

Can Blood Flow Restriction Be the Key to Reducing Quadriceps Weakness in the Early and Mid-Phases After Anterior Cruciate Ligament Reconstruction with a Hamstring Graft? A Systematic Review of Randomized Controlled Trials

 , , ,
, , ,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
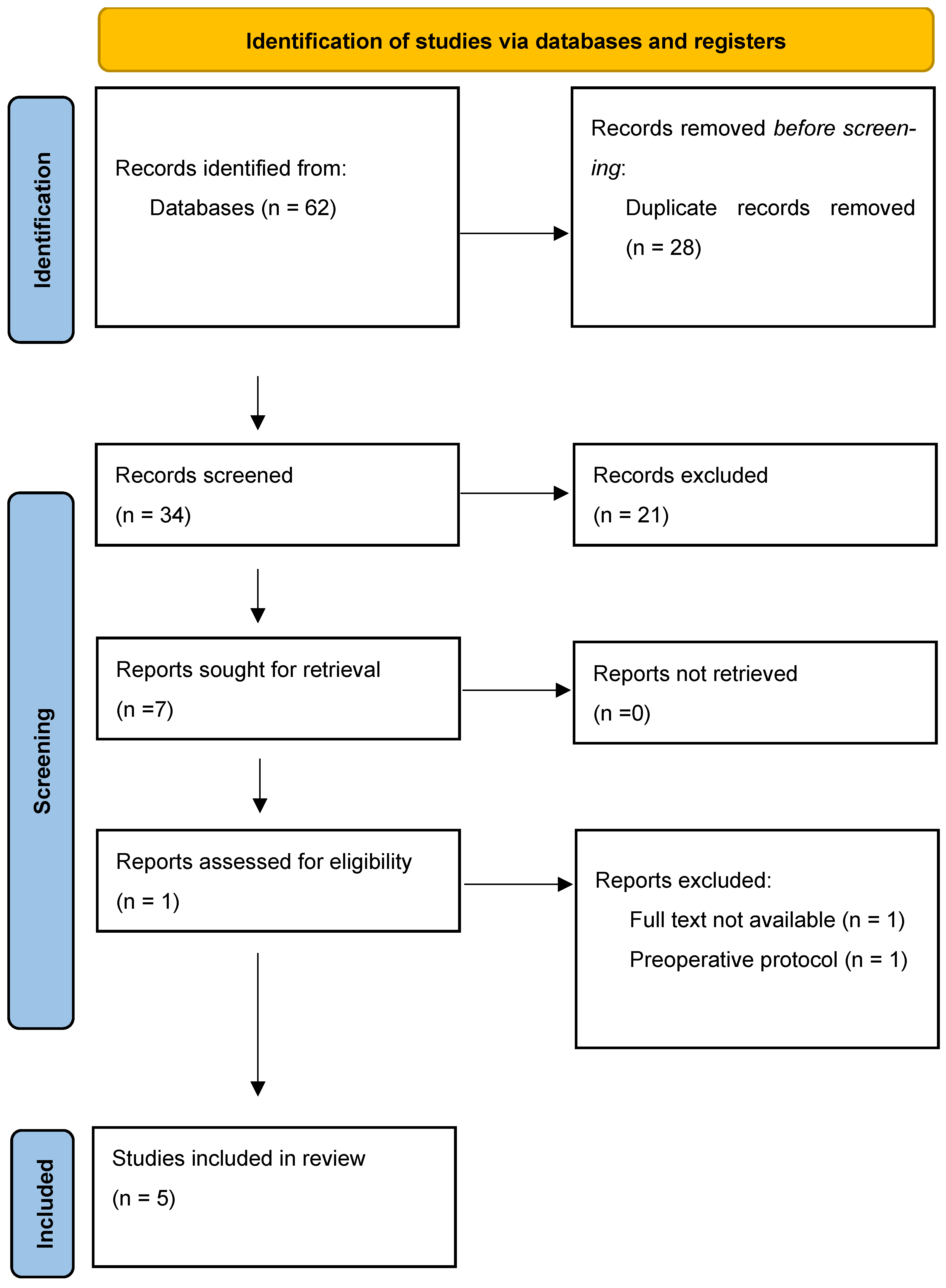
2.2. Information Sources, Literature Search, and Selection of Sources of Evidence
2.3. Data Extraction and Quality Assessment
3. Results
Data Quality
4. Discussion
4.1. Limitations
4.2. Clinical Implications and Perspectives
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Joseph, A.M.; Collins, C.L.; Henke, N.M.; Yard, E.E.; Fields, S.K.; Comstock, R.D. A Multisport Epidemiologic Comparison of Anterior Cruciate Ligament Injuries in High School Athletics. J. Athl. Train. 2013, 48, 810. [Google Scholar] [CrossRef] [PubMed]
- Vincelot-Chainard, C.; Buisson, X.; Taburet, J.-F.; Djian, P.; Robert, H. ACL autograft reconstruction revisions with tendon allografts: Possibilities and outcomes. A one-year follow-up of 39 patients. Orthop. Traumatol. Surg. Res. 2022, 108, 102832. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.; Mabrouk, A.; Nielson, J.L. Anterior Cruciate Ligament Knee Injury. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Lefevre, N.; Klouche, S.; Herman, S.; Bohu, Y. Les facteurs de risques de rupture du ligament croisé antérieur: Le genre féminin. J. Traumatol. Sport. 2014, 31, 58–62. [Google Scholar] [CrossRef]
- Filbay, S.R.; Grindem, H. Evidence-based recommendations for the management of anterior cruciate ligament (ACL) rupture. Best. Pract. Res. Clin. Rheumatol. 2019, 33, 33–47. [Google Scholar] [CrossRef]
- Kotsifaki, R.; Korakakis, V.; King, E.; Barbosa, O.; Maree, D.; Pantouveris, M.; Whiteley, R. Aspetar clinical practice guideline on rehabilitation after anterior cruciate ligament reconstruction. Br. J. Sports Med. 2023, 57, 500–514. [Google Scholar] [CrossRef]
- Palmieri-Smith, R.M.; Lepley, L.K. Quadriceps Strength Asymmetry After Anterior Cruciate Ligament Reconstruction Alters Knee Joint Biomechanics and Functional Performance at Time of Return to Activity. Am. J. Sports Med. 2015, 43, 1662–1669. [Google Scholar] [CrossRef]
- Hart, J.M.; Pietrosimone, B.; Hertel, J.; Ingersoll, C.D. Quadriceps activation following knee injuries: A systematic review. J. Athl. Train. 2010, 45, 87–97. [Google Scholar] [CrossRef]
- Lepley, L.K. Deficits in Quadriceps Strength and Patient-Oriented Outcomes at Return to Activity After ACL Reconstruction: A Review of the Current Literature. Sports Health 2015, 7, 231–238. [Google Scholar] [CrossRef]
- Hughes, L.; Paton, B.; Rosenblatt, B.; Gissane, C.; Patterson, S.D. Blood flow restriction training in clinical musculoskeletal rehabilitation: A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1003–1011. [Google Scholar] [CrossRef]
- Patterson, S.D.; Hughes, L.; Warmington, S.; Burr, J.; Scott, B.R.; Owens, J.; Loenneke, J. Blood Flow Restriction Exercise: Considerations of Methodology, Application, and Safety. Front. Physiol. 2019, 10, 533. [Google Scholar] [CrossRef]
- Caetano, D.; Oliveira, C.; Correia, C.; Barbosa, P.; Montes, A.; Carvalho, P. Rehabilitation outcomes and parameters of blood flow restriction training in ACL injury: A scoping review. Phys. Ther. Sport 2021, 49, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Herbawi, F.; Lozano-Lozano, M.; Lopez-Garzon, M.; Postigo-Martin, P.; Ortiz-Comino, L.; Martin-Alguacil, J.L.; Fernandez-Lao, C. A Systematic Review and Meta-Analysis of Strength Recovery Measured by Isokinetic Dynamometer Technology after Anterior Cruciate Ligament Reconstruction Using Quadriceps Tendon Autografts vs. Hamstring Tendon Autografts or Patellar Tendon Autografts. Int. J. Environ. Res. Public Health 2022, 19, 6764. [Google Scholar] [CrossRef] [PubMed]
- Fujita, S.; Abe, T.; Drummond, M.J.; Cadenas, J.G.; Dreyer, H.C.; Sato, Y.; Rasmussen, B.B. Blood flow restriction during low-intensity resistance exercise increases S6K1 phosphorylation and muscle protein synthesis. J. Appl. Physiol. Bethesda Md. 2007, 103, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Dolin, R.; Ben Zaki, B. L’entraînement sous restriction du flux sanguin, ou «Blood Flow Restriction», une alternative au renforcement musculaire à charge élevée. Kinésithérapie Rev. 2022, 22, 34–40. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Erickson, L.N.; Lucas, K.C.H.; Davis, K.A.; Jacobs, C.A.; Thompson, K.L.; Hardy, P.A.; Andersen, A.H.; Fry, C.S.; Noehren, B.W. Effect of Blood Flow Restriction Training on Quadriceps Muscle Strength, Morphology, Physiology, and Knee Biomechanics Before and After Anterior Cruciate Ligament Reconstruction: Protocol for a Randomized Clinical Trial. Phys. Ther. 2019, 99, 1010–1019. [Google Scholar] [CrossRef]
- Hughes, L.; Rosenblatt, B.; Haddad, F.; Gissane, C.; McCarthy, D.; Clarke, T.; Ferris, G.; Dawes, J.; Paton, B.; Patterson, S.D. Comparing the Effectiveness of Blood Flow Restriction and Traditional Heavy Load Resistance Training in the Post-Surgery Rehabilitation of Anterior Cruciate Ligament Reconstruction Patients: A UK National Health Service Randomised Controlled Trial. Sports Med. 2019, 49, 1787–1805. [Google Scholar] [CrossRef]
- Curran, M.T.; Bedi, A.; Mendias, C.L.; Wojtys, E.M.; Kujawa, M.V.; Palmieri-Smith, R.M. Blood Flow Restriction Training Applied with High-Intensity Exercise Does Not Improve Quadriceps Muscle Function After Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial. Am. J. Sports Med. 2020, 48, 825–837. [Google Scholar] [CrossRef]
- Kacin, A.; Drobnič, M.; Marš, T.; Miš, K.; Petrič, M.; Weber, D.; Tomc Žargi, T.; Martinčič, D.; Pirkmajer, S. Functional and molecular adaptations of quadriceps and hamstring muscles to blood flow restricted training in patients with ACL rupture. Scand. J. Med. Sci. Sports 2021, 31, 1636–1646. [Google Scholar] [CrossRef]
- Vieira de Melo, R.F.; Komatsu, W.R.; Freitas, M.S.; de Vieira de Melo, M.E.; Cohen, M. Comparison of Quadriceps and Hamstring Muscle Strength after Exercises with and without Blood Flow Restriction following Anterior Cruciate Ligament Surgery: A Randomized Controlled Trial. J. Rehabil. Med. 2022, 54, jrm00337. [Google Scholar] [CrossRef]
- Pignanelli, C.; Christiansen, D.; Burr, J.F. Blood flow restriction training and the high-performance athlete: Science to application. J. Appl. Physiol. Bethesda Md. 2021, 130, 1163–1170. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Construct | Keywords |
|---|---|
| Population | Anterior cruciate ligament reconstruction, Anterior cruciate ligament reconstruction graft, Anterior cruciate ligament reconstruction surgery |
| Concept | Blood flow restriction, Blood flow restriction therapy, Blood Flow Restriction Training |
| Context | Muscular strengthening, Resistance training, Strength training, Strengthening program |
| References | Study Title | Aim of the Study | Country of Study | N (Participants) |
|---|---|---|---|---|
| Erickson et al. [17] (2019) | Effect of Blood Flow Restriction Training on Quadriceps Muscle Strength, Morphology, Physiology and Knee Biomechanics Before and After Anterior Cruciate Ligament Reconstruction | Evaluate the effect of BFR-RT on quadriceps strength and knee biomechanics, and identify the potential mechanism(s) of action of BFR-RT at the cellular and morphological levels of the quadriceps. | USA (University of Kentucky) | A total of 60 patients (male or female, 15–40 years) with an isolated ACL tear or with a meniscus tear, without a specified graft type. They were randomly assigned to the following groups:
|
| Hughes et al. [18] (2019) | Comparing the Effectiveness of Blood Flow Restriction and Traditional Heavy Load Resistance Training in the Post-Surgery Rehabilitation of Anterior Cruciate Ligament Reconstruction | Compare the efficacy of BFR-RT and traditional heavy-load training (HL-RT) in improving skeletal muscle hypertrophy and strength, physical function, pain, and effusion in patients undergoing anterior cruciate ligament reconstruction. | UK (National Health Service) | A total of 28 patients (11 women and 17 men, age: 29 ± 7 years) underwent unilateral autograft surgery with a graft from the hamstrings. They were randomly assigned to the following groups:
|
| Curran et al. [19] (2019) | Blood Flow Restriction Training Applied with High-Intensity Exercise does not improve Quadriceps Muscle Function After Anterior Cruciate Ligament Reconstruction | Examine the efficacy of BFR-RT with high-intensity exercise on the recovery of quadriceps muscle function in patients after anterior cruciate ligament reconstruction. | USA (University of Michigan) | A total of 34 patients (19 women, 15 men, age: 16.5 ± 2.7 years) who had undergone ACLR were randomly assigned to one of four groups:
|
| Kacin et al. [20] (2021) | Functional and molecular adaptations of quadriceps and hamstring muscles to blood flow restricted training in patients with ACL rupture | Determine whether LL-BFR-RT can increase motor function and the size of quadriceps and hamstring muscles in patients after ACL reconstruction. | Slovenia (Ljubljana) | A total of 18 participants (9 women and 9 men, age: 37.5 ± 9 years) underwent ACLR. A total of 12 people were divided into three groups:
|
| De Melo et al. [21] (2022) | Comparison of Quadriceps and Hamstring Muscle Strength After Exercises with and without Blood Flow Restriction Following Anterior Cruciate Ligament Surgery | Compare quadriceps and hamstring muscle strength gain in patients after ACL reconstruction surgery using exercises with and without BFR-RT. | Brazil (University of São Paulo) | A total of 28 participants (male and female, age: 18–59) underwent ACLR using a hamstring autograft.The were randomly assigned to the following groups:
|
| References | Duration | nterventions | Main Findings |
|---|---|---|---|
| Erickson et al. [17] |
| BFR-RT: Stopped 4 months post-surgery for isolated ACL, or 5 months if meniscus repair is included. Pressure defined by manufacturer. Placebo: Minimal pressure (<20 mm Hg). All participants focused on quadriceps strengthening. |
|
| Hughes et al. [18] | 8 weeks 2X/week (16 sessions), beginning on day 14 post-op | BFR-RT group:
Both groups followed a standard rehab program 3X/week at home. |
|
| Curran et al. [19] | 8 weeks 2X/week (16 sessions), starting 10 weeks post-op | All participants followed standard rehabilitation. 1RM assessed on first day, then weekly. Experimental (BFR-RT): five sets of 10 reps at 70% of 1RM unilateral leg press with 2 min rest between sets; cuff deflated during rest and reinflated for sets. Pressure: 80% of LOP (110–186 mmHg). Control: Same exercises and intensity without occlusion. |
|
| Kacin et al. [20] | 3 weeks 3X/week for nine sessions | BFR-RT group: four sets of knee extension and flexion at 40RM until failure with operated leg only, workload constant. Cuff pressure: 150 mmHg. Isotonic knee extension with 45 s rest between first and third sets without reperfusion; 90 s reperfusion after second set. Same protocol for knee flexion. Placebo: Same protocol with cuff inflated to 20 mmHg. |
|
| De Melo et al. [21] | 12 weeks 2X/week | BFR-RT group: four sets (1×30, 3X15), with 30 s rest between sets, at 30% MR. Pressure: 80% of LOP. Control group: three sets of 10 reps at 70% of 1RM. Pressure maintained during all reps. 1RM tests conducted on leg press and flexion machine for BFR training on injured then uninjured leg. |
|
| Erickson et al. [17] | Hughes et al. [18] | Curran et al. [19] | Kacin et al. [20] | De Melo et al. [21] | |
|---|---|---|---|---|---|
| Randomization sequence generation |  | | | | |
| Allocation concealment | | | |  | |
| Performance biases | | | | | |
| Detection biases | | | | |  |
| Migration biases | | | | | |
| Notification biases | | | | | |
| Other sources of bias | | | | | |
. High risk of bias: . Risk of bias undetermined: .Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moiroux--Sahraoui, A.; Mazeas, J.; Blossier, M.; Douryang, M.; Kakavas, G.; Hewett, T.E.; Forelli, F. Can Blood Flow Restriction Be the Key to Reducing Quadriceps Weakness in the Early and Mid-Phases After Anterior Cruciate Ligament Reconstruction with a Hamstring Graft? A Systematic Review of Randomized Controlled Trials. Diagnostics 2025, 15, 382. https://doi.org/10.3390/diagnostics15030382
Moiroux--Sahraoui A, Mazeas J, Blossier M, Douryang M, Kakavas G, Hewett TE, Forelli F. Can Blood Flow Restriction Be the Key to Reducing Quadriceps Weakness in the Early and Mid-Phases After Anterior Cruciate Ligament Reconstruction with a Hamstring Graft? A Systematic Review of Randomized Controlled Trials. Diagnostics. 2025; 15(3):382. https://doi.org/10.3390/diagnostics15030382
Chicago/Turabian StyleMoiroux--Sahraoui, Ayrton, Jean Mazeas, Marine Blossier, Maurice Douryang, Georges Kakavas, Timothy E. Hewett, and Florian Forelli. 2025. "Can Blood Flow Restriction Be the Key to Reducing Quadriceps Weakness in the Early and Mid-Phases After Anterior Cruciate Ligament Reconstruction with a Hamstring Graft? A Systematic Review of Randomized Controlled Trials" Diagnostics 15, no. 3: 382. https://doi.org/10.3390/diagnostics15030382
APA StyleMoiroux--Sahraoui, A., Mazeas, J., Blossier, M., Douryang, M., Kakavas, G., Hewett, T. E., & Forelli, F. (2025). Can Blood Flow Restriction Be the Key to Reducing Quadriceps Weakness in the Early and Mid-Phases After Anterior Cruciate Ligament Reconstruction with a Hamstring Graft? A Systematic Review of Randomized Controlled Trials. Diagnostics, 15(3), 382. https://doi.org/10.3390/diagnostics15030382