Abstract
Ampullary neoplastic lesions (ANLs) represent a rare cancer, accounting for about 0.6–0.8% of all gastrointestinal malignancies, and about 6–17% of periampullary tumors. They can be sporadic or occur in the setting of a hereditary predisposition syndrome, mainly familial adenomatous polyposis (FAP). Usually, noninvasive ANLs are asymptomatic and detected accidentally during esophagogastroduodenoscopy (EGD). When symptomatic, ANLs can manifest differently with jaundice, pain, pancreatitis, cholangitis, and melaena. Endoscopy with a side-viewing duodenoscopy, endoscopic ultrasound (EUS), and magnetic resonance cholangiopancreatography (MRCP) play a crucial role in the ANL evaluation, providing an accurate assessment of the size, location, and characteristics of the lesions, including the staging of the depth of tumor invasion into the surrounding tissues and the involvement of local lymph nodes. Endoscopic papillectomy (EP) has been recognized as an effective treatment for ANLs in selected patients, providing an alternative to traditional surgical methods. Originally, EP was recommended for benign lesions and patients unfit for surgery. However, advancements in endoscopic techniques have broadened its indications to comprise early ampullary carcinoma, giant laterally spreading lesions, and ANLs with intraductal extension. In this paper, we review the existing evidence on endoscopic diagnosis and treatment of ampullary neoplastic lesions.
1. Introduction
Ampullary neoplastic lesions (ANLs) represent a rare cancer, accounting for about 0.6–0.8% of all gastrointestinal malignancies, and about 6–17% of periampullary tumors (arising from the ampulla of Vater, the distal common bile duct, the second portion of the duodenum, and the head of the pancreas) [1,2,3].
Although the overall incidence of ANLs in western countries is less than 1 case per 100,000 per year according to data from international registries, their incidence has risen during the last decades, probably due to the growing use of esophagogastroduodenoscopy (EGD) for diagnosis of other upper-GI disorders and for the screening of high-risk patients with familial adenomatous polyposis (FAP) [4,5].
ANLs are often sporadic and arise from intestinal-type mucosa, involving the major papilla, and following an adenoma-to-carcinoma sequence with a potential transformation into adenocarcinoma [6]. However, ANLs can originate from different tissues, expressing in a different way compared to the better-known intestinal type of lesions, including the pancreaticobiliary type (from pancreatic duct-type ampullary mucosa), the mixed type (glandular and squamous cell tissue), the mucinous type (colloid), the signet-ring cell carcinomas, the neuroendocrine type, and the undifferentiated type [7]. Historically, intestinal-type ANLs have been associated with a more benign clinical course compared to pancreaticobiliary-type malignancies [8,9]; nevertheless, recent studies have not confirmed this suggestion, finding no prognostic differences between the two groups [10,11].
Hereditary ANLs appear in younger age groups than sporadic ones; among hereditary syndromes that increase ANL predisposition, including the neurofibromatosis type I and the Muir–Torre syndrome, the familial adenomatous polyposis (FAP) is associated with a 120-fold increased relative risk to have an ampullary tumor compared to the general population [12].
2. Diagnosis
2.1. Clinical Assessment
Usually, noninvasive ANLs are asymptomatic and detected accidentally during EGD performed for another indication. When symptomatic, ANLs can manifest differently with jaundice, pain, diarrhea, pancreatitis, cholangitis, steatorrhea, and melaena, making the differential diagnosis with choledocholithiasis, extrahepatic cholangiocarcinoma, and pancreatic adenocarcinoma [13,14,15].
2.2. Endoscopy
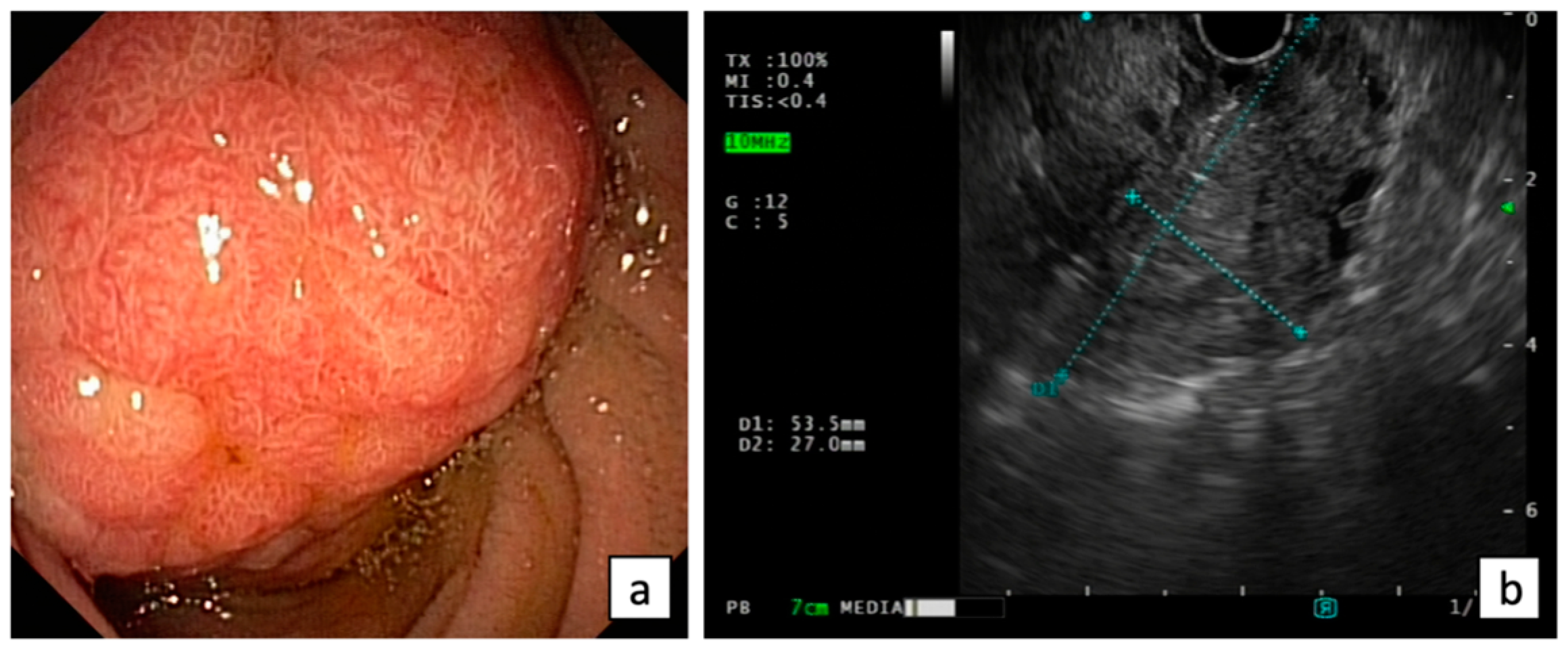
Endoscopic evaluation of ANLs may be challenging using a forward-viewing endoscope. The European Society of Gastrointestinal Endoscopy (ESGE) considers the visualization of the papilla as a research priority for a complete high-quality endoscopy [16]. Thus, cap-assisted upper endoscopy should be indicated when the major papilla is not seen by a gastroscope, but a side-viewing duodenoscopy is recommended for the optimal visualization of the papilla and the assessment of the feasibility of endoscopic resection in presence of ANLs [17] (Figure 1).
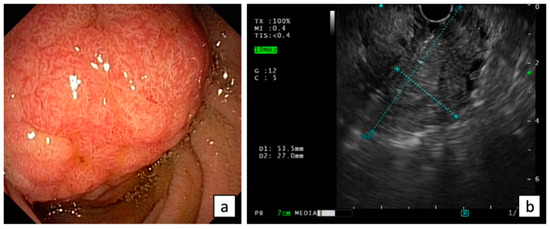
Figure 1.
Endoscopic (a) and EUS (b) evaluation of ANLs.
Currently, an endoscopic classification of ANLs is still lacking. They can present as isolated lesions of the papilla, have an extra-papillary component (7–44%), and in some cases an intra-ductal component [18,19,20,21,22,23]. Benign small ANLs can be indistinguishable from normal papilla, while ANLs with laterally spreading growth could have an extra-papillary component showing similar characteristics to non-ampullary duodenal adenomas [22]. Benign features include regularity of surface and margins, soft consistency, and mobility, while superficial erosions, ulcers, friability, hard consistency, firmness, and spontaneous bleeding are usually associated with malignancy [23,24]. Furthermore, large lesions (>20 mm) have been associated with an increased risk of deep invasion at histology and local recurrence after resection in several studies [25,26,27].
2.3. Chromoendoscopy
Chromoendoscopy is a valuable tool in the diagnosis ANL, enhancing the visualization of mucosal details and facilitating the differentiation between benign and neoplastic lesions. By evaluating the microsurface and microvessel patterns of lesions, chromoendoscopy can provide insights into the histology and grade of dysplasia, guiding endoscopic diagnosis and management. Indeed, irregular villous arrangement and abnormal microvasculature are evaluated with virtual chromoendoscopy, such as narrow band imaging (NBI), and it diagnoses adenocarcinoma with sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of 69%, 100%, 100%, 85%, and 89%, respectively [28]. Furthermore, dye-based chromoendoscopy with indigo carmine appeared particularly useful in delineating the margins of the lesion prior to endoscopic papillectomy, ensuring complete resection, and reducing the risk of local recurrence [29].
2.4. Histology
Endoscopic biopsies and hematoxylin and eosin-stained histopathology are mandatory for the diagnosis of ANLs, although their diagnostic accuracy has been reported to range widely from 38% to 85% [30,31,32,33,34,35]. The histological underestimation rate can reach up to 30% [36,37]. Prospectively evaluated, the overall rate of diagnostic overestimation, which can result in potentially inadequate and risky treatment, stands at 15%, with a specific rate of 21% for initial low-grade dysplasia diagnosis [18]. Furthermore, in two extensive retrospective series, post-papillectomy histological analysis revealed that normal intestinal mucosa or inflammation alone were found in 8% and 13.8%, respectively [35,38].
ESGE recommends obtaining histological confirmation through repeat endoscopic biopsies before initiating any treatment in the presence of low-grade dysplasia [19]. Conversely, if the presence of adenoma has not been established, ESGE does not recommend diagnostic or therapeutic papillectomy [19].
Several reports have suggested that in cases of a bulging papilla without features of abnormality, endoscopic biopsies should be performed subsequent to an endoscopic sphincterotomy. Nevertheless, conflicting findings have been documented, revealing low sensitivities ranging from 21% to 37% due to the potential occurrence of cytoarchitectural atypia resulting from post-sphincterotomy changes [39,40]. In this context, performing additional samplings, preferably at least 10 days after sphincterotomy, can prove beneficial in order to prevent initial false-negative results [41].
2.5. Immunohistochemistry, Polymerase Chain Reaction, and Flow Cytometry
Presently, it is not recommended to routinely employ immunohistochemical staining for the p53 tumor suppressor gene, polymerase chain reaction analysis of tumor DNA for K-ras gene mutations, and the addition of flow cytometry to assess aneuploidy for prognosis determination and/or prediction of treatment response. However, the subclassification of ANLs into intestinal or pancreaticobiliary phenotypes holds considerable prognostic significance. In resected specimens, immunohistochemistry (IHC) panels comprising MUC1, MUC2, CDX2, CK20, and MUC5AC can assist in subtyping into intestinal or pancreaticobiliary phenotypes [42,43]. However, for endoscopic biopsies, the morphological and IHC classifications into intestinal or pancreaticobiliary phenotypes lack consistency due to factors such as tissue heterogeneity, antigenicity, interpretation of staining patterns, and inter/intraobserver variability. The presence of K-ras and p53 mutations has been identified in various histological subtypes of ANLs. However, these mutations do not provide a definitive histological subtyping of intestinal and pancreaticobiliary phenotypes, highlighting the frequent occurrence of hybrid phenotypes [44].
2.6. EUS, MRCP, and IDUS
Endoscopic ultrasound (EUS) plays a crucial role in the ANL evaluation, providing an accurate assessment of the size, location, and characteristics of the lesions, including the staging of the depth of tumor invasion into the surrounding tissues such as duodenal wall, biliary duct, pancreatic duct, and pancreatic parenchyma, and the involvement of local lymph nodes, according to the latest TNM classification (Figure 1).
The diagnostic accuracy of endoscopic ultrasound EUS for detecting tumor depth (T-staging) and regional lymph node status (N-staging) was evaluated in a recent meta-analysis that included 21 studies [45]. The pooled sensitivity and specificity of EUS were 0.89 and 0.87 for T1, 0.76 and 0.91 for T2, 0.81 and 0.94 for T3, and 0.72 and 0.98 for T4, respectively. For N-staging, 16 studies using EUS were included with sensitivity and specificity of 0.61 and 0.77, respectively [45]. When compared with magnetic resonance cholangiopancreatography (MRCP), EUS demonstrates comparable or slightly higher accuracy for T staging, while for N staging, MRCP had the best performance [46,47,48,49,50].
Among intraductal biliopancreatic imaging techniques, intraductal ultrasonography (IDUS) offers real-time, cross-sectional imaging of the pancreatobiliary ducts and nearby structures while performing ERCP using a high-frequency ultrasound transducer. Consequently, IDUS is highly regarded as a sensitive and valuable tool for evaluating ANLs. According to Ye et al. The pooled sensitivity and specificity of IDUS were 0.90 and 0.88 for T1, 0.73 and 0.91 for T2, and 0.79 and 0.97 for T3, respectively. Considering N-staging, the pooled sensitivity and specificity of IDUS were 0.61 and 0.92, respectively [45]. However, IDUS is now regarded as an outdated technique that is no longer used mainly due to its high costs, the fragility of the devices, and the complexity of the training required to learn it.
3. Treatment
3.1. Endoscopic Treatment
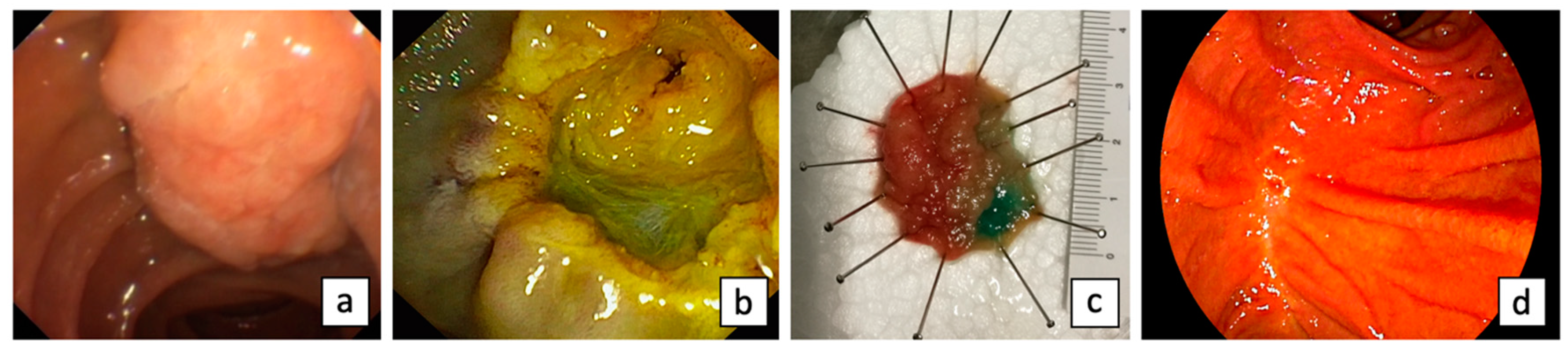
Endoscopic papillectomy (EP) refers to the endoscopic resection of the mucosa and submucosa of the duodenal wall, including the region where the ampulla of Vater is anatomically attached, including the excision of the surrounding tissue around the orifices of the bile duct and pancreatic duct [51] (Figure 2). First described in 1983 by Suzuki et al. [52], endoscopic papillectomy (EP) has been recognized as an effective treatment for ANLs in selected patients, providing an alternative to traditional surgical methods [53]. Originally, EP was recommended for benign lesions and patients unfit for surgery [53]. However, advancements in endoscopic techniques have broadened its indications to comprise early ampullary carcinoma, giant laterally spreading lesions, and ANLs with intraductal extension [53].
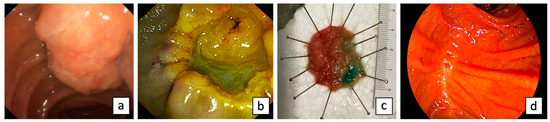
Figure 2.
Endoscopic papillectomy: ANL evaluated by side-viewing duodenoscopy (a); post-EP inspection (b); specimen (c); and scar at 1-year follow-up (d).
The primary purpose of submucosal injection for ANLs before EP is to assist in diagnosing the lateral extent of the lesion. Additionally, a no lifting sign may indicate the presence of deep submucosal invasion that cannot be effectively treated through a conventional endoscopic resection. Submucosal injection is also advocated to prevent bleeding and reduce the risk of causing deep thermal damage to the ducts and muscularis propria during the procedure. Nevertheless, according to a survey conducted with 46 expert biliary endoscopists in the USA and Canada, the use of submucosal injection in combination with EP does not appear to offer any significant advantage [54]. Currently, there is only one randomized controlled trial that has compared EP with or without submucosal injection [55]. The complete resection rate was significantly higher in the no-injection group compared to the injection group (80.8% vs. 50.0%, respectively; p = 0.02). However, there were no notable differences in terms of AEs, residual tumor at 1 month, and local recurrence at 12 months [55].
Although there is a lack of clear evidence from comparative trials, many authors recommend performing a cholangiogram and pancreatogram prior to EP to assess for deep intraductal extension exceeding 10 mm. The routine use of bi-ductal sphincterotomy before resection granted comparable technical and clinical success to the standard technique with a low adverse event (AE) rate of 8% [56]. However, it is worth noting that the number of en bloc and single-session resections appears to be lower, especially when sphincterotomy is combined with pancreatic stent placement before resection. Furthermore, it has been shown that altered papilla morphology is associated with a higher risk of biliary cannulation failure and AEs [57]. Additionally, some authors have reported challenges in obtaining a complete histopathological evaluation of the resected specimen due to thermal injury following sphincterotomy [58,59].
There is currently no consensus regarding the optimal current and power output for performing endoscopic papillectomy. In an RCT conducted by Iwasaki et al. [60], it was demonstrated that both autocut and endocut mode exhibit similar efficacy and safety for EP. However, the endocut mode may offer an advantage by potentially preventing immediate bleeding in cases involving large tumor sizes (88% vs. 46%, p = 0.04), although the rate of crush artifacts was higher in the endocut group compared to the autocut group (27% vs. 3.3%, p = 0.03).
According to a recent systematic review with pooled analysis, that included 29 studies reporting the results of EP in a total of 1751 patients with ANLs, complete endoscopic resection was achieved in 94.2% patients (95 %CI 90.5–96.5; I2 = 73%), and curative endoscopic resection in 87.1% patients (95 %CI 83.0–90.3; I2 = 70%) [25]. En bloc resection was achieved in 82.4 % (95 %CI 74.7–88.1; I2 = 84%), and this was the only factor affecting curative resection (odds ratio [OR] = 3.55, 95 %CI = 1.11–5.99, p = 0.004) [25]. The overall rate of AEs following EP was 24.9% (95% CI = 21.2%–29.0%; I2 = 66%) [25]. The most frequently reported AEs were post-procedural pancreatitis, occurring in 11.9% of cases (95% CI 10.4–13.6; I2 = 41%), followed by bleeding in 10.6% cases (95% CI = 5.2–13.6; I2 = 61%) [25]. Perforations and cholangitis were less common, reported in 3.1% (95% CI = 2.2–4.2; I2 = 17%) and 2.7% (95% CI = 1.9–4.0; I2 = 32%) of cases, respectively [25]. The occurrence of long-term AEs such as papillary stenosis was recorded in 2.4% of cases (95% CI = 1.6–3.4; I2 = 0). The mortality rate associated with the procedure was 0.3% [25].
Binda et al. [61] provided data on the effectiveness and safety of EP in a multicenter, retrospective, nationwide study, including a total of 225 ANL patients. En bloc resection was possible in 72.5% of cases, with an overall R0 resection rate of 50.7% [61]. During a mean follow-up period of 23.2 months, recurrences were diagnosed in 17.2% of patients, 61.3% of which were successfully treated with an additional endoscopic treatment with a clinical success achieved in 76.7% of the cases [61]. In multivariate analysis, R1 resection, lesion size, and histological diagnosis were predictors for recurrence. Intra-procedural bleeding occurred during 12.4% of EP [61]. Post-EP AEs occurred in 39.5% of patients, including delayed bleeding (20.9%), pancreatitis (13.3%), and perforation (2.2%) [61].
Among novel resection techniques of ANL, Takahara et al. [62] evaluated a modified EP with hybrid endoscopic submucosal dissection (hybrid ESD-EP), consisting of a (sub)circumferential incision with partial submucosal dissection, and subsequent snare resection, in order to attain a higher en bloc resection rate with curative safe margin compared to the standard technique. En bloc resection was achieved with hybrid ESD-EP in all eight cases (100%), with all lateral margins clear (100%), whereas vertical margin was uncertain in three (38%), resulting in the complete resection rate of 63% [62]. Post-operative bleeding and pancreatitis developed in 13% of cases [62]. After a median follow-up of 9 months, no tumor recurrence was observed even in those cases with uncertain vertical margin [62]. A summary of the more recent results described in the literature is provided in Table 1.
EP has proven to be a valuable treatment option also for FAP-related ANLs. Despite the effectiveness and safety of EP in treating FAP-related ANLs, it is important to note that FAP patients have a lifetime risk of relapse even after achieving complete resection. Consequently, long-term surveillance is necessary to closely monitor these patients. Recently, in a retrospective multicenter study involving 1422 endoscopic papillectomy procedures, a propensity score matching approach was employed [63]. The matching process considered factors such as age, sex, comorbidity, histologic subtype, and size [63]. The purpose was to analyze main outcomes, including complete resection (R0), technical success, complications, and recurrence, within matched cohorts of FAP-related and sporadic ANLs [63]. Among the FAP patients, the majority (79.2%; 95% CI = 71.2–87.3) were asymptomatic, which was significantly higher compared to the sporadic group (46.5%; 95% CI = 36.6–56.4; p < 0.001) [63]. The initial rate of complete resection (R0) was significantly lower in FAP patients (63.4%; 95% CI = 53.8–72.9) compared to controls (83.2%; 95% CI = 75.8–90.6; p = 0.001) [63]. However, after subsequent interventions (mean of 1.30 interventions per patient), the R0 rates became comparable between the two groups (FAP: 93.1%; 95% CI = 88.0–98.1 vs. sporadic: 97.0%; 95% CI = 93.7–100; p = 0.19) [63]. Adverse events were observed in 28.7% of cases, with pancreatitis and bleeding being the most common in both FAP and sporadic groups [63]. Severe AEs were rare, occurring in only 3.5% of cases [63]. Recurrence was observed in 21 FAP patients (20.8%; 95% CI = 12.7–28.8) and 16 sporadic patients (15.8%; 95% CI = 8.6–23.1; p = 0.36) [63]. However, recurrences were noted to occur later in FAP patients, with a median time of 25 months (95% CI = 18.3–31.7), compared to 2 months (95% CI = 0.06–3.9) in the control group [63].
Regarding laterally spreading tumors involving the papilla of Vater (LST-p), characterized as an ampullary tumor that extends laterally beyond the ampullary mound by ≥10 mm [22], or has an extra-papillary component on the duodenal wall larger than the size of the ANL [64], in several retrospective cohorts, it was shown that the endoscopic treatment has comparable outcomes in terms of endoscopic curative resection and recurrence rates, when compared to ANLs [19,22,64,65]. However, Klein et al. [22] have reported a higher risk of intraprocedural bleeding (50% vs. 24.7%, p = 0.003), as well as delayed bleeding (25% vs. 12.3%, p = 0.08) with LST-p. Similar findings were observed by Sahar et al. [64] in terms of delayed bleeding (14% vs. 4%, p = 0.02). However, cold snaring can lead to significant safety over hot snare-based techniques for treatment of the duodenal extra-papillary component such as for superficial non-ampullary duodenal epithelial tumors, without an impairment in terms of curability [66]. Indeed, as reported by Repici et al. in a retrospective multicenter study comparing 33 large duodenal adenomas treated with cold-snaring to 101 patients who had hot EMR, no serious AEs occurred in the cold group, while 17 intraprocedural serious AEs (16.8%) and 26 postprocedural serious AEs (25.7%) in the hot EMR group occurred with a local recurrence at first follow-up endoscopy comparable in both groups (cold EMR: 4/33; 12.1% versus hot EMR: 21/101; 20.8%) [67].
In cases of intraductal growth, Bohnacker et al. [68] have reported a lower rate of endoscopic curative resection (46% vs. 83%, p < 0.001) and a higher rate of rescue surgery (37% vs. 12%) compared with ANLs without intraductal extension. Nevertheless, ESGE suggests the use, in tertiary centers, of complementary techniques, including thermal ablation with cystotome, or radio-frequency ablation (RFA) with temporary biliary stenting, for ANLs with ≤20 mm intraductal extension [19]. In a retrospective observational study, Pérez-Cuadrado-Robles et al. [23] proposed the use of endoscopic thermal ablation performed with a wire-guided cystotome and soft/forced coagulation, obtaining an intraductal ablation in 100% of cases with a 20-month median follow-up. Furthermore, in a recent randomized controlled trial, involving 20 patients who had undergone endoscopic papillectomy for ampullary adenoma and were found to have histologically proven endobiliary adenoma remnants (with a ductal extent <20 mm), it was found that intraductal RFA achieved a 70% eradication of dysplasia at 12 months following a single session [69]. Endoscopic ID-RFA showed good long-term outcomes in treating residual or relapsed ANLs with intraductal extension, and repeated ID-RFA may be considered as an option for managing recurrence [70].
3.2. Management of Adverse Events
According to the literature, EP shows a lower overall adverse events (AEs) rate compared to surgical treatment. However, it is essential to note that even after EP, a significant AEs rate persists. An overall AEs rate of 24.9% (95% CI, 21.2% to 29%) was reported, but many complications are typically mild to moderate and can be managed conservatively [25]. AEs can be classified into two categories: early AEs, including pancreatitis, bleeding, and perforation, and delayed AEs, such as papillary and biliary stenosis or duodenal luminal stenosis.
Postprocedural pancreatitis, caused by the obstruction of the pancreatic orifice because of the transient edema from the electrocautery, has been reported to be the most common adverse event occurring in 11.9% of cases (95% CI, 10.5% to 13.6%) [25]. Prophylactic pancreatic duct stenting is recommended as an effective technique for prevention of pancreatitis after EP [17]. Indeed, a single RCT revealed a significantly lower incidence of pancreatitis (33%) in the stented group compared to the unstented group (p = 0.02) [71], while the only factor leading to acute pancreatitis as an outcome was the placement of a prophylactic pancreatic stent during the same session (OR −1.72, 95% CI −2.95 to −0.50; p = 0.006), as described in a systematic review with pooled analysis [25].
In this context, biodegradable pancreatic stents offer the promise of eliminating the need for repetitive endoscopies to remove stents, diminishing potential patient risks, and cutting down on healthcare expenses [72]. Furthermore, to prevent complications, it is recommended to administer 100 mg of rectal indomethacin or diclofenac immediately before EP in all patients without any contraindications [17]. The confirmation of a pancreas divisum, documented during the preoperative EUS or MRCP, avoids the need for pancreatic stent placement [17].
Bleeding is the second most frequent complication (10.6%; 95% CI, 5.2% to 13.6%) [25]. Bleeding can be distinguished in intraprocedural or delayed, usually in the first 12 h after resection [73]. In the more recent and largest retrospective studies, bleeding management was performed endoscopically in 69.1% of cases (n = 56/81) and mostly successfully [19,36,38,64,74]. If bleeding occurs, there are several approaches to manage it. One option is to attempt epinephrine injection, but also soft coagulation using the tip of the snare or coagulation forceps; alternatively, the use of APC (Argon Plasma Coagulation) or the application of clips can be considered [73]. In cases of endoscopic failure, an angiographic evaluation and embolization could be considered [19,36,38,65,74].

Table 1.
Main outcomes of endoscopic papillectomy.
Table 1.
Main outcomes of endoscopic papillectomy.
| First Author, Year | Subjects, n, Study Design | Outcomes, n, n (%) | |||
|---|---|---|---|---|---|
| En Bloc | Clinical Success | Overall AEs | Local Recurrence | ||
| Binda, 2023 [61] | 225, Retrospective Study | 163/225 (72.5%) | 173/225 (76.7%) | 89/225 (39.5%) | 39/225 (17.2%) |
| Takahara, 2020 [62] | 8, Retrospective Study | 8/8 (100%) | 8/8 (100%) | 6/8 (75%) | 0/8 (0%) |
| Sahar, 2020 [64] | 161, Retrospective Study | 115/161 (72%) | 106/128 (83%) | 24/161 (14.9%) | 12/161 (7%) |
| Tringali, 2020 [74] | 135, Retrospective Study | 112/135 (83%) | 96/103 (93%) | 29/135 (21.5%) | 24/103 (23%) |
| Li, 2019 [36] | 110, Retrospective Study | 83/110 (75.5%) | 86/110 (78.2%) | 39/110 (35%) | 13/110 (11.8%) |
| van der Wiel, 2019 [19] | 87, Retrospective Study | 41/87 (47.1%) | 67/87 (77%) | 23/87 (26.4%) | 10/87 (11.5%) |
Perforation related to electrocautery is reported in 3.1% of cases (95% CI, 2.2% to 4.2%) [25]. It is crucial to carefully inspect the defect both endoscopically and fluoroscopically to detect any deep tissue injury. Fortunately, due to its retroperitoneal location, perforation can typically be managed conservatively. In cases where perforation is diagnosed during the procedure, intravenous antibiotics should be administered, and an attempt to close the perforation using endoclips, along with biliary stenting using a fully covered self-expandable metallic stent, is recommended [73].
3.3. Surgical Treatment
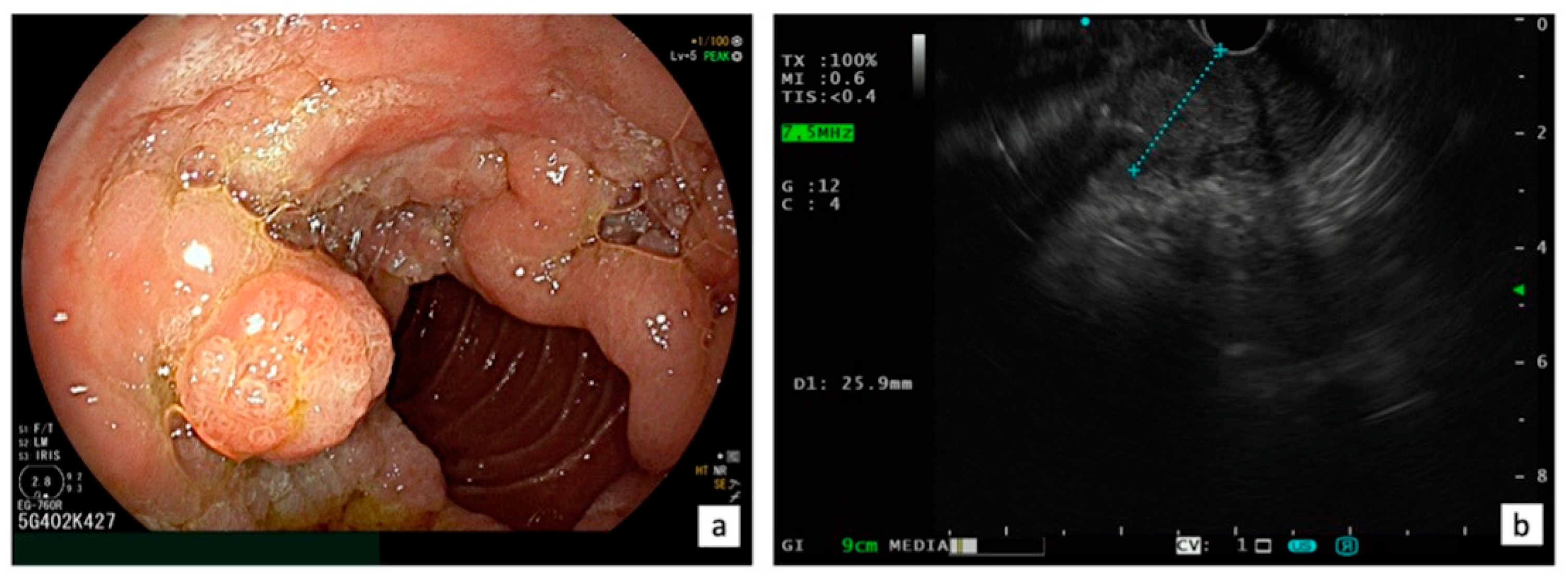
Presently, there is a lack of RCTs that compare EP and surgical treatments, such as transduodenal ampullectomy or pancreaticoduodenectomy, for ANLs. In a recent systematic review and meta-analysis, including a total of 39 studies with 1753 patients (1468 EP and 285 transduodenal ampullectomy), Garg et al. [75] aimed to compare long-term recurrence of benign sporadic ANLs after EP and transduodenal ampullectomy, showing that endoscopic and surgical ampullectomy have similar recurrence rates at 1, 2, 3, and 5 years of follow-up. Thus, when feasible, EP is considered the first choice for ANL. However, there are still situations where surgery remains a viable option for ANL, including the following: (1) intraductal involvement (>20 mm); (2) technical limitations (the presence of a diverticulum or the tumor size exceeding 4 cm); (3) incomplete resection after EP (positive margins); and (4) local recurrence not endoscopically treatable [76] (Figure 3). A systematic review, which included five retrospective cohort studies with 466 patients, revealed that surgical resection (transduodenal ampullectomy or pancreaticoduodenectomy) had better outcomes in achieving complete resection of ANLs compared to EP (risk difference [RD] −0.37, 95% CI −0.50 to −0.24, p < 0.001, I 2 = 71%) without any difference in complications [77]. However, when utilizing a fixed effects model, EP exhibited a lower rate of adverse events (RD −0.28, 95% CI −0.39 to −0.18, p < 0.001; I 2 = 95%) [77].
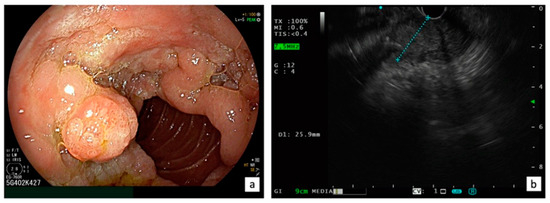
Figure 3.
Indication for surgical treatment: LST-p characterized with a circumferential extra-papillary component on the duodenal wall with a tumor size exceeding 4 cm (a) and an intraductal involvement >20 mm confirmed using EUS (b).
The treatment approach for ampullary cancer is pancreaticoduodenectomy, which is characterized by post-operative morbidity ranging from 34% to 59% and a mortality rate of 1% to 2%. After surgery, the 5-year survival rates for ampullary cancer range between 40% and 60% and the main prognostic factors that significantly impact survival are the T and N status of the tumor [26,78,79].
In case of Tis ampullary lesions, transduodenal ampullectomy has shown lower morbidity rates compared to pancreaticoduodenectomy, with no risk of recurrence [80,81,82]. The 5-year survival rate of patients with early ampullary cancer was 77.3% in transduodenal ampullectomy group and 75.9% in pancreaticoduodenectomy group (p = 0.927) [82].
Nevertheless, due to a significant percentage of T1 ampullary carcinomas showing lymph node metastasis, with rates ranging from 9% to 45% [26,78,80,83], pancreaticoduodenectomy with lymphadenectomy remains the procedure of choice for T1 adenocarcinoma.
4. Conclusions
ANLs represent a rare cancer that can be sporadic or occur in the setting of a hereditary predisposition syndrome. The management of ANLs is hampered by the paucity of data available in the literature, mainly represented by retrospective studies. Endoscopy, EUS, and MRCP play a crucial role in the evaluation and the staging of ANLs, providing an accurate assessment of the size, location, and characteristics of the lesions, and the depth of tumor invasion into the surrounding tissues and the involvement of local lymph nodes. EP has been recognized as an effective treatment for ANLs in selected patients, providing an alternative to traditional surgical methods. Advancements in endoscopic techniques have broadened its indications to comprise early ampullary carcinoma, giant laterally spreading lesions, and ANLs with intraductal extension. Nevertheless, EP remains a complex procedure with an increased risk of AEs. Thus, it is strongly recommended that this procedure be exclusively carried out within proficient medical centers, led by operators skilled in endoscopic resection methods able to effectively manage any associated AEs, ensuring good outcomes and low morbidity rates.
Author Contributions
Conceptualization, R.M., T.B. and A.R.; writing—original draft preparation, R.M., R.d.S. and A.F.; writing—review and editing, R.M., R.d.S. and A.F.; visualization, M.S., M.C. and A.C.; supervision, T.B. and A.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Westgaard, A.; Pomianowska, E.; Clausen, O.P.; Gladhaug, I.P. Intestinal-type and pancreatobiliary-type adenocarcinomas: How does ampullary carcinoma differ from other periampullary malignancies? Ann. Surg. Oncol. 2013, 20, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Perysinakis, I.; Margaris, I.; Kouraklis, G. Ampullary cancer-a separate clinical entity? Histopathology 2014, 64, 759–768. [Google Scholar] [CrossRef]
- Ramai, D.; Ofosu, A.; Singh, J.; John, F.; Reddy, M.; Adler, D.G. Demographics, tumor characteristics, treatment, and clinical outcomes of patients with ampullary cancer: A Surveillance, Epidemiology, and End Results (SEER) cohort study. Minerva Gastroenterol. Dietol. 2019, 65, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Rostain, F.; Hamza, S.; Drouillard, A.; Faivre, J.; Bouvier, A.M.; Lepage, C. Trends in incidence and management of cancer of the ampulla of Vater. World J. Gastroenterol. 2014, 20, 10144–10150. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, A.L.; Shiels, M.S.; Jones, G.S.; Pfeiffer, R.M.; Petrick, J.L.; Beebe-Dimmer, J.L.; Koshiol, J. Biliary tract cancer incidence and trends in the United States by demographic group, 1999–2013. Cancer 2019, 125, 1489–1498. [Google Scholar] [CrossRef]
- Kaiser, A.; Jurowich, C.; Schönekäs, H.; Gebhardt, C.; Wünsch, P.H. The adenoma-carcinoma sequence applies to epithelial tumours of the papilla of Vater. Z. Gastroenterol. 2002, 40, 913–920. [Google Scholar] [CrossRef]
- Fischer, H.; Zhou, H. Pathogenesis of carcinoma of the papilla of Vater. J. Hepatobiliary Pancreat. Surg. 2004, 11, 301–309. [Google Scholar] [CrossRef]
- Pea, A.; Riva, G.; Bernasconi, R.; Sereni, E.; Lawlor, R.T.; Scarpa, A.; Luchini, C. Ampulla of Vater carcinoma: Molecular landscape and clinical implications. World J. Gastrointest. Oncol. 2018, 10, 370–380. [Google Scholar] [CrossRef]
- Talamini, M.A.; Moesinger, R.C.; Pitt, H.A.; Sohn, T.A.; Hruban, R.H.; Lillemoe, K.D.; Yeo, C.J.; Cameron, J.L. Adenocarcinoma of the ampulla of Vater. A 28-year experience. Ann. Surg. 1997, 225, 590–600. [Google Scholar] [CrossRef]
- Beghelli, S.; Orlandini, S.; Moore, P.S.; Talamini, G.; Capelli, P.; Zamboni, G.; Falconi, M.; Scarpa, A. Ampulla of vater cancers: T-stage and histological subtype but not Dpc4 expression predict prognosis. Virchows Arch. 2002, 441, 19–24. [Google Scholar] [CrossRef]
- Roh, Y.H.; Kim, Y.H.; Lee, H.W.; Kim, S.J.; Roh, M.S.; Jeong, J.S.; Jung, G.J. The clinicopathologic and immunohistochemical characteristics of ampulla of Vater carcinoma: The intestinal type is associated with a better prognosis. Hepatogastroenterology 2007, 54, 1641–1644. [Google Scholar] [PubMed]
- Offerhaus, G.J.; Giardiello, F.M.; Krush, A.J.; Booker, S.V.; Tersmette, A.C.; Kelley, N.C.; Hamilton, S.R. The risk of upper gastrointestinal cancer in familial adenomatous polyposis. Gastroenterology 1992, 102, 1980–1982. [Google Scholar] [CrossRef] [PubMed]
- Perrone, G.; Santini, D.; Zagami, M.; Vincenzi, B.; Verz, A.; Morini, S.; Borzomati, D.; Coppola, R.; Antinori, A.; Magistrelli, P.; et al. COX-2 expression of ampullary carcinoma: Correlation with different histotypes and clinicopathological parameters. Virchows Arch. 2006, 449, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.F.; Tang, K.; Sun, F.B.; Sui, L.L.; Xu, G. Partial Resection of the Pancreatic Head and Duodenum for Management of Carcinoma of the Ampulla of Vater: A Case Report. Anticancer Res. 2016, 36, 1319–1324. [Google Scholar] [PubMed]
- Kimchi, N.A.; Mindrul, V.; Broide, E.; Scapa, E. The contribution of endoscopy and biopsy to the diagnosis of periampullary tumors. Endoscopy 1998, 30, 538–543. [Google Scholar] [CrossRef]
- Bisschops, R.; Areia, M.; Coron, E.; Dobru, D.; Kaskas, B.; Kuvaev, R.; Pech, O.; Ragunath, K.; Weusten, B.; Familiari, P.; et al. Performance measures for upper gastrointestinal endoscopy: A European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative. Endoscopy 2016, 48, 843–864. [Google Scholar] [CrossRef]
- Vanbiervliet, G.; Strijker, M.; Arvanitakis, M.; Aelvoet, A.; Arnelo, U.; Beyna, T.; Busch, O.; Deprez, P.H.; Kunovsky, L.; Larghi, A. Endoscopic management of ampullary tumors: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2021, 4, 429–448. [Google Scholar] [CrossRef]
- Napoleon, B.; Gincul, R.; Ponchon, T.; Berthiller, J.; Escourrou, J.; Canard, J.M.; Boyer, J.; Barthet, M.; Ponsot, P.; Laugier, R.; et al. Endoscopic papillectomy for early ampullary tumors: Long-term results from a large multicenter prospective study. Endoscopy 2014, 46, 127–134. [Google Scholar] [CrossRef]
- Van der Wiel, S.E.; Poley, J.W.; Koch, A.D.; Bruno, M.J. Endoscopic resection of advanced ampullary adenomas: A single-center 14-year retrospective cohort study. Surg. Endosc. 2019, 33, 1180–1188. [Google Scholar] [CrossRef]
- Irani, S.; Arai, A.; Ayub, K.; Biehl, T.; Brandabur, J.J.; Dorer, R.; Gluck, M.; Jiranek, G.; Patterson, D.; Schembre, D.; et al. Papillectomy for ampullary neoplasm: Results of a single referral center over a 10-year period. Gastrointest. Endosc. 2009, 70, 923–932. [Google Scholar] [CrossRef]
- Ödemiş, B.; Durak, M.B.; Cengiz, M. Endoscopic ampullectomy of benign ampullary lesions: Outcomes from a single center study. Surg. Laparosc. Endosc. Percutan. Tech. 2020, 30, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.; Qi, Z.; Bahin, F.F.; Awadie, H.; Nayyar, D.; Ma, M.; Voermans, R.P.; Williams, S.J.; Lee, E.; Bourke, M.J. Outcomes after endoscopic resection of large laterally spreading lesions of the papilla and conventional ampullary adenomas are equivalent. Endoscopy 2018, 50, 972–983. [Google Scholar] [PubMed]
- Pérez-Cuadrado-Robles, E.; Piessevaux, H.; Moreels, T.G.; Yeung, R.; Aouattah, T.; Komuta, M.; Dano, H.; Jouret-Mourin, A.; Deprez, P.H. Combined excision and ablation of ampullary tumors with biliary or pancreatic intraductal extension is effective even in malignant neoplasms. United Eur. Gastroenterol. J. 2019, 7, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Binmoeller, K.F.; Boaventura, S.; Ramsperger, K.; Soehendra, N. Endoscopic snare excision of benign adenomas of the papilla of Vater. Gastrointest. Endosc. 1993, 39, 127–131. [Google Scholar] [CrossRef]
- Spadaccini, M.; Fugazza, A.; Frazzoni, L.; Leo, M.D.; Auriemma, F.; Carrara, S.; Maselli, R.; Galtieri, P.A.; Chandrasekar, V.T.; Fuccio, L.; et al. Endoscopic papillectomy for neoplastic ampullary lesions: A systematic review with pooled analysis. United Eur. Gastroenterol. J. 2020, 8, 44–51. [Google Scholar] [CrossRef]
- Winter, J.M.; Cameron, J.L.; Olino, K.; Herman, J.M.; de Jong, M.C.; Hruban, R.H.; Wolfgang, C.L.; Eckhauser, F.; Edil, B.H.; Choti, M.A.; et al. Clinicopathologic analysis of ampullary neoplasms in 450 patients: Implications for surgical strategy and long-term prognosis. J. Gastrointest. Surg. 2010, 14, 379–387. [Google Scholar] [CrossRef]
- Patel, V.; Jowell, P.; Obando, J.; Guy, C.D.; Burbridge, R.A. Does ampullary adenoma size predict invasion on EUS? Does invasion on EUS predict presence of malignancy? Endosc. Int. Open 2016, 4, E1313–E1318. [Google Scholar] [CrossRef]
- Park, J.S.; Seo, D.W.; Song, T.J.; Park, D.H.; Lee, S.S.; Lee, S.K.; Kim, M.H. Usefulness of white light imaging-guided narrow-band imaging for the differential diagnosis of small ampullary lesions. Gastrointest. Endosc. 2015, 82, 94–101. [Google Scholar] [CrossRef]
- Itoi, T.; Tsuji, S.; Sofuni, A.; Itokawa, F.; Kurihara, T.; Tsuchiya, T.; Ishii, K.; Ikeuchi, N.; Igarashi, M.; Gotoda, T.; et al. A novel approach emphasizing preoperative margin enhancement of tumor of the major duodenal papilla with narrow-band imaging in comparison to indigo carmine chromo-endoscopy (with videos). Gastrointest. Endosc. 2009, 69, 136–141. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Enjoji, M.; Kitamura, K. Endoscopic biopsy has limited accuracy in diagnosis of ampullary tumors. Gastrointest. Endosc. 1990, 36, 588–592. [Google Scholar] [CrossRef]
- Rodríguez, C.; Borda, F.; Elizalde, I.; Jiménez Pérez, F.J.; Carral, D. How accurate is preoperative diagnosis by endoscopic biopsies in ampullary tumours? Rev. Española Enfermedades Dig. 2002, 94, 585–592. [Google Scholar]
- Menzel, J.; Poremba, C.; Dietl, K.H.; Böcker, W.; Domschke, W. Tumors of the papilla of Vater– inadequate diagnostic impact of endoscopic forceps biopsies taken prior to and following sphincterotomy. Ann. Oncol. 1999, 10, 1227–1231. [Google Scholar] [CrossRef]
- Elek, G.; Gyôri, S.; Tóth, B.; Pap, A. Histological evaluation of preoperative biopsies from ampulla vateri. Pathol. Oncol. Res. 2003, 9, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Grobmyer, S.R.; Stasik, C.N.; Draganov, P.; Hemming, A.W.; Dixon, L.R.; Vogel, S.B.; Hochwald, S.N. Contemporary results with ampullectomy for 29 “benign” neoplasms of the ampulla. J. Am. Coll. Surg. 2008, 206, 466–471. [Google Scholar] [CrossRef]
- Laleman, W.; Verreth, A.; Topal, B.; Aerts, R.; Komuta, M.; Roskams, T.; Van der Merwe, S.; Cassiman, D.; Nevens, F.; Verslype, C.; et al. Endoscopic resection of ampullary lesions: A single-center 8-year retrospective cohort study of 91 patients with long-term follow-up. Surg. Endosc. 2013, 27, 3865–3876. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Wang, Z.; Cai, F.; Linghu, E.; Sun, G.; Wang, X.; Meng, J.; Du, H.; Yang, Y.; Li, W. New experience of endoscopic papillectomy for ampullary neoplasms. Surg. Endosc. 2019, 33, 612–619. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.N.; Kim, K.M.; Shin, J.U.; Lee, J.K.; Lee, K.T.; Lee, K.H.; Kim, K.M.; Lim, J.H. Prediction of carcinoma after resection in subjects with ampullary adenomas on endoscopic biopsy. J. Clin. Gastroenterol. 2013, 47, 346–351. [Google Scholar] [CrossRef]
- Alali, A.; Espino, A.; Moris, M.; Martel, M.; Schwartz, I.; Cirocco, M.; Streutker, C.; Mosko, J.; Kortan, P.; Barkun, A.; et al. Endoscopic resection of ampullary tumours: Long-term outcomes and adverse events. J. Can. Assoc. Gastroenterol. 2020, 3, 17–25. [Google Scholar] [CrossRef]
- Bourgeois, N.; Dunham, F.; Verhest, A.; Cremer, M. Endoscopic biopsies of the papilla of Vater at the time of endoscopic sphincterotomy: Difficulties in interpretation. Gastrointest. Endosc. 1984, 30, 163–166. [Google Scholar] [CrossRef]
- Leese, T.; Neoptolemos, J.P.; West, K.P.; Talbot, I.C.; Carr-Locke, D.L. Tumours and pseudotumours of the region of the ampulla of Vater: An endoscopic, clinical and pathological study. Gut 1986, 27, 1186–1192. [Google Scholar] [CrossRef]
- Ponchon, T.; Aucia, N.; Mitchell, R.; Chavaillon, A.; Bory, R.; Hedelius, F. Biopsies of the ampullary region in patients suspected to have sphincter of Oddi dysfunction. Gastrointest. Endosc. 1995, 42, 296–300. [Google Scholar] [CrossRef]
- Zhou, Y.; Li, D.; Wu, L.; Si, X. The histopathologic type predicts survival of patients with ampullary carcinoma after resection: A meta-analysis. Pancreatology 2017, 17, 273–278. [Google Scholar] [CrossRef]
- Ang, D.C.; Shia, J.; Tang, L.H.; Katabi, N.; Klimstra, D.S. The utility of immunohistochemistry in subtyping adenocarcinoma of the ampulla of vater. Am. J. Surg. Pathol. 2014, 38, 1371–1379. [Google Scholar] [CrossRef] [PubMed]
- Gingras, M.C.; Covington, K.R.; Chang, D.K.; Donehower, L.A.; Gill, A.J.; Ittmann, M.M.; Creighton, C.J.; Johns, A.L.; Shinbrot, E.; Dewal, N.; et al. Ampullary cancers harbor ELF3 tumor suppressor gene mutations and exhibit frequent WNT dysregulation. Cell Rep. 2016, 14, 907–919. [Google Scholar] [CrossRef]
- Ye, X.; Wang, L.; Jin, Z. Diagnostic accuracy of endoscopic ultrasound and intraductal ultrasonography for assessment of ampullary tumors: A meta-analysis. Scand. J. Gastroenterol. 2022, 10, 1158–1168. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Tseng, L.J.; Yang, C.C.; Yeh, Y.H. Preoperative evaluation of periampullary tumors by endoscopic sonography, transabdominal sonography, and computed tomography. J. Clin. Ultrasound 2001, 29, 313–321. [Google Scholar] [CrossRef]
- Skordilis, P.; Mouzas, I.A.; Dimoulios, P.D.; Alexandrakis, G.; Moschandrea, J.; Kouroumalis, E. Is endosonography an effective method for detection and local staging of the ampullary carcinoma? A prospective study. BMC Surg. 2002, 2, 1. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.H.; Yang, C.C.; Yeh, Y.H.; Chou, D.A.; Nien, C.K. Reappraisal of endosonography of ampullary tumors: Correlation with transabdominal sonography, CT, and MRI. J. Clin. Ultrasound 2009, 37, 18–25. [Google Scholar] [CrossRef]
- Artifon, E.L.; Couto, D.; Sakai, P.; da Silveira, E.B. Prospective evaluation of EUS versus CT scan for staging of ampullary cancer. Gastrointest. Endosc. 2009, 70, 290–296. [Google Scholar] [CrossRef]
- Manta, R.; Conigliaro, R.; Castellani, D.; Messerotti, A.; Bertani, H.; Sabatino, G.; Vetruccio, E.; Losi, L.; Villanacci, V.; Bassotti, G. Linear endoscopic ultrasonography vs magnetic resonance imaging in ampullary tumors. World J. Gastroenterol. 2010, 16, 5592–5597. [Google Scholar] [CrossRef]
- Yamamoto, K.; Iwasaki, E.; Itoi, T. Insights and updates on endoscopic papillectomy. Expert. Rev. Gastroenterol. Hepatol. 2020, 14, 435–444. [Google Scholar] [CrossRef]
- Suzuki, K.; Kantou, U.; Murakami, Y. Two cases with ampullary cancer who underwent endoscopic excision. Prog. Dig. Endosc. 1983, 23, 236–239. [Google Scholar]
- Li, S.L.; Li, W.; Yin, J.; Wang, Z.K. Endoscopic papillectomy for ampullary adenomatous lesions: A literature review. World J. Gastrointest. Oncol. 2021, 13, 1466–1474. [Google Scholar] [CrossRef] [PubMed]
- Menees, S.B.; Schoenfeld, P.; Kim, H.M.; Elta, G.H. A survey of ampullectomy practices. World J. Gastroenterol. 2009, 15, 3486–3492. [Google Scholar] [CrossRef] [PubMed]
- Hyun, J.J.; Lee, T.H.; Park, J.S.; Han, J.H.; Jeong, S.; Park, S.M.; Lee, H.S.; Moon, J.H.; Park, S.H. A prospective multicenter study of sub-mucosal injection to improve endoscopic snare papillectomy for ampullary adenoma. Gastrointest. Endosc. 2017, 85, 746–755. [Google Scholar] [CrossRef]
- Desilets, D.J.; Dy, R.M.; Ku, P.M.; Hanson, B.L.; Elton, E.; Mattia, A.; Howell, D.A. Endoscopic management of tumors of the major duodenal papilla: Refined techniques to improve outcome and avoid complications. Gastrointest. Endosc. 2001, 54, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Fugazza, A.; Troncone, E.; Amato, A.; Tarantino, I.; Iannone, A.; Donato, G.; D’Amico, F.; Mogavero, G.; Amata, M.; Fabbri, C.; et al. Difficult biliary cannulation in patients with distal malignant biliary obstruction: An underestimated problem? Dig. Liver Dis. 2022, 54, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Espinel, J.; Pinedo, E.; Ojeda, V.; Guerra Del Río, M. Endoscopic ampullectomy: A technical review. Rev. Esp. Enferm. Dig. 2016, 108, 271–278. [Google Scholar] [CrossRef]
- Lee, S.K.; Kim, M.H.; Seo, D.W.; Lee, S.S.; Park, J.S. Endoscopic sphincterotomy and pancreatic duct stent placement before endoscopic papillectomy: Are they necessary and safe procedures? Gastrointest. Endosc. 2002, 55, 302–304. [Google Scholar] [CrossRef]
- Iwasaki, E.; Minami, K.; Itoi, T.; Yamamoto, K.; Tsuji, S.; Sofuni, A.; Tsuchiya, T.; Tanaka, R.; Tonozuka, R.; Machida, Y.; et al. Impact of electrical pulse cut mode during endoscopic papillectomy: Pilot randomized clinical trial. Dig. Endosc. 2020, 32, 127–135. [Google Scholar] [CrossRef]
- Binda, C.; Fabbri, S.; Cucchetti, A.; Mutignani, M.; Tringali, A.; Di Mitri, R.; Fugazza, A.; Sassatelli, R.; Gabbrielli, A.; Arcidiacono, P.; et al. Endoscopic papillectomy: A multicenter, retrospective, nationwide study after the standardization of the technique. Endoscopy 2023, 55, S94. [Google Scholar] [CrossRef]
- Takahara, N.; Tsuji, Y.; Nakai, Y.; Suzuki, Y.; Inokuma, A.; Kanai, S.; Noguchi, K.; Sato, T.; Hakuta, R.; Ishigaki, K.; et al. A Novel Technique of Endoscopic Papillectomy with Hybrid Endoscopic Submucosal Dissection for Ampullary Tumors: A Proof-of-Concept Study (with Video). J. Clin. Med. 2020, 9, 2671. [Google Scholar] [CrossRef]
- Vu Trung, K.; Abou-Ali, E.; Caillol, F.; Paik, W.H.; Napoleon, B.; Masaryk, V.; van der Wiel, S.E.; Pérez-Cuadrado-Robles, E.; Musquer, N.; Halimi, A. Endoscopic papillectomy for ampullary lesions in patients with familial adenomatous polyposis compared with sporadic lesions: A propensity score-matched cohort. Endoscopy 2023, 55, 709–718. [Google Scholar] [CrossRef] [PubMed]
- Sahar, N.; Krishnamoorthi, R.; Kozarek, R.A.; Gluck, M.; Larsen, M.; Ross, A.S.; Irani, S. Long-term outcomes of endoscopic papillectomy for ampullary adenomas. Dig. Dis. Sci. 2020, 65, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Sofuni, A.; Tsuchiya, T.; Ishii, K.; Tsuji, S.; Tanaka, R.; Tonozuka, R.; Honjo, M.; Mukai, S.; Fujita, M. Clinical impact of piecemeal resection concerning the lateral spread of ampullary adenomas. Intern. Med. 2019, 58, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Alfarone, L.; Spadaccini, M.; Franchellucci, G.; Khalaf, K.; Massimi, D.; De Marco, A.; Ferretti, S.; Poletti, V.; Facciorusso, A.; Maselli, R.; et al. Endoscopic resection of non-ampullary duodenal adenomas: Is cold snaring the promised land? World J. Gastrointest. Endosc. 2023, 15, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Repici, A.; Capogreco, A.; Spadaccini, M.; Maselli, R.; Galtieri, P.A.; Fugazza, A.; Carrara, S.; Colombo, M.; Schachschal, G.; Creutzfeld, A. Cold versus hot EMR for large duodenal adenomas. Gut 2022, 71, 1763–1765. [Google Scholar] [CrossRef]
- Bohnacker, S.; Seitz, U.; Nguyen, D.; Thonke, F.; Seewald, S.; de Weerth, A.; Ponnudurai, R.; Omar, S.; Soehendra, N. Endoscopic resection of benign tumors of the duodenal papilla without and with intraductal growth. Gastrointest. Endosc. 2005, 62, 551–560. [Google Scholar] [CrossRef]
- Camus, M.; Napoléon, B.; Vienne, A.; Le Rhun, M.; Leblanc, S.; Barret, M.; Chaussade, S.; Robin, F.; Kaddour, N.; Prat, F. Efficacy and safety of endo-biliary radiofrequency ablation for the eradication of residual neoplasia after endoscopic papillectomy: A multicenter prospective study. Gastrointest. Endosc. 2018, 88, 511–518. [Google Scholar] [CrossRef]
- Cho, S.H.; Oh, D.; Song, T.J.; Park, D.H.; Seo, D.W.; Lee, S.K.; Kim, M.H.; Lee, S.S. Long-term Outcomes of Endoscopic Intraductal Radiofrequency Ablation for Ampullary Adenoma with Intraductal Extension after Endoscopic Snare Papillectomy. Gut Liver 2023, 17, 638–646. [Google Scholar] [CrossRef]
- Harewood, G.C.; Pochron, N.L.; Gostout, C.J. Prospective, randomized, controlled trial of prophylactic pancreatic stent placement for endoscopic snare excision of the duodenal ampulla. Gastrointest. Endosc. 2005, 62, 367–370. [Google Scholar] [CrossRef]
- Anderloni, A.; Fugazza, A.; Maroni, L.; Ormando, V.; Maselli, R.; Carrara, S.; Cappello, A.; Mangiavillano, B.; Omodei, P.; Preatoni, P.; et al. New biliary and pancreatic biodegradable stent placement: A single-center, prospective, pilot study (with video). Gastrointest. Endosc. 2020, 92, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Campos, S.T.; Bruno, M.J. Endoscopic Papillectomy. Gastrointest. Endosc. Clin. N. Am. 2022, 32, 545–562. [Google Scholar] [CrossRef]
- Tringali, A.; Valerii, G.; Boškoski, I.; Familiari, P.; Landi, R.; Perri, V.; Costamagna, G. Endoscopic snare papillectomy for adenoma of the ampulla of vater: Long-term results in 135 consecutive patients. Dig. Liver Dis. 2020, 52, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Garg, R.; Thind, K.; Bhalla, J.; Simonson, M.T.; Simons-Linares, C.R.; Singh, A.; Joyce, D.; Chahal, P. Long-term recurrence after endoscopic versus surgical ampullectomy of sporadic ampullary adenomas: A systematic review and meta-analysis. Surg. Endosc. 2023, 37, 5022–5044. [Google Scholar] [CrossRef] [PubMed]
- Nappo, G.; Gentile, D.; Galvanin, J.; Capretti, G.; Ridolfi, C.; Petitti, T.; Spaggiari, P.; Carrara, S.; Gavazzi, F.; Repici, A.; et al. Trans-duodenal ampullectomy for ampullary neoplasms: Early and long-term outcomes in 36 consecutive patients. Surg. Endosc. 2020, 34, 4358–4368. [Google Scholar] [CrossRef]
- Mendonça, E.Q.; Bernardo, W.M.; Moura, E.G.; Chaves, D.M.; Kondo, A.; Pu, L.Z.; Baracat, F.I. Endoscopic versus surgical treatment of ampullary adenomas: A systematic review and meta-analysis. Clin. Sao Paulo Braz. 2016, 71, 28–35. [Google Scholar] [CrossRef]
- Yoon, Y.S.; Kim, S.W.; Park, S.J.; Lee, H.S.; Jang, J.Y.; Choi, M.G.; Kim, W.H.; Lee, K.U.; Park, Y.H. Clinicopathologic analysis of early ampullary cancers with a focus on the feasibility of ampullectomy. Ann. Surg. 2005, 242, 92–100. [Google Scholar] [CrossRef]
- Hsu, H.P.; Yang, T.M.; Hsieh, Y.H.; Shan, Y.S.; Lin, P.W. Predictors for patterns of failure after pancreaticoduodenectomy in ampullary cancer. Ann. Surg. Oncol. 2007, 14, 50–60. [Google Scholar] [CrossRef]
- Lee, H.; Park, J.Y.; Kwon, W.; Heo, J.S.; Choi, D.W.; Choi, S.H. Transduodenal ampullectomy for the treatment of early-stage ampulla of vater cancer. World J. Surg. 2016, 40, 967–973. [Google Scholar] [CrossRef]
- Kawabata, Y.; Ishikawa, N.; Moriyama, I.; Tajima, Y. What is an adequate surgical management for pTis and pT1 early ampullary carcinoma? Hepatogastroenterology 2014, 61, 12–17. [Google Scholar] [PubMed]
- Gao, Y.; Zhu, Y.; Huang, X.; Wang, H.; Huang, X.; Yuan, Z. Transduodenal ampullectomy provides a less invasive technique to cure early ampullary cancer. BMC Surg. 2016, 16, 36. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Liu, H.; Li, Z.; Yang, C.; Sun, Y.; Wang, C. Long-term prognosis of surgical treatment for early ampullary cancers and implications for local ampullectomy. BMC Surg. 2015, 15, 32. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).