Abstract
Quality improvement is an emerging field, that applies principles of improvement science and utilizes measurement methods with the aim of improving patient care. Systemic sclerosis (SSc) is a systemic autoimmune rheumatic disease associated with increased healthcare burden, cost, morbidity, and mortality. Gaps in delivering care to patients with SSc have been consistently observed. In this article, we introduce the discipline of quality improvement and its use of quality measures. We summarize and comparatively evaluate three sets of quality measures that have been proposed to evaluate the quality of care of patients with SSc. Finally, we highlight the areas of unmet needs and indicate future directions for quality improvement and quality measures in SSc.
1. Introduction
Systemic sclerosis (SSc) is a complex, multi-systemic rheumatic autoimmune disease with associated increased healthcare burden, cost, morbidity, and mortality [1,2]. While it occurs more commonly in women, it is a more aggressive disease in men [3,4,5]. Disease manifestations can vary across ethnicities [6,7] and adversely affects the ability to maintain gainful employment [8,9] and quality of life [10]. Gaps in delivering care to patients with SSc have been consistently observed. One retrospective cohort study showed low numbers of SSc patients who received baseline screening tests and specialty consultations [11]. Another national cross-sectional survey study observed significant variability in the use of diagnostic tests and management among SSc specialty centers [12].
The evaluation of quality in healthcare and the field of quality improvement has rapidly evolved in recent years. The Health and Medicine Division of the National Academies of Sciences, Engineering, and Medicine (previously known as the Institute of Medicine) defines healthcare quality as “the degree to which healthcare services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge” [13]. Multiple North American reports have demonstrated that healthcare quality is suboptimal [13,14,15], thus highlighting the need to improve care quality and prompting efforts to enhance healthcare quality. Quality improvement is a systematic approach of analyzing healthcare performance and the efforts made to improve it [16]. The discipline of quality improvement is underpinned by improvement science theory, and it utilizes measurement methods and tools and applies best practices in its implementation of sustainable quality improvement.
2. What Are Quality Measures?
Health quality must be measured to ensure that high-quality care is delivered [17,18]. Quality measures are evidence-based tools designed to help quantify the quality of care, inform systems’ performance, and identify potential healthcare gaps [18,19,20]. This term is often interchangeably used with quality indicators [21]. Quality measures are implemented into clinical practice for many purposes, such as quality improvement initiatives, accreditation, public accountability, and research. They are crucial to all stakeholders at all levels. Physicians may use them to evaluate their practices and implement positive change. Patients can use them to select their providers (in healthcare systems that allow them to) or to evaluate their personal outcomes. Finally, payers and regulators can use them to guide resource allocation and possibly reimbursement [21].
Quality measures are categorized into five major groups: structural measures (innate characteristics of the system and its providers), process measures (what health providers do to people), outcome measures (what happens to people in terms of their health), access, and patient experience [18,20]. A quality measure is composed of: a title; a numerator, which includes the outcome or process of interest during a specified risk period; and a denominator, which includes the population being measured during a reporting period [22]. The definitions and examples of quality measures are summarized in Table 1.

Table 1.
Healthcare quality measure domains and systemic sclerosis-related examples.
3. Quality Measures in Rheumatology
There have been significant shortcomings in delivering care in rheumatology [23,24]. The range of deficits includes increased wait times [25,26,27], suboptimal adherence to quality indicators and guidelines [28,29,30,31,32,33,34], decreased rates of vaccination in immunocompromised patients [35,36], and significant care gaps in youth transitioning from pediatric to adult care [37] across multiple rheumatic conditions. The most crucial and current gold standard step in measuring healthcare quality is through rigorously validated quality indicators that measure processes and outcomes [38]. Quality measures in rheumatology generally focus on process measures as outcomes tend to take years to develop, and they are often influenced by non-quality-related factors (i.e., medical comorbidities, social determinants of health, lifestyle choices, and environmental factors), making them very challenging to accurately measure [39]. Furthermore, if outcome measures are to be used, they must be adjusted for case mix differences (such as the patient’s age or disease severity) to control for their role in influencing the outcome of interest. Such adjustments are needed to ensure that the quality of care delivered is accurately reflected [21].
In efforts that have been made to bridge the quality gap, several quality indicator sets have been developed in many rheumatological conditions, including systemic autoimmune rheumatic diseases (ARDs) [40,41,42,43,44,45], metabolic conditions [46,47], and osteoarthritis [48]. National and international organizations then endorse the quality indicators. They are the basis for developing key performance indicators or performance measures used to quantify care quality for use by professional organizations, governmental, or private entities [23].
The American College of Rheumatology (ACR) published its white paper on quality measures in 2011. Using modified Delphi consensus methods, they defined the essential attributes, priorities, and uses of quality measures. Four areas were identified for the development of future quality measures. These include diseases, medications, comorbidities/prevention, and access/care experience. Rheumatic diseases with the highest priority ranking were rheumatoid arthritis, osteoporosis, juvenile idiopathic arthritis, gout, ankylosing spondylitis, psoriatic arthritis, and osteoarthritis [39]. With the widespread use of electronic health records, the ACR published its first two disease-specific electronic clinical quality measures in rheumatoid arthritis and gout [49,50,51,52], both of which were considered high-priority clinical areas.
Given the significant care gap in rheumatological care and the adoption of care quality as a priority by multiple professional and governmental organizations, there has been an encouraging rise of quality improvement initiatives in rheumatology. Liu et al. summarized quality improvement efforts in adult and pediatric rheumatology from 2013 to 2018. Interventions were focused on improving screening for comorbidities, adherence to clinical practice guidelines, vaccinations, and contraception counselling [53].
4. Systemic Sclerosis Quality Measures
The first significant advancement in developing SSc-specific quality measures was in 2011; Khanna et al. developed a set of quality indicators for SSc using consensus methodology [42]. The proposed process indicators were identified based on a literature review and were sent to a group of international SSc experts who refined them. The remaining indicators were evaluated by a United States (US)-based expert panel using the RAND/UCLA appropriateness method. Finally, 32 quality indicators were deemed valid. The final set was presented to the US members of the Scleroderma Clinical Trials Consortium (SCTC), who confirmed its validity and feasibility. The quality indicators were framed in an “IF, THEN, BECAUSE” format across eight disease domains grouped by body systems. The quality indicators were further categorized into 3 different sections: baseline (for patients with a new SSc diagnosis), follow-up monitoring, and treatment (for patients with established SSc), as shown in Table 2.
Table 2.
Systemic sclerosis process of care quality indicators derived from physicians for use in the US healthcare system.
4.1. Baseline
The baseline assessment of a newly diagnosed patient should include antibody tests [54], Doppler echocardiogram, functional status (e.g., Scleroderma Health Assessment Questionnaire [55]), creatinine kinase, and pulmonary function tests, all within the first 12 months. Assessment for tendon friction rubs should occur in the first 3 months, and serum creatinine should be assessed in the first 6 months. If a patient is within the first 5 years of diagnosis, they should be counselled on weekly blood pressure monitoring. If the forced vital capacity or diffusion capacity is less than 80% of the predicted, then a high-resolution CT thorax should be offered within 12 months [42].
4.2. Monitoring
Separate quality measures are outlined for the monitoring of a SSc patient with established disease. If the patient experiences new dyspnea on exertion or a new diffusion capacity below 65%, a Doppler echocardiogram should be performed within 3 months. If the examination reveals that proximal muscle weakness and creatine phosphokinase (CPK) is at least three times the normal limit, an electromyogram, muscle biopsy, or magnetic resonance imaging should be performed. For those who have been experiencing symptoms for less than 5 years, spirometry and diffusion capacity should be conducted annually for the first five years. In the case of new dyspnea on exertion, spirometry with diffusion capacity should be conducted within 6 months. If there is interstitial lung disease revealed by chest X-ray, high-resolution CT (HRCT) of the chest, or spirometry; spirometry and diffusion capacity should be performed at least annually until the forced vital capacity (FVC) is stabilized (within 10% over 1 year). If the patient presents new dyspnea on exertion or an abnormal FVC or diffusion capacity of less than 80%, HRCT thorax should be performed within 6 months. If dyspnea on exertion is present and an echocardiogram suggests new pulmonary hypertension, referral for right heart catheterization should be conducted within 3 months. Blood pressure should be recorded during every visit. If hypertension is detected (systolic BP > 140 or diastolic BP > 90 mmHg confirmed on 2 separate occasions), creatinine, complete blood cell count, and urinalysis should be performed within 72 h. Weight or body mass index (BMI) should be recorded annually. Symptoms of gastroesophageal reflux disease should be recorded annually. Hemoglobin test should be offered at least annually [42].
4.3. Treatment
Quality measures are also outlined for the treatment of SSc patients. Inactive influenza vaccine should be offered annually, while the pneumococcal vaccine should be offered every 5 years, unless contraindicated. If symptoms of diastolic dysfunction and heart failure are present, appropriate treatment such as ACE inhibitors, diuretics, or beta-blockers should be provided within three months, or a referral to a cardiologist should be performed. For patients with NYHA/WHO functional class II–IV secondary to pulmonary arterial hypertension, as diagnosed through right heart catheterization, treatment with endothelin blockers, prostacyclin analogs, and/or PDE-5 inhibitors should be initiated within three months. For those with a decreased range of motion or function in the hand and a diagnosis of less than five years, a range-of-motion exercise program should be offered within 6 months. In cases of interstitial lung disease and a greater than 10% decline in FVC over the past 12 months, immunosuppressive treatment options such as cyclophosphamide, methotrexate, azathioprine, cyclosporine, or mycophenolate mofetil should be offered within 3 months. If a patient is experiencing scleroderma renal crisis (accelerated hypertension [at least SBP ≥ 140 and a rise of SBP ≥ 30 mmHg from baseline] or rapidly progressive renal failure), an ACE inhibitor should be prescribed within 72 h. A proton pump inhibitor or H2 blocker should be offered for patients diagnosed with GERD within 3 months of diagnosis. Symptoms of early satiety, post-prandial abdominal bloating, postprandial vomiting, or regurgitation persisting for at least 1 month should prompt testing for impaired gastric emptying or an empiric trial of therapy within 6 months. If a patient experiences unintentional weight loss of 5% or more over 3 months with symptoms of nausea, vomiting, bloating, or diarrhea for 4 weeks, testing for malabsorption or bacterial overgrowth or an empiric trial of therapy should be offered within 3 months. If a patient has digital tip ulcers, treatment with calcium channel blockers, prostacyclin therapy, topical nitrate therapy, or PDE-5 inhibitors should be prescribed within 3 months [42].
Hoffmann-Vold et al. developed tools for the annual assessment of patients with SSc to facilitate an international standardization of follow-up care [56]. Using a stepwise Delphi consensus method, 157 multidisciplinary SSc expert and non-expert physicians from the European Scleroderma Trials and Research group (EUSTAR) and SCTC rated the proposed disease domains and assessment tools by the study authors. The domains and tools were included in the final quality indicator set if they were rated higher than 80% in importance by more than 75% of participants. Ten domains were deemed important by consensus: Raynaud’s phenomenon, digital ulcers, mucocutaneous, musculoskeletal, lung, heart, gastrointestinal, renal, laboratory, and treatment. The specific symptoms and assessment tools of the domains are listed in Table 3. The investigators felt these quality indicators could be easily applied across worldwide healthcare systems, including non-academic centers.
Table 3.
Annual assessment of organ involvement in systemic sclerosis.
Spierings et al. surveyed 650 SSc patients across 13 hospitals in the Netherlands using an online questionnaire [57]. Patients were asked to rank the proposed process, and outcome quality indicators developed following focus group interviews with patients, rheumatologists, and specialized nurses. The proposed process indicators were a good physician–patient relationship, multidisciplinary collaboration, receiving guideline-directed therapy, annual evaluations of pulmonary function and skin involvement, healthcare access, counselling of non-pharmacological care, and accuracy of diagnosis. The outcome indicators suggested were the absence of organ involvement, lack of disease progression, absence of digital ulcers, improved quality of life, reduced pain, reduced fatigue, and improved hand function. Among the proposed process indicators, the top three rated indicators were: the physician–patient relationship, multidisciplinary collaboration, and receiving guideline-directed therapy. Outcome indicators that were considered most important were the absence of disease progression, the absence of organ involvement, and the absence of digital ulcers, Table 4.
Table 4.
Process and outcome quality indicators ranked by SSc patients.
5. Comparative Evaluation of SSc Quality Measures
Choosing how to measure the quality of care in SSc is a challenge. Different stakeholders (patients, physicians, nurses, allied health staff, governments, and policymakers) can have differing priorities and perspectives. Indeed, there appear to be differences in quality measures between patients and physicians. SSc experts prioritize disease-specific processes as quality measures. This is also compatible with some process indicators identified by SSc patients, such as annual lung assessments and receiving appropriate therapy.
However, patients value processes that are not specific to their disease, such as their relationship with their providers and multidisciplinary collaboration. To date, healthcare providers and researchers have not established SSc outcome indicators. However, disease outcomes are a high priority for patients. There are also differences between physician-derived quality indicator sets. Compared to the quality indicator set of Khanna et al., Hoffman et al. additionally advocate for the inclusion of indicators related to Raynaud’s phenomenon (documentation of severity and frequency of attacks), digital ulceration (new ulcer occurring in the past year), co-morbidities affecting perfusion (i.e., diabetes mellitus), smoking status, cutaneous disease (telangiectasias, calcinosis), musculoskeletal disease (arthritis), and comorbidity (heart disease).
6. Unmet Needs and Future Directions
Although there has been remarkable progress made in the quality improvement field in SSc over the last decade, much remains to be done. Rigorously developed quality measures that reflect stakeholders’ priorities are essential for measuring the quality of care delivered to patients with SSc. It is uncertain if these can be successfully adhered to. Many of the quality measures recommended for the baseline assessment of SSc as they are required for the classification of SSc [58]. Many of the quality measures recommended for the monitoring of SSc patients with established disease are implemented worldwide [59]. However, it may be challenging to adhere to so many quality indicators. If the number of quality indicators is to be reduced to a more manageable number, it should be questioned: whose perspective should be prioritized? [60,61] (Patients? Physicians? Payers?) One shared provider–patient approach is the use of a health passport, which outlines quality measures and their timing [62]. This passport could serve as a point of discussion or reminder for a quality measure to occur.
Furthermore, it is essential that quality measures for systemic sclerosis are regularly updated to reflect recent advances in the field. Examples of such advances include the 2013 ACR/EULAR classification criteria [63], the 2018 ACR/EULAR treatment guidelines [64], and the validation of multiple SSc-specific patient-reported outcomes (PROs) [65,66,67] to ensure that patients receive the most appropriate and effective care using the most current and relevant guidelines.
To date, there are no quality improvement initiatives addressing care deficiencies in SSc. Local quality improvement initiatives are needed to measure SSc quality indicators uptake and diagnose any potential deficiencies. If a quality gap is established, then rapid quality improvement cycles can be designed to address it. Rapid improvement cycles use quality improvement methodology to develop a timely and specific aim, choosing a family of process, balancing and outcome measures, and designing thoughtful interventions to address the causes of the targeted gap. Interventions are then regularly defined using plan–do–study–act (PDSA) cycles to evaluate their efficacy until the target gap is bridged [68], as shown in Figure 1.
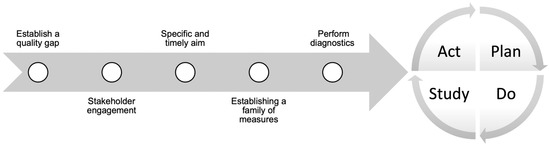
Figure 1.
Quality improvement process.
7. Conclusions
This discipline of quality improvement to improve the quality of care is rapidly evolving in rheumatology and emerging in SSc. Three sets of SSc quality indicators have been proposed. The physician-derived quality indicators are limited to process indicators. SSc quality indicators can be categorized by body system and/or function (screening, monitoring, and treatment). While there is some overlap between patient-derived and physician-derived quality indicators, patients also value outcome quality indicators. It is important for physicians to remember that patients prioritize quality indicators differently, giving higher priority to non-SSc-related quality indicators.
Funding
This research received no external funding.
Conflicts of Interest
The authors have no competing interest or conflict of interest to declare.
References
- Altman, R.D.; Medsger, T.A., Jr.; Bloch, D.A.; Michel, B.A. Predictors of survival in systemic sclerosis (scleroderma). Arthritis Rheum. 1991, 34, 403–413. [Google Scholar] [CrossRef]
- Bernatsky, S.; Hudson, M.; Panopalis, P.; Clarke, A.E.; Pope, J.; Leclercq, S.; St Pierre, Y.; Baron, M. The cost of systemic sclerosis. Arthritis Rheum. 2009, 61, 119–123. [Google Scholar] [CrossRef]
- Hussein, H.; Lee, P.; Chau, C.; Johnson, S.R. The effect of male sex on survival in systemic sclerosis. J. Rheumatol. 2014, 41, 2193–2200. [Google Scholar] [CrossRef] [PubMed]
- Pasarikovski, C.R.; Granton, J.T.; Roos, A.M.; Sadeghi, S.; Kron, A.T.; Thenganatt, J.; Moric, J.; Chau, C.; Johnson, S.R. Sex disparities in systemic sclerosis-associated pulmonary arterial hypertension: A cohort study. Arthritis Res. Ther. 2016, 18, 30. [Google Scholar] [CrossRef] [PubMed]
- Peoples, C.; Medsger, T.A., Jr.; Lucas, M.; Rosario, B.L.; Feghali-Bostwick, C.A. Gender differences in systemic sclerosis: Relationship to clinical features, serologic status and outcomes. J. Scleroderma Relat. Disord. 2016, 1, 177–240. [Google Scholar] [CrossRef] [PubMed]
- Low, A.H.; Johnson, S.R.; Lee, P. Ethnic influence on disease manifestations and autoantibodies in Chinese-descent patients with systemic sclerosis. J. Rheumatol. 2009, 36, 787–793. [Google Scholar] [CrossRef]
- Al-Sheikh, H.; Ahmad, Z.; Johnson, S.R. Ethnic variations in systemic sclerosis disease manifestations, internal organ involvement, and mortality. J. Rheumatol. 2019, 46, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Jetha, A.; Johnson, S.R.; Gignac, M.A.M. Unmet workplace support needs and lost productivity of workers with systemic sclerosis: A path analysis study. Arthritis Care Res. 2021, 73, 423–431. [Google Scholar] [CrossRef]
- Lee, J.J.Y.; Gignac, M.A.M.; Johnson, S.R. Employment outcomes in systemic sclerosis. Best. Pract. Res. Clin. Rheumatol. 2021, 35, 101667. [Google Scholar] [CrossRef]
- Johnson, S.R.; Glaman, D.D.; Schentag, C.T.; Lee, P. Quality of life and functional status in systemic sclerosis compared to other rheumatic diseases. J. Rheumatol. 2006, 33, 1117–1122. [Google Scholar]
- Johnson, S.R.; Carette, S.; Dunne, J.V. Scleroderma: Health services utilization from patients’ perspective. J. Rheumatol. 2006, 33, 1123–1127. [Google Scholar] [PubMed]
- Harding, S.; Khimdas, S.; Bonner, A.; Baron, M.; Pope, J. Best practices in scleroderma: An analysis of practice variability in SSc centres within the Canadian Scleroderma Research Group (CSRG). Clin. Exp. Rheumatol. 2012, 30, S38–S43. [Google Scholar]
- Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press (US): Washington, DC, USA, 2001.
- Kohn, L.T.; Corrigan, J.M.; Donaldson, M.S. (Eds.) To Err is Human: Building a Safer Health System; National Academies Press (US): Washington, DC, USA, 2000. [Google Scholar]
- Dhalla, I.A.; Tepper, J. Improving the quality of health care in Canada. Cmaj 2018, 190, E1162–E1167. [Google Scholar] [CrossRef] [PubMed]
- Quality Improvement Basics. Available online: https://www.aafp.org/family-physician/practice-and-career/managing-your-practice/quality-improvement-basics.html (accessed on 19 October 2022).
- Donabedian, A. The quality of care. How can it be assessed? JAMA 1988, 260, 1743–1748. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.H.; McGlynn, E.A.; Shekelle, P.G. Defining and measuring quality of care: A perspective from US researchers. Int. J. Qual. Health Care 2000, 12, 281–295. [Google Scholar] [CrossRef]
- NQMC Measure Domain Definitions: Guidelines and Measures. Available online: https://www.ahrq.gov/gam/index.html (accessed on 21 October 2022).
- Agency for Healthcare Research and Quality. NQMC Measure Domain Definitions. Available online: https://www.ahrq.gov/gam/summaries/domain-definitions/index.html (accessed on 6 December 2022).
- Wahl, E.; Makris, U.E.; Suter, L.G. Taxonomy of quality of care indicators: Tracing the path from clinical practice guidelines to quality measurement and beyond. Rheum. Dis. Clin. North Am. 2022, 48, 601–615. [Google Scholar] [CrossRef]
- Centers for Medicare & Medicaid Services (CMS). Quality Measures. Available online: https://www.cms.gov/medicare/quality-initiatives-patient-assessment-instruments/qualitymeasures (accessed on 6 December 2022).
- Yazdany, J.; MacLean, C.H. Quality of care in the rheumatic diseases: Current status and future directions. Curr. Opin. Rheumatol. 2008, 20, 159–166. [Google Scholar] [CrossRef]
- Jacobi, C.E.; Boshuizen, H.C.; Rupp, I.; Dinant, H.J.; van den Bos, G.A. Quality of rheumatoid arthritis care: The patient’s perspective. Int. J. Qual. Health Care 2004, 16, 73–81. [Google Scholar] [CrossRef][Green Version]
- Widdifield, J.; Tu, K.; Carter Thorne, J.; Bombardier, C.; Michael Paterson, J.; Liisa Jaakkimainen, R.; Wing, L.; Butt, D.A.; Ivers, N.; Hofstetter, C.; et al. Patterns of care among patients referred to rheumatologists in Ontario, Canada. Arthritis Care Res. 2017, 69, 104–114. [Google Scholar] [CrossRef]
- Qian, J.; Ehrmann Feldman, D.; Bissonauth, A.; Ménard, H.A.; Panopalis, P.; Stein, M.; Lee, J.; Bernatsky, S. A retrospective review of rheumatology referral wait times within a health centre in Quebec, Canada. Rheumatol. Int. 2010, 30, 705–707. [Google Scholar] [CrossRef]
- Barber, C.E.H.; Thorne, J.C.; Ahluwalia, V.; Burt, J.; Lacaille, D.; Marshall, D.A.; Hazlewood, G.S.; Mosher, D.; Denning, L.; Szamko, I.; et al. Feasibility of measurement and adherence to system performance measures for rheumatoid arthritis in 5 models of care. J. Rheumatol. 2018, 45, 1501–1508. [Google Scholar] [CrossRef]
- Schmajuk, G.; Schneeweiss, S.; Katz, J.N.; Weinblatt, M.E.; Setoguchi, S.; Avorn, J.; Levin, R.; Solomon, D.H. Treatment of older adult patients diagnosed with rheumatoid arthritis: Improved but not optimal. Arthritis Rheum. 2007, 57, 928–934. [Google Scholar] [CrossRef] [PubMed]
- Kahn, K.L.; MacLean, C.H.; Liu, H.; Rubenstein, L.Z.; Wong, A.L.; Harker, J.O.; Chen, W.P.; Fitzpatrick, D.M.; Bulpitt, K.J.; Traina, S.B.; et al. Application of explicit process of care measurement to rheumatoid arthritis: Moving from evidence to practice. Arthritis Rheum. 2006, 55, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Kahn, K.L.; Maclean, C.H.; Wong, A.L.; Rubenstein, L.Z.; Liu, H.; Fitzpatrick, D.M.; Harker, J.O.; Chen, W.P.; Traina, S.B.; Mittman, B.S.; et al. Assessment of American College of Rheumatology quality criteria for rheumatoid arthritis in a pre-quality criteria patient cohort. Arthritis Rheum. 2007, 57, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Agnew-Blais, J.C.; Coblyn, J.S.; Katz, J.N.; Anderson, R.J.; Mehta, J.; Solomon, D.H. Measuring quality of care for rheumatic diseases using an electronic medical record. Ann. Rheum. Dis. 2009, 68, 680–684. [Google Scholar] [CrossRef] [PubMed]
- McGlynn, E.A.; Asch, S.M.; Adams, J.; Keesey, J.; Hicks, J.; DeCristofaro, A.; Kerr, E.A. The quality of health care delivered to adults in the United States. N. Engl. J. Med. 2003, 348, 2635–2645. [Google Scholar] [CrossRef]
- Ganz, D.A.; Chang, J.T.; Roth, C.P.; Guan, M.; Kamberg, C.J.; Niu, F.; Reuben, D.B.; Shekelle, P.G.; Wenger, N.S.; MacLean, C.H. Quality of osteoarthritis care for community-dwelling older adults. Arthritis Rheum. 2006, 55, 241–247. [Google Scholar] [CrossRef]
- Mikuls, T.R.; Farrar, J.T.; Bilker, W.B.; Fernandes, S.; Saag, K.G. Suboptimal physician adherence to quality indicators for the management of gout and asymptomatic hyperuricaemia: Results from the UK General Practice Research Database (GPRD). Rheumatology 2005, 44, 1038–1042. [Google Scholar] [CrossRef]
- Pradeep, J.; Watts, R.; Clunie, G. Audit on the uptake of influenza and pneumococcal vaccination in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2007, 66, 837–838. [Google Scholar] [CrossRef]
- Bridges, M.J.; Coady, D.; Kelly, C.A.; Hamilton, J.; Heycock, C. Factors influencing uptake of influenza vaccination in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2003, 62, 685. [Google Scholar] [CrossRef]
- Barnabe, C.; Chomistek, K.; Luca, N.; Hazlewood, G.; Barber, C.E.H.; Steiman, A.; Stringer, E. National priorities for high-quality rheumatology transition care for youth in Canada. J. Rheumatol. 2021, 48, 426–433. [Google Scholar] [CrossRef] [PubMed]
- McGlynn, E.A.; Asch, S.M. Developing a clinical performance measure. Am. J. Prev. Med. 1998, 14, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Saag, K.G.; Yazdany, J.; Alexander, C.; Caplan, L.; Coblyn, J.; Desai, S.P.; Harrington, T., Jr.; Liu, J.; McNiff, K.; Newman, E.; et al. Defining quality of care in rheumatology: The American College of Rheumatology white paper on quality measurement. Arthritis Care Res. 2011, 63, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Khanna, D.; Arnold, E.L.; Pencharz, J.N.; Grossman, J.M.; Traina, S.B.; Lal, A.; MacLean, C.H. Measuring process of arthritis care: The Arthritis Foundation’s quality indicator set for rheumatoid arthritis. Semin. Arthritis Rheum. 2006, 35, 211–237. [Google Scholar] [CrossRef]
- Yazdany, J.; Panopalis, P.; Gillis, J.Z.; Schmajuk, G.; MacLean, C.H.; Wofsy, D.; Yelin, E. A quality indicator set for systemic lupus erythematosus. Arthritis Rheum. 2009, 61, 370–377. [Google Scholar] [CrossRef]
- Khanna, D.; Kowal-Bielecka, O.; Khanna, P.P.; Lapinska, A.; Asch, S.M.; Wenger, N.; Brown, K.K.; Clements, P.J.; Getzug, T.; Mayes, M.D.; et al. Quality indicator set for systemic sclerosis. Clin. Exp. Rheumatol. 2011, 29, S33–S39. [Google Scholar]
- Kiltz, U.; Landewé, R.B.M.; van der Heijde, D.; Rudwaleit, M.; Weisman, M.H.; Akkoc, N.; Boonen, A.; Brandt, J.; Carron, P.; Dougados, M.; et al. Development of ASAS quality standards to improve the quality of health and care services for patients with axial spondyloarthritis. Ann. Rheum. Dis. 2020, 79, 193–201. [Google Scholar] [CrossRef]
- Helliwell, P.S.; Favier, G.; Gladman, D.D.; Soriano, E.R.; Kirkham, B.W.; Coates, L.C.; Puig, L.; Boehncke, W.H.; Thaçi, D. Best-practice indicators in psoriatic disease care. J. Rheumatol. Suppl. 2019, 95, 38–45. [Google Scholar] [CrossRef]
- Kavanaugh, A.; Ritchlin, C.; Boehncke, W.H. Quality indicators in psoriatic arthritis. Clin. Exp. Rheumatol. 2007, 25, 98–101. [Google Scholar]
- Mikuls, T.R.; MacLean, C.H.; Olivieri, J.; Patino, F.; Allison, J.J.; Farrar, J.T.; Bilker, W.B.; Saag, K.G. Quality of care indicators for gout management. Arthritis Rheum. 2004, 50, 937–943. [Google Scholar] [CrossRef]
- Grossman, J.M.; MacLean, C.H. Quality indicators for the management of osteoporosis in vulnerable elders. Ann. Intern. Med. 2001, 135, 722–730. [Google Scholar] [CrossRef] [PubMed]
- MacLean, C.H. Quality indicators for the management of osteoarthritis in vulnerable elders. Ann. Intern. Med. 2001, 135, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Yazdany, J.; Myslinski, R.; Miller, A.; Francisco, M.; Desai, S.; Schmajuk, G.; Lacaille, D.; Barber, C.E.; Orozco, C.; Bunyard, M.; et al. Methods for developing the american college of rheumatology’s electronic clinical quality measures. Arthritis. Care Res. 2016, 68, 1402–1409. [Google Scholar] [CrossRef] [PubMed]
- Yazdany, J.; Robbins, M.; Schmajuk, G.; Desai, S.; Lacaille, D.; Neogi, T.; Singh, J.A.; Genovese, M.; Myslinski, R.; Fisk, N.; et al. Development of the American College of Rheumatology’s Rheumatoid Arthritis Electronic Clinical Quality Measures. Arthritis Care Res. 2016, 68, 1579–1590. [Google Scholar] [CrossRef]
- FitzGerald, J.D.; Mikuls, T.R.; Neogi, T.; Singh, J.A.; Robbins, M.; Khanna, P.P.; Turner, A.S.; Myslinski, R.; Suter, L.G. Development of the American College of Rheumatology Electronic Clinical Quality Measures for Gout. Arthritis Care Res. 2018, 70, 659–671. [Google Scholar] [CrossRef]
- Tonner, C.; Schmajuk, G.; Yazdany, J. A new era of quality measurement in rheumatology: Electronic clinical quality measures and national registries. Curr. Opin. Rheumatol. 2017, 29, 131–137. [Google Scholar] [CrossRef]
- Liu, L.H.; Choden, S.; Yazdany, J. Quality improvement initiatives in rheumatology: An integrative review of the last 5 years. Curr. Opin. Rheumatol. 2019, 31, 98–108. [Google Scholar] [CrossRef]
- Domsic, R.T. Scleroderma: The role of serum autoantibodies in defining specific clinical phenotypes and organ system involvement. Curr. Opin. Rheumatol. 2014, 26, 646–652. [Google Scholar] [CrossRef]
- Johnson, S.R.; Hawker, G.A.; Davis, A.M. The health assessment questionnaire disability index and scleroderma health assessment questionnaire in scleroderma trials: An evaluation of their measurement properties. Arthritis Rheum. 2005, 53, 256–262. [Google Scholar] [CrossRef]
- Hoffmann-Vold, A.M.; Distler, O.; Murray, B.; Kowal-Bielecka, O.; Khanna, D.; Allanore, Y. Setting the international standard for longitudinal follow-up of patients with systemic sclerosis: A Delphi-based expert consensus on core clinical features. RMD Open 2019, 5, e000826. [Google Scholar] [CrossRef]
- Spierings, J.; van den Ende, C.H.M.; Schriemer, R.M.; Bernelot Moens, H.J.; van der Bijl, E.A.; Bonte-Mineur, F.; de Buck, M.P.D.; de Kanter, M.A.E.; Knaapen-Hans, H.K.A.; van Laar, J.M.; et al. How do patients with systemic sclerosis experience currently provided healthcare and how should we measure its quality? Rheumatology 2020, 59, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef]
- Johnson, S.R.; Fransen, J.; Khanna, D.; Baron, M.; van den Hoogen, F.; Medsger, T.A., Jr.; Peschken, C.A.; Carreira, P.E.; Riemekasten, G.; Tyndall, A.; et al. Validation of potential classification criteria for systemic sclerosis. Arthritis Care Res. 2012, 64, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, A.; Tunnicliffe, D.J.; Thakkar, V.; Singh-Grewal, D.; O’Neil, S.; Craig, J.C.; Tong, A. Patients’ perspectives and experiences living with systemic sclerosis: Systematic review and thematic synthesis of qualitative studies. J. Rheumatol. 2016, in press. [Google Scholar] [CrossRef]
- Guzman, J.; Gomez-Ramirez, O.; Jurencak, R.; Shiff, N.J.; Berard, R.A.; Duffy, C.M.; Oen, K.; Petty, R.E.; Benseler, S.M.; Brant, R.; et al. What matters most for patients, parents, and clinicians in the course of juvenile idiopathic arthritis? A qualitative study. J. Rheumatol. 2014, 41, 2260–2269. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.R.; Mccarthy, M.A.; Ang, J.T.; Granton, J.T. Developing a pulmonary hypertension health passport to improve care: A qualitative study. Can. J. Respir. Crit. Care Sleep Med. 2022, 6, 193–198. [Google Scholar] [CrossRef]
- Van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American college of rheumatology/European league against rheumatism collaborative initiative. Ann. Rheum. Dis. 2013, 72, 1747–1755. [Google Scholar] [CrossRef]
- Kowal-Bielecka, O.; Fransen, J.; Avouac, J.; Becker, M.; Kulak, A.; Allanore, Y.; Distler, O.; Clements, P.; Cutolo, M.; Czirjak, L.; et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Ann. Rheum. Dis. 2017, 76, 1327–1339. [Google Scholar] [CrossRef]
- Hinchcliff, M.E.; Beaumont, J.L.; Carns, M.A.; Podlusky, S.; Thavarajah, K.; Varga, J.; Cella, D.; Chang, R.W. Longitudinal evaluation of PROMIS-29 and FACIT-dyspnea short forms in systemic sclerosis. J. Rheumatol. 2015, 42, 64–72. [Google Scholar] [CrossRef]
- Kwakkenbos, L.; Thombs, B.D.; Khanna, D.; Carrier, M.E.; Baron, M.; Furst, D.E.; Gottesman, K.; van den Hoogen, F.; Malcarne, V.L.; Mayes, M.D.; et al. Performance of the patient-reported outcomes measurement information system-29 in scleroderma: A scleroderma patient-centered intervention network Cohort Study. Rheumatology 2017, 56, 1302–1311. [Google Scholar] [CrossRef]
- Becker, M.O.; Dobrota, R.; Garaiman, A.; Debelak, R.; Fligelstone, K.; Tyrrell Kennedy, A.; Roennow, A.; Allanore, Y.; Carreira, P.E.; Czirják, L.; et al. Development and validation of a patient-reported outcome measure for systemic sclerosis: The EULAR Systemic Sclerosis Impact of Disease (ScleroID) questionnaire. Ann. Rheum. Dis. 2022, 81, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Institute for Health Care Improvement. How to Improve. Available online: https://www.ihi.org/resources/Pages/HowtoImprove/default.aspx (accessed on 6 December 2022).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).