
Temporal Trends in the Prevalence, Treatment and Outcomes of Patients with Acute Coronary Syndrome at High Bleeding Risk


 ,
,
Abstract
1. Introduction
2. Materials and Methods
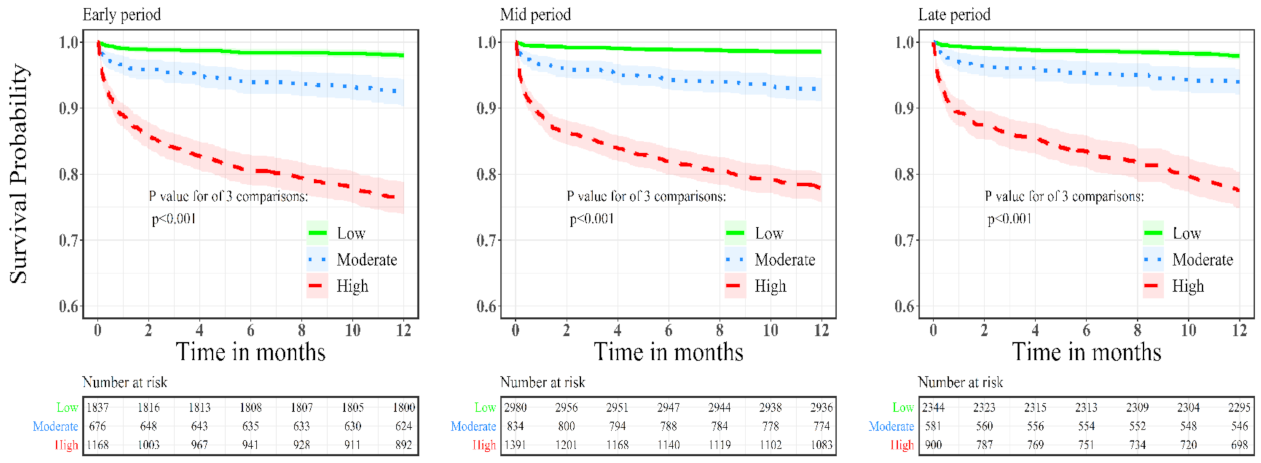
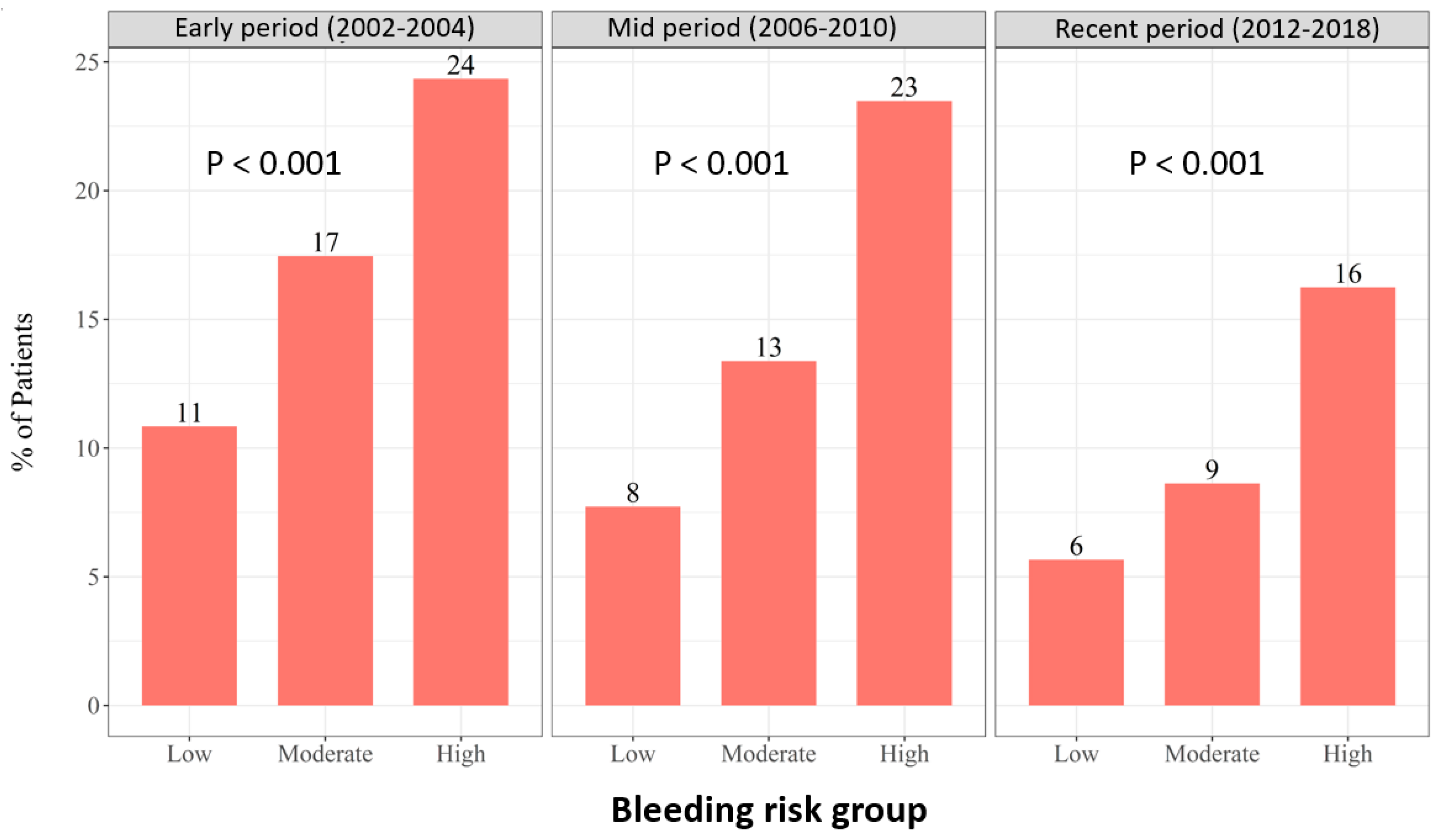
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Cordero, A.; Rodriguez-Manero, M.; García-Acuña, J.M.; López-Palop, R.; Cid, B.; Carrillo, P.; Agra-Bermejo, R.; González-Salvado, V.; Iglesias-Alvarez, D.; Bertomeu-Martínez, V.; et al. Additive value of the CRUSADE score to the GRACE score for mortality risk prediction in patients with acute coronary syndromes. Int. J. Cardiol. 2017, 245, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.J.; Lee, C.H.; Chen, C.C.; Chang, S.H.; Wang, C.Y.; Hsieh, I.C. Predictive performance of HAS-BLED risk score for long-term survival in patients with non-ST elevated myocardial infarction without atrial fibrillation. J. Cardiol. 2017, 69, 136–143. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mehran, R.; Pocock, S.J.; Nikolsky, E.; Clayton, T.; Dangas, G.D.; Kirtane, A.J.; Parise, H.; Fahy, M.; Manoukian, S.V.; Feit, F.; et al. A risk score to predict bleeding in patients with acute coronary syndromes. J. Am. Coll. Cardiol. 2010, 55, 2556–2566. [Google Scholar] [CrossRef] [PubMed]
- Natsuaki, M.; Morimoto, T.; Yamaji, K.; Watanabe, H.; Yoshikawa, Y.; Shiomi, H.; Nakagawa, Y.; Furukawa, Y.; Kadota, K.; Ando, K.; et al. Prediction of Thrombotic and Bleeding Events After Percutaneous Coronary Intervention: CREDO-Kyoto Thrombotic and Bleeding Risk Scores. J. Am. Heart Assoc. 2018, 7, e008708. [Google Scholar] [CrossRef] [PubMed]
- Authors/Task Force Members; ESC Committee for Practice Guidelines (CPG); ESC National Cardiac Societies. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Atherosclerosis 2019, 290, 140–205. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.J.; Ardissino, D.; Murphy, S.A.; Riesmeyer, J.; et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [PubMed]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Puymirat, E.; Taldir, G.; Aissaoui, N.; Lemesle, G.; Lorgis, L.; Cuisset, T.; Bourlard, P.; Maillier, B.; Ducrocq, G.; Ferrieres, J.; et al. Use of invasive strategy in non-ST-segment elevation myocardial infarction is a major determinant of improved long-term survival: FAST-MI (French Registry of Acute Coronary Syndrome). JACC Cardiovasc. Interv. 2012, 5, 893–902. [Google Scholar] [CrossRef] [PubMed]
- Bueno, H.; Rossello, X.; Pocock, S.J.; Van de Werf, F.; Chin, C.T.; Danchin, N.; Lee, S.W.; Medina, J.; Huo, Y. In-Hospital Coronary Revascularization Rates and Post-Discharge Mortality Risk in Non-ST-Segment Elevation Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2019, 74, 1454–1461. [Google Scholar] [CrossRef] [PubMed]
- Shuvy, M.; Beeri, G.; Klein, E.; Cohen, T.; Shlomo, N.; Minha, S.; Pereg, D. Accuracy of the Global Registry of Acute Coronary Events (GRACE) Risk Score in Contemporary Treatment of Patients With Acute Coronary Syndrome. Can. J. Cardiol. 2018, 34, 1613–1617. [Google Scholar] [CrossRef] [PubMed]
- Shuvy, M.; Chen, S.; Vorobeichik, D.; Krashin, E.; Shlomo, N.; Goldenberg, I.; Pereg, D. Temporal trends in management and outcomes of patients with acute coronary syndrome according to renal function. Int. J. Cardiol. 2017, 232, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Subherwal, S.; Bach, R.G.; Chen, A.Y.; Gage, B.F.; Rao, S.V.; Newby, L.K.; Wang, T.Y.; Gibler, W.B.; Ohman, E.M.; Roe, M.T.; et al. Baseline risk of major bleeding in non-ST-segment-elevation myocardial infarction: The CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines) Bleeding Score. Circulation 2009, 119, 1873–1882. [Google Scholar] [CrossRef] [PubMed]
- Ariza-Solé, A.; Sánchez-Elvira, G.; Sánchez-Salado, J.C.; Lorente-Tordera, V.; Salazar-Mendiguchía, J.; Sánchez-Prieto, R.; Romaguera-Torres, R.; Ferreiro-Gutiérrez, J.L.; Gómez-Hospital, J.A.; Cequier-Fillat, A. CRUSADE bleeding risk score validation for ST-segment-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Thromb. Res. 2013, 132, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.K.M.; Mehta, O.H.; Liao, Y.B.; Wang, M.T.M.; Stewart, R.; White, H. Meta-Analysis of Bleeding Scores Performance for Acute Coronary Syndrome. Heart Lung Circ. 2020, 29, 1749–1757. [Google Scholar] [CrossRef] [PubMed]
- Abu-Assi, E.; Raposeiras-Roubin, S.; Lear, P.; Cabanas-Grandío, P.; Girondo, M.; Rodríguez-Cordero, M.; Pereira-López, E.; Romaní, S.G.; González-Cambeiro, C.; Alvarez-Alvarez, B.; et al. Comparing the predictive validity of three contemporary bleeding risk scores in acute coronary syndrome. Eur. Heart J. Acute Cardiovasc. Care 2012, 1, 222–231. [Google Scholar] [CrossRef] [PubMed]
- Castini, D.; Centola, M.; Ferrante, G.; Cazzaniga, S.; Persampieri, S.; Lucreziotti, S.; Salerno-Uriarte, D.; Sponzilli, C.; Carugo, S. Comparison of CRUSADE and ACUITY-HORIZONS Bleeding Risk Scores in Patients With Acute Coronary Syndromes. Heart Lung Circ. 2019, 28, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Kikkert, W.J.; Delewi, R.; Ouweneel, D.M.; van Nes, S.H.; Vis, M.M.; Baan JJr Koch, K.T.; Dangas, G.D.; Mehran, R.; de Winter, R.J.; Peters, R.J.; et al. Prognostic value of access site and nonaccess site bleeding after percutaneous coronary intervention: A cohort study in ST-segment elevation myocardial infarction and comprehensive meta-analysis. JACC Cardiovasc. Interv. 2014, 7, 622–630. [Google Scholar] [CrossRef] [PubMed]
- Kikkert, W.J.; van Geloven, N.; van der Laan, M.H.; Vis, M.M.; Baan, J., Jr.; Koch, K.T.; Peters, R.J.; de Winter, R.J.; Piek, J.J.; Tijssen, J.G.; et al. The prognostic value of bleeding academic research consortium (BARC)-defined bleeding complications in ST-segment elevation myocardial infarction: A comparison with the TIMI (Thrombolysis In Myocardial Infarction), GUSTO (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries), and ISTH (International Society on Thrombosis and Haemostasis) bleeding classifications. J. Am. Coll. Cardiol. 2014, 63, 1866–1875. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | CRUSADE Bleeding Risk | |||
|---|---|---|---|---|
| Low | Moderate | High | p-Value | |
| n | 7386 | 2147 | 3525 | |
| Age, years (median) | 57 | 69 | 75 | <0.001 |
| Gender, male n (%) | 6748 (91) | 1496 (70) | 1927 (55) | <0.001 |
| Dyslipidemia, n (%) | 4746 (64) | 1485 (69) | 2462 (70) | <0.001 |
| Hypertension, n (%) | 3578 (48) | 1477 (69) | 2793 (79) | <0.001 |
| Diabetes mellitus, n (%) | 1745 (24) | 900 (42) | 2071 (59) | <0.001 |
| CKD, n (%) | 109 (1.5) | 175 (8) | 1157 (33) | <0.001 |
| Prior MI, n (%) | 1664 (23) | 731 (34) | 1612 (46) | <0.001 |
| Prior CABG, n (%) | 387 (5) | 261 (12) | 597 (17) | <0.001 |
| Prior CVA/TIA, n (%) | 260 (3.5) | 183 (8.5) | 619 (18) | <0.001 |
| PVD, n (%) | 215 (3) | 200 (9) | 652 (19) | <0.001 |
| Prior medications | ||||
| Aspirin, n (%) | 2709 (38) | 1122 (54) | 2158 (63) | <0.001 |
| Clopidogrel, n (%) | 462 (7) | 207 (10) | 468 (14) | <0.001 |
| ACE-I/ARB, n (%) | 2044 (28) | 959 (45) | 1862 (53) | <0.001 |
| Beta blockers, n (%) | 1908 (27) | 883 (43) | 1797 (53) | <0.001 |
| Statins, n (%) | 2677 (39) | 1078 (53) | 1926 (57) | <0.001 |
| Bleeding Risk | Low | Mod | High | p-Value | Low | Mod | High | p-Value | Low | Mod | High | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | 1855 | 676 | 1171 | 3006 | 845 | 1397 | 2525 | 626 | 957 | |||
| Reperfusion therapy, n (%) | ||||||||||||
| Coronary angiography | 1714 (92) | 619 (92) | 952 (81) | <0.001 | 2855 (95) | 744 (88) | 1012 (72) | <0.001 | 2446 (97) | 593 (95) | 773 (81) | <0.001 |
| PCI | 1160 (63) | 362 (54) | 455 (39) | <0.001 | 2324 (77) | 555 (66) | 690 (49) | <0.001 | 1915 (76) | 438 (70) | 535 (56) | <0.001 |
| CABG | 51 (7) | 22 (10) | 49 (12) | 0.01 | 138 (5) | 74 (9) | 74 (5) | 0.09 | 130 (5) | 32 (5) | 59 (6) | 0.2 |
| Treatment at discharge, n (%) | ||||||||||||
| Aspirin | 1779 (96) | 622 (92) | 988 (84) | <0.001 | 2938 (98) | 807 (97) | 1214 (92) | <0.001 | 2461 (98) | 599 (97) | 818 (91) | <0.001 |
| P2Y12 inhibitor | 1245 (67) | 398 (59) | 499 (43) | <0.001 | 2580 (86) | 637 (76) | 922 (70) | <0.001 | 2309 (92) | 558 (91) | 762 (85) | <0.001 |
| Clopidogrel | 1245 (67) | 398 (59) | 499 (43) | <0.001 | 2579 (86) | 633 (76) | 921 (70) | <0.001 | 608 (24) | 247 (40) | 486 (54) | <0.001 |
| Prasugrel | 0 | 0 | 0 | - | 1 (0) | 4 (0.5) | 1 (0.1) | 0.3 | 883 (35) | 107 (17) | 74 (8) | <0.001 |
| Ticagrelor | 0 | 0 | 0 | - | 0 | 0 | 0 | - | 818 (33) | 204 (33) | 202 (22) | <0.001 |
| Statins | 1483 (80) | 509 (75) | 736 (63) | <0.001 | 2879 (96) | 784 (94) | 1178 (89) | <0.001 | 2429 (98) | 591 (98) | 828 (94) | <0.001 |
| Beta blockers | 1534 (83) | 554 (82) | 811 (69) | <0.001 | 2489 (83) | 685 (82) | 1049 (79) | 0.001 | 1921 (81) | 499 (84) | 698 (80) | 0.52 |
| ACEI/ARB | 1255 (68) | 489 (72) | 825 (71) | 0.07 | 2333 (78) | 681 (82) | 961 (73) | 0.001 | 1998 (85) | 510 (87) | 624 (74) | <0.001 |
| Hypoglycemic drugs | 202 (11) | 105 (16) | 221 (19) | <0.001 | 402 (13) | 196 (23) | 338 (25) | <0.001 | 492 (20) | 208 (33) | 297 (31) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arow, Z.; Ovdat, T.; Gabarin, M.; Omelchenko, A.; Shuvy, M.; Or, T.; Assali, A.; Pereg, D. Temporal Trends in the Prevalence, Treatment and Outcomes of Patients with Acute Coronary Syndrome at High Bleeding Risk. Diagnostics 2022, 12, 1784. https://doi.org/10.3390/diagnostics12081784
Arow Z, Ovdat T, Gabarin M, Omelchenko A, Shuvy M, Or T, Assali A, Pereg D. Temporal Trends in the Prevalence, Treatment and Outcomes of Patients with Acute Coronary Syndrome at High Bleeding Risk. Diagnostics. 2022; 12(8):1784. https://doi.org/10.3390/diagnostics12081784
Chicago/Turabian StyleArow, Ziad, Tal Ovdat, Mustafa Gabarin, Alexander Omelchenko, Mony Shuvy, Tsafrir Or, Abid Assali, and David Pereg. 2022. "Temporal Trends in the Prevalence, Treatment and Outcomes of Patients with Acute Coronary Syndrome at High Bleeding Risk" Diagnostics 12, no. 8: 1784. https://doi.org/10.3390/diagnostics12081784
APA StyleArow, Z., Ovdat, T., Gabarin, M., Omelchenko, A., Shuvy, M., Or, T., Assali, A., & Pereg, D. (2022). Temporal Trends in the Prevalence, Treatment and Outcomes of Patients with Acute Coronary Syndrome at High Bleeding Risk. Diagnostics, 12(8), 1784. https://doi.org/10.3390/diagnostics12081784