
Influence of Deep Neuromuscular Blockade on Perioperative Stress Response in Patients Undergoing Robot-Assisted Gastrectomy: A Prospective Double-Blinded Randomized-Controlled Trial

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design and Intervention
2.3. Anesthetic Management
2.4. Outcome Assessments
2.5. Statistical Analyses
3. Results
3.1. Patients
3.2. Demographic and Intraoperative Characteristics
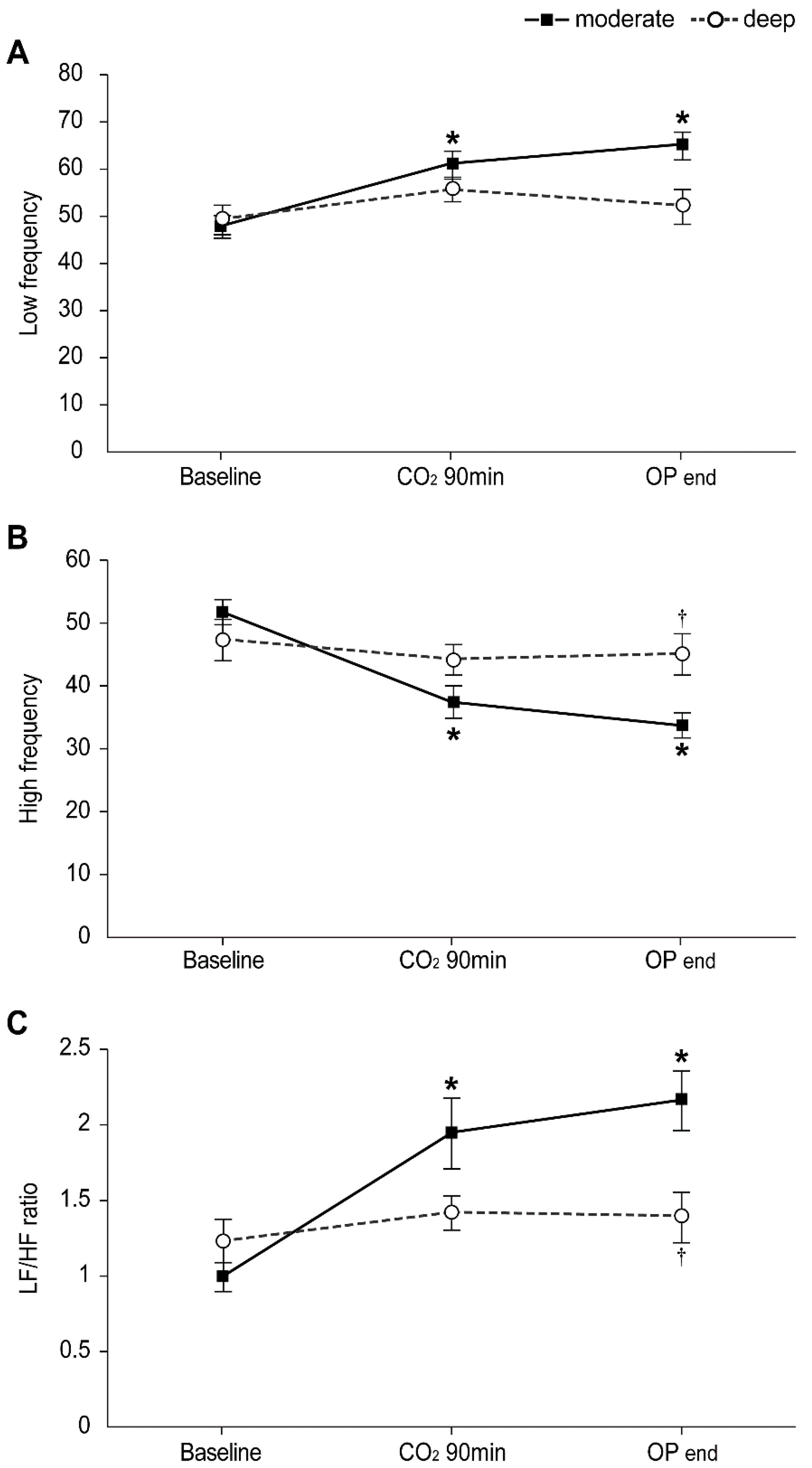
3.3. The Intraopeartive HRV
3.4. Stress Response-Related Laboratory Markers: Cortisol, Prolactin, IL-6 Levels, and NK Cell Percentage
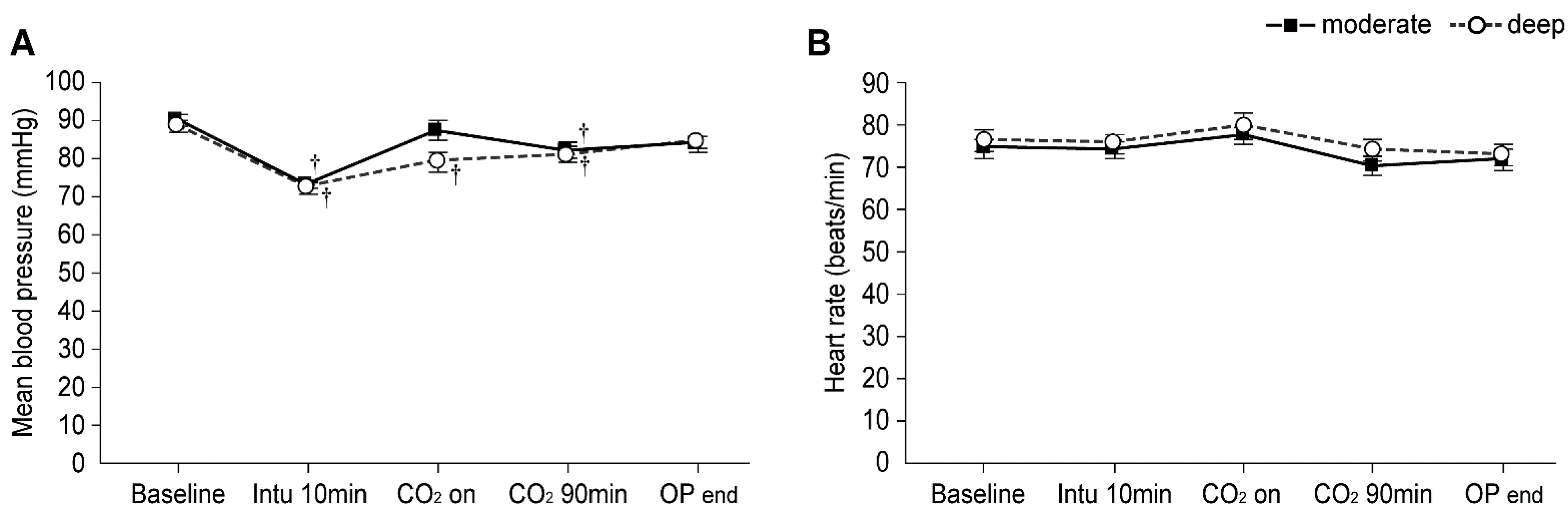
3.5. Intraoperative Mean Blood Pressure and Heart Rate
3.6. Postoperative Recovery Profiles
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caruso, S.; Patriti, A.; Roviello, F.; De Franco, L.; Franceschini, F.; Coratti, A.; Ceccarelli, G. Laparoscopic and robot-assisted gastrectomy for gastric cancer: Current considerations. World J. Gastroenterol. 2016, 22, 5694–5717. [Google Scholar] [CrossRef]
- Caruso, S.; Franceschini, F.; Patriti, A.; Roviello, F.; Annecchiarico, M.; Ceccarelli, G.; Coratti, A. Robot-assisted laparoscopic gastrectomy for gastric cancer. World J. Gastrointest Endosc. 2017, 9, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.Y.; Bai, S.J.; Kim, H.-I.; Hong, J.H.; Nam, H.; Koh, J.C.; Kim, H.J. Effects of long periods of pneumoperitoneum combined with the head-up position on heart rate-corrected QT interval during robotic gastrectomy: An observational study. J. Int. Med Res. 2018, 46, 4586–4595. [Google Scholar] [CrossRef]
- Sato, N.; Kawamoto, M.; Yuge, O.; Suyama, H.; Sanuki, M.; Matsumoto, C.; Inoue, K. Effects of pneumoperitoneum on cardiac autonomic nervous activity evaluated by heart rate variability analysis during sevoflurane, isoflurane, or propofol anesthesia. Surg. Endosc. 2000, 14, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Uemura, N.; Nomura, M.; Inoue, S.; Endo, J.; Kishi, S.; Saito, K.; Ito, S.; Nakaya, Y. Changes in hemodynamics and autonomic nervous activity in patients undergoing laparoscopic cholecystectomy: Differences between the pneumoperitoneum and abdominal wall-lifting method. Endoscopy 2002, 34, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Coffey, J.C.; Wang, J.H.; Smith, M.J.; Bouchier-Hayes, D.; Cotter, T.G.; Redmond, H.P. Excisional surgery for cancer cure: Therapy at a cost. Lancet Oncol. 2003, 4, 760–768. [Google Scholar] [CrossRef]
- Ramsay, M.A. Acute postoperative pain management. Proceedings (Bayl. Univ. Med. Cent.) 2000, 13, 244–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottschalk, A.; Sharma, S.; Ford, J.; Durieux, M.E.; Tiouririne, M. Review article: The role of the perioperative period in recurrence after cancer surgery. Anesth. Analg. 2010, 110, 1636–1643. [Google Scholar] [CrossRef]
- Al-Hashimi, M.; Scott, S.W.; Thompson, J.P.; Lambert, D.G. Opioids and immune modulation: More questions than answers. Br. J. Anaesth. 2013, 111, 80–88. [Google Scholar] [CrossRef] [Green Version]
- Bruintjes, M.H.; van Helden, E.V.; Braat, A.E.; Dahan, A.; Scheffer, G.J.; van Laarhoven, C.J.; Warlé, M.C. Deep neuromuscular block to optimize surgical space conditions during laparoscopic surgery: A systematic review and meta-analysis. Br. J. Anaesth. 2017, 118, 834–842. [Google Scholar] [CrossRef] [Green Version]
- Koo, B.W.; Oh, A.Y.; Na, H.S.; Lee, H.J.; Kang, S.B.; Kim, D.W.; Seo, K.-S. Effects of depth of neuromuscular block on surgical conditions during laparoscopic colorectal surgery: A randomised controlled trial. Anaesthesia 2018, 73, 1090–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.K.; Son, Y.G.; Yoo, S.; Lim, T.; Kim, W.H.; Kim, J.T. Deep vs. moderate neuromuscular blockade during laparoscopic surgery: A systematic review and meta-analysis. Eur. J. Anaesthesiol. 2018, 35, 867–875. [Google Scholar] [CrossRef]
- Yoo, Y.C.; Kim, N.Y.; Shin, S.; Choi, Y.D.; Hong, J.H.; Kim, C.Y.; Park, H.J.; Bai, S.-J. The Intraocular Pressure under Deep versus Moderate Neuromuscular Blockade during Low-Pressure Robot Assisted Laparoscopic Radical Prostatectomy in a Randomized Trial. PLoS ONE 2015, 10, e0135412. [Google Scholar] [CrossRef]
- Cho, J.S.; Kim, H.-I.; Lee, K.-Y.; Son, T.; Bai, S.J.; Choi, H.; Yoo, Y.C. Comparison of the effects of patient-controlled epidural and intravenous analgesia on postoperative bowel function after laparoscopic gastrectomy: A prospective randomized study. Surg. Endosc. 2017, 31, 4688–4696. [Google Scholar] [CrossRef]
- Kim, M.H.; Lee, K.Y.; Lee, K.Y.; Min, B.S.; Yoo, Y.C. Maintaining Optimal Surgical Conditions with Low Insufflation Pressures is Possible With Deep Neuromuscular Blockade during Laparoscopic Colorectal Surgery: A Prospective, Randomized, Double-Blind, Parallel-Group Clinical Trial. Medicine 2016, 95, e2920. [Google Scholar] [CrossRef]
- Fuchs-Buder, T.; Claudius, C.; Skovgaard, L.T.; Eriksson, L.I.; Mirakhur, R.K.; Viby-Mogensen, J. Good clinical research practice in pharmacodynamic studies of neuromuscular blocking agents II: The Stockholm revision. Acta Anaesthesiol. Scand. 2007, 51, 789–808. [Google Scholar] [CrossRef] [PubMed]
- Rajendra Acharya, U.; Paul Joseph, K.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.; Hoggart, B. Pain: A review of three commonly used pain rating scales. J. Clin. Nurs. 2005, 14, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Desborough, J.P. The stress response to trauma and surgery. Br. J. Anaesth. 2000, 85, 109–117. [Google Scholar] [CrossRef] [Green Version]
- Gouin, J.P.; Kiecolt-Glaser, J.K. The impact of psychological stress on wound healing: Methods and mechanisms. Crit. Care Nurs. Clin. N. Am. 2012, 24, 201–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parker, S.D.; Breslow, M.J.; Frank, S.M.; Rosenfeld, B.A.; Norris, E.J.; Christopherson, R.; Rock, P.; Gottlieb, S.O.; Raff, H.; Perler, B.A.; et al. Catecholamine and cortisol responses to lower extremity revascularization: Correlation with outcome variables. Perioperative Ischemia Randomized Anesthesia Trial Study Group. Crit. Care Med. 1995, 23, 1954–1961. [Google Scholar] [CrossRef]
- Taylor, L.K.; Auchus, R.J.; Baskin, L.S.; Miller, W.L. Cortisol response to operative stress with anesthesia in healthy children. J. Clin. Endocrinol. Metab. 2013, 98, 3687–3693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth-Isigkeit, A.K.; Schmucker, P. Postoperative dissociation of blood levels of cortisol and adrenocorticotropin after coronary artery bypass grafting surgery. Steroids 1997, 62, 695–699. [Google Scholar] [CrossRef]
- Gibbison, B.; Angelini, G.D.; Lightman, S.L. Dynamic output and control of the hypothalamic-pituitary-adrenal axis in critical illness and major surgery. Br. J. Anaesth. 2013, 111, 347–360. [Google Scholar] [CrossRef] [Green Version]
- Khoo, B.; Boshier, P.R.; Freethy, A.; Tharakan, G.; Saeed, S.; Hill, N.; Williams, E.L.; Moorthy, K.; Tolley, N.; Jiao, L.R.; et al. Redefining the stress cortisol response to surgery. Clin. Endocrinol. 2017, 87, 451–458. [Google Scholar] [CrossRef]
- Labad, J.; Stojanovic-Perez, A.; Montalvo, I.; Sole, M.; Cabezas, A.; Ortega, L.; Moreno, I.; Vilella, E.; Martorell, L.; Reynolds, R.M.; et al. Stress biomarkers as predictors of transition to psychosis in at-risk mental states: Roles for cortisol, prolactin and albumin. J. Psychiatr. Res. 2015, 60, 163–169. [Google Scholar] [CrossRef]
- Torner, L. Actions of Prolactin in the Brain: From Physiological Adaptations to Stress and Neurogenesis to Psychopathology. Front Endocrinol. 2016, 7, 25. [Google Scholar] [CrossRef] [Green Version]
- Kumari, N.; Dwarakanath, B.S.; Das, A.; Bhatt, A.N. Role of interleukin-6 in cancer progression and therapeutic resistance. Tumour. Biol. 2016, 37, 11553–11572. [Google Scholar] [CrossRef]
- Porter, C.; Tompkins, R.G.; Finnerty, C.C.; Sidossis, L.S.; Suman, O.E.; Herndon, D.N. The metabolic stress response to burn trauma: Current understanding and therapies. Lancet 2016, 388, 1417–1426. [Google Scholar] [CrossRef] [Green Version]
- Shibayama, O.; Yoshiuchi, K.; Inagaki, M.; Matsuoka, Y.; Yoshikawa, E.; Sugawara, Y.; Akechi, T.; Wada, N.; Imoto, S.; Murakami, K.; et al. Association between adjuvant regional radiotherapy and cognitive function in breast cancer patients treated with conservation therapy. Cancer Med. 2014, 3, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Xu, F.; Lu, T.; Duan, Z.; Zhang, Z. Interleukin-6 signaling pathway in targeted therapy for cancer. Cancer Treat. Rev. 2012, 38, 904–910. [Google Scholar] [CrossRef]
- Angka, L.; Khan, S.T.; Kilgour, M.K.; Xu, R.; Kennedy, M.A.; Auer, R.C. Dysfunctional Natural Killer Cells in the Aftermath of Cancer Surgery. Int. J. Mol. Sci. 2017, 18, 1787. [Google Scholar] [CrossRef] [Green Version]
- Brochner, A.C.; Mikkelsen, S.; Hegelund, I.; Hokland, M.; Mogensen, O.; Toft, P. The immune response is affected for at least three weeks after extensive surgery for ovarian cancer. Dan. Med. J. 2016, 63, A5243. [Google Scholar]
- Kang, Y.-J.; Jeung, I.C.; Park, A.; Park, Y.-J.; Jung, H.; Kim, T.-D.; Lee, H.G.; Choi, I.; Yoon, S.R. An increased level of IL-6 suppresses NK cell activity in peritoneal fluid of patients with endometriosis via regulation of SHP-2 expression. Hum. Reprod. 2014, 29, 2176–2189. [Google Scholar] [CrossRef] [Green Version]
- Cifaldi, L.; Prencipe, G.; Caiello, I.; Bracaglia, C.; Locatelli, F.; De Benedetti, F.; Strippoli, R. Inhibition of natural killer cell cytotoxicity by interleukin-6: Implications for the pathogenesis of macrophage activation syndrome. Arthritis Rheumatol. 2015, 67, 3037–3046. [Google Scholar] [CrossRef]
- Vredevoe, D.L.; Widawski, M.; Fonarow, G.C.; Hamilton, M.; Martinez-Maza, O.; Gage, J.R. Interleukin-6 (IL-6) expression and natural killer (NK) cell dysfunction and anergy in heart failure. Am. J. Cardiol. 2004, 93, 1007–1011. [Google Scholar] [CrossRef] [PubMed]
- Neukirchen, M.; Kienbaum, P. Sympathetic nervous system: Evaluation and importance for clinical general anesthesia. Anesthesiology 2008, 109, 1113–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrone, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ. Res. 1986, 59, 178–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Moderate NMB (n = 23) | Deep NMB (n = 23) | p Value |
|---|---|---|---|
| Age, year | 55.0 ± 8.2 | 52.1 ± 8.8 | 0.253 |
| Male sex | 10 (43%) | 12 (52%) | 0.555 |
| Body mass index, kg/m2 | 23.0 ± 3.3 | 23.5 ± 3.0 | 0.553 |
| ASA physical status | >0.999 | ||
| I | 4 (17%) | 5 (22%) | |
| II | 19 (83%) | 18 (78%) | |
| Pneumoperitoneum time, min | 149 ± 51 | 170 ± 64 | 0.228 |
| Operation time, min | 177 ± 47 | 194 ± 67 | 0.312 |
| Anesthesia time, min | 207 ± 48 | 228 ± 68 | 0.232 |
| Administered dose of remifentanil, μg | 708 ± 249 | 717 ± 296 | 0.918 |
| Administered dose of rocuronium, mg | 88 ± 37 | 133 ± 60 | 0.004 * |
| Additional request of rocuronium | 9 (39%) | 2 (9%) | 0.016 * |
| Intraoperative fluid intake and outtake | |||
| Crystalloid, mL | 1339 ± 448 | 1378 ± 463 | 0.772 |
| Colloid, mL | 102 ± 192 | 217 ± 295 | 0.124 |
| Blood loss, mL | 42 ± 53 | 41 ± 42 | 0.903 |
| Urine output, mL | 196 ± 126 | 202 ± 138 | 0.872 |
| Type of operation | 0.498 | ||
| Subtotal gastrectomy | 18 (78%) | 21 (91%) | |
| Proximal subtotal gastrectomy | 2 (9%) | 0 (0%) | |
| Total gastrectomy | 3 (13%) | 2 (9%) | |
| Type of reconstruction and anastomosis | 0.259 | ||
| Billoth I | 17 (74%) | 21 (91%) | |
| Billoth II | 2 (9%) | 0 (0%) | |
| Double tract | 2 (9%) | 0 (0%) | |
| Roux-en-Y | 2 (9%) | 4 (17%) | |
| Extent of lymph node dissection | 0.500 | ||
| D1 | 18 (78%) | 17 (74%) | |
| D2 | 5 (22%) | 6 (26%) | |
| TNM stage | 0.346 | ||
| I | 22 (96%) | 19 (83%) | |
| II | 1 (4%) | 3 (13%) | |
| III | 0 (0%) | 1 (4%) |
| Variable | Moderate NMB (n = 23) | Deep NMB (n = 23) | p Value |
|---|---|---|---|
| In post-anesthetic care unit | |||
| Numeric rating scale, resting | 4.1 ± 1.5 | 4.1 ± 1.6 | >0.999 |
| Numeric rating scale, active | 6.2 ± 1.4 | 6.3 ± 1.3 | 0.749 |
| The number of patients requesting for rescue analgesics | 7 (30%) | 7 (30%) | >0.999 |
| Morphine equivalent dose of analgesics, mg | 1.7 ± 3.1 | 1.6 ± 3.0 | 0.923 |
| The number of patients receiving additional antiemetic agents | 1 (4%) | 1 (4%) | >0.999 |
| Duration in the PACU, min | 45 ± 16 | 47 ± 18 | 0.703 |
| Postoperative 1–6 h | |||
| Numeric rating scale, resting | 4.1 ± 1.3 | 4.7 ± 1.3 | 0.116 |
| Numeric rating scale, active | 6.5 ± 1.3 | 6.7 ± 1.3 | 0.573 |
| The number of patients requesting for rescue analgesics | 9 (39%) | 16 (70%) | 0.075 |
| Morphine equivalent dose of analgesics, mg | 1.8 ± 2.3 | 3.1 ± 2.1 | 0.059 |
| The number of patients receiving additional antiemetic agents | 1 (4%) | 1 (4%) | >0.999 |
| Postoperative 6–24 h | |||
| Numeric rating scale, resting | 3.8 ± 1.2 | 4.0 ± 1.9 | 0.584 |
| Numeric rating scale, active | 5.9 ± 1.2 | 6.1 ± 1.5 | 0.593 |
| The number of patients requesting for rescue analgesics | 9 (39%) | 13 (57%) | 0.376 |
| Morphine equivalent dose of analgesics, mg | 1.8 ± 2.3 | 2.8 ± 2.7 | 0.189 |
| The number of patients receiving additional antiemetic agents | 3 (13%) | 1 (4%) | 0.608 |
| Postoperative 24–48 h | |||
| Numeric rating scale, resting | 3.1 ± 1.8 | 3.3 ± 2.0 | 0.757 |
| Numeric rating scale, active | 5.2 ± 1.7 | 5.1 ± 1.8 | 0.869 |
| The number of patients requesting for rescue analgesics | 8 (35%) | 10 (43%) | 0.763 |
| Morphine equivalent dose of analgesics, mg | 1.8 ± 2.7 | 2.4 ± 3.0 | 0.528 |
| The number of patients receiving additional antiemetic agents | 0 (0%) | 2 (9%) | 0.489 |
| Time to first passing of gas, h | 80.7 ± 21.0 | 72.8 ± 14.9 | 0.145 |
| Length of postoperative hospital stay, d | 5 (5–11) | 5 (5–8) | 0.150 |
| Satisfaction of surgeon | 0.014 * | ||
| 2 | 3 (13%) | 0 (0%) | |
| 3 | 7 (30%) | 2 (9%) | |
| 4 | 11 (48%) | 12 (52%) | |
| 5 | 2 (9%) | 9 (39%) | |
| Postoperative complications | 0.200 | ||
| Pleural effusion | 3 (13%) | 0 (0%) | |
| Intraperitoneal infection | 1 (4%) | 1 (4%) | |
| Ileus | 0 (0%) | 1 (4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, M.H.; Kim, N.Y.; Yoo, Y.C.; Kong, H.J.; Lee, H.S.; Jo, A.; Bai, S.J. Influence of Deep Neuromuscular Blockade on Perioperative Stress Response in Patients Undergoing Robot-Assisted Gastrectomy: A Prospective Double-Blinded Randomized-Controlled Trial. J. Pers. Med. 2021, 11, 1308. https://doi.org/10.3390/jpm11121308
Kim MH, Kim NY, Yoo YC, Kong HJ, Lee HS, Jo A, Bai SJ. Influence of Deep Neuromuscular Blockade on Perioperative Stress Response in Patients Undergoing Robot-Assisted Gastrectomy: A Prospective Double-Blinded Randomized-Controlled Trial. Journal of Personalized Medicine. 2021; 11(12):1308. https://doi.org/10.3390/jpm11121308
Chicago/Turabian StyleKim, Myoung Hwa, Na Young Kim, Young Chul Yoo, Hee Jung Kong, Hye Sun Lee, Arim Jo, and Sun Joon Bai. 2021. "Influence of Deep Neuromuscular Blockade on Perioperative Stress Response in Patients Undergoing Robot-Assisted Gastrectomy: A Prospective Double-Blinded Randomized-Controlled Trial" Journal of Personalized Medicine 11, no. 12: 1308. https://doi.org/10.3390/jpm11121308
APA StyleKim, M. H., Kim, N. Y., Yoo, Y. C., Kong, H. J., Lee, H. S., Jo, A., & Bai, S. J. (2021). Influence of Deep Neuromuscular Blockade on Perioperative Stress Response in Patients Undergoing Robot-Assisted Gastrectomy: A Prospective Double-Blinded Randomized-Controlled Trial. Journal of Personalized Medicine, 11(12), 1308. https://doi.org/10.3390/jpm11121308