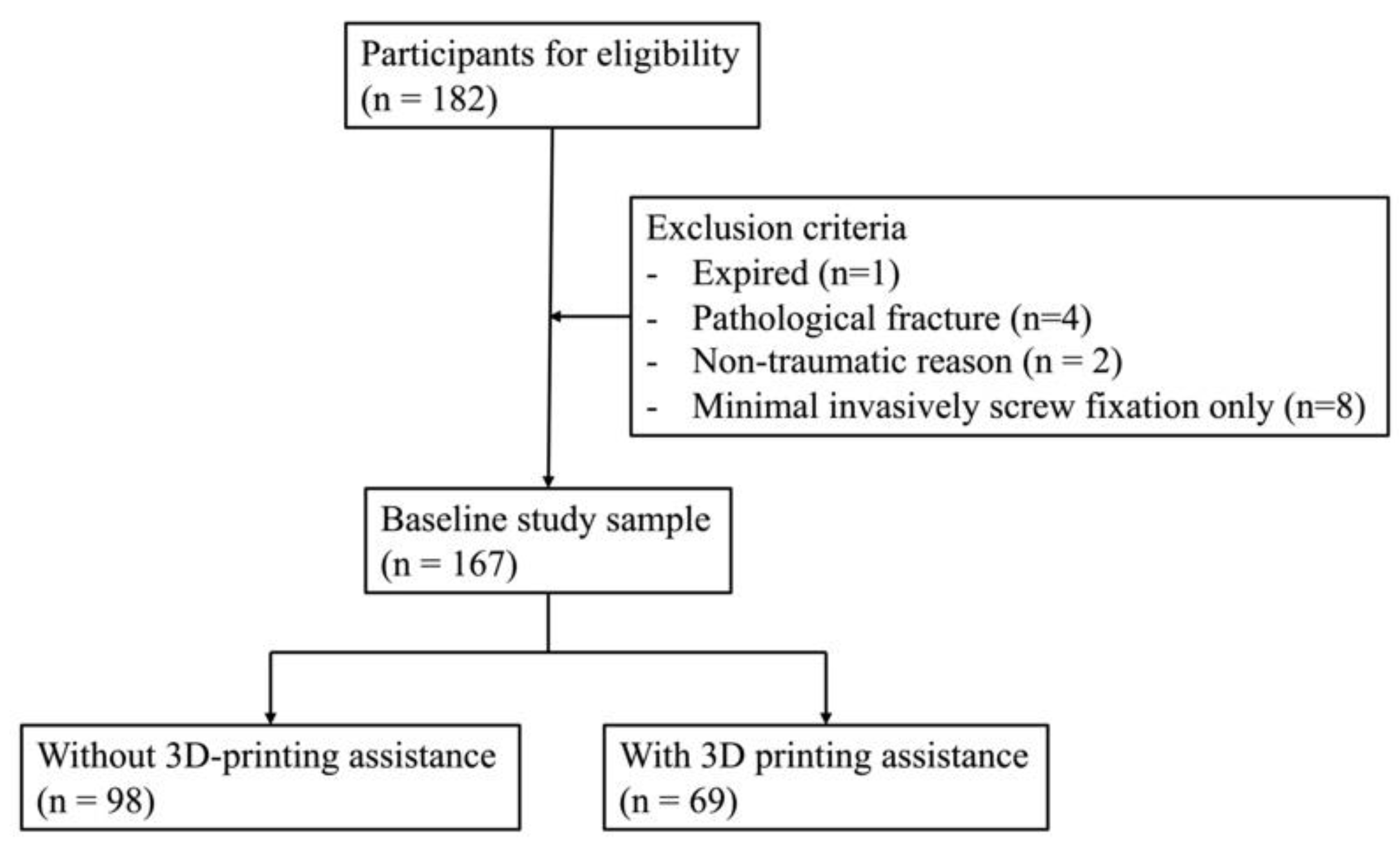
2.1. Study Design and Participant Selection
2.2. Surgical Treatment of Pelvic or Acetabular Fracture
2.3. Severity of Trauma
2.4. Covariates
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Demographics of the Study Participants
3.2. Measurable Factors and the LHS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Adams, J.E.; Davis, G.G.; Alexander, C.B.; Alonso, J.E. Pelvic trauma in rapidly fatal motor vehicle accidents. J. Orthop Trauma 2003, 17, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Ooi, C.K.; Goh, H.K.; Tay, S.Y.; Phua, D.H. Patients with pelvic fracture: What factors are associated with mortality? Int. J. Emerg. Med. 2010, 3, 299–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegmeth, A.; Müllner, T.; Kukla, C.; Vécsei, V. Associated injuries in severe pelvic trauma. Unfallchirurg 2000, 103, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Hermans, E.; Edwards, M.J.R.; Goslings, J.C.; Biert, J. Open pelvic fracture: The killing fracture? J. Orthop. Surg. Res. 2018, 13, 83. [Google Scholar] [CrossRef]
- Jones, A.L.; Powell, J.N.; Kellam, J.F.; McCormack, R.G.; Dust, W.; Wimmer, P. Open pelvic fractures. A multicenter retrospective analysis. Orthop Clin. N. Am. 1997, 28, 345–350. [Google Scholar] [CrossRef]
- Buller, L.T.; Best, M.J.; Quinnan, S.M. A Nationwide Analysis of Pelvic Ring Fractures: Incidence and Trends in Treatment, Length of Stay, and Mortality. Geriatr. Orthop. Surg. Rehabil. 2015, 7, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Ventola, C.L. Medical Applications for 3D Printing: Current and Projected Uses. P T 2014, 39, 704–711. [Google Scholar]
- Aimar, A.; Palermo, A.; Innocenti, B. The Role of 3D Printing in Medical Applications: A State of the Art. J. Healthcare Eng. 2019, 2019, 5340616. [Google Scholar] [CrossRef] [Green Version]
- Pugliese, L.; Marconi, S.; Negrello, E.; Mauri, V.; Peri, A.; Gallo, V.; Auricchio, F.; Pietrabissa, A. The clinical use of 3D printing in surgery. Updates Surg. 2018, 70, 381–388. [Google Scholar] [CrossRef]
- Askari, M.; Afzali Naniz, M.; Kouhi, M.; Saberi, A.; Zolfagharian, A.; Bodaghi, M. Recent progress in extrusion 3D bioprinting of hydrogel biomaterials for tissue regeneration: A comprehensive review with focus on advanced fabrication techniques. Biomater. Sci. 2021, 9, 535–573. [Google Scholar] [CrossRef]
- Tsoulfas, G.; Bangeas, P.I.; Suri, J.S.; Papadopoulos, V.N. Chapter 1—Introduction: The role of 3D printing in surgery. In 3D Printing: Applications in Medicine and Surgery; Tsoulfas, G., Bangeas, P.I., Suri, J.S., Eds.; Elsevier: St. Louis, MI, USA, 2020; pp. 1–6. [Google Scholar]
- Anderson, P.A. Chapter 6—3D Printing for Education and Surgical Planning in Orthopedic Surgery. In 3D Printing in Orthopaedic Surgery; Dipaola, M., Wodajo, F.M., Eds.; Elsevier: St. Louis, MI, USA, 2019; pp. 55–63. [Google Scholar]
- Coccolini, F.; Stahel, P.F.; Montori, G.; Biffl, W.; Horer, T.M.; Catena, F.; Kluger, Y.; Moore, E.E.; Peitzman, A.B.; Ivatury, R.; et al. Pelvic trauma: WSES classification and guidelines. World J. Emerg. Surg. 2017, 12, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morshed, S.; Knops, S.; Jurkovich, G.J.; Wang, J.; MacKenzie, E.; Rivara, F.P. The impact of trauma-center care on mortality and function following pelvic ring and acetabular injuries. J. Bone Joint Surg. Am. 2015, 97, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Cai, H.; Kuong, E.; Chui, E.; Siu, Y.C.; Ji, T.; Drstvenšek, I. Surgical applications of three-dimensional printing in the pelvis and acetabulum: From models and tools to implants. Unfallchirurg 2019, 122, 278–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, C.C.; Li, Y.T.; Chou, Y.C.; Chen, J.E.; Wu, C.C.; Shen, H.C.; Yeh, T.T. Conventional plate fixation method versus pre-operative virtual simulation and three-dimensional printing-assisted contoured plate fixation method in the treatment of anterior pelvic ring fracture. Int. Orthop. 2019, 43, 425–431. [Google Scholar] [CrossRef]
- Morgan, C.; Khatri, C.; Hanna, S.A.; Ashrafian, H.; Sarraf, K.M. Use of three-dimensional printing in preoperative planning in orthopaedic trauma surgery: A systematic review and meta-analysis. World J. Orthop. 2020, 11, 57–67. [Google Scholar] [CrossRef]
- Baker, S.P.; O’Neill, B.; Haddon, W., Jr.; Long, W.B. The injury severity score: A method for describing patients with multiple injuries and evaluating emergency care. J. Trauma 1974, 14, 187–196. [Google Scholar] [CrossRef]
- Rating the severity of tissue damage. I. The abbreviated scale. JAMA 1971, 215, 277–280. [CrossRef]
- Laird, A.; Keating, J.F. Acetabular fractures: A 16-year prospective epidemiological study. J. Bone Joint Surg. Br. 2005, 87, 969–973. [Google Scholar] [CrossRef]
- Balogh, Z.; King, K.L.; Mackay, P.; McDougall, D.; Mackenzie, S.; Evans, J.A.; Lyons, T.; Deane, S.A. The epidemiology of pelvic ring fractures: A population-based study. J. Trauma 2007, 63, 1066–1073. [Google Scholar] [CrossRef]
- Hung, C.-C.; Wu, J.-L.; Cheng, Y.-W.; Chen, W.-L.; Lee, S.-H.; Yeh, T.-T. Does 3D Printing-Assisted Acetabular or Pelvic Fracture Surgery Shorten Hospitalization Durations among Older Adults? J. Pers. Med. 2022, 12, 189. [Google Scholar] [CrossRef]
- Abe, T.; Komori, A.; Shiraishi, A.; Sugiyama, T.; Iriyama, H.; Kainoh, T.; Saitoh, D. Trauma complications and in-hospital mortality: Failure-to-rescue. Crit. Care 2020, 24, 223. [Google Scholar] [CrossRef] [PubMed]
- Divo, M.J.; Martinez, C.H.; Mannino, D.M. Ageing and the epidemiology of multimorbidity. Eur. Respir. J. 2014, 44, 1055–1068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turgut, K.; Sarihan, M.E.; Colak, C.; Güven, T.; Gür, A.; Gürbüz, S. Falls from height: A retrospective analysis. World J. Emerg. Med. 2018, 9, 46–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hahn, M.P.; Richter, D.; Ostermann, P.A.; Muhr, G. Injury pattern after fall from great height. An analysis of 101 cases. Unfallchirurg 1995, 98, 609–613. [Google Scholar]
- Kent, T.; Miller, J.; Shreve, C.; Allenback, G.; Wentz, B. Comparison of injuries among motorcycle, moped and bicycle traffic accident victims. Traffic Inj. Prev. 2022, 23, 34–39. [Google Scholar] [CrossRef]
- Lim, A.K. Abnormal liver function tests associated with severe rhabdomyolysis. World J. Gastroenterol. 2020, 26, 1020–1028. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Without 3D (n = 98) | With 3D (n = 69) | p Value * | |
|---|---|---|---|
| Continuous Variables, Median (IQR) | |||
| Age, year | 32 (23.75–44) | 35 (27–48.5) | 0.163 |
| BMI, kg/m2 | 25.06 (22.32–26.87) | 25.43 (23.21–27.04) | 0.288 |
| Hb, g/dL | 13.90 (12.50–14.93) | 13.7 (12.3–14.8) | 0.502 |
| Platelet, 103/uL | 209.00 (167.50–250.25) | 251.0 (197.0–301.0) | 0.004 |
| Glucose, mg/dL | 124 (107–151) | 131 (112–162.5) | 0.230 |
| Creatinine, mg/dL | 0.95 (0.8–1.1) | 0.9 (0.8–1.0) | 0.732 |
| AST, U/L | 39 (27.75–78) | 42.0 (31.0–65.5) | 0.750 |
| Sodium, mmol/L | 138 (136–139) | 138 (137–140) | 0.157 |
| Potassium, mmol/L | 3.7 (3.475–4.0) | 3.8 (3.5–4.0) | 0.496 |
| ISS | 10 (9–22.75) | 9 (9–22) | 0.428 |
| Length of hospital stay, days | 18 (13–26) | 21 (13–27) | 0.059 |
| Duration from injury to pelvic or acetabular surgery | 4 (2–7) | 4 (3–9) | 0.095 |
| Category variables, n (%) | |||
| Number of surgical procedures | 0.260 | ||
| One | 34 (34.7%) | 16 (29.9%) | |
| Two | 36 (36.7%) | 28 (38.3 %) | |
| More than 3 | 28 (28.6%) | 25 (31.7%) | |
| Mechanism | 0.600 | ||
| Traffic accident | 71 (72.4%) | 45 (65.2%) | |
| Falling from height | 24 (24.5%) | 21 (30.4%) | |
| Other | 3 (3.1%) | 3 (4.3%) | |
| Age | BMI | ISS | Hb | plt | GLU(ER) | Creatinine | AST | Na | K | Duration from Injury to Pelvic or Acetabulur Surgery | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pearson correlation | −0.072 | −0.029 | 0.497 | −0.350 | 0.069 | 0.153 | 0.111 | 0.319 | 0.023 | 0.066 | 0.137 |
| p value | 0.355 | 0.736 | 0.000 | 0.000 | 0.376 | 0.050 | 0.152 | <0.001 | 0.767 | 0.399 | 0.079 |
| Without 3D | |||||||||||
| Pearson correlation | −0.054 | −0.093 | 0.487 | −0.393 | 0.001 | 0.273 | 0.089 | 0.287 | −0.033 | 0.042 | 0.128 |
| p value | 0.598 | 0.401 | <0.001 | <0.001 | 0.990 | 0.007 | 0.384 | 0.004 | 0.747 | 0.678 | 0.212 |
| With 3D | |||||||||||
| Pearson correlation | −0.122 | 0.054 | 0.540 | −0.278 | 0.147 | 0.014 | 0.164 | 0.386 | 0.101 | 0.116 | 0.520 |
| p value | 0.317 | 0.706 | <0.001 | 0.021 | 0.228 | 0.908 | 0.177 | 0.001 | 0.414 | 0.344 | <0.001 |
| Univariable 1 | Multivariable 2 | |||
|---|---|---|---|---|
| β (SE) | p Value | β (SE) | p Value | |
| Age 18–40 (n = 105) | ||||
| Age | 0.039 (0.241) | 0.691 | ||
| BMI | 0.034 (0.349) | 0.825 | ||
| Hb | −0.432 (0.595) | <0.001 | −0.201 (0.489) | 0.013 |
| Platelet | 0.025 (0.016) | 0.801 | ||
| Glucose | 0.267 (0.038) | 0.006 | 0.139 (0.051) | 0.096 |
| Creatinine | −0.004 (6.286) | 0.965 | ||
| AST | 0.285 (0.008) | 0.003 | 0.099 (0.008) | 0.267 |
| Na | 0.051 (0.485) | 0.610 | ||
| K | −0.064 (2.917) | 0.516 | ||
| ISS | 0.464 (0.101) | <0.001 | 0.091 (0.094) | 0.292 |
| With 3D | 0.126 (2.879) | 0.202 | ||
| Duration from injury to pelvic or acetabular surgery | 0.101 (0.038) | 0.310 | ||
| Number of surgical procedures | 0.616 (1.450) | <0.001 | 0.500 (1.364) | <0.001 |
| Age 40–60 (n = 62) | ||||
| Age | −0.235 (0.445) | 0.117 | ||
| BMI | −0.084 (0.522) | 0.588 | ||
| Hb | −0.180 (0.851) | 0.161 | ||
| Platelet | 0.151 (0.017) | 0.241 | ||
| Glucose | 0.067 (0.030) | 0.609 | ||
| Creatinine | 0.310 (5.377) | 0.014 | −0.189 (4.281) | 0.059 |
| AST | 0.378 (0.011) | 0.002 | −0.127 (0.009) | 0.188 |
| Na | −0.024 (0.675) | 0.853 | ||
| K | 0.269 (3.368) | 0.035 | 0.018 (2.298) | 0.836 |
| ISS | 0.577 (0.148) | <0.001 | 0.449 (0.140) | <0.001 |
| With 3D | 0.024 (3.398) | 0.852 | ||
| Duration from injury to pelvic or acetabular surgery | 0.627 (0.190) | <0.001 | 0.359 (0.238) | 0.007 |
| Number of surgical procedures | 0.606 (1.765) | <0.001 | 0.516 (1.447) | <0.001 |
| Univariable 1 | Multivariable 2 | |||
|---|---|---|---|---|
| β (SE) | p Value | β (SE) | p Value | |
| Non-major trauma (n = 107) | ||||
| Age | 0.021 (0.078) | 0.829 | ||
| BMI | −0.040 (0.290) | 0.718 | ||
| Hb | −0.401 (0.537) | <0.001 | −0.212 (0.391) | 0.002 |
| Platelet | 0.237 (0.011) | 0.014 | 0.099 (0.008) | 0.128 |
| Glucose | 0.167 (0.023) | 0.086 | 0.010 (0.015) | 0.875 |
| Creatinine | 0.041 (5.199) | 0.673 | ||
| AST | 0.055 (0.037) | 0.573 | ||
| Na | 0.042 (0.433) | 0.669 | ||
| K | −0.164 (2.539) | 0.092 | −0.061 (1.650) | 0.340 |
| ISS | 0.185 (0.482) | 0.057 | 0.150 (0.319) | 0.019 |
| With 3D | 0.210 (1.984) | 0.030 | −0.003 (1.340) | 0.965 |
| Duration from injury to pelvic or acetabular surgery | 0.528 (0.236) | <0.001 | 0.291 (0.196) | <0.001 |
| Number of surgical procedures | 0.678 (1.002) | <0.001 | 0.492 (0.980) | <0.001 |
| Major trauma (n = 60) | ||||
| Age | −0.057 (0.192) | 0.666 | ||
| BMI | 0.112 (0.515) | 0.439 | ||
| Hb | −0.132 (0.884) | 0.298 | ||
| Platelet | −0.059 (0.020) | 0.652 | ||
| Glucose | 0.053 (0.045) | 0.691 | ||
| Creatinine | 0.084 (6.077) | 0.525 | ||
| AST | 0.276 (0.008) | 0.034 | 0.217 (0.008) | 0.071 |
| Na | −0.079 (0.637) | 0.553 | ||
| K | 0.234 (3.347) | 0.075 | 0.132 (2.990) | 0.257 |
| ISS | 0.384 (0.196) | 0.002 | 0.072 (0.189) | 0.567 |
| With 3D | 0.056 (4.415) | 0.672 | ||
| Duration from injury to pelvic or acetabular surgery | 0.053 (0.044) | 0.689 | ||
| Number of surgical procedures | 0.496 (2.264) | <0.001 | 0.439 (2.097) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, C.-C.; Shen, P.-H.; Wu, J.-L.; Cheng, Y.-W.; Chen, W.-L.; Lee, S.-H.; Yeh, T.-T. Association between 3D Printing-Assisted Pelvic or Acetabular Fracture Surgery and the Length of Hospital Stay in Nongeriatric Male Adults. J. Pers. Med. 2022, 12, 573. https://doi.org/10.3390/jpm12040573
Hung C-C, Shen P-H, Wu J-L, Cheng Y-W, Chen W-L, Lee S-H, Yeh T-T. Association between 3D Printing-Assisted Pelvic or Acetabular Fracture Surgery and the Length of Hospital Stay in Nongeriatric Male Adults. Journal of Personalized Medicine. 2022; 12(4):573. https://doi.org/10.3390/jpm12040573
Chicago/Turabian StyleHung, Chun-Chi, Pei-Hung Shen, Jia-Lin Wu, Yung-Wen Cheng, Wei-Liang Chen, Shih-Han Lee, and Tsu-Te Yeh. 2022. "Association between 3D Printing-Assisted Pelvic or Acetabular Fracture Surgery and the Length of Hospital Stay in Nongeriatric Male Adults" Journal of Personalized Medicine 12, no. 4: 573. https://doi.org/10.3390/jpm12040573
APA StyleHung, C.-C., Shen, P.-H., Wu, J.-L., Cheng, Y.-W., Chen, W.-L., Lee, S.-H., & Yeh, T.-T. (2022). Association between 3D Printing-Assisted Pelvic or Acetabular Fracture Surgery and the Length of Hospital Stay in Nongeriatric Male Adults. Journal of Personalized Medicine, 12(4), 573. https://doi.org/10.3390/jpm12040573