
IL17F: A Possible Risk Marker for Spondyloarthritis in HLA-B*27 Negative Brazilian Patients


 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
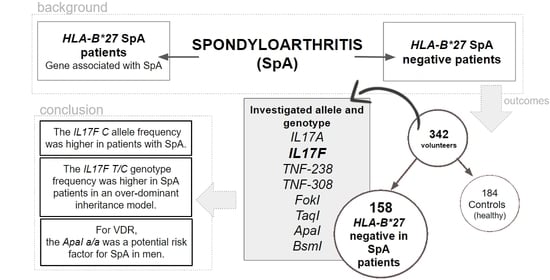
2.1. Sample Selection
2.2. Technical Procedures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cortes, A.; Hadler, J.; Pointon, J.P.; Robinson, P.C.; Karaderi, T.; Leo, P.; Cremin, K.; Pryce, K.; Harris, J.; Lee, S.; et al. Identification of multiple risk variants for ankylosing spondylitis through high-density genotyping of immune-related loci. Nat. Genet. 2013, 45, 730–738. [Google Scholar] [CrossRef]
- Singh, J.A.; Guyatt, G.; Ogdie, A.; Gladman, D.D.; Deal, C.; Deodhar, A.; Dubreuil, M.; Dunham, J.; Husni, M.E.; Kenny, S.; et al. Special Article: 2018 American College of Rheumatology/National Psoriasis Foundation Guideline for the Treatment of Psoriatic Arthritis. Arthritis Care Res. 2019, 71, 2–29. [Google Scholar] [CrossRef]
- Duffin, K.C.; Chandran, V.; Gladman, D.D.; Krueger, G.G.; Elder, J.T.; Rahman, P. Genetics of psoriasis and psoriatic arthritis: Update and future direction. J. Rheumatol. 2008, 35, 1449–1453. [Google Scholar]
- Akkoç, N.; Yarkan, H.; Kenar, G.; Khan, M.A. Ankylosing Spondylitis: HLA-B*27-Positive Versus HLA-B*27-Negative Disease. Curr. Rheumatol. Rep. 2017, 19. [Google Scholar] [CrossRef] [PubMed]
- Colbert, R.A.; Navid, F.; Gill, T. The role of HLA-B*27 in spondyloarthritis. Best Pract. Res. Clin. Rheumatol. 2017, 31, 797–815. [Google Scholar] [CrossRef] [PubMed]
- DeLay, M.L.; Turner, M.J.; Klenk, E.I.; Smith, J.A.; Sowders, D.P.; Colbert, R.A. HLA-B27 misfolding and the unfolded protein response augment interleukin-23 production and are associated with Th17 activation in transgenic rats. Arthritis Rheum. 2009, 60, 2633–2643. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.J.; Maksymowych, W.P. Beyond the TNF-α Inhibitors: New and Emerging Targeted Therapies for Patients with Axial Spondyloarthritis and their Relation to Pathophysiology. Drugs 2018, 78, 1397–1418. [Google Scholar] [CrossRef]
- Pedersen, S.J.; Maksymowych, W.P. The Pathogenesis of Ankylosing Spondylitis: An Update. Curr. Rheumatol. Rep. 2019, 21. [Google Scholar] [CrossRef] [PubMed]
- Guillot, X.; Prati, C.; Wendling, D. Vitamin D and spondyloarthritis. Expert Rev. Clin. Immunol. 2014, 10, 1581–1589. [Google Scholar] [CrossRef]
- Tang, J.; Zhou, R.; Luger, D.; Zhu, W.; Silver, P.B.; Grajewski, R.S.; Su, S.-B.; Chan, C.-C.; Adorini, L.; Caspi, R.R. Calcitriol Suppresses Antiretinal Autoimmunity through Inhibitory Effects on the Th17 Effector Response. J. Immunol. 2009, 182, 4624–4632. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Pantalena, L.-C.; Liu, X.K.; Gaffen, S.L.; Liu, H.; Rohowsky-Kochan, C.; Ichiyama, K.; Yoshimura, A.; Steinman, L.; Christakos, S.; et al. 1,25-Dihydroxyvitamin D3 Ameliorates Th17 Autoimmunity via Transcriptional Modulation of Interleukin-17A. Mol. Cell. Biol. 2011, 31, 3653–3669. [Google Scholar] [CrossRef] [PubMed]
- Neves, J.S.F.; Visentainer, J.E.L.; da Reis, D.M.S.; Rocha Loures, M.A.; Alves, H.V.; Lara-Armi, F.F.; De Alencar, J.B.; Valentin Zacarias, J.M.; Sell, A.M. The Influence of Vitamin D Receptor Gene Polymorphisms in Spondyloarthritis. Int. J. Inflam. 2020, 2020. [Google Scholar] [CrossRef]
- Rocha Loures, M.A.; Macedo, L.C.; Reis, D.M.; Oliveira, C.F.; Meneguetti, J.L.; Martines, G.F.; Neves, J.S.F.; de Souza, E.; Sell, A.M.; Visentainer, J.E.L. Influence of TNF and IL17 Gene Polymorphisms on the Spondyloarthritis Immunopathogenesis, Regardless of HLA-B27, in a Brazilian Population. Mediators Inflamm. 2018, 2018, 1–7. [Google Scholar] [CrossRef]
- Sieper, J.; Rudwaleit, M.; Baraliakos, X.; Brandt, J.; Braun, J.; Burgos-Vargas, R.; Dougados, M.; Hermann, K.G.; Landewe, R.; Maksymowych, W.; et al. The Assessment of SpondyloArthritis international Society (ASAS) handbook: A guide to assess spondyloarthritis. Ann. Rheum. Dis. 2009, 68, ii1–ii44. [Google Scholar] [CrossRef] [PubMed]
- Rudwaleit, M.; Van Der Heijde, D.; Landewé, R.; Akkoc, N.; Brandt, J.; Chou, C.T.; Dougados, M.; Huang, F.; Gu, J.; Kirazli, Y.; et al. The Assessment of SpondyloArthritis international Society classification criteria for peripheral spondyloarthritis and for spondyloarthritis in general. Ann. Rheum. Dis. 2011, 70, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Probst, C.M.; Bompeixe, E.P.; Pereira, N.F.; de O. Dalalio, M.M.; Visentainer, J.E.; Tsuneto, L.T.; Petzl-Erler, M.L. HLA polymorphism and evaluation of European, African, and Amerindian contribution to the white and mulatto populations from Paraná, Brazil. Hum. Biol. 2000, 72, 597–617. [Google Scholar]
- Reis, P.G.; Ambrosio-Albuquerque, E.P.; Fabreti-Oliveira, R.A.; Moliterno, R.A.; de Souza, V.H.; Sell, A.M.; Visentainer, J.E.L. HLA-A, -B, -DRB1, -DQA1, and -DQB1 profile in a population from southern Brazil. HLA 2018, 92, 298–303. [Google Scholar] [CrossRef]
- John, S.W.M.; Weitzner, G.; Rozen, R.; Scriver, C.R. A rapid procedure for extracting genomic DNA from leukocytes. Nucleic Acids Res. 1991, 19, 408. [Google Scholar] [CrossRef]
- Lara-Armi, F.; Visentainer, J.; Alves, H.; Rocha-Lourdes, M.; Neves, J.; Colli, C.; Sell, A. Optimization of HLA-B*27 ALLELE Genotyping by PCR-SSP. Clinics 2020, 75, 1840. [Google Scholar] [CrossRef]
- Zacarias, J.M.V.; Sippert, E.Â.; Tsuneto, P.Y.; Visentainer, J.E.L.; e Silva, C.d.O.; Sell, A.M. The Influence of Interleukin 17A and IL17F Polymorphisms on Chronic Periodontitis Disease in Brazilian Patients. Mediat. Inflamm. 2015, 2015, 1–8. [Google Scholar] [CrossRef]
- Nemenqani, D.M.; Karam, R.A.; Amer, M.G.; Abd El Rahman, T.M. Vitamin D receptor gene polymorphisms and steroid receptor status among Saudi women with breast cancer. Gene 2015, 558, 215–219. [Google Scholar] [CrossRef]
- Papadopoulou, A.; Kouis, P.; Middleton, N.; Kolokotroni, O.; Karpathios, T.; Nicolaidou, P.; Yiallouros, P.K. Association of vitamin D receptor gene polymorphisms and vitamin D levels with asthma and atopy in Cypriot adolescents: A case-control study. Multidiscip. Respir. Med. 2015, 10. [Google Scholar] [CrossRef]
- Pepineli, A.C.; Alves, H.V.; Tiyo, B.T.; Macedo, L.C.; Visentainer, L.; de Lima Neto, Q.A.; Zacarias, J.M.V.; Sell, A.M.; Visentainer, J.E.L. Vitamin D Receptor Gene Polymorphisms Are Associated With Leprosy in Southern Brazil. Front. Immunol. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Torres, T.M.; Ciconelli, R.M. Instrumentos de avaliação em espondilite anquilosante. Rev. Bras. Reumatol. 2006, 46, 52–59. [Google Scholar] [CrossRef][Green Version]
- Solé, X.; Guinó, E.; Valls, J.; Iniesta, R.; Moreno, V. SNPStats: A web tool for the analysis of association studies. Bioinformatics 2006, 22, 1928–1929. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.C.; Fry, B.; Maller, J.; Daly, M.J. Haploview: Analysis and visualization of LD and haplotype maps. Bioinformatics 2005, 21, 263–265. [Google Scholar] [CrossRef] [PubMed]
- Reis, P.G.; de Alencar, J.B.; Macedo, L.C.; Ambrosio-Albuquerque, E.P.; de Aquino, J.S.; Zacarias, J.M.V.; Tsuneto, P.Y.; Moliterno, R.A.; Sell, A.M.; Visentainer, J.E.L. Cytokine gene polymorphisms in populations from Parana, Southern Brazil. Hum. Immunol. 2017, 78. [Google Scholar] [CrossRef]
- De Carvalho, H.M.S.; Bortoluzzo, A.B.; Gonçalves, C.R.; Da Silva, J.A.B.; Ximenes, A.C.; Bértolo, M.B.; Ribeiro, S.L.E.; Keiserman, M.; Menin, R.; Skare, T.L.; et al. Gender characterization in a large series of Brazilian patients with spondyloarthritis. Clin. Rheumatol. 2012, 31, 687–695. [Google Scholar] [CrossRef]
- Lin, H.; Gong, Y.Z. Association of HLA-B27 with ankylosing spondylitis and clinical features of the HLA-B27-associated ankylosing spondylitis: A meta-analysis. Rheumatol. Int. 2017, 37, 1267–1280. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A. Update on spondyloarthropathies. Ann. Intern. Med. 2002, 136, 896–907. [Google Scholar] [CrossRef]
- Syrbe, U.; Baraliakos, X. Spondyloarthritis. Z. Rheumatol. 2018, 77, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Marwa, O.S.; Kalthoum, T.; Wajih, K.; Kamel, H. Association of IL17A and IL17F genes with rheumatoid arthritis disease and the impact of genetic polymorphisms on response to treatment. Immunol. Lett. 2017, 183, 24–36. [Google Scholar] [CrossRef] [PubMed]
- Shao, M.; Xu, S.; Yang, H.; Xu, W.; Deng, J.; Chen, Y.; Gao, X.; Guan, S.; Xu, S.; Shuai, Z.; et al. Association between IL-17A and IL-17F gene polymorphism and susceptibility in inflammatory arthritis: A meta-analysis. Clin. Immunol. 2020, 213. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Ma, C.; Wang, W.; Zhao, B.; Xie, B.; Liu, J. Common variants in IL17F gene contributed to the risk of hip osteoarthritis susceptibility in Han Chinese population. Int. J. Rheum. Dis. 2020, 23, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Bafrani, H.H.; Ahmadi, M.; Jahantigh, D.; Karimian, M. Association analysis of the common varieties of IL17A and IL17F genes with the risk of knee osteoarthritis. J. Cell. Biochem. 2019, 120, 18020–18030. [Google Scholar] [CrossRef] [PubMed]
- Choi, B.G.; Hong, J.Y.; Hong, J.R.; Hur, M.S.; Kim, S.M.; Lee, Y.W.; Choe, Y.B.; Ahn, K.J. The IL17F His161Arg polymorphism, a potential risk locus for psoriasis, increases serum levels of interleukin-17F in an Asian population. Sci. Rep. 2019, 9, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Erkol Inal, E.; Görükmez, O.; Dündar, Ü.; Görükmez, Ö.; Yener, M.; Sağ, Ş.Ö.; Yakut, T. The Influence of Polymorphisms of Interleukin-17A and -17F Genes on Susceptibility and Activity of Rheumatoid Arthritis. Genet. Test. Mol. Biomarkers 2015, 19, 461–464. [Google Scholar] [CrossRef]
- Weaver, C.T.; Harrington, L.E.; Mangan, P.R.; Gavrieli, M.; Murphy, K.M. Th17: An Effector CD4 T Cell Lineage with Regulatory T Cell Ties. Immunity 2006, 24, 677–688. [Google Scholar] [CrossRef]
- Amatya, N.; Garg, A.V.; Gaffen, S.L. IL-17 Signaling: The Yin and the Yang. Trends Immunol. 2017, 38, 310–322. [Google Scholar] [CrossRef]
- Rossini, M.; Viapiana, O.; Adami, S.; Idolazzi, L.; Fracassi, E.; Gatti, D. Focal bone involvement in inflammatory arthritis: The role of IL17. Rheumatol. Int. 2016, 36, 469–482. [Google Scholar] [CrossRef]
- Ehrenfeld, M. Spondyloarthropathies. Best Pract. Res. Clin. Rdheumatol. 2012, 26, 135–145. [Google Scholar] [CrossRef] [PubMed]
- De Toledo, R.A.; de Toledo, R.A.; Camargo, U.; da Silveira Camargo, A.V.; Xavier, D.H.; Batista, M.F.; Carneiro, O.A.; Robles, J.A.; de Mattos, C.C.; Júnior, O.R.; et al. HLA-B*27-Frequency of clinical signs in Brazilian patients with spondyloarthritis. Biomarkers Genomic Med. 2015, 7, 72–77. [Google Scholar] [CrossRef]
- Gallinaro, A.L.; Ventura, C.; Barros, P.D.S.; Gonçalves, C.R. Espondiloartrites: Análise de uma série Brasileira comparada a uma grande casuística Ibero-Americana (estudo RESPONDIA). Rev. Bras. Reumatol. 2010, 50, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, S.L.E.; de Campos, A.P.B.; Palominos, P.E.; Bortoluzzo, A.B.; da Costa, M.A.C.; de Oliveira Ribeiro, T.; Sampaio-Barros, P.D. Different ethnic background is associated with distinct clinical profiles in the spondyloarthritides in the North and South of Brazil. Clin. Rheumatol. 2019, 38, 195–203. [Google Scholar] [CrossRef]
- Deng, S.; He, Y.; Nian, X.; Sun, E.; Li, L. Relationship between Vitamin D levels and pain and disease activity in patients with newly diagnosed axial spondyloarthritis. Int. J. Nurs. Sci. 2020, 7, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Kolahi, S.; Khabbazi, A.; Kazemi, N.; Malek Mahdavi, A. Does vitamin D deficiency contribute to higher disease activity in patients with spondyloarthritis? Immunol. Lett. 2019, 212, 1–5. [Google Scholar] [CrossRef]
- Zhao, S.; Thong, D.; Duffield, S.; Goodson, N. Vitamin D deficiency in axial spondyloarthritis is associated with higher disease activity. Arch. Rheumatol. 2017, 32, 209–215. [Google Scholar] [CrossRef]
- Pokhai, G.G.; Bandagi, S.; Abrudescu, A. Vitamin D levels in ankylosing spondylitis: Does deficiency correspond to disease activity? Rev. Bras. Reumatol. 2014, 54, 330–334. [Google Scholar] [CrossRef] [PubMed]
- Kocyigit, B.F.; Akyol, A. Vitamin D levels in patients with ankylosing spondylitis: Is it related to disease activity? Pakistan, J. Med. Sci. 2018, 34, 1209–1214. [Google Scholar] [CrossRef]
- Blauvelt, A.; Chiricozzi, A. The Immunologic Role of IL-17 in Psoriasis and Psoriatic Arthritis Pathogenesis. Clin. Rev. Allergy Immunol. 2018, 55, 379–390. [Google Scholar] [CrossRef]
- Barnas, J.L.; Ritchlin, C.T. Etiology and Pathogenesis of Psoriatic Arthritis. Rheum. Dis. Clin. N. Am. 2015, 41, 643–663. [Google Scholar] [CrossRef] [PubMed]
- Jansen, D.T.S.L.; Hameetman, M.; Van Bergen, J.; Huizinga, T.W.J.; Van Der Heijde, D.; Toes, R.E.M.; Van Gaalen, F.A. IL-17-producing CD4+ T cells are increased in early, active axial spondyloarthritis including patients without imaging abnormalities. Rheumatology 2014, 54, 728–735. [Google Scholar] [CrossRef] [PubMed]
- Gaston, J.S.H.; Jadon, D.R. Th17 cell responses in spondyloarthritis. Best Pract. Res. Clin. Rheumatol. 2017, 31, 777–796. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | SpA | AS | PsA | Controls |
|---|---|---|---|---|
| N = 158 | N = 102 | N = 56 | N = 184 | |
| Mean age ± SD (year) | 49.36 (±16.04) | 45.57 (±16.06) | 54.83 (±14.33) | 40.92 (±12.16) |
| Male n (%) | 64 (40.50) | 40 (39.22) | 24 (42.86) | 77 (41.85) |
| Male mean age ± SD (year) | 50.63 (±15.73) | 47.30 (±16.09) | 56.17 (±13.70) | 40.88 (±11.63) |
| BASDAI | N = 66 | |||
| <4.0 | 23 (34.84%) | |||
| ≥4.0 | 43 (65.16%) | |||
| Vitamin D | N = 40 | |||
| <29.9 ng/mL | 27 (67.50%) | |||
| >30.0 ng/mL | 13 (32.50%) |
| Genotypes and Alleles | SpA | AS | PsA | Control | OR (95% CI) | p-Value | Pc |
|---|---|---|---|---|---|---|---|
| n (f) | n (f) | n (f) | n (f) | ||||
| IL17A | N = 156 * | N = 100 * | N = 56 | N = 182 * | |||
| G/G | 79 (0.51) | 55 (0.55) | 24 (0.43) | 102 (0.56) | |||
| G/A | 60 (0.38) | 38 (0.38) | 22 (0.39) | 67 (0.37) | |||
| A/A | 17 (0.11) | 7 (0.07) | 10 (0.18) | 13 (0.07) | |||
| Recessive G/G+A/G = Ref | 46 (0.82) | 169 (0.93) | |||||
| A/A | 10 (0.18) c | 13 (0.07) | 2.89 (1.18–7.08) c | 0.02 | 0.10 | ||
| G | 218 (0.70) | 148 (0.74) | 70 (0.62) | 271 (0.74) | |||
| A | 94 (0.30) | 52 (0.26) | 42 (0.38) | 93 (0.26) | |||
| IL17F | N = 156 | N = 100 | N = 56 | N = 184 | |||
| T/T | 110 (0.71) | 77 (0.77) | 33 (0.59) | 167 (0.91) | |||
| T/C | 45 (0.28) | 22 (0.22) | 23 (0.41) | 15 (0.08) | |||
| C/C | 1 (0.006) | 1 (0.01) | 0 (0.00) | 2 (0.01) | |||
| Overdominant T/T+C/C = Ref. | 111 (0.71) | 78 (0.78) | 33 (0.59) | 169 (0.92) | |||
| T/C | 45 (0.29) a | 22 (0.22) b | 23 (0.41) c | 15 (0.08) | 4.31 (2.32–8.01) a 3.36 (1.63–6.91) b 8.33 (3.88–17.85) c | <10−4 <10−4 <10−4 | <0.001 <0.001 <0.001 |
| T | 265 (0.85) | 176 (0.88) | 89 (0.79) | 349 (0.95) | |||
| C | 47 (0.15) | 24 (0.12) | 23 (0.21) | 18 (0.05) | 3.39 (1.92–5.97) a 2.61 (1.38–4.93) b 4.93 (2.55–9.55) c | <10−4 0.003 <10−4 | <0.0001 0.015 <0.0001 |
| TNF-238 | N = 156 | N = 100 | N = 56 | N = 182 | |||
| G/G | 130 (0.83) | 88 (0.88) | 42 (0.75) | 155 (0.85) | |||
| G/A | 25 (0.16) | 12 (0.12) | 13 (0.23) | 26 (0.14) | |||
| A/A | 1 (0.006) | 0 (0.00) | 1 (0.18) | 1 (0.006) | |||
| G | 285 (0.91) | 188 (0.94) | 97 (0.87) | 336 (0.92) | |||
| A | 27 (0.09) | 12 (0.06) | 15 (0.13) | 28 (0.08) | |||
| TNF-308 | N = 156 | N = 100 | N = 56 | N = 182 | |||
| G/G | 106 (0.68) | 68 (0.67) | 38 (0.68) | 119 (0.65) | |||
| G/A | 48 (0.31) | 31 (0.31) | 17 (0.30) | 61 (0.34) | |||
| A/A | 2 (0.01) | 1 (0.01) | 1 (0.02) | 2 (0.01) | |||
| G | 260 (0.83) | 167 (0.84) | 93 (0.83) | 299 (0.82) | |||
| A | 52 (0.17) | 33 (0.16) | 19 (0.17) | 65 (0.18) | |||
| FokI | N = 158 | N = 102 | N = 56 | N = 184 | |||
| F/F | 62 (0.39) | 41 (0.40) | 21 (0.38) | 82 (0.45) | |||
| F/f | 81 (0.51 | 49 (0.48) | 32 (0.57) | 85 (0.46) | |||
| f/f | 15 (0.10) | 12 (0.12) | 3 (0.05) | 17 (0.09) | |||
| F | 205 (0.65) | 131 (0.64) | 74 (0.66) | 249 (0.68) | |||
| f | 111 (0.35) | 73 (0.36) | 38 (0.34) | 119 (0.32) | |||
| TaqI | N = 158 | N = 102 | N = 56 | N = 184 | |||
| T/T | 61 (0.39) | 38 (0.37) | 23 (0.41) | 74 (0.40) | |||
| T/t | 77 (0.49) | 52 (0.51) | 25 (0.45) | 89 (0.48) | |||
| t/t | 20 (0.13) | 12 (0.12) | 8 (0.14) | 21 (0.12) | |||
| T | 199 (0.63) | 128 (0.63) | 71 (0.63) | 237 (0.64) | |||
| t | 117 (0.37) | 76 (0.37) | 41 (0.37) | 131 (0.36) | |||
| ApaI | N = 158 | N = 102 | N = 56 | N = 184 | |||
| A/A | 52 (0.33) | 29 (0.28) | 23 (0.41) | 57 (0.31) | |||
| A/a | 73 (0.46) | 45 (0.44) | 28 (0.50) | 96 (0.52) | |||
| a/a | 33 (0.21) | 28 (0.27) | 5 (0.09) | 31 (0.17) | |||
| Recessive: A/A-A/a = Ref | 74 (0.73) | 153 (0.83) | |||||
| a/a | 28 (0.27) b | 31 (0.17) | 1.88 (1.05-3.36) b | 0.035 | 0.175 | ||
| A | 177 (0.56) | 103 (0.50) | 74 (0.66) | 210 (0.57) | |||
| a | 139 (0.44) | 101 (0.50) | 38 (0.34) | 158 (0.43) | |||
| BsmI | N = 158 | N = 102 | N = 56 | N = 184 | |||
| b/b | 55 (0.35) | 34 (0.33) | 21 (0.38) | 70 (0.38) | |||
| B/b | 81 (0.51) | 54 (0.53) | 27 (0.48) | 89 (0.48) | |||
| B/B | 22 (0.14) | 14 (0.14) | 8 (0.14) | 25 (0.14) | |||
| b | 191 (0.60) | 122 (0.60) | 69 (0.62) | 229 (0.62) | |||
| B | 125 (0.40) | 82 (0.40) | 43 (0.38) | 139 (0.38) | |||
| SpAn (f) | Controlsn (f) | p-Value | Pc | OR (95% CI) | ||
|---|---|---|---|---|---|---|
| IL17F | N = 156 | N = 182 | ||||
| female | ||||||
| T/T | 62 (0.67) | 96 (0.91) | Ref. | |||
| T/C | 29 (0.31) | 7 (0.067) | 10−5 | 0.0001 | 6.41 (2.65-15.54) | |
| C/C | 1 (0.01) | 2 (0.02) | ||||
| male | ||||||
| T/T | 48 (0.75) | 69 (0.90) | Ref. | |||
| T/C | 16 (0.25) | 8 (0.09) | 0.011 | 0.05 | 3.29 (1.26-8.59) | |
| C/C | 0 | 0 | ||||
| ApaI | N = 158 | N = 182 | ||||
| male | ||||||
| A/A | 19 (0.30) | 26 (0.34) | Ref. | |||
| A/a | 25 (0.39) | 42 (0.55) | ||||
| a/a | 20 (0.31) | 9 (0.12) | 0.004 | 0.02 | 3.04 (1.14-8.14) | |
| Spondyloarthritis (SpA) N = 66 | |||||
|---|---|---|---|---|---|
| Genotype | Vitamin D | BASDAI < 4.0 | BASDAI ≥ 4.0 | p-Value | OR (95% CI) |
| n (f) | n (f) | ||||
| IL17A G/G | Deficiency | 3 (0.20) | 6 (0.67) | ||
| Sufficiency | 12 (0.80) | 3 (0.33) | 0.03 | 0.12 (0.02–0.82) | |
| TNF-308 G/G | Deficiency | 3 (0.12) | 9 (0.42) | ||
| Sufficiency | 20 (0.88) | 12 (0.57) | 0.03 | 0.20 (0.05–0.89) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neves, J.S.F.; Visentainer, J.E.L.; Reis, D.M.d.S.; Rocha Loures, M.A.; Alves, H.V.; Zacarias, J.M.V.; Sell, A.M. IL17F: A Possible Risk Marker for Spondyloarthritis in HLA-B*27 Negative Brazilian Patients. J. Pers. Med. 2021, 11, 520. https://doi.org/10.3390/jpm11060520
Neves JSF, Visentainer JEL, Reis DMdS, Rocha Loures MA, Alves HV, Zacarias JMV, Sell AM. IL17F: A Possible Risk Marker for Spondyloarthritis in HLA-B*27 Negative Brazilian Patients. Journal of Personalized Medicine. 2021; 11(6):520. https://doi.org/10.3390/jpm11060520
Chicago/Turabian StyleNeves, Janisleya Silva Ferreira, Jeane Eliete Laguila Visentainer, Denise Manjurma da Silva Reis, Marco Antonio Rocha Loures, Hugo Vicentin Alves, Joana Maira Valentini Zacarias, and Ana Maria Sell. 2021. "IL17F: A Possible Risk Marker for Spondyloarthritis in HLA-B*27 Negative Brazilian Patients" Journal of Personalized Medicine 11, no. 6: 520. https://doi.org/10.3390/jpm11060520
APA StyleNeves, J. S. F., Visentainer, J. E. L., Reis, D. M. d. S., Rocha Loures, M. A., Alves, H. V., Zacarias, J. M. V., & Sell, A. M. (2021). IL17F: A Possible Risk Marker for Spondyloarthritis in HLA-B*27 Negative Brazilian Patients. Journal of Personalized Medicine, 11(6), 520. https://doi.org/10.3390/jpm11060520