
Analysis of Nasal Foreign Bodies in South Korea: Over 10-Year Experience



Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Park, J.W.; Jung, J.H.; Kwak, Y.H.; Jung, J.Y. Epidemiology of pediatric visits to the emergency department due to foreign body injuries in South Korea: Nationwide cross-sectional study. Medicine 2019, 98, e15838. [Google Scholar] [CrossRef]
- Kiger, J.R.; Brenkert, T.E.; Losek, J.D. Nasal foreign body removal in children. Pediatr. Emerg. Care 2008, 24, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Gregori, D.; Salerni, L.; Scarinzi, C.; Morra, B.; Berchialla, P.; Snidero, S.; Corradetti, R.; Passali, D. Foreign bodies in the nose causing complications and requiring hospitalization in children 0–14 age: Results from the European survey of foreign bodies injuries study. Rhinology 2008, 46, 28–33. [Google Scholar] [PubMed]
- Zavdy, O.; Viner, I.; London, N.; Menzely, T.; Hod, R.; Raveh, E.; Gilony, D. Intranasal foreign bodies: A 10-year analysis of a large cohort, in a tertiary medical center. Am. J. Emerg. Med. 2021, 50, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Zeng, N.; Chen, G.; Chen, Y.; Wu, Z.; Pan, H.; Teng, Y.; Ma, X.; Li, L. Presentation and management of nasal foreign bodies in a Chinese metro area. Medicine 2021, 100, e25626. [Google Scholar] [CrossRef] [PubMed]
- Pagella, F.; Pusateri, A.; Matti, E.; Riceputi, G.; Brambilla, I.; Marseglia, G.L.; Benazzo, M. Nasal foreign bodies management in children: Our experience in 106 patients. Clin. Otolaryngol. 2019, 44, 660–663. [Google Scholar] [CrossRef] [PubMed]
- Cetinkaya, E.A.; Arslan, İ.B.; Cukurova, İ. Nasal foreign bodies in children: Types, locations, complications and removal. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1881–1885. [Google Scholar] [CrossRef]
- Sajid, T.; Shah, M.I.; Qamar Naqvi, S.R. Pattern of presentation of nasal foreign bodies, An Experience with 155 Patients. J. Ayub Med. Coll. Abbottabad 2018, 30, 548–550. [Google Scholar] [PubMed]
- Hira, İ.; Tofar, M.; Bayram, A.; Yaşar, M.; Mutlu, C.; Özcan, İ. Childhood nasal foreign bodies: Analysis of 1724 cases. Turk. Arch. Otorhinolaryngol. 2019, 57, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Ocagli, H.; Azzolina, D.; Bressan, S.; Bottigliengo, D.; Settin, E.; Lorenzoni, G.; Gregori, D.; Da Dalt, L. Epidemiology and trends over time of foreign body injuries in the pediatric emergency department. Children 2021, 8, 938. [Google Scholar] [CrossRef] [PubMed]
- Abou-Elfadl, M.; Horra, A.; Abada, R.L.; Mahtar, M.; Roubal, M.; Kadiri, F. Nasal foreign bodies: Results of a study of 260 cases. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2015, 132, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Peyre, H.; Hoertel, N.; Bernard, J.Y.; Rouffignac, C.; Forhan, A.; Taine, M.; Heude, B.; Ramus, F. Sex differences in psychomotor development during the preschool period: A longitudinal study of the effects of environmental factors and of emotional, behavioral, and social functioning. J. Exp. Child. Psychol. 2019, 178, 369–384. [Google Scholar] [CrossRef] [PubMed]
- Toivainen, T.; Papageorgiou, K.A.; Tosto, M.G.; Kovas, Y. Sex differences in non-verbal and verbal abilities in childhood and adolescence. Intelligence 2017, 64, 81–88. [Google Scholar] [CrossRef]
- Dann, L.; Doody, J.; Howard, R.; Blackburn, C.; Russell, J.; Barrett, M. Nasal foreign bodies in the paediatric emergency department. Ir. J. Med. Sci. 2019, 188, 1401–1405. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.A.; Goldberg, E.; Horev, Z. Removal of nasal foreign bodies in children. Clin. Pediatr. 1993, 32, 192. [Google Scholar] [CrossRef] [PubMed]
- Lou, Z.C. Analysis of nasal foreign bodies in 341 children. J. Laryngol. Otol. 2019, 133, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Yaroko, A.A.; Baharudin, A. Patterns of nasal foreign body in northeast Malaysia: A five-year experience. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2015, 132, 257–259. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Thabet, M.H.; Basha, W.M.; Askar, S. Button battery foreign bodies in children: Hazards, management, and recommendations. Biomed. Res. Int. 2013, 2013, 846091. [Google Scholar] [CrossRef] [PubMed]
- Guidera, A.K.; Stegehuis, H.R. Button batteries: The worst case scenario in nasal foreign bodies. N. Z. Med. J. 2010, 123, 68–73. [Google Scholar]
- Mackle, T.; Conlon, B. Foreign bodies of the nose and ears in children. Should these be managed in the accident and emergency setting? Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 425–428. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
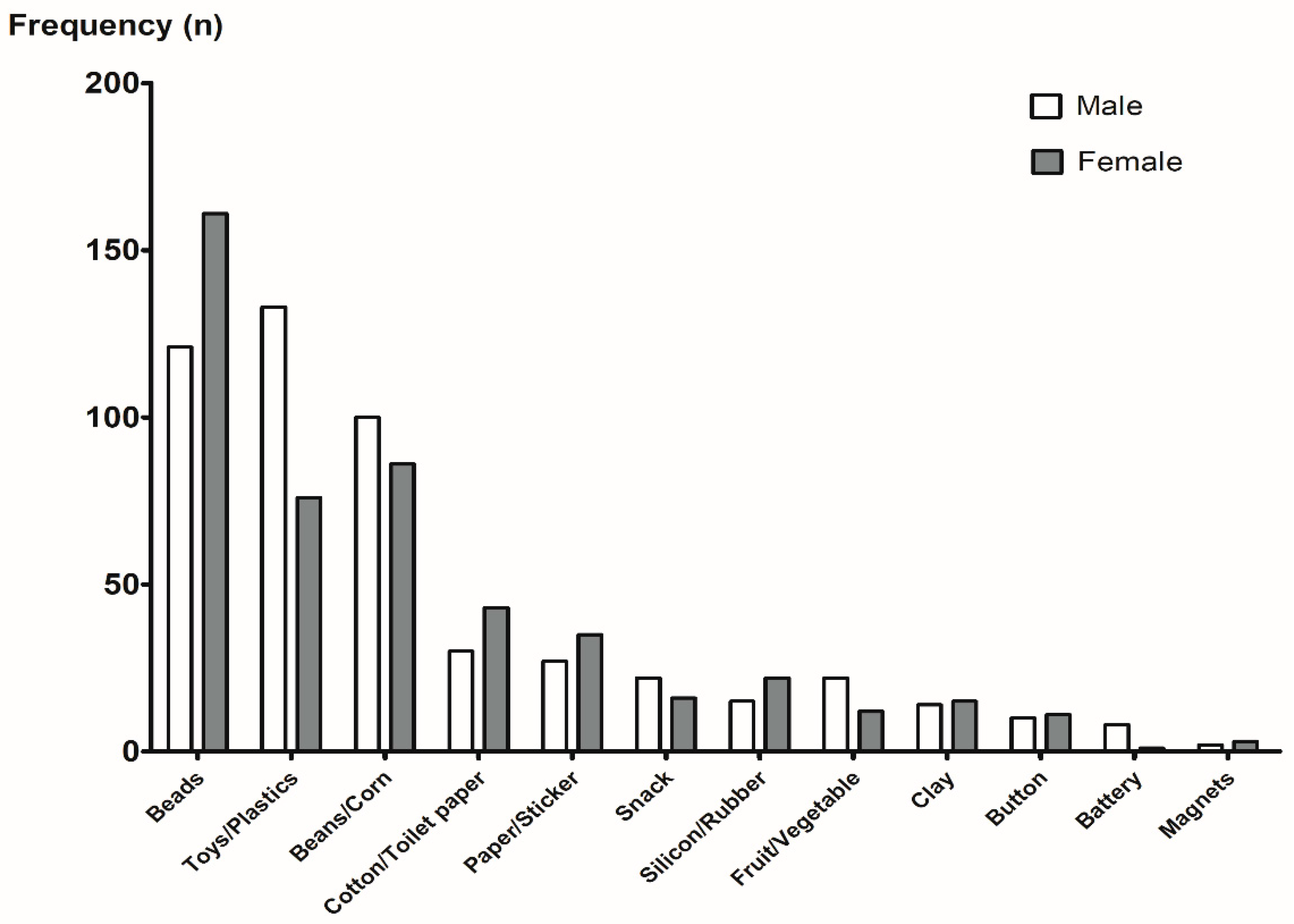
| Types of Foreign Bodies | Number (Percentage) |
|---|---|
| Beads | 282 (24.0) |
| Toys/Plastics | 209 (17.8) |
| Beans/Corn | 186 (15.8) |
| Cotton/Toilet paper | 73 (6.2) |
| Paper/Sticker | 62 (5.3) |
| Snack | 38 (3.2) |
| Silicon/Rubber | 37 (3.1) |
| Fruit/Vegetable | 34 (2.9) |
| Clay | 29 (2.5) |
| Button | 21 (1.8) |
| Battery | 9 (0.8) |
| Magnets | 5 (0.4) |
| Others | 171 (14.5) |
| Age Groups | Top 5 Types of Foreign Bodies (Percentage) |
|---|---|
| 1–2 years | Beans/Corn (34.0%), Beads (17.5%), Toys/Plastics (11.3%), Cotton/Toilet paper (9.3%), Fruit/Vegetable (8.2%) |
| 2–3 years | Beans/Corn (24.5%), Beads (21.6%), Toys/Plastics (16.4%), Cotton/Toilet paper (8.6%), Paper/Sticker (7.5%) |
| 3–4 years | Beads (28.0%), Toys/Plastics (26.2%), Beans/Corn (16.8%), Paper/Sticker (6.1%), Silicon/Rubber (5.0%) |
| 4–5 years | Beads (45.0%), Toys/Plastics (25.5%), Beans/Corn (7.4%), Cotton/Toilet paper (6.0%), Paper/Sticker, Seeds (3.4%) |
| 5–6 years | Beads (42.1%), Toys/Plastics (24.6%), Cotton/Toilet paper (12.3%), Beans/Corn, Paper/Sticker (3.5%) |
| 6–7 years | Beads (30.8%), Toys/Plastics (26.9%), Beans/Corn, Cotton/Toilet paper, Paper/Sticker (3.5%) |
| 7–12 years | Beads (35.0%), Toys/Plastics (25.0%), Cotton/Toilet paper (15.0%), Paper/Sticker, Clay (10.0%) |
| ≥19 years | Cotton/Toilet paper (30.0%), Beads (10.0%), Rubber (10.0%), Fruits/Vegetable (10.0%), Paper/Sticker (10.0%) |
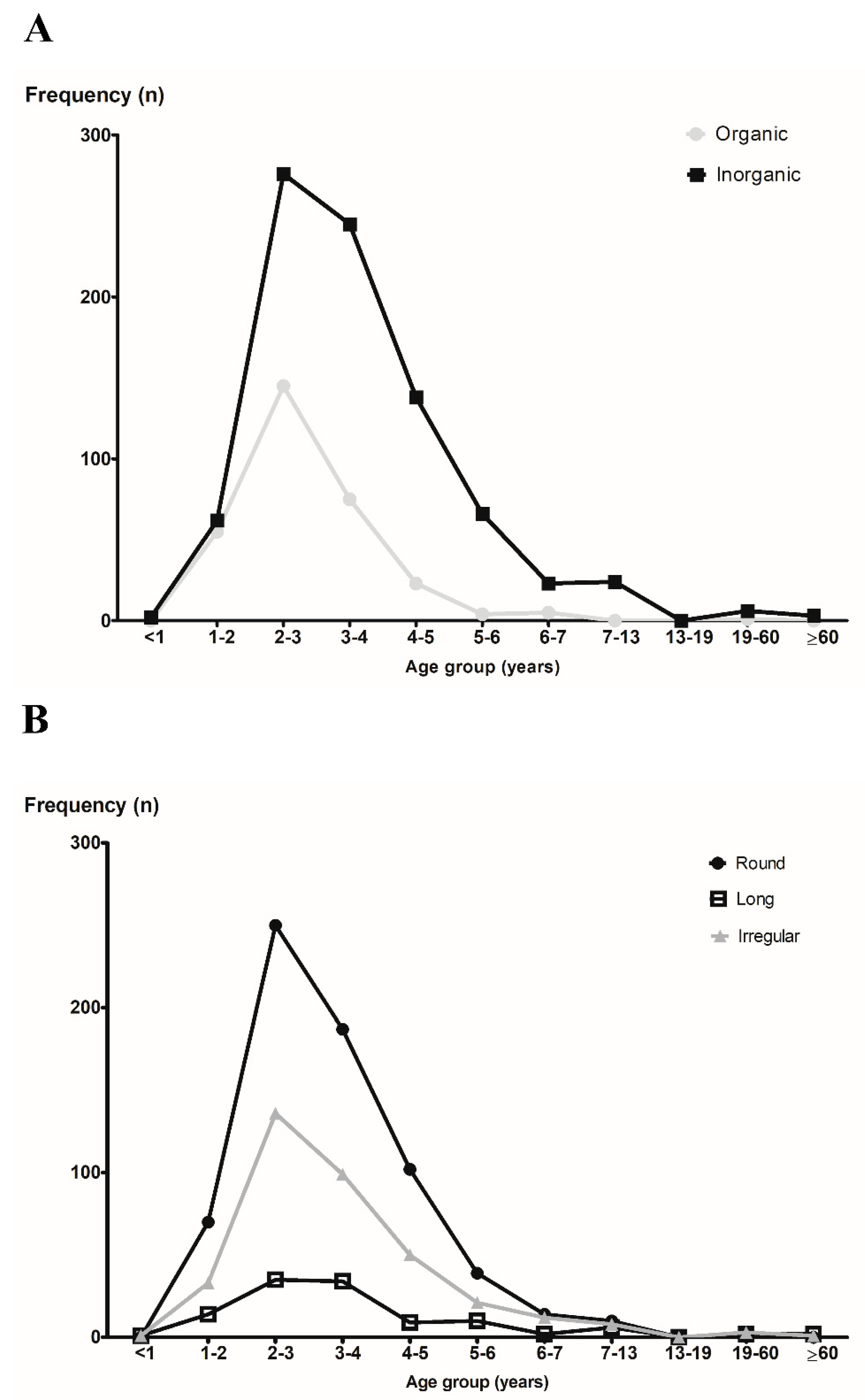
| Shape | Organic | Inorganic | Total |
|---|---|---|---|
| Round | 276 | 398 | 674 (58.5%) |
| Long | 13 | 102 | 115 (10.0%) |
| Irregular | 19 | 345 | 364 (31.5%) |
| Total | 308 (26.7%) | 845 (73.3%) | 1153 |
| Symptoms | Onset (Days), Number (Percentage) | |||
|---|---|---|---|---|
| 0 | 1 | ≥2 | Total | |
| No symptoms | 1010 (98.6) | 13 (1.3) | 1 (0.1) | 1024 (83.4) |
| Foreign body sense | 25 (89.3) | 2 (7.1) | 1 (3.6) | 28 (2.3) |
| Pain | 24 (92.3) | 1 (3.8) | 1 (3.8) | 26 (2.1) |
| Epistaxis | 21 (91.3) | 0 (0.0) | 2 (8.7) | 23 (1.9) |
| Rhinorrhea | 12 (66.7) | 4 (22.2) | 2 (11.1) | 18 (1.5) |
| Cough | 10 (90.9) | 0 (0.0) | 1 (9.1) | 11 (0.9) |
| Nasal obstruction | 7 (70.0) | 1 (10.0) | 2 (20.0) | 10 (0.8) |
| Hoarseness | 1 (100.0) | 0 (0.0) | 0 (0.0) | 1 (0.1) |
| Foul odor | 0 (0.0) | 1 (100.0) | 0 (0.0) | 1 (0.1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, H.J.; Kim, S.W.; Lee, J.S.; Choi, H.G.; Wee, J.H. Analysis of Nasal Foreign Bodies in South Korea: Over 10-Year Experience. Diagnostics 2022, 12, 1810. https://doi.org/10.3390/diagnostics12081810
Jung HJ, Kim SW, Lee JS, Choi HG, Wee JH. Analysis of Nasal Foreign Bodies in South Korea: Over 10-Year Experience. Diagnostics. 2022; 12(8):1810. https://doi.org/10.3390/diagnostics12081810
Chicago/Turabian StyleJung, Hahn Jin, Sun Wook Kim, Joong Seob Lee, Hyo Geun Choi, and Jee Hye Wee. 2022. "Analysis of Nasal Foreign Bodies in South Korea: Over 10-Year Experience" Diagnostics 12, no. 8: 1810. https://doi.org/10.3390/diagnostics12081810
APA StyleJung, H. J., Kim, S. W., Lee, J. S., Choi, H. G., & Wee, J. H. (2022). Analysis of Nasal Foreign Bodies in South Korea: Over 10-Year Experience. Diagnostics, 12(8), 1810. https://doi.org/10.3390/diagnostics12081810