
The Association Between Serum Isthmin-1 and Disease Activity, Inflammation, and Autoantibody Status in Rheumatoid Arthritis

 ,
,  , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographic and Clinical Characteristics
3.2. ISM1 Levels and Autoantibody Status
3.3. ISM1 Levels According to Disease Activity
3.4. ISM1 Levels According to Disease Duration
3.5. Correlation Between Serum ISM1 Levels and Inflammatory and Disease Activity Markers
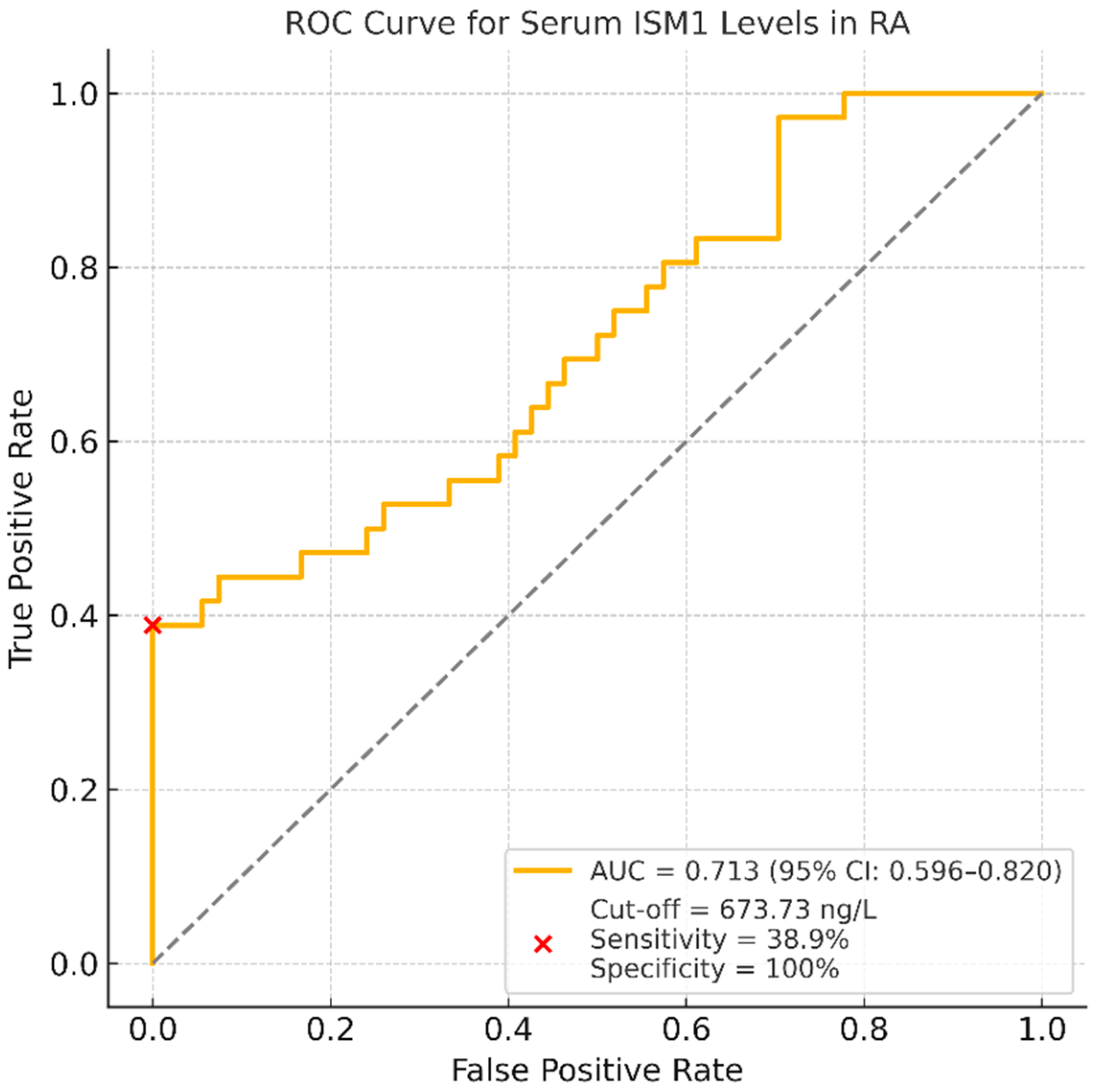
3.6. Predictive Value of Serum ISM1 Levels for Low Disease Activity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AUC | Area Under the Curve |
| BMI | Body Mass Index |
| CI | Confidence Interval |
| CRP | C-Reactive Protein |
| DAS28 | Disease Activity Score in 28 Joints |
| DMARDs | Disease-Modifying Anti-Rheumatic Drugs |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| ESR | Erythrocyte Sedimentation Rate |
| IQR | Interquartile Range |
| ISM1 | Isthmin-1 |
| NF-κB | Nuclear Factor kappa B |
| NK | Natural Killer cells |
| NKT | Natural Killer T cells |
| RA | Rheumatoid Arthritis |
| RF | Rheumatoid Factor |
| ROC | Receiver Operating Characteristic |
| SD | Standard Deviation |
| Th17 | T helper 17 cells |
| anti-CCP | Anti-Cyclic Citrullinated Peptide |
References
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef]
- McInnes, I.B.; Schett, G. The pathogenesis of rheumatoid arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef] [PubMed]
- Pera, E.M.; Kim, J.I.; Martinez, S.L.; Brechner, M.; Li, S.-Y.; Wessely, O.; De Robertis, E. Isthmin is a novel secreted protein expressed as part of the Fgf-8 synexpression group in the Xenopus midbrain–hindbrain organizer. Mech. Dev. 2002, 116, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Zhang, X.; Gao, Y.-P.; Hu, Y.-X.; Teng, T.; Wang, S.-S.; Tang, Q.-Z. Isthmin-1 Improves Aging-Related Cardiac Dysfunction in Mice through Enhancing Glycolysis and SIRT1 Deacetylase Activity. Aging Dis. 2024, 15, 2682–2696. [Google Scholar] [CrossRef] [PubMed]
- Menghuan, L.; Yang, Y.; Qianhe, M.; Na, Z.; Shicheng, C.; Bo, C.; XueJie, Y. Advances in research of biological functions of Isthmin-1. J. Cell Commun. Signal. 2023, 17, 507–521. [Google Scholar] [CrossRef]
- Valle-Rios, R.; Maravillas-Montero, J.L.; Burkhardt, A.M.; Martinez, C.; Buhren, B.A.; Homey, B.; Gerber, P.A.; Robinson, O.; Hevezi, P.; Zlotnik, A. Isthmin 1 is a secreted protein expressed in skin, mucosal tissues, and NK, NKT, and th17 cells. J. Interferon Cytokine Res. 2014, 34, 795–801. [Google Scholar] [CrossRef]
- Wu, Y.; Liang, X.; Ni, J.; Zhao, R.; Shao, S.; Lu, S.; Han, W.; Yu, L. Effect of ISM1 on the immune microenvironment and epithelial-mesenchymal transition in colorectal cancer. Front. Cell Dev. Biol. 2021, 9, 681240. [Google Scholar] [CrossRef]
- Shakhawat, H.M.; Hazrat, Z.; Zhou, Z. Isthmin—A multifaceted protein family. Cells 2022, 12, 17. [Google Scholar] [CrossRef]
- Nguyen, N.; Xu, S.; Lam, T.Y.W.; Liao, W.; Wong, W.S.F.; Ge, R. ISM1 suppresses LPS-induced acute lung injury and post-injury lung fibrosis in mice. Mol. Med. 2022, 28, 72. [Google Scholar] [CrossRef]
- Firestein, G.S.; McInnes, I.B. Immunopathogenesis of rheumatoid arthritis. Immunity 2017, 46, 183–196. [Google Scholar] [CrossRef]
- Wang, Y.; Wu, H.; Deng, R. Angiogenesis as a potential treatment strategy for rheumatoid arthritis. Eur. J. Pharmacol. 2021, 910, 174500. [Google Scholar] [CrossRef] [PubMed]
- Shanmugasundaram, M.; Xu, S.; Yang, Y.; Tee, J.H.; Lam, T.Y.W.; Ge, R. Ism1 deficiency in mice exacerbates bleomycin-induced pulmonary fibrosis with enhanced cellular senescence and delayed fibrosis resolution. hLife 2024, 2, 342–359. [Google Scholar] [CrossRef]
- Sahiri, V.; Caron, J.; Roger, E.; Desterke, C.; Ghachem, K.; Mohamadou, I.; Serre, J.; Prakoura, N.; Fellahi, S.; Placier, S. The angiogenesis inhibitor Isthmin-1 (Ism1) is Overexpressed in experimental models of Glomerulopathy and impairs the viability of Podocytes. Int. J. Mol. Sci. 2023, 24, 2723. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Zhang, X.; Hu, C.; Ma, Z.-G.; Wang, S.-S.; Teng, T.; Zeng, X.-F.; Tang, Q.-Z. Isthmin-1 alleviates cardiac ischaemia/reperfusion injury through cGMP-PKG signalling pathway. Cardiovasc. Res. 2024, 120, 1051–1064. [Google Scholar] [CrossRef]
- Sebastian Herlitz-Cifuentes, H.; Carola Fernandez Garces, P.; Ivone Lamperti Fernandez, L.; Alberto Guzman-Gutierrez, E. Effect of systemic inflammation on the function of insulin and glucose metabolism in rheumatoid arthritis. Curr. Diabetes Rev. 2016, 12, 156–162. [Google Scholar] [CrossRef]
- Hu, M.; Zhang, X.; Hu, C.; Teng, T.; Tang, Q.-Z. A brief overview about the adipokine: Isthmin-1. Front. Cardiovasc. Med. 2022, 9, 939757. [Google Scholar] [CrossRef]
- Liang, J.-Y.; Wei, H.-J.; Tang, Y.-Y. Isthmin: A multifunctional secretion protein. Cytokine 2024, 173, 156423. [Google Scholar] [CrossRef]
- Lam, T.Y.W.; Nguyen, N.; Peh, H.Y.; Shanmugasundaram, M.; Chandna, R.; Tee, J.H.; Ong, C.B.; Hossain, M.Z.; Venugopal, S.; Zhang, T.; et al. ISM1 protects lung homeostasis via cell-surface GRP78-mediated alveolar macrophage apoptosis. Proc. Natl. Acad. Sci. USA 2022, 119, e2019161119. [Google Scholar] [CrossRef]
- Tee, J.H.; Vijayakumar, U.; Shanmugasundaram, M.; Lam, T.Y.W.; Liao, W.; Yang, Y.; Wong, W.S.F.; Ge, R. Isthmin-1 attenuates allergic Asthma by stimulating adiponectin expression and alveolar macrophage efferocytosis in mice. Respir. Res. 2023, 24, 269. [Google Scholar] [CrossRef]
- Sun, S.-C.; Chang, J.-H.; Jin, J. Regulation of nuclear factor-κB in autoimmunity. Trends Immunol. 2013, 34, 282–289. [Google Scholar] [CrossRef]
- Rao, N.; Lee, Y.F.; Ge, R. Novel endogenous angiogenesis inhibitors and their therapeutic potential. Acta Pharmacol. Sin. 2015, 36, 1177–1190. [Google Scholar] [CrossRef] [PubMed]
- Osório, L.; Wu, X.; Zhou, Z. Distinct spatiotemporal expression of ISM1 during mouse and chick development. Cell Cycle 2014, 13, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Liao, H.; Zheng, J.; Lu, J.; Shen, H.-L. NF-κB Signaling Pathway in Rheumatoid Arthritis: Mechanisms and Therapeutic Potential. Mol. Neurobiol. 2025, 62, 6998–7021. [Google Scholar] [CrossRef] [PubMed]
- Makarov, S.S. NF-κB in rheumatoid arthritis: A pivotal regulator of inflammation, hyperplasia, and tissue destruction. Arthritis Res. Ther. 2001, 3, 200–206. [Google Scholar] [CrossRef]
- Guo, Q.; Jin, Y.; Chen, X.; Ye, X.; Shen, X.; Lin, M.; Zeng, C.; Zhou, T.; Zhang, J. NF-κB in biology and targeted therapy: New insights and translational implications. Signal Transduct. Target. Ther. 2024, 9, 53. [Google Scholar] [CrossRef]
- Herrington, F.D.; Carmody, R.J.; Goodyear, C.S. Modulation of NF-κB signaling as a therapeutic target in autoimmunity. J. Biomol. Screen. 2016, 21, 223–242. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Control Group (n = 30) | RA Group (n = 90) | p | |
|---|---|---|---|
| Age (Years) | 52.5 ± 6.43 (53.5) | 54.4 ± 11.2 (56) | 0.207 + |
| Gender (Female %) | 70% (n = 21) | 72.2% (n = 65) | 0.815 # |
| BMI (kg/m2) | 23.8 ± 1.18 (24) | 23.9 ± 2.65 (24) | 0.797 + |
| Glucose (mg/dL) | 87.3 ± 3.25 (87) | 98.6 ± 36.9 (86) | 0.730 + |
| AST (U/L) | 27.1 ± 7.82 | 24.7 ± 23.0 | 0.579 * |
| ALT (U/L) | 20.8 ± 2.64 (21) | 20.1 ± 5.16 (20) | 0.655 + |
| Urea (mg/dL) | 28.3 ± 3.74 (29) | 28.8 ± 8.68 (28) | 0.745 + |
| Creatinine (mg/dL) | 0.707 ± 0.136 | 0.757 ± 0.282 | 0.348 * |
| Uric acid (mg/dL) | 4.56 ± 0.741 (4.70) | 4.50 ± 1.34 (4.35) | 0.271 + |
| Total protein (g/dL) | 6.88 ± 0.225 (6.90) | 6.94 ± 0.517 (7.00) | 0.391 + |
| Albumin (g/dL) | 4.20 ± 0.244 | 4.30 ± 0.334 | 0.134 * |
| WBCs (10 × 103/µL) | 8613 ± 1478 (8725) | 8204 ± 2782 (7720) | 0.098 + |
| Lym (10 × 103/µL) | 2294 ± 347 (2275) | 2316 ± 525 (2250) | 0.995 + |
| Platelet (/µL) | 269,833 ± 70,472 | 287,900 ± 98,488 | 0.356 * |
| Hemoglobin (g/dL) | 13.5 ± 0.38 (13.6) | 12.8 ± 1.51 (12.8) | 0.001 + |
| CRP (mg/L) | 4.57 ± 1.30 (4.0) | 13.7 ± 20.3 (7.18) | 0.004 + |
| ESR (mm/h) | 16.7 ± 3.55 (16) | 30.1 ± 18.4 (29) | <0.001 + |
| ISM-1 (ng/L) | 972 ± 809 (678) | 454 ± 378 (342) | <0.001 + |
| ISM-1 (ng/L) | p | Cohen’s d | ||||
|---|---|---|---|---|---|---|
| Mean ± SD | Median | IQR | ||||
| Rf status | Positive (n = 59) | 383 ± 286 | 312 | 160 | 0.004 | 0.561 |
| Negative (n = 31) | 589 ± 487 | 421 | 384 | |||
| Anti-CCP status | Positive (n = 76) | 385 ± 247 | 329 | 171 | 0.007 | 1.091 |
| Negative (n = 14) | 750 ± 637 | 437 | 697 | |||
| Rf and Anti-CCP status | Positive (n = 58) | 333 ± 176 | 303 | 150 | <0.001 | 0.945 |
| Negative (n = 32) | 653 ± 518 | 443 | 539 | |||
| 95% CI | ||||||||
|---|---|---|---|---|---|---|---|---|
| Mean ± SD | IQR | Median | Lower | Upper | p | Cohen’s d | ||
| Healthy Control Group (n = 30) | ISM1 (ng/L) | 972 ± 809 | 710 | 678 | 670 | 1274 | ||
| RA (DAS28 CRP ≥ 3.2) (n = 54) | 315 ± 125 | 184 | 311 | 281 | 349 | <0.001 * 0.002 # | 1.337 * 1.027 # | |
| RA (DAS28 CRP < 3.2) (n = 36) | 663 ± 515 | 584 | 407 | 488 | 837 | 0.104 * | ||
| RA (DAS28 ESR ≥ 3.2) (n = 59) | 317 ± 116 | 165 | 306 | 286 | 347 | <0.001 * <0.001 + | 1.374 * 1.215 + | |
| RA (DAS28 ESR < 3.2) (n = 31) | 716 ± 539 | 654 | 475 | 518 | 913 | 0.334 * | ||
| Variable | Spearman’s Rho (rs) | p |
|---|---|---|
| ESR | −0.291 | 0.001 |
| CRP | −0.342 | <0.001 |
| DAS28 ESR | −0.385 | <0.001 |
| DAS28 CRP | −0.405 | <0.001 |
| Model | Predictor | β Coefficient | 95% CI (Lower–Upper) | p | VIF |
|---|---|---|---|---|---|
| Model 1 (DAS28-CRP) | Const | 1724.38 | 722.63 to 2726.12 | 0.001 | 195.07 |
| DAS28_CRP | −147.76 | −217.80 to −77.72 | <0.001 | 1.36 | |
| Age | −3.00 | −10.00 to 4.01 | 0.397 | 1.18 | |
| Gender | 8.95 | −174.21 to 192.11 | 0.923 | 1.31 | |
| BMI | −7.25 | −36.15 to 21.65 | 0.619 | 1.13 | |
| Hb | −29.05 | −85.29 to 27.19 | 0.307 | 1.39 | |
| CRP | 3.50 | −0.94 to 7.94 | 0.121 | 1.57 | |
| ESR | −3.37 | −8.32 to 1.58 | 0.179 | 1.60 | |
| Model 2 (DAS28-ESR) | Const | 1815.66 | 827.43 to 2803.89 | 0.000 | 196.91 |
| DAS28_ESR | −151.32 | −216.52 to −86.13 | <0.001 | 1.58 | |
| Age | −2.68 | −9.54 to 4.18 | 0.439 | 1.18 | |
| Gender | 12.23 | −167.59 to 192.05 | 0.893 | 1.31 | |
| BMI | −6.44 | −34.83 to 21.95 | 0.653 | 1.13 | |
| Hb | −38.61 | −93.59 to 16.37 | 0.166 | 1.38 | |
| CRP | 1.45 | −2.75 to 5.66 | 0.494 | 1.46 | |
| ESR | 0.13 | −5.29 to 5.56 | 0.962 | 2.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oz, B.; Gunduz, I.; Yamancan, G.; Dogan, Y.; Akkoc, R.F.; Gozel, N.; Gur, M.; Karatas, A.; Koca, S.S. The Association Between Serum Isthmin-1 and Disease Activity, Inflammation, and Autoantibody Status in Rheumatoid Arthritis. Diagnostics 2025, 15, 1316. https://doi.org/10.3390/diagnostics15111316
Oz B, Gunduz I, Yamancan G, Dogan Y, Akkoc RF, Gozel N, Gur M, Karatas A, Koca SS. The Association Between Serum Isthmin-1 and Disease Activity, Inflammation, and Autoantibody Status in Rheumatoid Arthritis. Diagnostics. 2025; 15(11):1316. https://doi.org/10.3390/diagnostics15111316
Chicago/Turabian StyleOz, Burak, Ibrahım Gunduz, Gulsah Yamancan, Yusuf Dogan, Ramazan Fazıl Akkoc, Nevzat Gozel, Mustafa Gur, Ahmet Karatas, and Suleyman Serdar Koca. 2025. "The Association Between Serum Isthmin-1 and Disease Activity, Inflammation, and Autoantibody Status in Rheumatoid Arthritis" Diagnostics 15, no. 11: 1316. https://doi.org/10.3390/diagnostics15111316
APA StyleOz, B., Gunduz, I., Yamancan, G., Dogan, Y., Akkoc, R. F., Gozel, N., Gur, M., Karatas, A., & Koca, S. S. (2025). The Association Between Serum Isthmin-1 and Disease Activity, Inflammation, and Autoantibody Status in Rheumatoid Arthritis. Diagnostics, 15(11), 1316. https://doi.org/10.3390/diagnostics15111316