
Effects of a Cognitive Stimulation Program in Institutionalized Patients with Dementia

 ,
,  ,
, 
Abstract
1. Introduction
2. Material and Methods
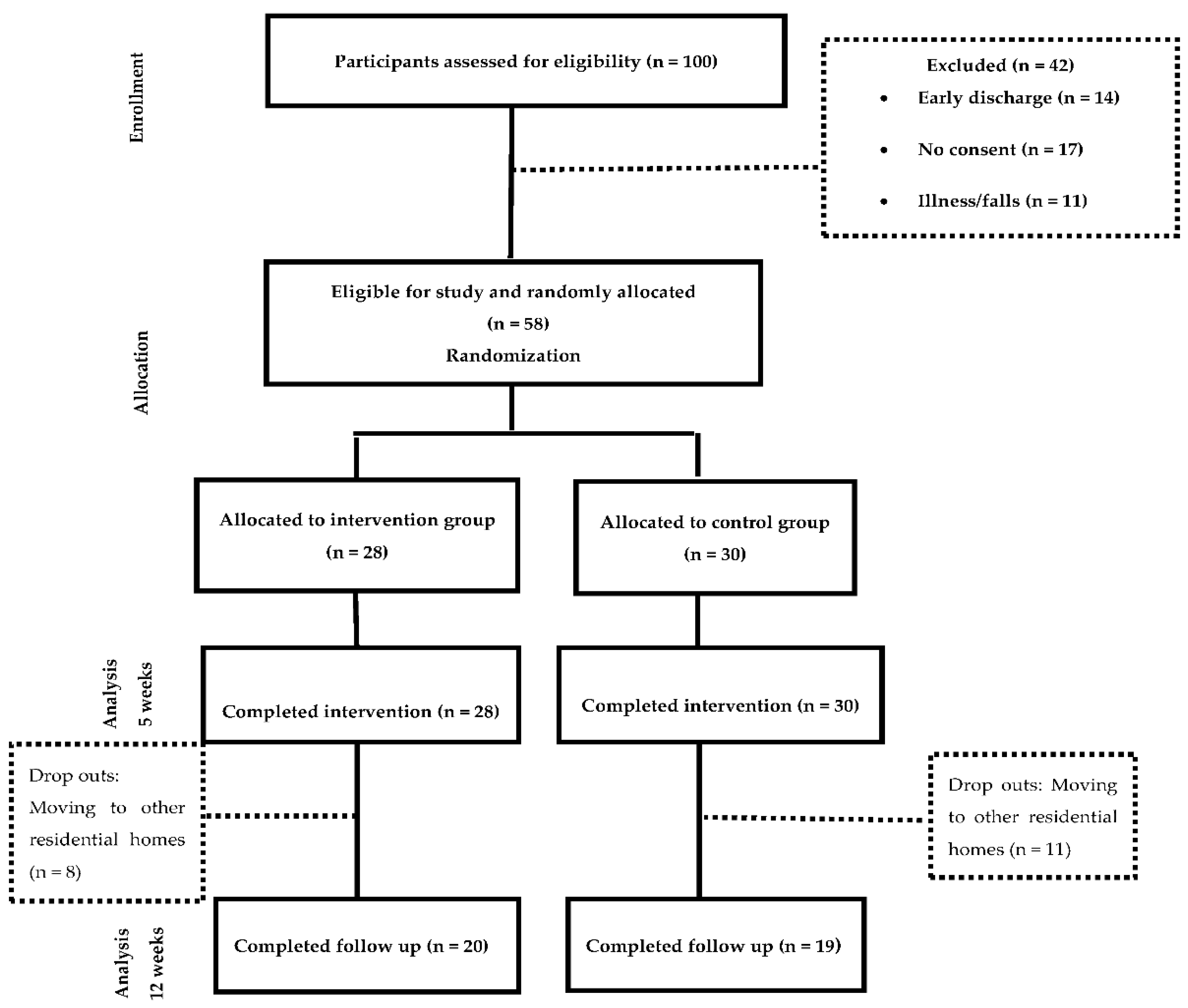
2.1. Study Design
2.2. Participants
2.3. Procedure and Interventions
2.4. Outcome Measures and Data Collection
2.5. Statistical Analysis
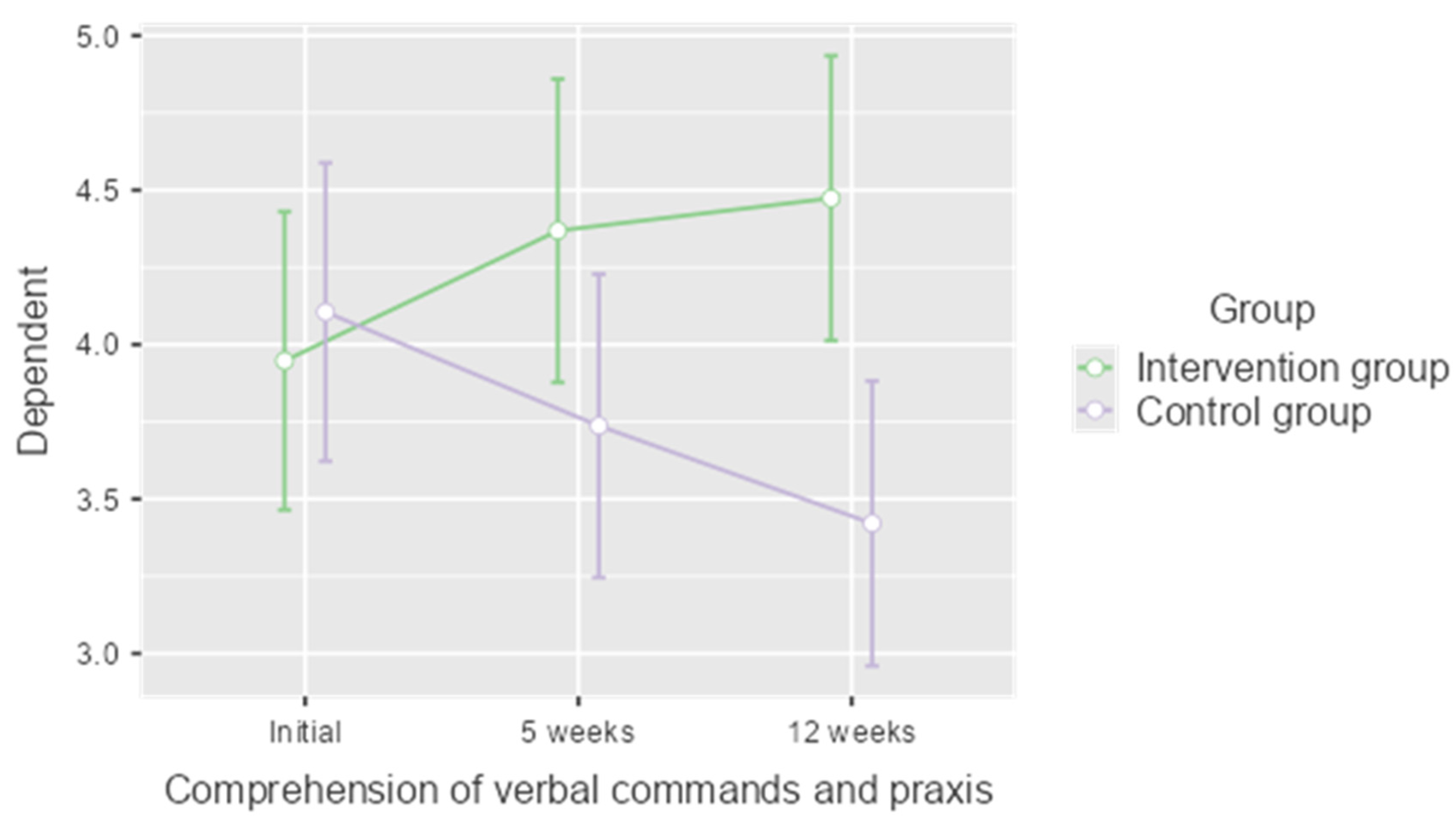
3. Results
4. Discussion
5. Clinical Implications
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Asociación Americana de Psiquiatría. DSM-5 Manual Diagnóstico y Estadístico de Los. Trastornos Mentales, 5th ed.; Panamericana E: Madrid, Spain, 2014. [Google Scholar]
- Custodio, N.; Montesinos, R.; Alarcón, J.O. Evolución histórica del concepto y criterios actuales para el diagnóstico de demencia. Rev. Neuropsiquiatr. 2018, 81, 235–249. [Google Scholar] [CrossRef]
- Alzheimer’s Disease International. The Global Impact of Dementia. An analysis of prevalence, Incidence, Cost and Trends. In World Alzheimer Report 2015; Alzheimer’s Disease International: London, UK, 2015; Available online: https://www.alzint.org/u/WorldAlzheimerReport2015.pdf (accessed on 10 June 2019).
- Galende, A.V.; Ortiz, M.E.; Velasco, S.L.; Luque, M.L.; Miguel, C.L.D.S.D.; Jurczynska, C.P. Informe de la Fundación del Cerebro. Impacto social de la enfermedad de Alzheimer y otras demencias. Neurología 2021, 36, 39–49. [Google Scholar]
- Ramos, P.; Serrano, P.; Ribera, J.M.; Bermejo, F.; Vega, S.; Gil, P. La Enfermedad de Alzheimer y Otras Demencias Detección y Cuidados en las Personas Mayores. Madrid. 2007. Available online: https://fiapam.org/wp-content/uploads/2013/12/235-comunidadmadrid-enfermedad-011.pdf (accessed on 11 May 2019).
- Clare, L.; Woods, R.T.; Moniz, E.D.; Orrell, M.; Spector, A. Rehabilitación Cognitive y Entrenamientos Cognitive Para la Enfermedad de Alzheimer y la Demencia Vascular de Estadío Temprano. Cochrane Database of Systematic Reviews Review. 2008. Available online: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD003260/full/es (accessed on 11 May 2019). [CrossRef]
- Cordero, P.R.; Yubero, R. Tratamiento no farmacologico del deterioro cognitivo. Rev. Esp. Geriatr. Gerontol. 2016, 51, 12–21. [Google Scholar] [CrossRef]
- Lorenzo, J.; Fontan, L. La rehabilitación de los trastornos congitivos. Rev. Med. Urug. 2001, 17, 133–139. [Google Scholar]
- Gay, F.J.; González, V.; Pablos, C. Guía de Orientación en la Práctica Profesional de la Valoración Reglamentaria de la Situación de Dependencia en Personas con Enfermedad de Alzheimer y otras Demencias. 2011. Available online: https://fiapam.org/wpcontent/uploads/2012/10/GuiaOrientacion.pdf (accessed on 11 May 2019).
- Zamarrón, M.D.; Tárraga, L.; Fernández, R. Plasticidad cognitiva en personas con la enfermedad de Alzheimer que reciben programas de estimulación cognitiva. Psicothema 2008, 20, 432–437. [Google Scholar]
- Gómez, I.; Andrés, E.M.; Gómez, A.; Peralta, P. Análisis del efecto a largo plazo de un programa de estimulación cognitiva en mayores con deterioro cognitivo leve en atención primaria: Ensayo controlado aleatorizado. Atención Primaria 2021, 53, 102053. [Google Scholar] [CrossRef]
- Clare, L.; Woods, R.T. Cognitive training and cognitive rehabilitation for people with early-stage Alzheimer‘s disease: A review. Neuropsychol. Rehabil. 2004, 14, 385–401. [Google Scholar] [CrossRef]
- Franco, M.A.; Orihuela, T.; Buenos, Y.; Cid, T. Programa Gradior. In Programa de Evaluación y Rehabilitación Cognitiva Por Ordenador; Edintras: Valladolid, Spain, 2000. [Google Scholar]
- Martínez, T. Estimulación Cognitiva: Guía y Material para la Intervención. In Asturias (España): Gobierno del Principado de Asturias; Consejería de Asuntos Sociales: Asturias, Spain, 2002. [Google Scholar]
- Montejo, P.; Montenegro, M.; Reinoso, A.I.; De Andrés, M.E.; Claver, M.D. Programa de Memoria; Ayuntamiento de Madrid: Madrid, Spain, 1997. [Google Scholar]
- Tárraga, L. Programa de Psicoestimulación Integral (PPI). Tratamientos de psicoestimulación. In Libro Blanco Sobre la Enfermedad de Alzheimer; Fernández Ballesteros, R., Nicolás, J., Eds.; Obra Social de Caja Madrid: Madrid, Spain, 1991. [Google Scholar]
- Tárraga, L.; Boada, M.; Morera, A.; Domènech, S.; Llorente, A. Volver a empezar. In Ejercicios Prácticos de Estimulación Cognitiva Para Enfermos de Alzheimer; Glosa Ediciones: Barcelona, Spain, 1999. [Google Scholar]
- García, J.; Carro, J. Programa de Actuación Cognitiva Integral en Demencia, 1st ed.; Ministerio de Sanidad, Política Social e Igualdad. Secretaria General de Política Social y Consumo; Instituto de Mayores y Servicios Sociales: Madrid, Spain, 2011. [Google Scholar]
- Matilla-Mora, R.; Martínez-Piédrola, R.M.; Huete, J.F. Eficacia de la terapia ocupacional y otras terapias no farmacológicas en el deterioro cognitivo y la enfermedad de Alzheimer. Rev. Española Geriatría Gerontol. 2016, 51, 349–356. [Google Scholar] [CrossRef]
- Tarraga, L. Tratamiento de psicoestimulación. In Libro Blanco Sobre la Enfermedad de Alzheimer y Trastornos Afines; Fernández-Ballesteros, R., Díez Nicolás, J., Eds.; Editorial Medica-Panamericana: Barcelona, Spain, 2001; pp. 305–323. [Google Scholar]
- Peña-Casanova, J. Activemos la Mente; Fundación La Caixa: Barcelona, Spain, 1999. [Google Scholar]
- Associations of Relatives of Alzheimer’s and other Dementia Patients (Asociaciones de Familiares de Enfermos de Alzheimer y otras Demencias—AFAL). El Baúl de los Recuerdos; AFAL-Fundación la Caixa: Madrid, Spain, 2003. [Google Scholar]
- Fernández, R.; Zamarrón, M.D.; Tárraga, L.; Moya, R.; Iñiguez, J. Cognitive Plasticity in Healthy, Mild Congitive Impairment (MCI) Subjects and Alzheimer‘s Disease Patients: A Research Project in Spain. Eur. Psychol. 2003, 8, 148–159. [Google Scholar] [CrossRef]
- Santos del Riego, S. El ser humano como ser ocupacional. Rehabilitación 2005, 39, 195–200. [Google Scholar] [CrossRef][Green Version]
- Salmon, N. Cognitive stimulation therapy versus acetyl cholinesterase inhibitors for mild to moderate dementia: A latter-day David and Goliath? Br. J. Occup. Ther. 2006, 69, 528–530. [Google Scholar] [CrossRef]
- American Occupational Therapy Association. Occupational therapy practice framework: Domain and process. Am. Occup. Ther. Assoc. 2014, 68 (Suppl. 1), 19–20. Available online: http://www.terapia-ocupacional.org.ar/wp-content/uploads/2014/05/3a-Edicion-Marco-de-Trabajo-2013.pdf (accessed on 14 August 2019).
- Francés, I.; Barandiarán, M.; Marcellán, T.; Moreno, L. Estimulacion psiconognitiva en demencia. Anales. Sis. San. Navar. 2003, 26, 405–422. [Google Scholar]
- Bahar-Fuchs, A.; Martyr, A.; Goh, A.M.; Sabates, J.; Clare, L. Entrenamiento cognitivo para personas con demencia leve a moderada. Cochrane Database Syst. Rev. 2019, 3, CD013069. [Google Scholar] [CrossRef]
- Woods, R.; Aguirre, E.; Spector, A.E.; Orrell, M. Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst. Rev. 2012, 2, CD005562. [Google Scholar] [CrossRef]
- Lucinda Aguirre-Cruz, M.; Cruz Aguilera, D.L.; San Juan Orta, D. Líneas de investigación en demencias en el Instituto Nacional de Neurología y Neurocirugía Manuel Velasco Suárez. Arch. Neurocien. (Mex.) 2016, 21 (Suppl. 1), 155–159. [Google Scholar]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. J. Clin. Epidemiol. 2010, 63, e1–e37. [Google Scholar] [CrossRef]
- Boutron, I.; Moher, D.; Altman, D.G.; Schulz, K.F.; Ravaud, P.; CONSORT Group. Extending the CONSORT Statement to Randomized Trials of Nonpharmacologic Treatment: Explanation and Elaboration. Ann. Intern. Med. 2008, 148, 295–309. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; (Text Revised) DSM-IV-TR; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Solís Barrero, C.L.; García Arrioja, S.; Ojeda Manzano, A. Indice de Barthel (IB): Un instrumento esencial para la evaluación funcional y la rehabilitación. Plast Restauración Neurológica 2005, 4, 81–85. Available online: http://www.sld.cu/galerias/pdf/sitios/rehabilitacion/indice_1.pdf (accessed on 18 July 2019).
- Lobo, A.; Sanz, O.; Marcos, G. Revalidación y normalización del mini examen cognoscitivo (primer versión en castellano del Mini Mental Status Examination) en la población general geriátrica. Med. Clin. 1999, 112, 767–774. [Google Scholar]
- Fernandez, E.J.; Sanchez, C.; Monroy, M.L.; Barbero, F.J.; Calvo, J.I. Estudio aleatorizado de un programa de entrenamiento de cognición cotidiana frente a estimulación cognitiva tradicional en adultos mayores. Gerokomos 2018, 29, 65–71. [Google Scholar]
- Tárraga, L. Estrategia no Farmacológica del Deterioro Cerebral Senil y Demencia. Medicine 1994, 6, 44–53. [Google Scholar]
- Reisberg, B.; Ferris, S.H.; De Leon, M.J.; Crook, T. The Global Deterioration Scale for assessment of primary degenerative dementia. Am. J. Psychiatry 1982, 139, 1136–1139. [Google Scholar] [PubMed]
- Broche, Y. Instrumental alternatives for brief cognitive screening of the elderly: Beyond the Minimental Test. Rev. Cuba. Med. Gen. Integr. 2017, 32, 251–257. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-21252017000200010 (accessed on 19 July 2019).
- Lee, C.T. Introductory Biostatistics; Wiley-Interscience: Hoboken, NJ, USA, 2003; pp. 152–153. [Google Scholar]
- Orgeta, V.; McDonald, K.R.; Poliakoff, E.; Hindle, J.V.; Clare, L.; Leroi, I. Cognitive training interventions for dementia and mild cognitive impairment in Parkinson’s disease. Cochrane Database Syst. Rev. 2020, 2, CD011961. [Google Scholar] [CrossRef] [PubMed]
- Chandra, S.R.; Issac, T.G.; Abbas, M.M. Apraxias in Neurodegenerative Dementias. Indian J. Psychol. Med. 2015, 37, 42–47. [Google Scholar] [CrossRef]
- Olazarán, J.; Reisberg, B.; Clare, L.; Cruz, I.; Peña-Casanova, J.; Del Ser, T.; Woods, B.; Beck, C.; Auer, S.; Lai, C.; et al. Nonpharmacological Therapies in Alzheimer’s Disease: A Systematic Review of Efficacy. Dement. Geriatr. Cogn. Disord. 2010, 30, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Villalba, S.; Espert, R. Estimulación cognitiva: Una revisión neuropsicológica. Therapeia 2014, 6, 73–93. [Google Scholar]
- Rubinstein, W.; Politis, D. Estudio sobre la apraxia y las actividades de la vida diaria en relación al grado de severidad de la demencia. In XIII Jornadas de Investigación y Segundo Encuentro de Investigadores en Psicología del Mercosur; Facultad de Psicología—Universidad de Buenos Aires: Buenos Aires, Argentina, 2006. [Google Scholar]
- Breuil, V.; De Rotrou, J.; Forette, F.; Tortrat, D.; Ganansia-Ganem, A.; Frambourt, A.; Moulin, F.; Boller, F. Cognitive stimulation of patients with dementia: Preliminary results. Int. J. Geriatr. Psychiatry 1994, 9, 211–217. [Google Scholar] [CrossRef]
- Spector, A.; Orrell, M.; Davies, S.; Woods, R. Can reality orientation be rehabilitated? Development and piloting of an evidence-based programme of cognition-based therapies for people with dementia. Neuropsychol. Rehabil. 2001, 11, 377–397. [Google Scholar] [CrossRef]
- Bach, D.; Bach, M.; Böhmer, F.; Frühwald, T.; Grilc, B. Reactivating Occupational Therapy: A Method to improve Cognitive Performance in Geriatric Patients. Age Ageing 1995, 24, 222–226. [Google Scholar] [CrossRef]
- Matsuda, O. Cognitive stimulation therapy for Alzheimer’s disease: The effect of cognitive stimulation therapy on the progression of mild Alzheimer’s disease in patients treated with donepezil. Int. Psychogeriatr. 2006, 19, 241–252. [Google Scholar] [CrossRef]
- Chapman, S.B.; Weiner, M.F.; Rackley, A.; Hynan, L.S.; Zientz, J. Effects of Cognitive-Communication Stimulation for Alzheimer’s Disease Patients Treated with Donepezil. J. Speech Lang. Hear. Res. 2004, 47, 1149–1163. [Google Scholar] [CrossRef][Green Version]
- Koh, K.; Ray, R.; Lee, J.; Nair, A.; Ho, T.; Ang, P.C. Dementia in Elderly Patients: Can the 3R Mental Stimulation Programme improve Mental Status? Age Ageing 1994, 23, 195–198. [Google Scholar] [CrossRef]
- Spector, A.; Thorgrimsen, L.; Woods, R.; Royan, L.; Davies, S.; Butterworth, M.; Orrell, M. Efficacy of an evidence-based cognitive stimulation therapy programme for people with dementia. Br. J. Psychiatry 2003, 183, 248–254. [Google Scholar] [CrossRef]
- Woods, R.T.; Thorgrimsen, L.; Spector, A.; Royan, L.; Orrell, M. Improved quality of live and cognitive stimulation in dementia. Aging Ment. Health 2006, 10, 219–226. [Google Scholar] [CrossRef]
- Orrell, M.; Spector, A.; Thorgrimsen, L.; Woods, B. A pilot study examining the effectiveness of maintenance cogni-tive stimulation therapy (MCST) for people with dementia. Int. J. Geriatr. Psychiatry 2005, 20, 446–451. [Google Scholar] [CrossRef]
- Ermini, D.; Meier, D. Memory training: An important part of a “milieu therapy” for patients with senile dementia. Z. Fuer Gerontol. Und Geriatr. 1995, 28, 190–194. [Google Scholar]
- Moore, S.; Sandman, C.A.; McGrady, K.; Kesslak, J.P. Memory training improves cognitive ability in patients with dementia. Neuropsychol. Rehabil. 2001, 11, 245–261. [Google Scholar] [CrossRef]
- Koltai, D.C.; Welsh-Bohmer, K.A.; Smechel, D.E. Influence of anosognosia on treatment outcome among dementia patients. Neuropsychol. Rehabil. 2001, 11, 455–475. [Google Scholar] [CrossRef]
- Kesslak, J.; Nackoul, K.; Sandman, C. Memory training for individuals with Alzheimer’s disease improves name recall. Behav. Neurol. 1997, 10, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, T.; Maurer, K.; Frölich, L. Influence of a memory training program on attention and memory performance of patients with dementia. Z. Fuer Gerontol. Und Geriatr. 2002, 35, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Ermini, D.; Hendriksen, C.; Meier, D.; Regard, M.; Stähelin, H. Entrenamiento cognitivo en pacientes externos con demencia leve: Efectos sobre el estado de ánimo y las funciones cognitivas. In Investigación y Práctica en la Enfermedad de Alzheimer; Fitten, J., Frisoni, G., Vellas, B., Eds.; Glosa Ediciones: Barcelona, Spain, 1998; pp. 221–239. [Google Scholar]
- Tárraga, L. Terapias blandas: Programa de Psicoestimulacion Integral. Alternativa terapéutica para las personas con enfermedad de Alzheimer. Rev. Neurol. 1998, 27, S51–S62. [Google Scholar] [CrossRef]
- Gomez-Soria, I.; Peralta-Marrupe, P.; Plo, F. Cognitive stimulation program in mild cognitive impairment A randomized controlled trial. Dement. Neuropsychol. 2020, 14, 110–117. [Google Scholar] [CrossRef]
- Arroyo, E.M. Estimulación Psicocognoscitiva en las Demencias; Prous Science: Barcelona, Spain, 2002. [Google Scholar]
- Grupo de trabajo de la Guía de Práctica Clínica sobre la atención integral a las personas con enfermedad de Alzheimer y otras demencias. Guía de Práctica Clínica sobre la atención integral a las personas con enfermedad de Alzheimer y otras demencias. In Plan de Calidad para el Sistema Nacional de Salud del Ministerio de Sanidad, Política Social e Igualdad; Agència d’Informació, Avaluació i Qualitat en Salut de Cataluña: Cataluña, Spain, 2010. [Google Scholar]
- Buschert, V.C.; Friese, U.; Teipel, S.J.; Schneider, P.; Merensky, W.; Rujescu, D.; Möller, H.-J.; Hampel, H.; Buerger, K. Effects of a Newly Developed Cognitive Intervention in Amnestic Mild Cognitive Impairment and mild Alzheimer’s disease: A Pilot Study. J. Alzheimer’s Dis. 2011, 25, 679–694. [Google Scholar] [CrossRef]
- Coen, R.F.; Flynn, B.; Rigney, E.; O’Connor, E.; Fitzgerald, L.; Murray, C.; Dunleavy, C.; McDonald, M.; Delaney, D.; Merriman, N.; et al. Efficacy of a cognitive stimulation therapy programme for people with dementia. Ir. J. Psychol. Med. 2011, 28, 145–147. [Google Scholar] [CrossRef]
- Yuill, N.; Hollis, V. A Systematic Review of Cognitive Stimulation Therapy for Older Adults with Mild to Moderate Dementia: An Occupational Therapy Perspective. Occup. Ther. Int. 2011, 18, 163–186. [Google Scholar] [CrossRef]
- Schell, B.A.B.; Gillen, G. Scaffa ESC. Terapia Ocupacional, 12th ed.; Editorial Médica Panamericana: Madrid, Spain, 2016. [Google Scholar]
- Roley, S.S.; DeLany, J.V.; Barrows, C.J.; Brownrigg, S.; Honaker, D.; Sava, D.I.; Talley, V.; Voelkerding, K.; Amini, D.A.; Smith, E.; et al. Occupational Therapy Practice Framework: Domain & Process 2nd Edition. Am. J. Occup. Ther. 2008, 62, 625–683. [Google Scholar] [CrossRef]
- Ciro, C.A.; Anderson, M.P.; Hershey, L.A.; Prodan, C.I.; Holm, M.B. Instrumental Activities of Daily Living Performance and Role Satisfaction in People with and Without Mild Cognitive Impairment: A Pilot Project. Am. J. Occup. Ther. 2015, 69, 6903270020p1–6903270020p10. [Google Scholar] [CrossRef][Green Version]



{kind=link}
{kind=link}
| Demographics/ Clinical Data | Intervention Group | Control Group | p | |||
|---|---|---|---|---|---|---|
| Category | N | % | N | % | ||
| Gender | Male | 8 | 28.6 | 5 | 16.7 | 0.277 a |
| Female | 20 | 71.4 | 25 | 83.3 | ||
| Education level (N = 57) | No studies | 2 | 7.4 | 2 | 6.7 | 0.094 b |
| Primary School | 22 | 81.5 | 28 | 93.3 | ||
| Secondary School | 3 | 11.1 | 0 | 0.0 | ||
| Date of institutionalization | −2008 | 5 | 17.9 | 4 | 13.3 | 0.180 b |
| 2009–2010 | 3 | 10.7 | 9 | 30.0 | ||
| 2011–2012 | 20 | 71.4 | 17 | 56.7 | ||
| Type of dementia | Alzheimer’s | 4 | 14.3 | 8 | 2.7 | 0.127 b |
| Vascular | 6 | 21.4 | 8 | 26.7 | ||
| Mixed | 1 | 3.6 | 2 | 6.7 | ||
| Lewy body | 0 | 0.0 | 2 | 6.7 | ||
| Frontotemporal | 0 | 0.0 | 1 | 3.3 | ||
| Not specified | 17 | 60.7 | 9 | 30.0 | ||
| Neuroleptic treatment (N = 54) | Yes | 10 | 35.7 | 5 | 19.2 | 0.177 a |
| No | 18 | 64.3 | 21 | 80.8 | ||
| Anxiolytic treatment (N = 54) | Yes | 10 | 35.7 | 5 | 19.2 | 0.177 a |
| No | 18 | 64.3 | 21 | 80.8 | ||
| Antidepressive treatment (N = 54) | Yes | 6 | 21.4 | 12 | 46.2 | 0.054 a |
| No | 22 | 78.6 | 14 | 53.8 | ||
| Analgesic treatment (N = 54) | Yes | 0 | 0.0 | 1 | 3.8 | 0.223 b |
| No | 28 | 100 | 25 | 96.2 | ||
| Other treatments of associated pathologies (N = 54) | Yes | 8 | 28.6 | 5 | 19.2 | 0.422 a |
| No | 20 | 71.4 | 21 | 80.8 | ||
| Occupational therapy treatment—cognitive program | Yes | 16 | 57.1 | 21 | 70.0 | 0.309 a |
| No | 12 | 42.9 | 9 | 30.0 | ||
| Occupational therapy treatment—functional rehabilitation program | Yes | 11 | 39.3 | 13 | 43.3 | 0.754 a |
| No | 17 | 60.7 | 17 | 56.7 | ||
| Occupational therapy treatment—ADL | Yes | 28 | 100 | 30 | 100 | * |
| No | 0 | 0.0 | 0 | 0.0 | ||
| Occupational therapy treatment—leisure | Yes | 22 | 78.6 | 28 | 93.3 | 0.098 b |
| No | 6 | 21.4 | 2 | 6.7 | ||
| Occupational therapy treatment—psychomotricity | Yes | 5 | 17.9 | 7 | 23.3 | 0.607 a |
| No | 23 | 82.1 | 23 | 76.7 | ||
| Demographics/Clinical Data | Intervention Group | Control Group | p | |||
| Media | SD | Media | SD | |||
| Age | 84.21 | 7.781 | 81.87 | 6.673 | 0.222 c | |
| Diagnosis of dementia (years) | 3.18 | 2.294 | 4.03 | 3.409 | 0.307 d | |
| Global | Intervention Group | Control Group | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcome Measure | Mean | SD | Z | p * | Mean | SD | Z | p * | Mean | SD | Z | p * |
| Initial LCMT Test | 21.40 | 3.287 | 1.153 | 0.140 | 21.14 | 3.363 | 0.893 | 0.403 | 21.63 | 3.253 | 1.038 | 0.232 |
| Week 5 LCMT Test | 22.64 | 3.582 | 0.948 | 0.329 | 23.11 | 3.833 | 0.785 | 0.569 | 22.20 | 3.336 | 0.769 | 0.595 |
| Week 12 LCMT | 21.64 | 3.970 | 0.845 | 0.473 | 21.85 | 4.475 | 0.835 | 0.489 | 21.42 | 3.469 | 0.808 | 0.532 |
| Outcome Measure | Intervention Group | Control Group | p | ||
|---|---|---|---|---|---|
| Mean | SD | Media | DT | ||
| LCMT at 0 weeks | 21.14 | 3.363 | 21.63 | 3.253 | 0.574 a |
| LCMT at 5 weeks | 23.11 | 3.833 | 22.20 | 3.336 | 0.340 a |
| LCTM at 12 weeks | 21.85 | 4.475 | 21.42 | 3.469 | 0.741 a |
| GDS at 5 Weeks | Control Group | Intervention Group | ||||
|---|---|---|---|---|---|---|
| Mean | SD | p | Mean | SD | p | |
| No cognitive decline | * | * | <0.001 a | 30.00 | 0.000 | <0.001 a |
| Very mild cognitive decline | 25.43 | 4.077 | 27.17 | 1.835 | ||
| Mild cognitive decline | 22.44 | 1.504 | 22.64 | 2.560 | ||
| Moderate cognitive decline (mild dementia) | 18.43 | 1.618 | 19.57 | 3.101 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiménez-Palomares, M.; González-López-Arza, M.V.; Garrido-Ardila, E.M.; Montanero-Fernández, J.; Rodríguez-Domínguez, T.; Rodríguez-Mansilla, J. Effects of a Cognitive Stimulation Program in Institutionalized Patients with Dementia. J. Pers. Med. 2022, 12, 1808. https://doi.org/10.3390/jpm12111808
Jiménez-Palomares M, González-López-Arza MV, Garrido-Ardila EM, Montanero-Fernández J, Rodríguez-Domínguez T, Rodríguez-Mansilla J. Effects of a Cognitive Stimulation Program in Institutionalized Patients with Dementia. Journal of Personalized Medicine. 2022; 12(11):1808. https://doi.org/10.3390/jpm12111808
Chicago/Turabian StyleJiménez-Palomares, María, María Victoria González-López-Arza, Elisa María Garrido-Ardila, Jesús Montanero-Fernández, Trinidad Rodríguez-Domínguez, and Juan Rodríguez-Mansilla. 2022. "Effects of a Cognitive Stimulation Program in Institutionalized Patients with Dementia" Journal of Personalized Medicine 12, no. 11: 1808. https://doi.org/10.3390/jpm12111808
APA StyleJiménez-Palomares, M., González-López-Arza, M. V., Garrido-Ardila, E. M., Montanero-Fernández, J., Rodríguez-Domínguez, T., & Rodríguez-Mansilla, J. (2022). Effects of a Cognitive Stimulation Program in Institutionalized Patients with Dementia. Journal of Personalized Medicine, 12(11), 1808. https://doi.org/10.3390/jpm12111808