
A Systematic Review: The Role of Artificial Intelligence in Lung Cancer Screening in Detecting Lung Nodules on Chest X-Rays

 ,
,  , ,
, ,
Abstract
1. Introduction
1.1. Background
1.2. Objective of the Review
- Evaluate and compare the performance of AI algorithms against radiologists in detecting lung nodules in CXRs.
- Analyze performance variations of AI algorithms and radiologists based on nodule sizes, morphology, and locations of the nodules.
- Identify and examine factors contributing to discrepancies between AI and radiologist interpretations in lung nodule detection.
- Investigate patterns of missed lung nodules when comparing AI algorithms with radiologists in chest radiograph interpretation.
2. Materials and Methods
2.1. Reference Source (PRISMA)
2.2. Formation of Research Questions
2.3. Systematic Search Strategy
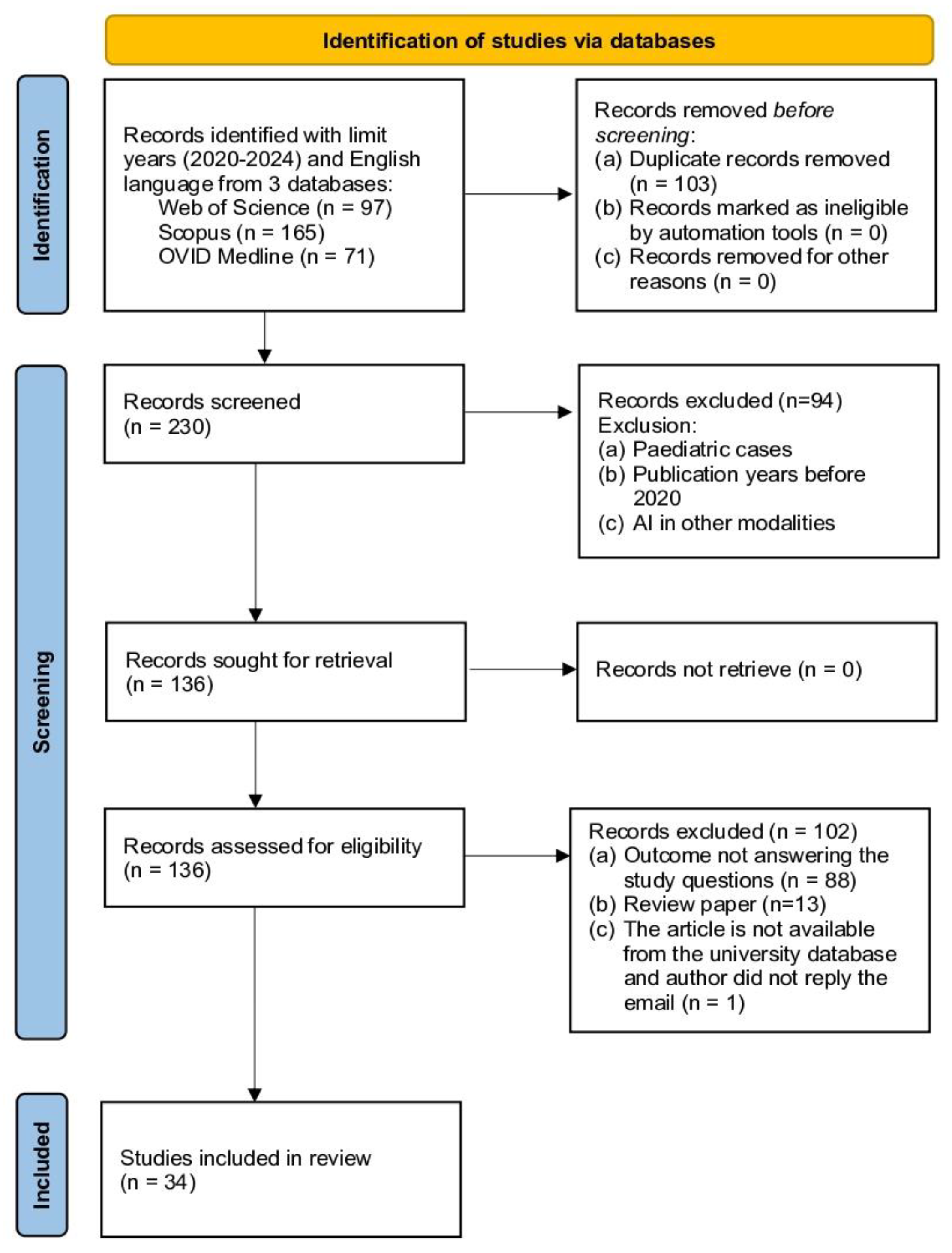
2.3.1. Identification
2.3.2. Screening
2.3.3. Eligibility
2.4. Evaluation of Article Quality
2.5. Data Extraction and Synthesis
3. Results
3.1. Overview of the Study
3.2. Study Design and Population

{kind=link}
| Author and Year | Country | Study Design | Study Population | Study Setting |
|---|---|---|---|---|
| Nam et al., 2020 [13] | Republic of Korea | Retrospective case-control study | 168 patients (mean age 71.9 ± 9.5 years) with 187 initially undetected lung cancer nodules, plus 50 normal controls; CT or X-ray validated; from March 2017 until December 2018 | A single center |
| Sim et al., 2020 [30] | Republic of Korea | Retrospective cross-sectional study | 800 radiographs (200 per center: 150 cancer cases, 50 normal); from October 2015 until September 2017 | Four tertiary hospitals |
| Lee et al., 2020 [32] | Republic of Korea | Retrospective cross-sectional study | Two cohorts: validation (10,289 X-rays from 10,206 individuals) and screening (100,576 X-rays from 50,098 individuals) | Seoul National University Hospital |
| Koo et al., 2020 [33] | Republic of Korea | Retrospective cross-sectional study | 378 patients (61% male; mean age 61.4 years) with ≤three pathologically proven nodules; excluding nodules < 5 mm or calcified; from January 2016 until December 2018 | Tertiary hospital |
| Majkowska et al., 2020 [38] | India | Retrospective cross-sectional study | Two datasets: DS1 (759,611 X-rays from 538,390 patients) with natural prevalence; ChestX-ray14 (112,120 X-rays from 30,805 patients) enriched for abnormalities | Five Indian centers (DS1) and NIH database (ChestX-ray14) |
| Yoo et al., 2020 [15] | United States | Retrospective cross-sectional study | 5485 high-risk smokers (age 55–74 years; ≥30 pack-years; 55.2% male) receiving three annual screenings; from August 2002 until April 2004 | NLST multicenter trial (21 sites) |
| Teng et al., 2021 [35] | Taiwan | Retrospective cross-sectional study | 100 subjects with CXR (47 with CT-validated nodules or masses, 53 normal); mean age 55.07 ± 13.80 years | A single center |
| Yoo et al., 2021 [41] | United States | Retrospective cross-sectional study | 519 screening X-rays from 294 patients (98 cancer cases, 196 controls); from August 2002 until April 2004 | NLST trial dataset |
| Homayounieh et al., 2021 [44] | Germany | Retrospective cross-sectional study | Adult patients of both genders with PA chest radiographs; including cases with nodules, non-nodular abnormalities, and normal findings | Two sites (A and B) |
| Tam et al., 2021 [49] | United Kingdom | Retrospective cross-sectional study | 400 cases (200 tumors, 200 controls); mean ages 72.6 and 61.8 years; seven years retrospective review | NHS setting |
| Peters et al., 2021 [50] | Switzerland | Experiment study | 61 chest phantoms with 140 solid lung nodules were placed in artificial lung parenchyma (53 phantoms with lung nodules and eight without nodules). | A phantom study using PACS-workstation |
| Nam et al., 2022 [25] | Republic of Korea | Retrospective cohort study | 6452 health checkup participants (52% male; mean age 57.6 ± 13.0 years); a subset of 3073 with CT validation | Seoul National University Healthcare Screening Center |
| Bae et al., 2022 [31] | Republic of Korea | Retrospective cross-sectional study | 111 patients with PA chest radiographs including 49 patients with 83 pulmonary nodules; excluding complex pathologies and CT-only visible nodules; from April 2016 until December 2019 | A single center |
| Chiu et al., 2022 [36] | Taiwan | Retrospective cross-sectional study | Adults (≥20 years) with single lung nodule confirmed by biopsy/resection; plus, cases from four external datasets; from 2011 until 2014 | Taipei Veterans General Hospital |
| Kaviani et al., 2022 [37] | United States | Retrospective cross-sectional study | 2407 adults (≥21 years; 1248 males; mean age 39 years); de-identified CXR data; from 2015 until 2021 | Eight sites (three in India, five in the US); including quaternary and community hospitals |
| Govindarajan et al., 2022 [14] | India | Prospective cross-sectional study | 65,604 CXRs (median age 42 years); PA/AP views; excluding incomplete/artifact cases | 35 centers across Six Indian states |
| Ahn et al., 2022 [40] | United States | Retrospective cohort study | Adult patients with specific radiograph findings (pneumonia, nodules, pneumothorax, pleural effusion) | Deaconess Medical Centre and Massachusetts General Hospital |
| Nam et al., 2023 [23] | Republic of Korea | Randomized control trial | 10,476 adults (>18 years) undergoing chest radiography; median age 59 years; 5121 men; from June 2020 until December 2021 | Tertiary hospital health screening center |
| You et al., 2023 [24] | Republic of Korea | Retrospective cross-sectional study | 300 patients: 100 normal cases (50% male, mean age 46.5 years) and 200 with pulmonary nodules (57% male, mean age 60.0 years) | A single tertiary hospital |
| Hwang et al., 2023 [26] | Republic of Korea | Retrospective cross-sectional study | 73 first-visit outpatients (median age 70 years) with AI-detected incidental nodules; excluding known thoracic cases | Hospital outpatient clinic |
| Huh et al., 2023 [27] | Republic of Korea | Retrospective case-control study | 100 cases (50 pathologically confirmed lung cancers, 50 normal); December 2015 until February 2021 | Seoul National University Hospital (tertiary) |
| Kim et al., 2023 [28] | Republic of Korea | Retrospective cross-sectional study | Training set (n = 998; 54% male; mean age 54.2 years) plus two validation sets (n = 246 and n = 205); including normal and nodule cases; from November 2015 until July 2019 | Severance Hospital, Pusan National University Hospital and Dongsan Medical Centre |
| Kwak et al., 2023 [29] | Republic of Korea | Retrospective cross-sectional study | Patients with incidentally detected, pathologically proven resectable lung cancer; referred from various departments; from March 2020 until February 2022 | A single center |
| Lee et al., 2023 [17] | Republic of Korea | Retrospective cross-sectional study | 120 cases (60 biopsy-proven cancers from 5647 registry, 60 controls); expert-annotated with CT validation; from December 2015 until February 2021 | Seoul National University Hospital, Korea |
| Ueno et al., 2023 [16] | Japan | Retrospective cross-sectional study | 388 patients with suspected lung cancer; required both CT and CXR (PA view) within one-month intervals; from June 2020 until May 2022 | Single institution, |
| Higuchi et al., 2023 [34] | Japan | Retrospective cross-sectional study | 5800 CXRs total: 800 from Fukushima (50% normal, 50% nodules) and 5000 from the NIH dataset | Fukushima health centre and NIH database |
| Farouk et al., 2023 [39] | Egypt | Retrospective cross-sectional study | 150 adults with varied lung pathologies; requiring both X-ray and CT; excluding poor-quality images and complex cases; from May 2021 until July 2022 | Ain Sham University |
| Tang et al., 2023 [43] | Australia | Retrospective cross-sectional study | Volunteer radiologists evaluating three AI interfaces vs. no AI in paired-reader design | Royal Melbourne Hospital |
| Bennani et al., 2023 [45] | France | Retrospective cross-sectional study | 500 patients (52% female; mean age 54 ± 19 years) with paired CXR and CT within 72 h; From emergency, inpatient, and day hospital settings; from January 2010 until December 2020 | Cochin Hospital, Paris, France |
| Maiter et al., 2023 [48] | United Kingdom | Retrospective cross-sectional study | 5722 radiographs from 5592 adults (53.8% female; median age 59 years); from July 2020 until February 2021 | Sheffield Teaching Hospitals (tertiary) |
| Hamanaka et al., 2024 [18] | Japan | Retrospective cross-sectional study | Patients who underwent malignant lung tumor resection; from November 2021 until July 2023 | Shin-Yurigaoka General Hospital |
| Kirshenboim et al., 2024 [42] | Israel | Retrospective cross-sectional study | 683 chest radiographs from an initial pool of 50,286; excluding interpreted cases and duplicates | A single center |
| Topff et al., 2024 [46] | The Netherland | Retrospective cross-sectional study | 25,104 radiographs from 21,039 adults (≥18 years; mean age 61.1 ± 16.2 years); Institution 1 (April 2021–February 2022) and Institution 2 (January–December 2018) | Two institutions |
| van Leeuwen et al., 2024 [47] | The Netherland | Retrospective cohort study | Two cohorts: 95 hand radiographs (age range 0–18 years; from January 2017–January 2022) and 140 chest radiographs (January 2012–May 2022); CT-validated reference standard | Seven Dutch hospitals |
3.3. Performance in Lung Nodule Detection of AI Algorithms and Radiologists
3.4. AI and Radiologist Performance Across Nodule Size, Morphological Type, and Location
3.5. Factors Contributing to AI-Radiologist Discrepancies
3.6. Pattern of Missed Lung Nodule Findings: AI Versus Radiologist
| Author and Year | Performance | Nodule Characteristics (Morphology Type, Size, and Location) | Discrepancies Factors Between AI and Radiologists in Lung Nodule Detection | The Pattern of Missed Lung Nodule Finding | |||
|---|---|---|---|---|---|---|---|
| AI | Radiologist | Combined | AI | Radiologist | |||
| Nam et al., 2020 [13] |
Software: Lunit INSIGHT CXR version 1.0.1.1 (Lunit Inc., Seoul, Republic of Korea) |
| AI-aided radiologists improve AUROC to 0.685–0.724 |
|
|
Radiologist challenges:
| N/A |
| Sim et al., 2020 [30] | Sensitivity: 67.3% FPPI: 0.2 Software: Samsung Auto Lung Nodule Detection-ALND, version 1.00 (Suwon, Republic of Korea) | Sensitivity: 65.1% FPPI: 0.2 | Radiologists’ sensitivity with DCNN: 70.3% FPPI: 0.18 | N/A |
| The DCNN software improved the sensitivity of radiologists, irrespective of radiologist experience, nodule characteristics, or the vendor of the radiography acquisition system | AI helped find 15% of missed nodules from standalone sessions |
| Lee et al., 2020 [32] | Validation test performance:
Screening cohort performance:
Software: Lunit INSIGHT CXR version 4.7.2 (Lunit Inc., Seoul, Republic of Korea) |
| N/A | N/A | N/A | AI performance improved with increased visibility of lung cancer in radiographs | N/A |
| Koo et al., 2020 [33] |
Software: Lunit INSIGHT CXR, version 1.00 (Lunit Inc., Seoul, Republic of Korea) |
|
| DCNN is better at the detection of nodules larger than 5 mm, solid, round-shaped, well-marginated, and laterally located nodules. DCNN struggles with masked nodules due to overlapping structure and GGO-dominant nodules | The radiologist missed a masked nodule due to overlapping with bony lesions and a GGO-dominant nodule in the upper left lobe | Radiologist interpretation errors due to:
DCNN limitations:
|
|
| Majkowska et al., 2020 [38] | Sensitivity
CNN architecture: Xception | Sensitivity
| N/A | N/A | N/A |
| N/A |
| Yoo et al., 2020 [15] | All radiograph
Digital radiograph
Malignant nodule detection:
Software: Lunit INSIGHT CXR, version not stated (Lunit Inc., Seoul, Republic of Korea) | All radiograph
Digital radiograph
Malignant nodule detection:
| N/A | N/A | N/A |
| Missed cases in nodule detection
Missed cases in cancer detection
Missed cases in malignant nodules
|
| Teng et al., 2021 [35] |
Software: QUIBIM Chest X-ray Classifier (Valencia, Spain) |
| N/A | N/A | N/A | N/A | N/A |
| Yoo et al., 2021 [41] | N/A | Radiology residents
Radiologist
| Radiology residents with AI
Radiologist with AI
Software: Lunit INSIGHT CXR version 2.4.11.0 (Lunit Inc., Seoul, Republic of Korea) |
|
| AI benefits for different experience levels:
|
|
| Homayounieh et al., 2021 [44] | N/A |
|
Software: AI-Rad Companion Chest X-ray Algorithm (Siemens Healthineers AG, Erlangen, Germany) | AI improved detection across all difficulty nodule levels (easy, moderate, and challenging) | N/A |
|
|
| Tam et al., 2021 [49] |
Software: Red Dot (Behold.ai, London, UK) |
|
| Overall sensitivity increases with tumor size 1–2 cm | N/A |
|
|
| Peters et al., 2021 [50] |
Software: InferRead®DR (Infervision Technology Ltd., Beijing, China) |
| N/A |
|
|
| AI-CAD identified lesions missed by radiologists although had reduced overall sensitivity compared to radiologists |
| Nam et al., 2022 [25] |
Software: Lunit INSIGHT CXR version 2.0, Lunit Inc, Seoul, Republic of Korea |
|
| The median nodule detection size was 1.2 cm | N/A | N/A | N/A |
| Bae et al., 2022 [31] | N/A |
Sensitivity use of CXR alone:
| Sensitivity withBSt-DE:
Sensitivity with BSp-DL:
| BSt-DE has good performance with small nodules, bone overlapping, and peripheral location | N/A |
| |
| Chiu et al., 2022 [36] |
Deep Learning architecture: You Only Look Once version 4 (YOLOv4) |
| N/A |
| N/A |
|
|
| Kaviani et al., 2022 [37] |
Software: qXR (Qure.Ai Technology, Mumbai, India) | N/A | N/A | AI has higher performance on detection of calcified nodules—calcified nodules (AUC 0.71) vs. non-calcified nodules (AUC 0.55) | N/A | Radiologist challenges:
AI challenges:
| AI detected 69/131 (53%) of missed lung nodules |
| Govindarajan et al., 2022 [14] | AI performance in categorizing normal and abnormal CXR (use radiologist as reference standard)
AI performance in categorizing CXR into sub abnormality (in this case lung nodule)
Software: qXR (Qure.Ai Technology, Mumbai, India) | N/A | Turnaround time of radiologists is reduced with AI assistance specifically:
| N/A | N/A |
| N/A |
| Ahn et al., 2022 [40] |
Software: Lunit INSIGHT CXR, version 3.1.2.0 (Lunit Inc., Seoul, Republic of Korea) |
| Reading time improved with AI assistance with an overall reduction was 3.9 s (p < 0.001) | N/A | N/A | Factors that influence reader performance with AI:
Impact of extensive AI output:
| N/A |
| Nam et al., 2023 [23] |
Software: Lunit INSIGHT CXR version 2.0.2.0 (Lunit Inc., Seoul, Republic of Korea) |
| AI-based CAD improved actionable lung nodule detection (odds ratio: 2.4) | AI improved the detection rate of
| N/A | N/A | N/A |
| You et al., 2023 [24] |
Software: Med-Chest X-ray System, version 1.0.1, (VUNO, Seoul, Republic of Korea) | N/A | Non-expert radiologists: improved DZ nodule detection with DLD | DLD has better performance for:
| N/A | Factors affecting DLD performance:
Data quantity vs. performance:
| N/A |
| Hwang et al., 2023 [26] |
Software: Lunit INSIGHT CXR version 3, Lunit Inc., Seoul, Republic of Korea) | N/A | N/A | False positive due to:
| N/A | Imaging challenges:
|
|
| Huh et al., 2023 [27] | N/A | Expert performance (seven experts)
|
Software: Lunit INSIGHT CXR version 4.7.2 (Lunit Inc., Seoul, Republic of Korea) | Limitations in the detection of those non-visible malignant nodules or obscured by anatomical structure (bone, heart, diaphragm, and mediastinum) | Limitations in the detection of those non-visible malignant nodules or obscured by anatomical structure (bone, heart, diaphragm, and mediastinum) |
| N/A |
| Kim et al., 2023 [28] |
| Radiologists’ mean sensitivity: 77.5% |
| DLBS model improved detection across nodule types by suppressing bone structures (rib, clavicle, and other anatomic structures) | N/A | N/A | N/A |
| Kwak et al., 2023 [29] |
Software: Lunit INSIGHT CXR, version 2 and 3 (Lunit Inc., Seoul, Republic of Korea) | N/A | N/A | Nodule Characteristics detected by AI:
| N/A | N/A | N/A |
| Lee et al., 2023 [17] | High Diagnostic Accuracy (full dataset) AI Performance:
CNN architecture: ResNet34 |
| Readers with high diagnostic accuracy AI:
Readers with low diagnostic accuracy AI (no significant improvement):
| N/A | N/A |
| N/A |
| Ueno et al., 2023 [16] |
Software: EIRL Chest X-ray Lung Nodule (LPIXEL Inc., Tokyo, Japan) | N/A | N/A |
| N/A | Challenges for radiologists:
| N/A |
| Higuchi et al., 2023 [34] | Sensitivity
Specificity
AUC
CNN architecture: CheXNet model |
| N/A | N/A | N/A | A massive teaching dataset is needed to increase the accuracy of the AI | N/A |
| Farouk et al., 2023 [39] |
Software: Lunit INSIGHT CXR version 2.4.11.0 (Lunit Inc., Seoul, Republic of Korea) |
|
|
|
| AI and radiologists cannot detect nodules at blind or obscured areas on CXR |
|
| Tang et al., 2023 [43] | N/A | Sensitivity of radiologists without AI: 64% Specificity of radiologists without AI: 88% AUC of radiologist without AI: 0.82 | Sensitivity of radiologist with
Specificity of radiologist with
AUC of radiologist with
Software: Annalise Enterprise CXR (Annalise.ai, Sydney, Australia) | N/A | N/A |
| N/A |
| Bennani et al., 2023 [45] | N/A | Sensitivity without AI
Specificity without AI
| Sensitivity with AI
Specificity with AI
Software: ChestView version 1.2.0 (Gleamer, Paris, France) | AI increase detection of small nodules that are usually overlooked | N/A | Reader-AI interaction:
|
|
| Maiter et al., 2023 [48] | Compared with suspicious nodules:
Compared with cancer diagnosis:
Software: ALND version 1.0 (Samsung Electronics, Suwon, Republic of Korea) |
| N/A | N/A | N/A | AI challenges:
|
|
| Hamanaka et al., 2024 [18] | AI detection rate:
Software: EIRL X-ray Lung Nodule version 1.12 (LPIXEL Inc., Tokyo, Japan) | N/A | N/A |
| N/A |
|
|
| Kirshenboim et al., 2024 [42] |
Software: Lunit INSIGHT CXR version 2.0.2.0 (Lunit Inc., Seoul, Republic of Korea) | N/A |
| N/A | N/A | AI software limitations:
|
|
| Topff et al., 2024 [46] | N/A | N/A | N/A |
| N/A |
|
|
| van Leeuwen et al., 2024 [47] |
*** Software used |
| N/A |
| Decrease performance with lower nodule conspicuity | The difference in image reading platforms compare to clinical practice and absence of clinical information may contribute to discrepancies between AI and radiologists | N/A |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| AUROC | Area under the receiver operating characteristic |
| AUC | Area under the curve |
| CAD | Computer-aided detection |
| CXR | Chest X-ray |
| DLAD | Deep learning-based automatic detection |
| GGO | Ground-glass opacity |
| LDCT | Low-dose computed tomography |
| NPV | Negative predictive value |
| PPV | Positive predictive value |
References
- Xia, C.; Dong, X.; Li, H.; Cao, M.; Sun, D.; He, S.; Yang, F.; Yan, X.; Zhang, S.; Li, N. Cancer statistics in China and United States, 2022: Profiles, trends, and determinants. Chin. Med. J. 2022, 135, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Teh, H.; Woon, Y. Burden of cancers attributable to modifiable risk factors in Malaysia. BMC Public Health 2021, 21, 410. [Google Scholar] [CrossRef]
- Rajadurai, P.; How, S.H.; Liam, C.K.; Sachithanandan, A.; Soon, S.Y.; Tho, L.M. Lung cancer in Malaysia. J. Thorac. Oncol. 2020, 15, 317–323. [Google Scholar] [CrossRef]
- National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef]
- Dwyer, L.L.; Vadagam, P.; Vanderpoel, J.; Cohen, C.; Lewing, B.; Tkacz, J. Disparities in lung cancer: A targeted literature review examining lung cancer screening, diagnosis, treatment, and survival outcomes in the United States. J. Racial Ethn. Health Disparities 2024, 11, 1489–1500. [Google Scholar] [CrossRef] [PubMed]
- Thames, M.; Liu, J.; Colditz, G.; James, A. Urban–Rural Disparities in Access to Low-Dose Computed Tomography Lung Cancer Screening in Missouri and Illinois. PCD Staff 2020, 17, E140. [Google Scholar]
- Alberto, N.R.I.; Alberto, I.R.I.; Puyat, C.V.M.; Antonio, M.A.R.; Ho, F.D.V.; Dee, E.C.; Mahal, B.A.; Eala, M.A.B. Disparities in access to cancer diagnostics in ASEAN member countries. Lancet Reg. Health–West. Pac. 2023, 32, 100667. [Google Scholar] [CrossRef]
- Sahar, L.; Douangchai Wills, V.L.; Liu, K.K.; Fedewa, S.A.; Rosenthal, L.; Kazerooni, E.A.; Dyer, D.S.; Smith, R.A. Geographic access to lung cancer screening among eligible adults living in rural and urban environments in the United States. Cancer 2022, 128, 1584–1594. [Google Scholar] [CrossRef] [PubMed]
- Ueda, D.; Yamamoto, A.; Shimazaki, A.; Walston, S.L.; Matsumoto, T.; Izumi, N.; Tsukioka, T.; Komatsu, H.; Inoue, H.; Kabata, D. Artificial intelligence-supported lung cancer detection by multi-institutional readers with multi-vendor chest radiographs: A retrospective clinical validation study. BMC Cancer 2021, 21, 1120. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.; Song, H.; Shin, Y.J.; Kim, J.; Kim, J.; Lee, K.W.; Lee, S.S.; Lee, W.; Lee, S.; Lee, K.H. Deep learning–based automatic detection algorithm for reducing overlooked lung cancers on chest radiographs. Radiology 2020, 296, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Chassagnon, G.; Vakalopoulou, M.; Paragios, N.; Revel, M.-P. Artificial intelligence applications for thoracic imaging. Eur. J. Radiol. 2020, 123, 108774. [Google Scholar] [CrossRef] [PubMed]
- Hwang, E.J.; Park, S.; Jin, K.-N.; Im Kim, J.; Choi, S.Y.; Lee, J.H.; Goo, J.M.; Aum, J.; Yim, J.-J.; Cohen, J.G. Development and validation of a deep learning–based automated detection algorithm for major thoracic diseases on chest radiographs. JAMA Netw. Open 2019, 2, e191095. [Google Scholar] [CrossRef]
- Nam, J.G.; Hwang, E.J.; Kim, D.S.; Yoo, S.-J.; Choi, H.; Goo, J.M.; Park, C.M. Undetected lung cancer at posteroanterior chest radiography: Potential role of a deep learning–based detection algorithm. Radiol. Cardiothorac. Imaging 2020, 2, e190222. [Google Scholar] [CrossRef]
- Govindarajan, A.; Govindarajan, A.; Tanamala, S.; Chattoraj, S.; Reddy, B.; Agrawal, R.; Iyer, D.; Srivastava, A.; Kumar, P.; Putha, P. Role of an automated deep learning algorithm for reliable screening of abnormality in chest radiographs: A prospective multicenter quality improvement study. Diagnostics 2022, 12, 2724. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.; Kim, K.H.; Singh, R.; Digumarthy, S.R.; Kalra, M.K. Validation of a deep learning algorithm for the detection of malignant pulmonary nodules in chest radiographs. JAMA Netw. Open 2020, 3, e2017135. [Google Scholar] [CrossRef] [PubMed]
- Ueno, M.; Yoshida, K.; Takamatsu, A.; Kobayashi, T.; Aoki, T.; Gabata, T. Deep learning-based automatic detection for pulmonary nodules on chest radiographs: The relationship with background lung condition, nodule characteristics, and location. Eur. J. Radiol. 2023, 166, 111002. [Google Scholar] [CrossRef]
- Lee, J.H.; Hong, H.; Nam, G.; Hwang, E.J.; Park, C.M. Effect of human-AI interaction on detection of malignant lung nodules on chest radiographs. Radiology 2023, 307, e222976. [Google Scholar] [CrossRef] [PubMed]
- Hamanaka, R.; Oda, M. Can Artificial Intelligence Replace Humans for Detecting Lung Tumors on Radiographs? An Examination of Resected Malignant Lung Tumors. J. Pers. Med. 2024, 14, 164. [Google Scholar] [CrossRef]
- Goncalves, S.; Fong, P.-C.; Blokhina, M. Artificial intelligence for early diagnosis of lung cancer through incidental nodule detection in low-and middle-income countries-acceleration during the COVID-19 pandemic but here to stay. Am. J. Cancer Res. 2022, 12, 1. [Google Scholar] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Richardson, W.S.; Wilson, M.C.; Nishikawa, J.; Hayward, R.S. The well-built clinical question: A key to evidence-based decisions. ACP J. Club 1995, 123, A12–A13. [Google Scholar] [CrossRef] [PubMed]
- Abouzahra, A.; Sabraoui, A.; Afdel, K. Model composition in Model Driven Engineering: A systematic literature review. Inf. Softw. Technol. 2020, 125, 106316. [Google Scholar] [CrossRef]
- Nam, J.G.; Hwang, E.J.; Kim, J.; Park, N.; Lee, E.H.; Kim, H.J.; Nam, M.; Lee, J.H.; Park, C.M.; Goo, J.M. AI Improves Nodule Detection on Chest Radiographs in a Health Screening Population: A Randomized Controlled Trial. Radiology 2023, 307, e221894. [Google Scholar] [CrossRef]
- You, S.; Park, J.H.; Park, B.; Shin, H.-B.; Ha, T.; Yun, J.S.; Park, K.J.; Jung, Y.; Kim, Y.N.; Kim, M. The diagnostic performance and clinical value of deep learning-based nodule detection system concerning influence of location of pulmonary nodule. Insights Into Imaging 2023, 14, 149. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.G.; Kim, H.J.; Lee, E.H.; Hong, W.; Park, J.; Hwang, E.J.; Park, C.M.; Goo, J.M. Value of a deep learning-based algorithm for detecting Lung-RADS category 4 nodules on chest radiographs in a health checkup population: Estimation of the sample size for a randomized controlled trial. Eur. Radiol. 2022, 32, 213–222. [Google Scholar] [CrossRef]
- Hwang, S.H.; Shin, H.J.; Kim, E.-K.; Lee, E.H.; Lee, M. Clinical outcomes and actual consequence of lung nodules incidentally detected on chest radiographs by artificial intelligence. Sci. Rep. 2023, 13, 19732. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.E.; Lee, J.H.; Hwang, E.J.; Park, C.M. Effects of expert-determined reference standards in evaluating the diagnostic performance of a deep learning model: A malignant lung nodule detection task on chest radiographs. Korean J. Radiol. 2023, 24, 155. [Google Scholar] [CrossRef]
- Kim, H.; Lee, K.H.; Han, K.; Lee, J.W.; Kim, J.Y.; Im, D.J.; Hong, Y.J.; Choi, B.W.; Hur, J. Development and validation of a deep learning–based synthetic bone-suppressed model for pulmonary nodule detection in chest radiographs. JAMA Netw. Open 2023, 6, e2253820. [Google Scholar] [CrossRef] [PubMed]
- Kwak, S.H.; Kim, E.K.; Kim, M.H.; Lee, E.H.; Shin, H.J. Incidentally found resectable lung cancer with the usage of artificial intelligence on chest radiographs. PLoS ONE 2023, 18, e0281690. [Google Scholar] [CrossRef]
- Sim, Y.; Chung, M.J.; Kotter, E.; Yune, S.; Kim, M.; Do, S.; Han, K.; Kim, H.; Yang, S.; Lee, D.-J. Deep convolutional neural network–based software improves radiologist detection of malignant lung nodules on chest radiographs. Radiology 2020, 294, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Bae, K.; Oh, D.Y.; Yun, I.D.; Jeon, K.N. Bone suppression on chest radiographs for pulmonary nodule detection: Comparison between a generative adversarial network and dual-energy subtraction. Korean J. Radiol. 2022, 23, 139. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Sun, H.Y.; Park, S.; Kim, H.; Hwang, E.J.; Goo, J.M.; Park, C.M. Performance of a deep learning algorithm compared with radiologic interpretation for lung cancer detection on chest radiographs in a health screening population. Radiology 2020, 297, 687–696. [Google Scholar] [CrossRef] [PubMed]
- Koo, Y.H.; Shin, K.E.; Park, J.S.; Lee, J.W.; Byun, S.; Lee, H. Extravalidation and reproducibility results of a commercial deep learning-based automatic detection algorithm for pulmonary nodules on chest radiographs at tertiary hospital. J. Med. Imaging Radiat. Oncol. 2020, 65, 15–22. [Google Scholar] [CrossRef]
- Higuchi, M.; Nagata, T.; Iwabuchi, K.; Sano, A.; Maekawa, H.; Idaka, T.; Yamasaki, M.; Seko, C.; Sato, A.; Suzuki, J. Development of a novel artificial intelligence algorithm to detect pulmonary nodules on chest radiography. Fukushima J. Med. Sci. 2023, 69, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Teng, P.-H.; Liang, C.-H.; Lin, Y.; Alberich-Bayarri, A.; González, R.L.; Li, P.-W.; Weng, Y.-H.; Chen, Y.-T.; Lin, C.-H.; Chou, K.-J. Performance and educational training of radiographers in lung nodule or mass detection: Retrospective comparison with different deep learning algorithms. Medicine 2021, 100, e26270. [Google Scholar] [CrossRef]
- Chiu, H.-Y.; Peng, R.H.-T.; Lin, Y.-C.; Wang, T.-W.; Yang, Y.-X.; Chen, Y.-Y.; Wu, M.-H.; Shiao, T.-H.; Chao, H.-S.; Chen, Y.-M. Artificial intelligence for early detection of chest nodules in X-ray images. Biomedicines 2022, 10, 2839. [Google Scholar] [CrossRef] [PubMed]
- Kaviani, P.; Digumarthy, S.R.; Bizzo, B.C.; Reddy, B.; Tadepalli, M.; Putha, P.; Jagirdar, A.; Ebrahimian, S.; Kalra, M.K.; Dreyer, K.J. Performance of a Chest Radiography AI Algorithm for Detection of Missed or Mislabeled Findings: A Multicenter Study. Diagnostics 2022, 12, 2086. [Google Scholar] [CrossRef]
- Majkowska, A.; Mittal, S.; Steiner, D.F.; Reicher, J.J.; McKinney, S.M.; Duggan, G.E.; Eswaran, K.; Cameron Chen, P.-H.; Liu, Y.; Kalidindi, S.R. Chest radiograph interpretation with deep learning models: Assessment with radiologist-adjudicated reference standards and population-adjusted evaluation. Radiology 2020, 294, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Farouk, S.; Osman, A.M.; Awadallah, S.M.; Abdelrahman, A.S. The added value of using artificial intelligence in adult chest X-rays for nodules and masses detection in daily radiology practice. Egypt. J. Radiol. Nucl. Med. 2023, 54, 142. [Google Scholar] [CrossRef]
- Ahn, J.S.; Ebrahimian, S.; McDermott, S.; Lee, S.; Naccarato, L.; Di Capua, J.F.; Wu, M.Y.; Zhang, E.W.; Muse, V.; Miller, B. Association of artificial intelligence–aided chest radiograph interpretation with reader performance and efficiency. JAMA Netw. Open 2022, 5, e2229289. [Google Scholar] [CrossRef]
- Yoo, H.; Lee, S.H.; Arru, C.D.; Doda Khera, R.; Singh, R.; Siebert, S.; Kim, D.; Lee, Y.; Park, J.H.; Eom, H.J.; et al. AI-based improvement in lung cancer detection on chest radiographs: Results of a multi-reader study in NLST dataset. Eur. Radiol. 2021, 31, 9664–9674. [Google Scholar] [CrossRef] [PubMed]
- Kirshenboim, Z.; Gilat, E.K.; Carl, L.; Bekker, E.; Tau, N.; Klug, M.; Konen, E.; Marom, E.M. Retrospectively assessing evaluation and management of artificial-intelligence detected nodules on uninterpreted chest radiographs in the era of radiologists shortage. Eur. J. Radiol. 2024, 170, 111241. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.S.; Lai, J.K.; Bui, J.; Wang, W.; Simkin, P.; Gai, D.; Chan, J.; Pascoe, D.M.; Heinze, S.B.; Gaillard, F. Impact of different artificial intelligence user interfaces on lung nodule and mass detection on chest radiographs. Radiol. Artif. Intell. 2023, 5, e220079. [Google Scholar] [CrossRef]
- Homayounieh, F.; Digumarthy, S.; Ebrahimian, S.; Rueckel, J.; Hoppe, B.F.; Sabel, B.O.; Conjeti, S.; Ridder, K.; Sistermanns, M.; Wang, L. An artificial intelligence–based chest X-ray model on human nodule detection accuracy from a multicenter study. JAMA Netw. Open 2021, 4, e2141096. [Google Scholar] [CrossRef]
- Bennani, S.; Regnard, N.-E.; Ventre, J.; Lassalle, L.; Nguyen, T.; Ducarouge, A.; Dargent, L.; Guillo, E.; Gouhier, E.; Zaimi, S.-H. Using AI to improve Radiologist performance in detection of abnormalities on chest Radiographs. Radiology 2023, 309, e230860. [Google Scholar] [CrossRef]
- Topff, L.; Steltenpool, S.; Ranschaert, E.R.; Ramanauskas, N.; Menezes, R.; Visser, J.J.; Beets-Tan, R.G.; Hartkamp, N.S. Artificial intelligence-assisted double reading of chest radiographs to detect clinically relevant missed findings: A two-centre evaluation. Eur. Radiol. 2024, 34, 5876–5885. [Google Scholar] [CrossRef] [PubMed]
- van Leeuwen, K.G.; Schalekamp, S.; Rutten, M.J.; Huisman, M.; Schaefer-Prokop, C.M.; de Rooij, M.; van Ginneken, B.; Maresch, B.; Geurts, B.H.; van Dijke, C.F. Comparison of commercial AI software performance for radiograph lung nodule detection and bone age prediction. Radiology 2024, 310, e230981. [Google Scholar] [CrossRef]
- Maiter, A.; Hocking, K.; Matthews, S.; Taylor, J.; Sharkey, M.; Metherall, P.; Alabed, S.; Dwivedi, K.; Shahin, Y.; Anderson, E. Evaluating the performance of artificial intelligence software for lung nodule detection on chest radiographs in a retrospective real-world UK population. BMJ Open 2023, 13, e077348. [Google Scholar] [CrossRef]
- Tam, M.; Dyer, T.; Dissez, G.; Morgan, T.N.; Hughes, M.; Illes, J.; Rasalingham, R.; Rasalingham, S. Augmenting lung cancer diagnosis on chest radiographs: Positioning artificial intelligence to improve radiologist performance. Clin. Radiol. 2021, 76, 607–614. [Google Scholar] [CrossRef]
- Peters, A.A.; Decasper, A.; Munz, J.; Klaus, J.; Loebelenz, L.I.; Hoffner, M.K.M.; Hourscht, C.; Heverhagen, J.T.; Christe, A.; Ebner, L. Performance of an AI based CAD system in solid lung nodule detection on chest phantom radiographs compared to radiology residents and fellow radiologists. J. Thorac. Dis. 2021, 13, 2728. [Google Scholar] [CrossRef] [PubMed]
| Research Questions | Motivation |
|---|---|
| How does the overall performance of AI algorithms compare to that of radiologists in detecting lung nodules in CXRs? | To assess the current state of AI technology in medical imaging and determine if AI can match or surpass human performance in this critical diagnostic task. |
| How does the performance of AI systems and radiologists vary across different nodule sizes, morphology types, and locations of lung nodules? | To identify the strengths and limitations of AI systems and radiologists across different nodule characteristics in diverse clinical scenarios. |
| What factors contribute to discrepancies between AI and radiologist interpretations? | To pinpoint areas where AI and human expertise differ, which can lead to insights for improving both AI algorithms and radiologist training. |
| What are the key patterns of missed lung nodule findings when comparing AI algorithms to radiologists in CXR interpretation across varying levels of radiologist experience and different types of nodules? | To identify specific areas where either AI or radiologists tend to make errors, considering factors such as nodule characteristics and radiologist experience. |
| Year | Number of Research | References |
|---|---|---|
| 2020 | 6 | [13,15,30,32,33,38] |
| 2021 | 6 | [35,44,49,50] |
| 2022 | 5 | [14,25,31,36,37,40] |
| 2023 | 13 | [16,17,23,24,26,27,28,29,34,39,43,45,48] |
| 2024 | 4 | [18,42,46,47] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Megat Ramli, P.N.; Aizuddin, A.N.; Ahmad, N.; Abdul Hamid, Z.; Ismail, K.I. A Systematic Review: The Role of Artificial Intelligence in Lung Cancer Screening in Detecting Lung Nodules on Chest X-Rays. Diagnostics 2025, 15, 246. https://doi.org/10.3390/diagnostics15030246
Megat Ramli PN, Aizuddin AN, Ahmad N, Abdul Hamid Z, Ismail KI. A Systematic Review: The Role of Artificial Intelligence in Lung Cancer Screening in Detecting Lung Nodules on Chest X-Rays. Diagnostics. 2025; 15(3):246. https://doi.org/10.3390/diagnostics15030246
Chicago/Turabian StyleMegat Ramli, Puteri Norliza, Azimatun Noor Aizuddin, Norfazilah Ahmad, Zuhanis Abdul Hamid, and Khairil Idham Ismail. 2025. "A Systematic Review: The Role of Artificial Intelligence in Lung Cancer Screening in Detecting Lung Nodules on Chest X-Rays" Diagnostics 15, no. 3: 246. https://doi.org/10.3390/diagnostics15030246
APA StyleMegat Ramli, P. N., Aizuddin, A. N., Ahmad, N., Abdul Hamid, Z., & Ismail, K. I. (2025). A Systematic Review: The Role of Artificial Intelligence in Lung Cancer Screening in Detecting Lung Nodules on Chest X-Rays. Diagnostics, 15(3), 246. https://doi.org/10.3390/diagnostics15030246