Abstract
Autologous fillet flaps are a common reconstructive option for large defects after forequarter amputation (FQA) due to advanced local malignancy or trauma. The inclusion of osseous structures into these has several advantages. This article therefore systematically reviews reconstructive options after FQA, using osteomusculocutaneous fillet flaps, with emphasis on personalized surgical technique and outcome. Additionally, we report on a case with an alternative surgical technique, which included targeted muscle reinnervation (TMR) of the flap. Our literature search was conducted in the PubMed and Cochrane databases. Studies that were identified were thoroughly scrutinized with regard to relevance, resulting in the inclusion of four studies (10 cases). FQA was predominantly a consequence of local malignancy. For vascular supply, the brachial artery was predominantly anastomosed to the subclavian artery and the brachial or cephalic vein to the subclavian or external jugular vein. Furthermore, we report on a case of a large osteosarcoma of the humerus. Extended FQA required the use of the forearm for defect coverage and shoulder contour reconstruction. Moreover, we performed TMR. Follow-up showed a satisfactory result and no phantom limb pain. In case of the need for free flap reconstruction after FQA, this review demonstrates the safety and advantage of osteomusculocutaneous fillet flaps. If the inclusion of the elbow joint into the flap is not possible, we recommend the use of the forearm, as described. Additionally, we advocate for the additional implementation of TMR, as it can be performed quickly and is likely to reduce phantom limb and neuroma pain.
1. Introduction
The multimodal treatment of primary malignant bone or soft tissue tumors involves multiagent chemotherapy, radiotherapy, and wide surgical resection. Since the combination and enhancement of these regimes, long-term survival rates have improved significantly over the last decades and the operative treatment advanced from direct amputation to limb-sparing surgery [1]. However, for patients with locally advanced tumors of the limbs, amputation remains the only curative option.
With regard to the upper extremity, interscapulothoracic amputation (ISTA) or forequarter amputation (FQA) is the most radical ablative procedure [2]. It involves the amputation of the complete upper extremity, including the anatomic structures of the shoulder girdle, leading to the loss of the shoulder silhouette. Besides malignant bone tumors, post-radiation defects and traumatic scapulothoracic dissociation are the most common indications for this rare procedure [2,3,4]. Depending on the extent of FQA, direct wound closure is often not possible. A common reconstructive option for large defects after FQA are fillet flaps. These are harvested from the amputated limb and do not create any additional donor side morbidity. Depending on the surgical technique, different flap designs have been established for the upper extremity—the fasciocutaneous, the musculocutaneous, and the osteomusculocutaneous fillet flap [5,6,7]. While the first two techniques are viable options for the coverage of skin and soft-tissue defects, the inclusion of osseous structures can also stabilize the thoracic wall and reconstruct the shoulder contour. Hence, this flap is called the “epaulette” flap, similar to the ornamental shoulder piece of military uniforms [2]. Besides cosmetic advantages, the “epaulette” flap also creates a stable osseous and soft-tissue envelope that provides a socket for an upper-limb prosthesis [7,8].
Recent developments in prosthetic medicine have created devices that offer multi-functional joints with fine motor capabilities, as well as improved comfort and aesthetics [9]. With the aim to accelerate the cortical control of these advanced prosthetic systems, the concept of targeted muscle reinnervation (TMR) was presented in 2002. In TMR, transected peripheral nerves are transferred to recipient motor nerves of residual muscles in the amputated limb in order to avert muscle atrophy and reinitiate organized muscle innervation [10,11]. Prior studies revealed that TMR additionally significantly reduces the risk of developing neuromas and phantom limb pain [9,12,13]. These two characteristics make TMR a viable option for reconstructive procedures following curative or palliative FQA.
The aim of this article was to systematically review previous approaches for chest wall stabilization and shoulder contour reconstruction after FQA with osteomusculocutaneous free fillet flaps. Moreover, we report on a case with an alternative surgical technique that incorporates the forearm, wrist, and metacarpus of the amputated limb into the flap in combination with TMR. The simultaneous utilization of TMR provides the first results on feasibility and improved neuropathic pain management after FQA and osseous “spare-parts” reconstruction.
2. Methods
The identification of studies for this review was based on the Preferred Reporting Systems for Systematic Reviews and Meta-Analysis (PRISMA) statement [14]. The MeSH terms “fillet flap”, “epaulette flap”, “osteomusculocutaneous flap”, “forequarter amputation”, and “interscapulothoracic amputation” were used to search the PubMed and Cochrane databases for publications that focus on shoulder contour reconstruction and thoracic wall stabilization with osteomusculocutaneous free fillet flaps after FQA. The literature search was completed on 3 February 2022. In total, 387 articles were identified (Figure 1). All of the results were imported into the Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia) for the removal of duplicates.
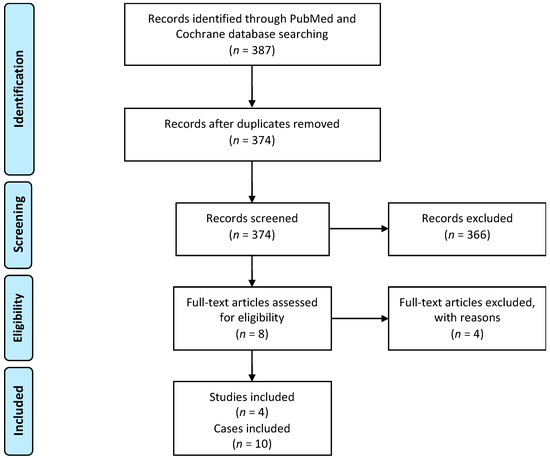
Figure 1.
Study-selection algorithm based on the Preferred Reporting Systems for Systematic Reviews and Meta-Analysis (PRISMA) statement.
First, the titles and abstracts of the citations were individually scrutinized to determine which were relevant to the review. Subsequently, studies were excluded if they were not available in English or German, or if they described the usage of cutaneous and musculocutaneous (soft-tissue) fillet flaps or other reconstructive procedures (non-fillet flaps) after FQA. This resulted in the identification of six articles that describe the usage of osteomusculocutaneous fillet flaps for reconstruction following FQA. Two of these were excluded from the study as they did not provide enough details on the surgical technique used, as well as outcome measurements [7,15]. Four studies remained that met the inclusion criteria.
3. Results
3.1. Literature Search
Ten cases of shoulder contour reconstruction and thoracic wall stabilization with osteomusculocutaneous free fillet flaps after FQA were described in the four publications that were identified (Table 1). In 8 out of 10 cases, FQA was a consequence of a local malignancy, whereas two cases were due to prior trauma. Four patients required palliative FQA, the rest were treated in a curative intention (n = 6). All of the patients survived the initial surgery.

Table 1.
Overview of all 10 cases that previously described free osteomusculocutaneous fillet flaps for thoracic wall stabilization and shoulder contour reconstruction after FQA.
Considering the vascular supply of the flap, the subclavian artery was predominantly anastomosed to the brachial artery (n = 8). Other options were the suprascapular artery (n = 1) and the internal thoracic artery (n = 1). In 5 out of 10 cases, two venous anastomoses were completed. In the majority of cases, the brachial or cephalic vein of the flap was connected to the subclavian or the external jugular vein (n = 7). Three cases required revision surgery due to an infected hematoma (n = 1), partial skin necrosis (n = 2), and/or arterial thrombosis (n = 1). Another case required tumor re-excision after the confirmation of a R1 tumor margin. Three out of a total of six sarcoma patients developed pulmonary metastases within the first 18 months after surgery, and two of these patients died within the observation period. Another patient died 13 years after the initial operation from a local recurrence of the sarcoma. Both patients with traumatic FQA survived the follow-up period.
3.2. Case Report
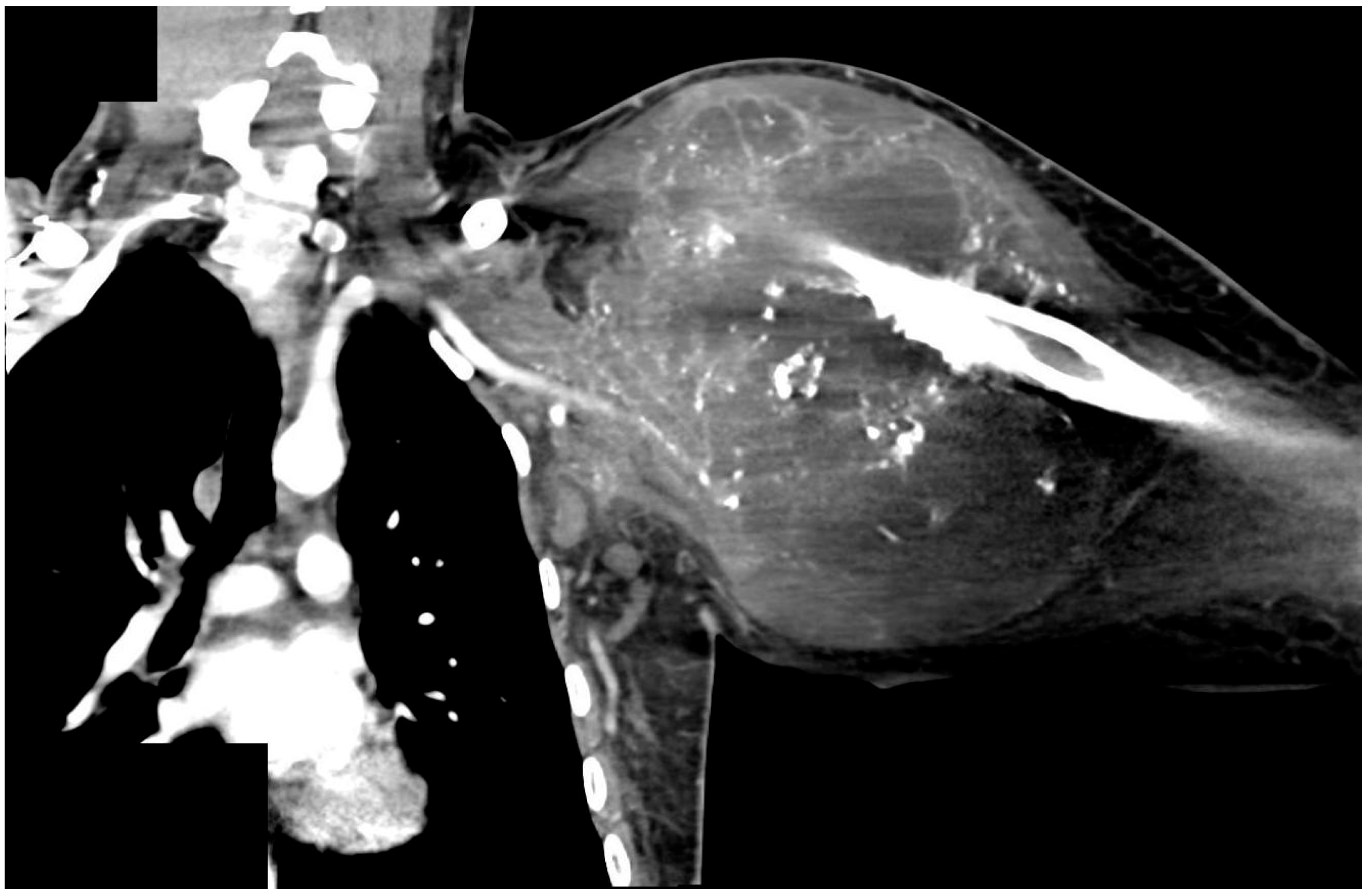
A 25-year-old male patient with a large chondroblastic osteosarcoma of the left upper humerus presented to our hospital and was treated by our multidisciplinary sarcoma team (Table 2). The patient was initially diagnosed eight months earlier but unfortunately decided to pursue an alternative treatment with a homeopathic practitioner for three months. When he returned to our hospital, the tumor had increased considerably in size and was staged as cT2 cN0, cM1, infiltrating the glenohumeral joint, the muscles of the upper arm and rotator cuff, as well as the latissimus dorsi and both pectoral muscles (Figure 2). Additionally, three suspect pulmonary lesions, thrombosis of the subclavian, axillar and brachial vein was observed on CT-Angio scans. Due to oligometastasis and the young age of the patient a curative treatment approach was initiated, including neoadjuvant chemotherapy followed by wide tumor resection. Oncological treatment following the protocol of the European and American Osteosarcoma Study Group (EURAMOS-1) was initiated [19,20]. After 6 weeks of chemotherapy, wide resection was conducted. The surgery was performed in an interdisciplinary collaboration of Tumor Orthopedics, Thoracic and Plastic Surgeons. Due to the extent of the sarcoma, an extended FQA, including an atypical lung segment resection and the resection of the first three ribs as well as the complete clavicle, was necessary to allow complete resection. Suspect pulmonary lesions were individually resected by atypical lung resections.
Table 2.
Overview of the presented case using an osteomusculocutaneous fillet flap for defect coverage after FQA.
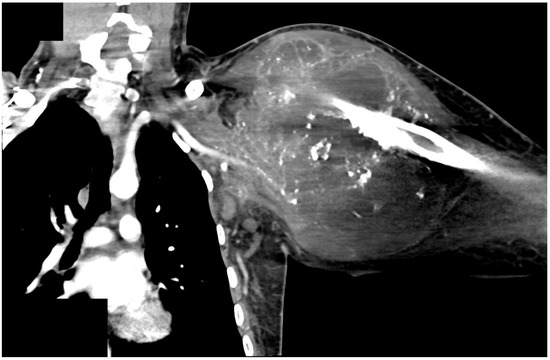
Figure 2.
CT-Scan of a 25 year old male who presented with a chondroblastic osteosarcoma of the left proximal humerus, infiltrating the left glenohumeral joint and the muscles of the upper arm and rotator cuff, including latissimus dorsi and both pectoral muscles (staged at cT2 cN0, and cM1).
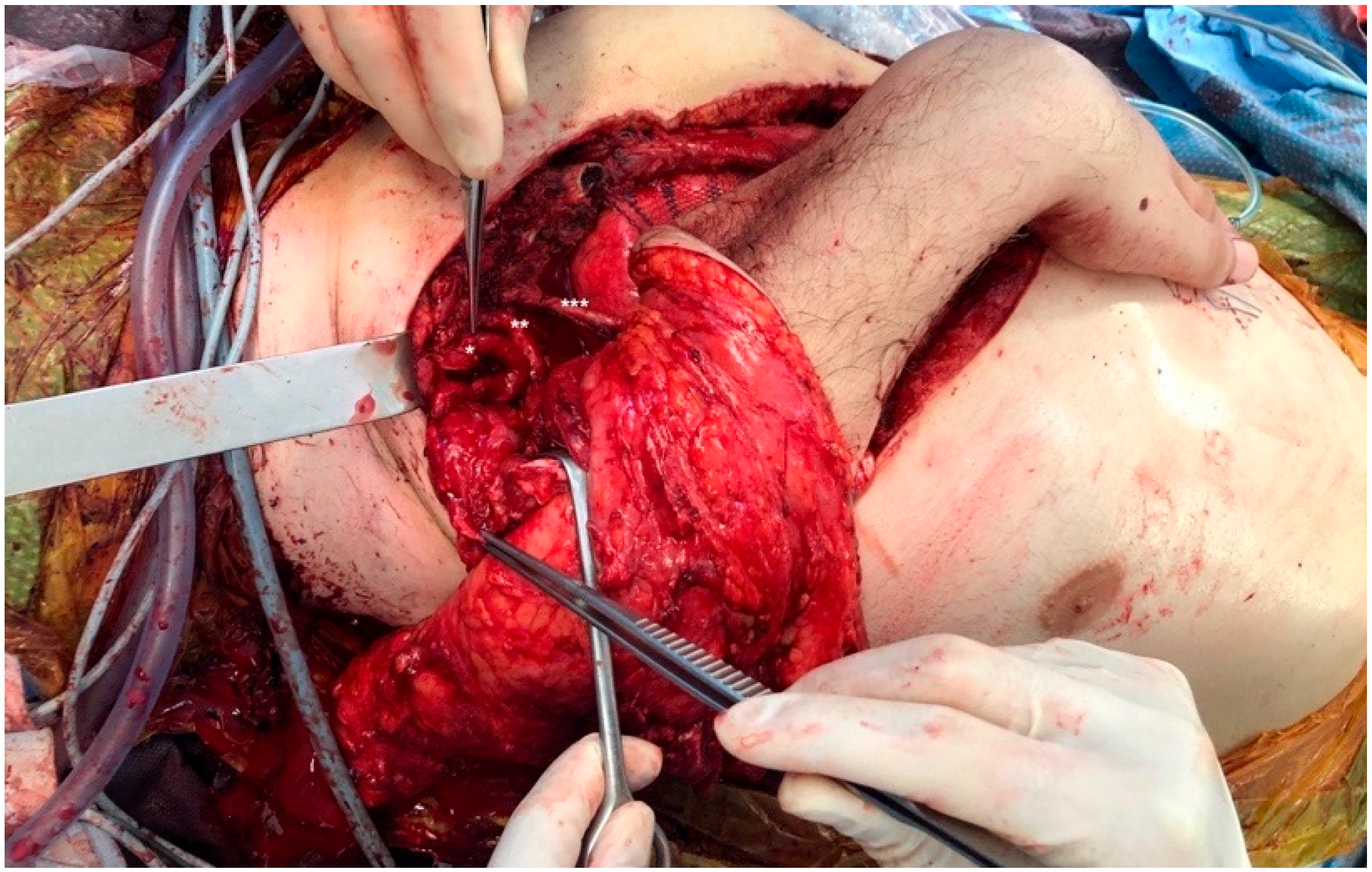
Tumor infiltration into the distal end of the humerus prohibited a reconstructive option that used the elbow joint [17,18]. We therefore decided to use an osteomusculocutaneous free fillet flap from the tumor-free forearm for defect coverage and shoulder contour reconstruction. The flexed wrist and metacarpal bones were incorporated into the flap to create a shoulder contour that would function as a prosthetic socket. The radius and ulna were shortened at the proximal end to a length of 14 cm and the skin and soft tissue were opened longitudinally on the ventral aspect of the forearm. The radius was then attached to the sternum with a plate. Subsequently, microsurgical anastomoses were performed between the brachial artery and thoracoacromial artery and between the cephalic vein and remaining stump of the subclavian vein in end-to-end technique with interrupted sutures (total time of ischemia: 165 min). The metacarpal bones were connected to the lateral thoracic wall using a non-resorbable suture to ensure lateral stability of the construct. TMR was performed by epineural coaptation of the three forearm motor-nerves (i.e., median, radial, and ulnar nerve) to the three trunks of the brachial plexus (Figure 3). The skin and soft tissue of the flap was fitted to the chest wall. The patient was transferred to the intensive-care unit after surgery and was extubated on the following day. Pathology confirmed R0-resection and complete wound healing occurred without infection or tissue loss. The patient was discharged 11 days after surgery.
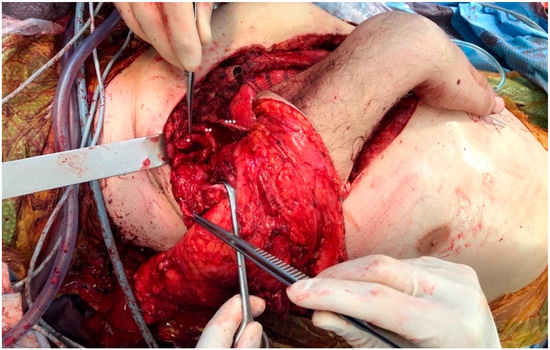
Figure 3.
Intraoperative view of osteomusculocutaneous free fillet flap for defect coverage after forequarter amputation (FQA). The radius (and ulna) was shortened and attached to the sternum with a plate. Microsurgical anastomoses were performed between the brachial artery and thoracoacromial artery, and between the cephalic vein and the remaining stump of the subclavian vein. Subsequently, targeted muscle reinnervation (TMR) by epineural coaptation of the three forearm motor-nerves was performed: the superior trunk was connected to the median nerve (*), the middle trunk to the radial nerve (**), and the inferior trunk to the ulnar nerve (***).
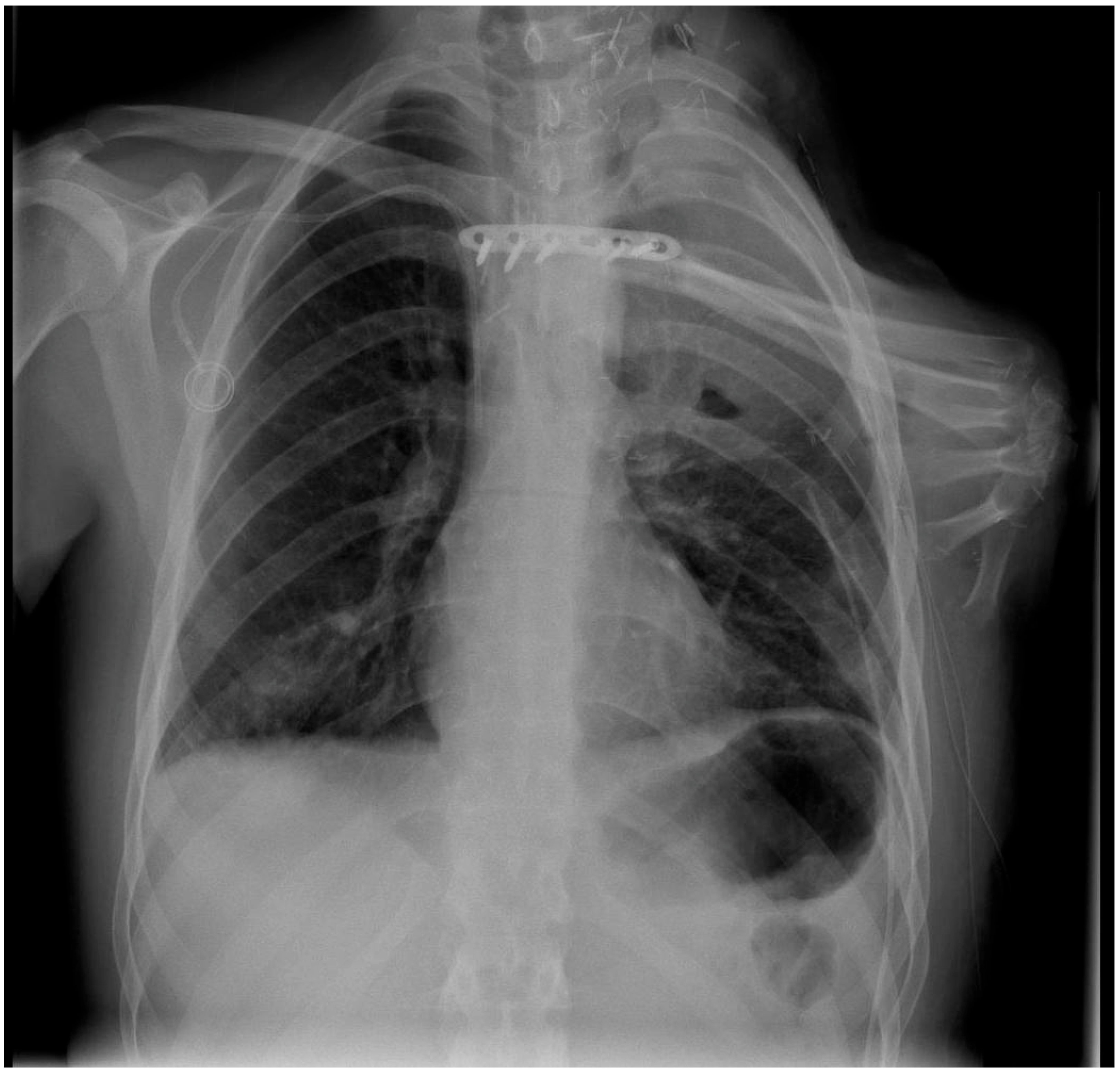
Clinical follow-up showed a solid osseous framework with good protection of the thoracic organs (Figure 4) and an acceptable improvement of the shoulder contour (Figure 5). The patient did not suffer from phantom limb or neuroma pain. Moreover, neurological examination six weeks after surgery showed an increasing tactile sensation of the flap. However, pulmonary and lymph-node metastases occurred during follow-up, resulting in the continuous deterioration of the clinical condition. A palliative therapeutic concept commenced, and the patient died three months after tumor resection.
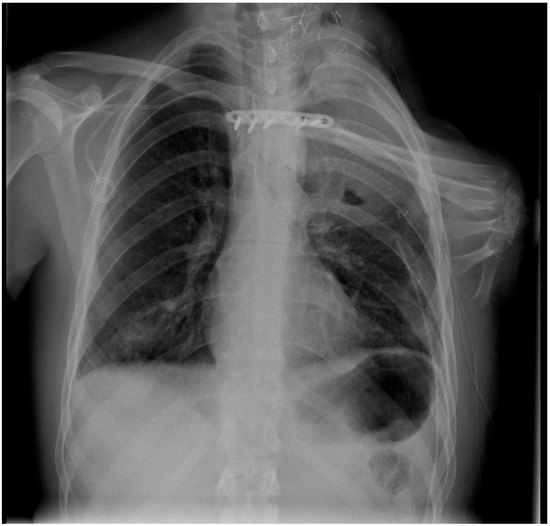
Figure 4.
Osteomusculocutaneous free fillet flap including the tumor-free forearm for defect coverage and shoulder contour reconstruction (radiograph taken one week after surgery). The 90° flexed wrist, as well as the carpal and metacarpal bones, were incorporated into the flap to create a shoulder contour that would function as a prosthetic socket. Plate osteosynthesis was used to attach the sternum to the radius.

Figure 5.
Clinical follow-up six weeks after osteomusculocutaneous free fillet flap defect coverage, including targeted muscle reinnervation (TMR). The results demonstrate an adequate reconstruction of the chest wall integrity, as a well as an improved appearance of the shoulder contour. The patient did not suffer from phantom limb or neuroma pain, and neurological examination showed an increasing tactile sensation of the flap. Due to disease progression in the course of treatment, cutaneous metastasis developed above the left breast.
4. Discussion
Improved reconstructive options and a multimodal treatment of mesenchymal tumors, such as osteosarcomas, enabled limb salvage in the majority of patients [21,22]. Nevertheless, radical tumor resection is usually necessary as inadequate surgical margins are significantly associated with higher local recurrence rates and decreased overall survival of patients [15,16,23]. With regard to locally progressed primary tumors of the proximal upper extremity, limb salvage is not always possible. In these cases, FQA allows for wide resection margins [24]. However, albeit technically feasible, the radical ablation of the arm and the anatomical structures of the shoulder girdle are associated with severe comorbidities, such as possible life-threatening intraoperative hemorrhage, as well as respiratory impairment or even failure [16,25], especially when including the resection of the chest wall and/or parts of the lung [16,26]. Nevertheless, while such a radical procedure has to be carefully assessed for its advisability for each individual patient, FQA allows for wide resection margins and, thus, a curative treatment concept [24,25].
A common consequence of the radical ablation of the arm and the anatomical structures of the shoulder girdle is the requirement of a subsequent microsurgical reconstruction in order to enable adequate defect coverage and wound closure. The “spare-parts concept”, which utilizes tissue from the amputated limb to reconstruct a defect without creating additional donor side morbidity (i.e., fillet flap), is a recognized technique in reconstructive and traumatic surgery [7,15,27,28,29]. Küntscher and colleagues provided a thorough overview of this surgical technique in an extensive study on 104 fillet flaps. The authors classify fillet flaps into pedicled finger and toe, pedicled limb, and free filet flaps [15]. With regard to free fillet flaps used for reconstructive surgery after FQA, flaps have been predominantly described according to their tissue content (fasciocutaneous, musculocutaneous, and osteomusculocutaneous) [5,6]. In contrast to fasciocutaneous and musculocutaneous flaps, the inclusion of bones in the osteomusculocutaneous fillet flap enables restoration of the shoulder silhouette and provides additional stability, as well as protection of the thorax and its inner organs, when using this technique for reconstruction after FQA [5,6,7,30]. Indeed, the reconstruction of the chest wall integrity after extensive resection is of the highest priority as a reduced structural integrity of the chest is associated with paradox respiratory movement and therefore impaired ventilatory function [7,31]. Alternative methods that offer stability, such as the use of alloplastic materials (e.g., synthetic mesh), have been successfully described for the reconstruction of large chest wall defects [32,33]. These often require additional soft tissue coverage, commonly by extensive free flaps in the case of FQA. However, due to the risk of predominantly intraoperative bacterial contamination, these are associated with a higher rate of infection and impaired wound healing [34,35,36,37,38].
Instead of utilizing the amputated limb, local or free flap reconstructive options may be used for defect coverage after FQA. Indeed, several reports exist, which demonstrate the successful use of these techniques, such as the fasciocutaneous deltoid, the tensor fascia latae (TFL), or the TFL + rectus femoris flap [7,39,40]. Similarly, extensive studies have been published regarding the reconstruction of the chest wall using primarily local myocutaneous flaps [41,42,43]. However, in the case of FQA, where the subscapular system is often severed, pedicled flaps like latissimus dorsi, (para)scapular, and serratus flaps become unavailable local options. In addition, when compared to an osteomusculocutaneous fillet flap, these procedures involve additional donor site morbidity, as well as limited stability for the shoulder girdle.
Despite the potential physiological and psychological benefits for the patient, very few cases of osteomusculocutaneous free fillet flaps for chest wall and shoulder reconstruction have been described in previous publications. Our systematic literature search identified four articles that give detailed information on this technique in a total of ten cases (Table 1) [2,16,17,18]. Hitherto published surgical techniques on osteomusculocutaneous free fillet flaps after FQA can be separated into two main subgroups, depending on the choice of bones that were included into the flap—the approach by Steinau et al. as well as the one by Kuhn and colleagues, who described the utilization of the radius and/ or ulna to stabilize the thoracic wall [2,16]. Thus, Steinau et al. reported on three cases in which the proximal forearm was fixated to the remaining parts of the clavicle or the sternum with the distal ends of the radius and ulna being attached to the thoracic wall [2]. Two years later, Kuhn et al. published a case report describing the use of the bones and soft-tissue of the forearm to reconstruct the thoracic wall and to allow for mediastinal protection after extended FQA, including complete anterior and posterior chest wall resection, as well as pneumectomy [16].
In contrast, in their subsequently published articles, Osanai and colleagues as well as Koulaxouzidis et al. described techniques that connect the distal humerus to the clavicle or the sternum (in cases where a complete resection of the clavicle was necessary) and created a lateral prominence that resembles the natural silhouette of the shoulder [17,18,37,44,45]. Thus, Osanai et al. included the flexed elbow joint into the flap to imitate the natural shoulder contour through the eminence of the olecranon [17]. Similarly, Koulaxouzidis et al. also used the elbow joint for shoulder contour reconstruction in a total of four patients [18]. Moreover, this technique also involved the reconstruction of the axillary fold in addition to the shoulder contour. The authors avoided large scale soft-tissue separation to preserve the outline of the elbow, and the cubital skin crease was thus used to recreate the axilla.
The results illustrate that the functional and cosmetic outcomes are highly dependent on the location and extent of the tumor or trauma. Local tumor progression of our patient required the resection of the complete clavicle, scapula, and the first three ribs. The upper arm had to be excluded from the flap to accomplish tumor free margins, permitting the previously published surgical approach that incorporates the elbow joint into the flap [17,18].
Thus, our surgical options were limited to the utilization of the forearm and the hand, as the osteomusculocutaneous free flap for the reconstruction of the thoracic wall and shoulder. Therefore, we decided to use a new surgical approach—by connecting the radius to the sternum, we were able to utilize the flexed wrist instead of the elbow joint to imitate the natural shoulder contour (Table 2). Short-term follow-up of the patient revealed limited appearance of the shoulder silhouette; however, sufficient protection of the thoracic organs through the osseous framework of the flap, and good anatomical conditions for attachment of a socket prosthesis. Consequently, we present a third subgroup of osteomusculocutaneous fillet flaps for reconstruction with “spare-parts” after FQA that incorporates the bones of the forearm, wrist, and metacarpus. Unfortunately, we cannot provide long-term results using this technique due to the rapid development of metastatic disease, resulting in the patient’s death three months after surgery.
Common complications following extremity amputation are the occurrence of phantom limb pain and the development of neuromas [11]. The prevalence of phantom limb pain ranges between 45 and 85%, and typically displays two peaks in its incidence: one month and one year after amputation [46,47]. The concept of TMR was initially developed to enable advanced control of myoelectric prostheses, but has also shown to significantly reduce phantom pain and neuroma formation after limb amputation [13,47]. To exploit these features, we connected the trunks of the brachial plexus to the forearm nerves in the fillet flap. The epineural end-to-end coaptation required only a little extra time due to the large caliber of the peripheral nerves and was completed within 35 min. The patient did not develop any phantom limb or neuroma pain during the follow-up period. These findings provide new data on the feasibility and possible functional improvement of phantom pain management in patients who undergo fillet flap reconstruction after FQA. While the validity of our results is significantly limited due to the short observation period and single-case experience, previous studies have demonstrated the high effectiveness of TMR when performed as a preemptive measure, as well as when used as a treatment option for patients with postamputation pain [48,49,50,51]. Indeed, Mioton and colleagues demonstrated significant improvements of residual limb and phantom limb pain parameters in 33 patients with major limb amputations due to TMR one year after treatment [49]. Moreover, in a recent prospective randomized clinical trial, TMR was shown to reduce chronic pain in amputees when compared with the gold standard (excision and muscle burying) [48]. Similar results were shown by Valerio et al. when implementing TMR as a preemptive measure to reduce chronic postamputation pain [50]. In their multi-institutional cohort study, the authors demonstrated that patients who underwent TMR had less phantom and residual limb pain when compared with untreated amputee controls. This effect was shown across all subgroups. Considering these previous findings and also the outcome of our presented case, a high benefit to cost ratio of TMR along with fillet-flap reconstruction after FQA seems highly likely.
In the majority of reports, including our own case, tumor infiltration of the shoulder girdle or chest wall was the indication for FQA. Using the “spare-parts” of an extremity that was impaired by local cancerous progression asks the question of whether this procedure is a safe oncological approach. In this context, the fillet flap technique uses the identical principle of the resection–replantation technique reported by Windhager et al. [52]. The authors resected the tumor-bearing area of the upper extremity and replanted the distal part of the arm to the proximal stump. None of the 12 patients developed a local recurrence within the follow-up period. Furthermore, a different study by Ver Halen et al. described 27 soft tissue fillet flaps from the upper and lower extremity after soft tissue malignancies; none of the patients developed cancer recurrence within the flap itself, supporting the thesis that the fillet flap technique is oncologically safe [29].
However, in cases where FQA may be prevented or primary wound closure is possible, the overall prognosis of this special patient group must be taken into account, in particular when considering osteomusculocutaneous fillet flap reconstruction after FQA due to sarcoma. Even if primary tumor resection is successful, the disease-free five year survival of sarcoma patients requiring FQA is below 30% [53]. While Steinau et al. advocated that the use of osteomusculocutaneous fillet flaps even applies to a palliative reconstruction, the apparent limitations of ultra-radical interdisciplinary oncological surgery, albeit technically feasible, have to be critically reflected [2,25]. This holds true, in particular, when considering previously reported long-term impairment of respiratory function and of quality of life in patients with chest wall resection, as well as the significantly increased depressive symptoms of family members that often need to be consulted in the course of the intensive care treatment of critically ill patients [25,54,55].
Therefore, we advocate that the indication for FQA has to be individually considered and carefully evaluated with each patient after case discussion in a specialized interdisciplinary tumor board (if applicable, i.e., if FQA is considered to treat an underlying malignancy). However, if this process concludes that FQA is the best treatment option, radical tumor resections and subsequent osteomusculocutaneous fillet flap reconstruction, including TMR (when manageable in limited additional operating time), should be the first choice of surgical treatment.
5. Conclusions
In case of FQA and the need for free flap reconstruction, we consider the osteomusculocutaneous free fillet flap as the first choice. It enables the reconstruction of the chest wall integrity, provides support for a prosthesis socket, and improves the appearance of the shoulder contour. When using this technique, the remaining anatomical structures of the thorax, the vascular supply, and the distal resection margin of the amputated upper extremity are crucial components that have to be considered when the overall design of the flap is determined. If the inclusion of the elbow joint into the flap is not possible due to local tumor expansion or trauma, we recommend the use of the forearm and hand, as described. In general, we advocate for the additional implementation of TMR, as it can be performed quickly and is likely to reduce the occurrence of phantom limb and neuroma pain. However, the reviewed case series, as well as our own experience, emphasize that patients require careful evaluation of the benefit of FQA, as well as an individual solution for reconstructive surgery if the procedure is deemed to be the best possible option.
Author Contributions
Conceptualization, D.E., C.P.S., H.R.D., D.B. and R.E.G.; methodology, N.W. and C.K.; validation, D.E., D.B., C.K. and N.W.; investigation, N.W. and C.K.; resources, R.E.G., C.P.S. and H.R.D.; data curation, D.E., D.B., C.K. and N.W.; writing—original draft preparation, N.W., C.K. and D.B.; writing—review and editing, D.E. and R.E.G.; visualization, N.W.; supervision, R.E.G., C.P.S. and H.R.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the anonymous case presentation in the article. A written consent was secured from the patient before publication.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Isakoff, M.S.; Bielack, S.S.; Meltzer, P.; Gorlick, R. Osteosarcoma: Current Treatment and a Collaborative Pathway to Success. J. Clin. Oncol. 2015, 33, 3029–3035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinau, H.U.; Germann, G.; Klein, W.; Roehrl, S.P.; Josten, C. The “Epaulette” Flap: Replantation of Osteomyocutaneous Forearm Segments in Interscapulothoracic Amputations. Eur. J. Plast. Surg. 1992, 15, 283–288. [Google Scholar] [CrossRef]
- Anbarasan, A.; Mohamad, N.H.; Mariapan, S. Open Traumatic Scapulothoracic Dissociation: Case Report of a Rare Injury. Trauma Case Rep. 2018, 18, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Wittig, J.C.; Bickels, J.; Kollender, Y.; Kellar-Graney, K.L.; Meller, I.; Malawer, M.M. Palliative Forequarter Amputation for Metastatic Carcinoma to the Shoulder Girdle Region: Indications, Preoperative Evaluation, Surgical Technique, and Results. J. Surg. Oncol. 2001, 77, 105–113. [Google Scholar] [CrossRef]
- Ayyala, H.S.; Mohamed, O.M.; Therattil, P.J.; Lee, E.S.; Keith, J.D. The Forearm Fillet Flap: ‘Spare Parts’ Reconstruction for Forequarter Amputations. Case Rep. Plast. Surg. Hand Surg. 2019, 6, 95–98. [Google Scholar] [CrossRef]
- Cordeiro, P.G.; Cohen, S.; Burt, M.; Brennan, M.F. The Total Volar Forearm Musculocutaneous Free Flap for Reconstruction of Extended Forequarter Amputations. Ann. Plast. Surg. 1998, 40, 388–396. [Google Scholar] [CrossRef]
- Tukiainen, E.; Barner-Rasmussen, I.; Popov, P.; Kaarela, O. Forequarter Amputation and Reconstructive Options. Ann. Plast. Surg. 2020, 84, 651–656. [Google Scholar] [CrossRef]
- Pierrie, S.N.; Gaston, R.G.; Loeffler, B.J. Current Concepts in Upper-Extremity Amputation. J. Hand Surg. Am. 2018, 43, 657–667. [Google Scholar] [CrossRef]
- Mioton, L.M.; Dumanian, G.A. Targeted Muscle Reinnervation and Prosthetic Rehabilitation after Limb Loss. J. Surg. Oncol. 2018, 118, 807–814. [Google Scholar] [CrossRef]
- Bowen, J.B.; Ruter, D.; Wee, C.; West, J.; Valerio, I.L. Targeted Muscle Reinnervation Technique in Below-Knee Amputation. Plast. Reconstr. Surg. 2019, 143, 309–312. [Google Scholar] [CrossRef]
- Bowen, J.B.; Wee, C.E.; Kalik, J.; Valerio, I.L. Targeted Muscle Reinnervation to Improve Pain, Prosthetic Tolerance, and Bioprosthetic Outcomes in the Amputee. Adv. Wound Care 2017, 6, 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheesborough, J.E.; Smith, L.H.; Kuiken, T.A.; Dumanian, G.A. Targeted Muscle Reinnervation and Advanced Prosthetic Arms. Semin. Plast. Surg. 2015, 29, 62–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elmaraghi, S.; Albano, N.J.; Israel, J.S.; Michelotti, B.F. Targeted Muscle Reinnervation in the Hand: Treatment and Prevention of Pain After Ray Amputation. J. Hand Surg. Am. 2019, 45, 884.e1–884.e6. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [Green Version]
- Küntscher, M.V.; Erdmann, D.; Homann, H.H.; Steinau, H.U.; Levin, S.L.; Germann, G. The Concept of Fillet Flaps: Classification, Indications, and Analysis of Their Clinical Value. Plast. Reconstr. Surg. 2001, 108, 885–896. [Google Scholar] [CrossRef]
- Kuhn, J.A.; Wagman, L.D.; Lorant, J.A.; Grannis, F.W.; Dunst, M.; Dougherty, W.R.; Jacobs, D.I. Radical Forequarter Amputation with Hemithoracectomy and Free Extended Forearm Flap: Technical and Physiologic Considerations. Ann. Surg. Oncol. 1994, 1, 353–359. [Google Scholar] [CrossRef]
- Osanai, T.; Kashiwa, H.; Ishikawa, A.; Takahara, M.; Ogino, T. Improved Shoulder Contour Following Forequarter Amputation with an Osteomyocutaneous Free Flap from the Amputated Extremity: Two Cases. Br. J. Plast. Surg. 2005, 58, 165–169. [Google Scholar] [CrossRef]
- Koulaxouzidis, G.; Simunovic, F.; Stark, G.B. Shoulder Silhouette and Axilla Reconstruction with Free Composite Elbow Tissue Transfer Following Interscapulothoracic Amputation. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 81–86. [Google Scholar] [CrossRef]
- Bielack, S.S.; Werner, M.; Tunn, P.U.; Helmke, K.; Jürgens, H.; Calaminus, G.; Gerss, J.; Butterfass-Bahloul, T.; Reichardt, P.; Smeland, S.; et al. Methotrexate, Doxorubicin, and Cisplatin (MAP) plus Maintenance Pegylated Interferon Alfa-2b versus MAP Alone in Patients with Resectable High-Grade Osteosarcoma and Good Histologic Response to Preoperative MAP: First Results of the EURAMOS-1 Good Respons. J. Clin. Oncol. 2015, 33, 2279–2287. [Google Scholar] [CrossRef]
- Marina, N.; Bielack, S.; Whelan, J.; Smeland, S.; Krailo, M.; Sydes, M.R.; Butterfass-Bahloul, T.; Calaminus, G.; Bernstein, M. International Collaboration Is Feasible in Trials for Rare Conditions: The EURAMOS Experience. Cancer Treat. Res. 2009, 152, 573–575. [Google Scholar] [CrossRef]
- Lehnhardt, M.; Hirche, C.; Daigeler, A.; Goertz, O.; Ring, A.; Hirsch, T.; Drücke, D.; Hauser, J.; Steinau, H.U. Weichgewebssarkome Der Oberen Extremität: Analyse Prognoserelevanter Faktoren Bei 160 Patienten. Chirurg 2012, 83, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Zeller, J.; Kiefer, J.; Braig, D.; Winninger, O.; Dovi-Akue, D.; Herget, G.W.; Stark, G.B.; Eisenhardt, S.U. Efficacy and Safety of Microsurgery in Interdisciplinary Treatment of Sarcoma Affecting the Bone. Front. Oncol. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez-brouchet, A.; Mascard, E.; Siegfried, A.; De Pinieux, G.; Gaspar, N.; Bouvier, C.; Aubert, S.; Marec-bérard, P.; Piperno-neumann, S.; Marie, B.; et al. Assessment of Resection Margins in Bone Sarcoma Treated by Neoadjuvant Chemotherapy: Literature Review and Guidelines of the Bone Group ( GROUPOS ) of the French Sarcoma Group and Bone Tumor Study Group (GSF-GETO/RESOS). Orthop. Traumatol. Surg. Res. 2019, 105, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Elsner, U.; Henrichs, M.; Gosheger, G.; Dieckmann, R.; Nottrott, M.; Hardes, J.; Streitbürger, A. Forequarter Amputation: A Safe Rescue Procedure in a Curative and Palliative Setting in High-Grade Malignoma of the Shoulder Girdle. World J. Surg. Oncol. 2016, 14, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Dragu, A.; Hohenberger, W.; Lang, W.; Schmidt, J.; Horch, R.E. Forequarter amputation of the right upper chest: Limitations of ultra radical interdisciplinary oncological surgery. Chirurg 2011, 82, 834–838. [Google Scholar] [CrossRef]
- O’Connor, B.; Collins, F.J. The Management of Chest Wall Resection in a Patient with Polyostotic Fibrous Dysplasia and Respiratory Failure. J. Cardiothorac. Vasc. Anesth. 2009, 23, 518–521. [Google Scholar] [CrossRef]
- Jakubietz, R.G.; Jakubietz, M.G.; Kloss, D.F.; Gruenert, J.G. Combination of a Total Free Forearm Flap and a Sensate Local Flap for Preservation of the Shoulder Girdle in Massive, Nonreplantable Upper Extremity Injuries. J. Trauma Acute Care Surg. 2009, 66, 561–563. [Google Scholar] [CrossRef]
- Scaglioni, M.F.; Lindenblatt, N.; Barth, A.A.; Fuchs, B.; Weder, W.; Giovanoli, P. Free Fillet Flap Application to Cover Forequarter or Traumatic Amputation of an Upper Extremity: A Case Report. Microsurgery 2016, 36, 700–704. [Google Scholar] [CrossRef]
- Ver Halen, J.P.; Yu, P.; Skoracki, R.J.; Chang, D.W. Reconstruction of Massive Oncologic Defects Using Free Fillet Flaps. Plast. Reconstr. Surg. 2010, 125, 913–922. [Google Scholar] [CrossRef]
- Steinau, H.U.; Germann, G.; Klein, W.; Josten, C. The Epaulette Flap: Replantation of Osteomyocutaneous Forearm Segments in Interscapulo-Thoracic Amputation. Chirurg 1992, 63, 368–372. [Google Scholar]
- Netscher, D.T.; Baumholtz, M.A. Chest Reconstruction: I. Anterior and Anterolateral Chest Wall and Wounds Affecting Respiratory Function. Plast. Reconstr. Surg. 2009, 124, 240–252. [Google Scholar] [CrossRef] [PubMed]
- Gonfiotti, A.; Santini, P.F.; Campanacci, D.; Innocenti, M.; Ferrarello, S.; Caldarella, A.; Janni, A. Malignant Primary Chest-Wall Tumours: Techniques of Reconstruction and Survival. Eur. J. Cardio-Thorac. Surg. 2010, 38, 39–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lardinois, D.; Müller, M.; Furrer, M.; Banic, A.; Gugger, M.; Krueger, T.; Ris, H.B. Functional Assessment of Chest Wall Integrity after Methylmethacrylate Reconstruction. Ann. Thorac. Surg. 2000, 69, 919–923. [Google Scholar] [CrossRef]
- Arnold, P.G.; Pairolero, P.C. Chest-Wall Reconstruction: An Account of 500 Consecutive Patients. Plast. Reconstr. Surg. 1996, 98, 804–810. [Google Scholar] [CrossRef]
- Hazel, K.; Weyant, M.J. Chest Wall Resection and Reconstruction: Management of Complications. Thorac. Surg. Clin. 2015, 25, 517–521. [Google Scholar] [CrossRef]
- Huang, H.; Kitano, K.; Nagayama, K.; Nitadori, J.I.; Anraku, M.; Murakawa, T.; Nakajima, J. Results of Bony Chest Wall Reconstruction with Expanded Polytetrafluoroethylene Soft Tissue Patch. Ann. Thorac. Cardiovasc. Surg. 2015, 21, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.; Shen, K.R. Primary Tumors of the Osseous Chest Wall and Their Management. Thorac. Surg. Clin. 2017, 27, 181–193. [Google Scholar] [CrossRef]
- Dietz, U.A.; Spor, L.; Germer, C.-T. Management of mesh-related infections. Chirurg. 2011, 82, 208–217. [Google Scholar] [CrossRef]
- Volpe, C.M.; Peterson, S.; Doerr, R.J.; Karakousis, C.P. Forequarter Amputation with Fasciocutaneous Deltoid Flap Reconstruction for Malignant Tumors of the Upper Extremity. Ann. Surg. Oncol. 1997, 4, 298–302. [Google Scholar] [CrossRef]
- Ferrario, T.; Palmer, P.; Karakousis, C.P. Technique of Forequarter (Interscapulothoracic) Amputation. Clin. Orthop. Relat. Res. 2004, 423, 191–195. [Google Scholar] [CrossRef]
- Skoracki, R.J.; Chang, D.W. Reconstruction of the Chestwall and Thorax. J. Surg. Oncol. 2006, 94, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Lasso, J.M.; Uceda, M.; Peñalver, R.; Moreno, N.; Casteleiro, R.; Cano, R.P. Large Posterior Chest Wall Defect Reconstructed with a De-Epithelised Trans-Thoracic TRAM Flap. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, e458-62. [Google Scholar] [CrossRef] [PubMed]
- Kishi, K.; Imanishi, N.; Ninomiya, R.; Okabe, K.; Ohara, H.; Hattori, N.; Nakajima, H.; Nakajima, T. A Novel Approach to Thoracic Wall Reconstruction Based on a Muscle Perforator. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, 1289–1293. [Google Scholar] [CrossRef] [PubMed]
- Hubmer, M.; Leithner, A.; Kamolz, L.P. Re: Shoulder Silhouette and Axilla Reconstruction with Free Composite Elbow Tissue Transfer Following Interscapulothoracic Amputation. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, e232–e233. [Google Scholar] [CrossRef]
- Wilks, D.J.; Hassan, Z.; Bhasker, D.; Kay, S.P.J. Re: Shoulder Silhouette and Axilla Reconstruction with Free Composite Elbow Tissue Transfer Following Interscapulothoracic Amputation. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 1162–1164. [Google Scholar] [CrossRef]
- Kuffler, D.P. Coping with Phantom Limb Pain. Mol. Neurobiol. 2018, 55, 70–84. [Google Scholar] [CrossRef]
- Luo, Y.; Anderson, T.A. Phantom Limb Pain A Review of the Literature. Int. Anesthesiol. Clin. 2016, 54, 121–139. [Google Scholar] [CrossRef]
- Dumanian, G.A.; Potter, B.K.; Mioton, L.M.; Ko, J.H.; Cheesborough, J.E.; Souza, J.M.; Ertl, W.J.; Tintle, S.M.; Nanos, G.P.; Valerio, I.L.; et al. Targeted Muscle Reinnervation Treats Neuroma and Phantom Pain in Major Limb Amputees: A Randomized Clinical Trial. Ann. Surg. 2019, 270, 238–246. [Google Scholar] [CrossRef]
- Mioton, L.M.; Dumanian, G.A.; Shah, N.; Qiu, C.S.; Ertl, W.J.; Potter, B.K.; Souza, J.M.; Valerio, I.L.; Ko, J.H.; Jordan, S.W. Targeted Muscle Reinnervation Improves Residual Limb Pain, Phantom Limb Pain, and Limb Function: A Prospective Study of 33 Major Limb Amputees. Clin. Orthop. Relat. Res. 2020, 478, 2161–2167. [Google Scholar] [CrossRef]
- Valerio, I.L.; Dumanian, G.A.; Jordan, S.W.; Mioton, L.M.; Bowen, J.B.; West, J.M.; Porter, K.; Ko, J.H.; Souza, J.M.; Potter, B.K. Preemptive Treatment of Phantom and Residual Limb Pain with Targeted Muscle Reinnervation at the Time of Major Limb Amputation. J. Am. Coll. Surg. 2019, 228, 217–226. [Google Scholar] [CrossRef] [Green Version]
- Souza, J.M.; Cheesborough, J.E.; Ko, J.H.; Cho, M.S.; Kuiken, T.A.; Dumanian, G.A. Targeted Muscle Reinnervation: A Novel Approach to Postamputation Neuroma Pain. Clin. Orthop. Relat. Res. 2014, 472, 2984–2990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Windhager, R.; Millesi, H.; Kotz, R. Resection-Replantation for Primary Malignant Tumours of the Arm. An Alternative to Fore-Quarter Amputation. J. Bone Joint Surg. Br. 1995, 77, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Rickelt, J.; Hoekstra, H.; Van Coevorden, F.; De Vreeze, R.; Verhoef, C.; Van Geel, A.N. Forequarter Amputation for Malignancy. Br. J. Surg. 2009, 96, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Heuker, D.; Lengele, B.; Delecluse, V.; Weynand, B.; Liistro, G.; Balduyck, B.; Noirhomme, P.; Poncelet, A.J. Subjective and Objective Assessment of Quality of Life after Chest Wall Resection. Eur. J. Cardio-Thorac. Surg. 2011, 39, 102–108. [Google Scholar] [CrossRef]
- Hickman, R.L.J.; Daly, B.J.; Douglas, S.L.; Clochesy, J.M. Informational Coping Style and Depressive Symptoms in Family Decision Makers. Am. J. Crit. Care 2010, 19, 410–420. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).