
Chronological Registration of OCT and Autofluorescence Findings in CSCR: Two Distinct Patterns in Disease Course

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Method
2.1. Materials
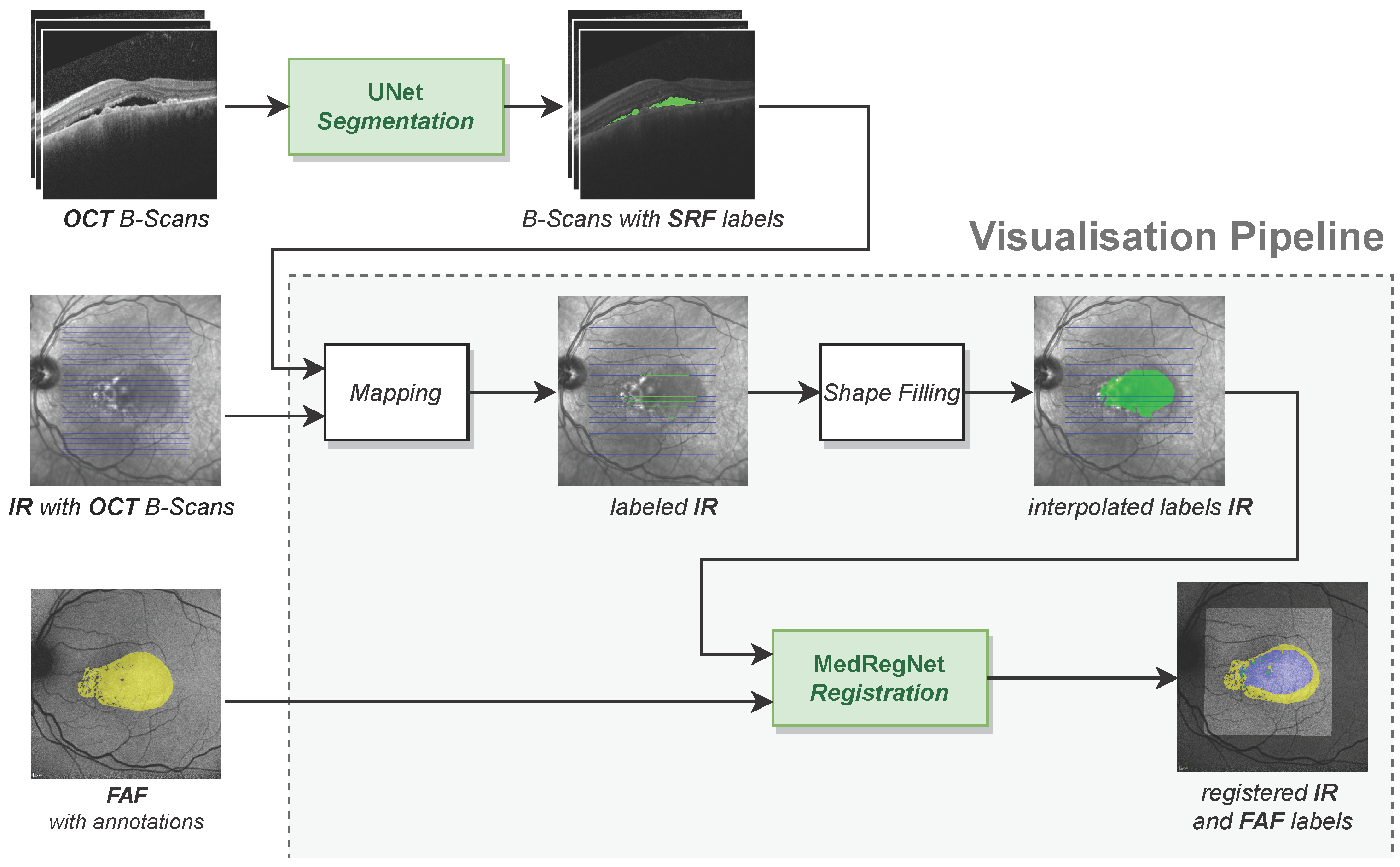
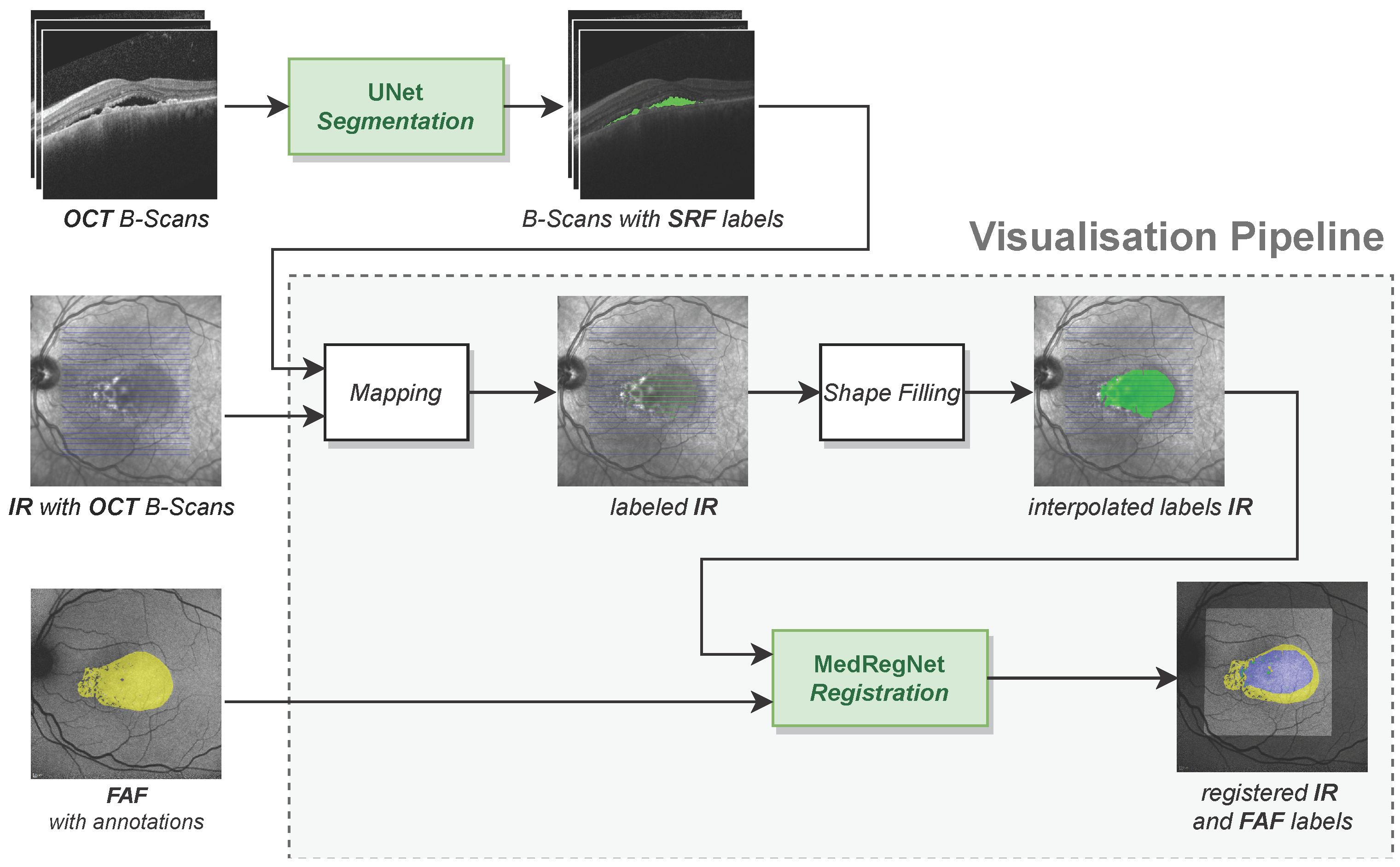
2.2. Technical Methods
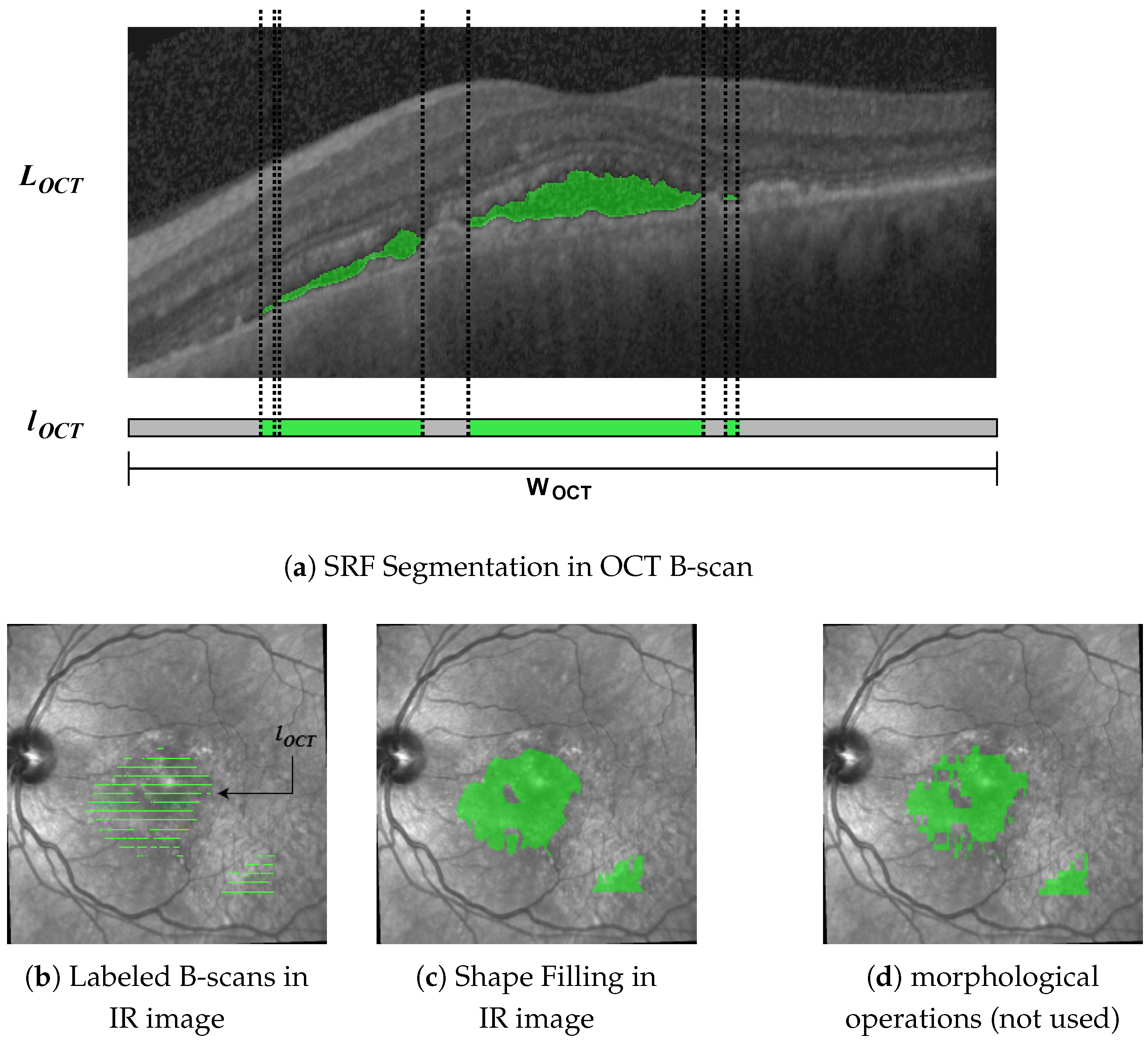
2.2.1. OCT Segmentation Network
2.2.2. OCT to IR Mapping
2.2.3. Shape Filling
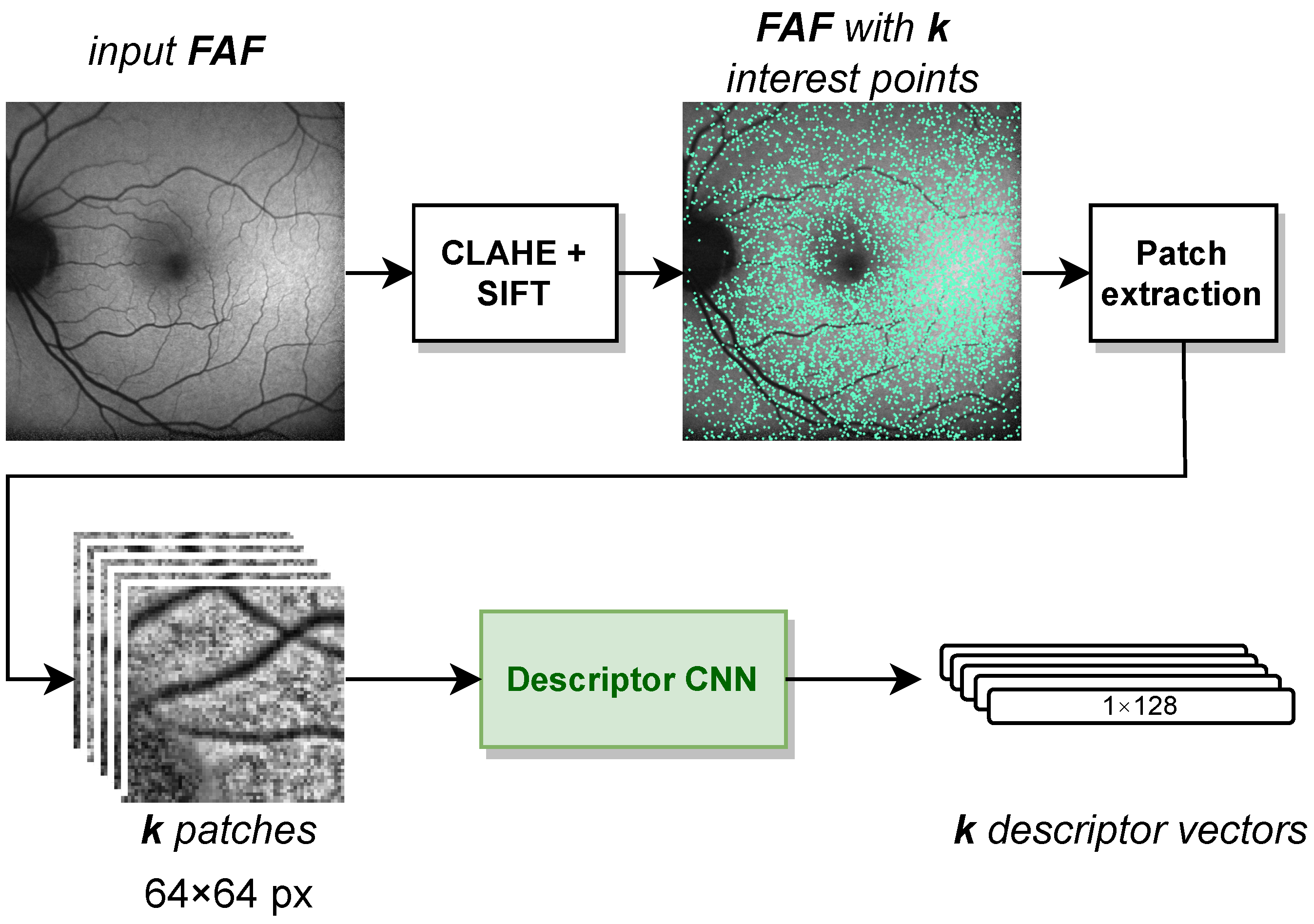
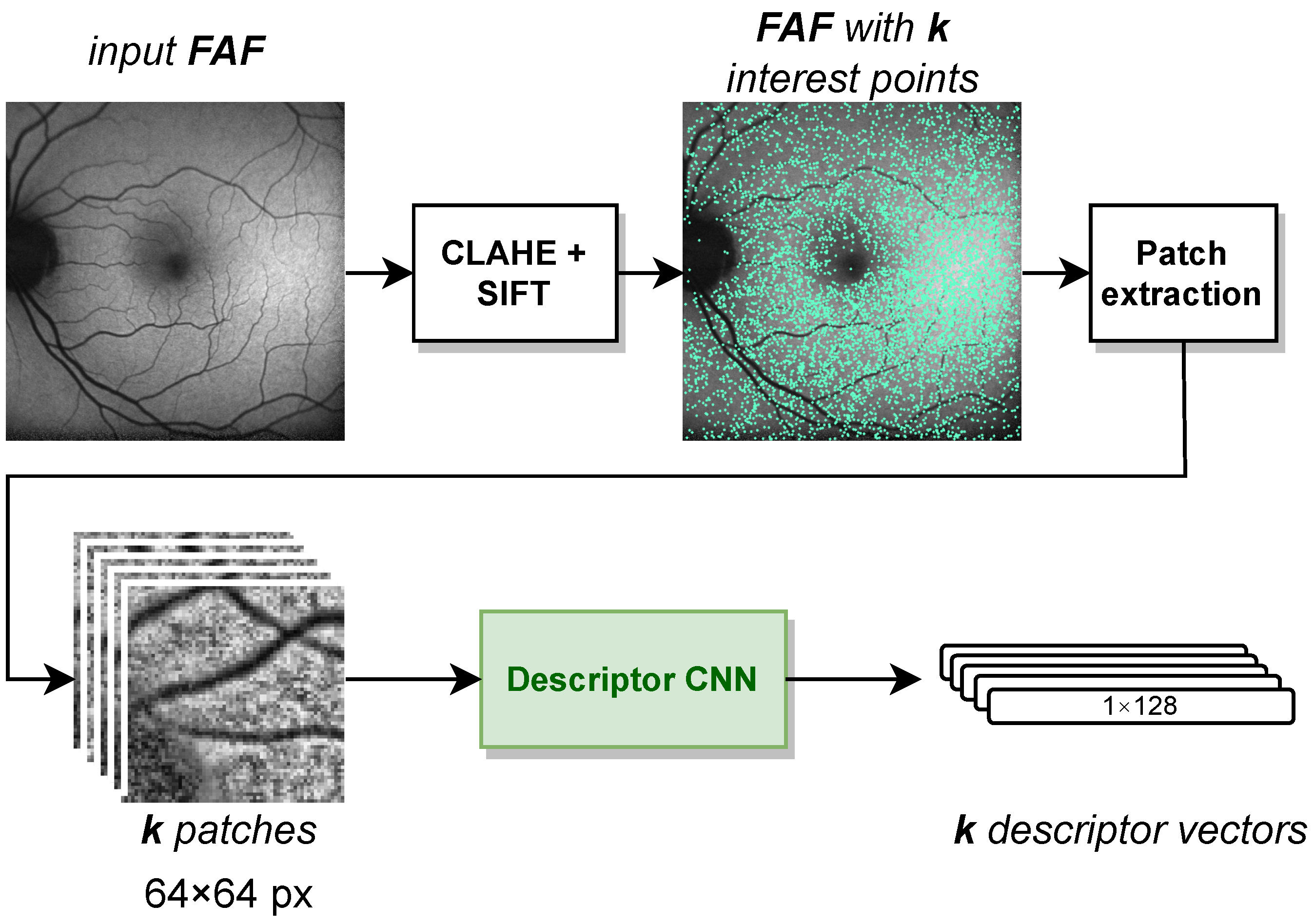
2.2.4. IR to FAF Registration
3. Technical Results
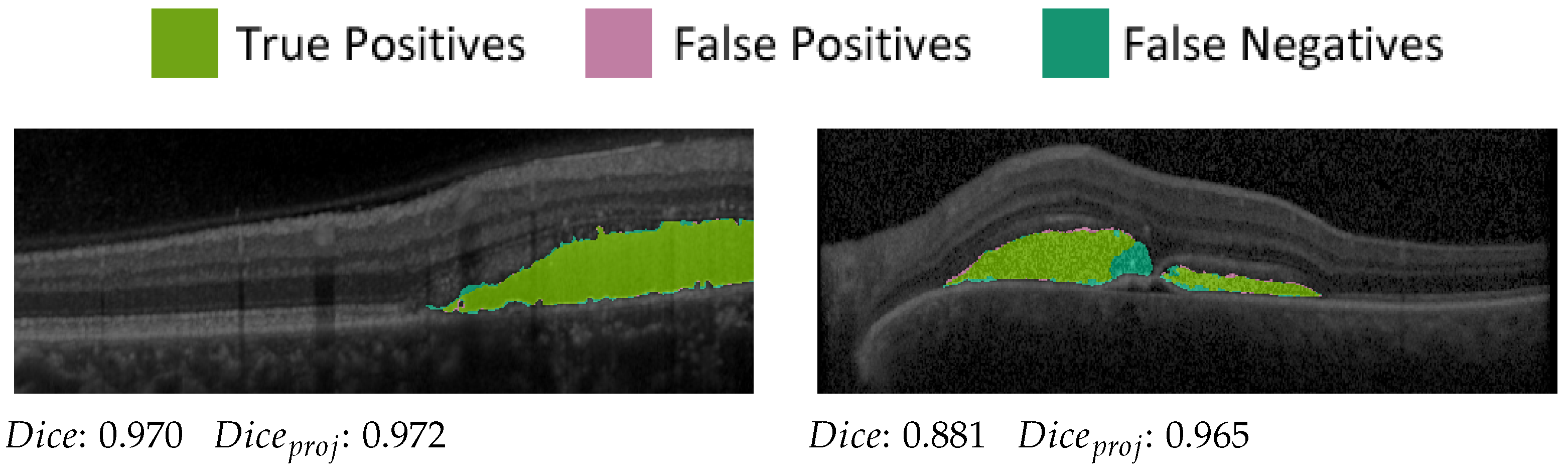
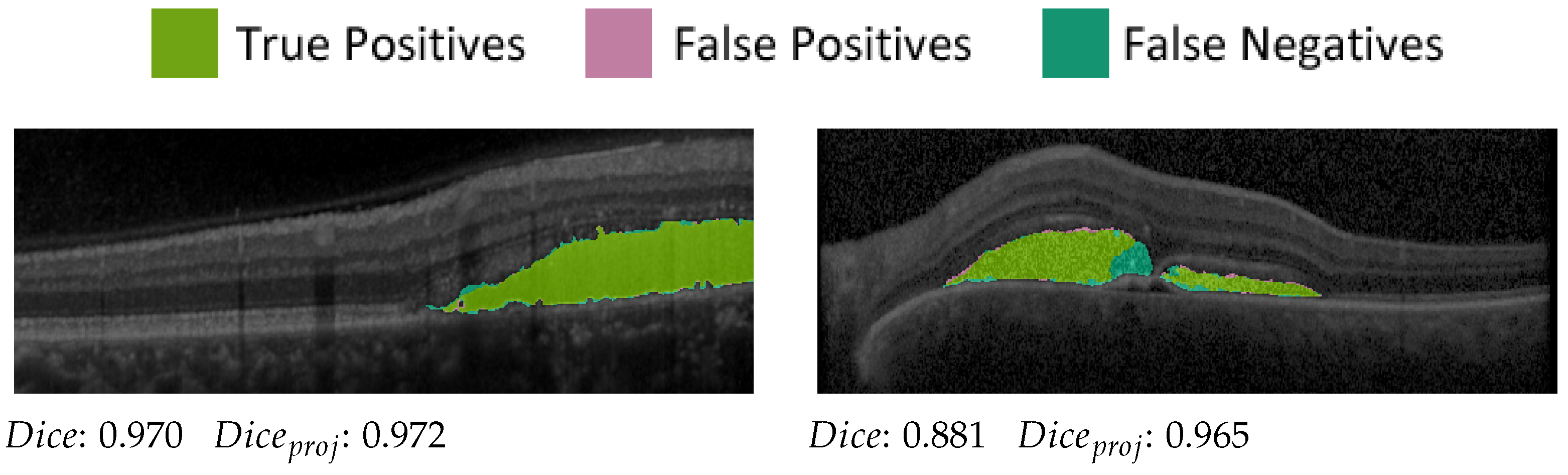
3.1. Segmentation Network
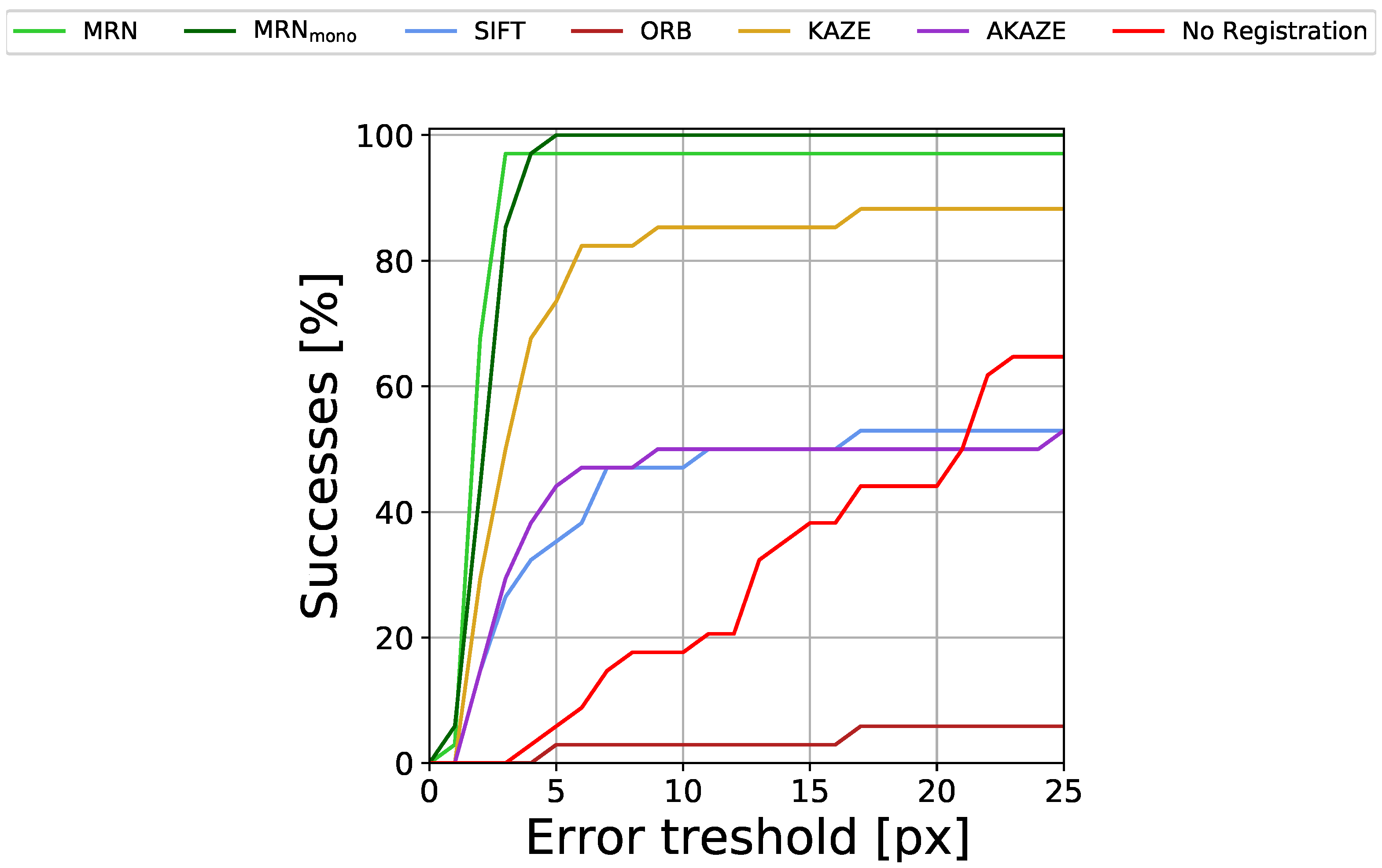
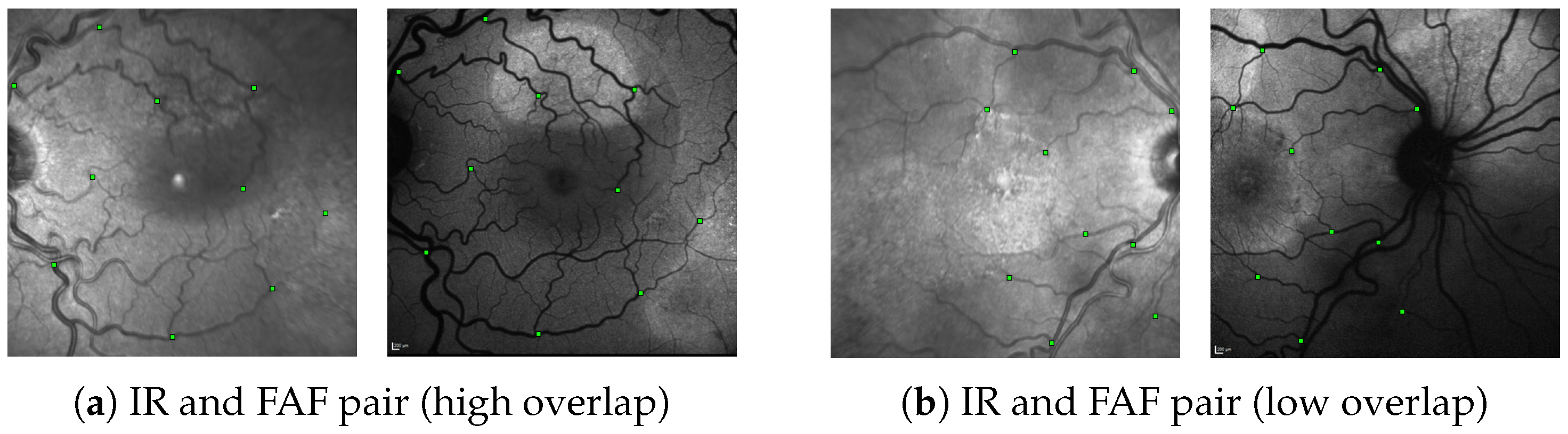
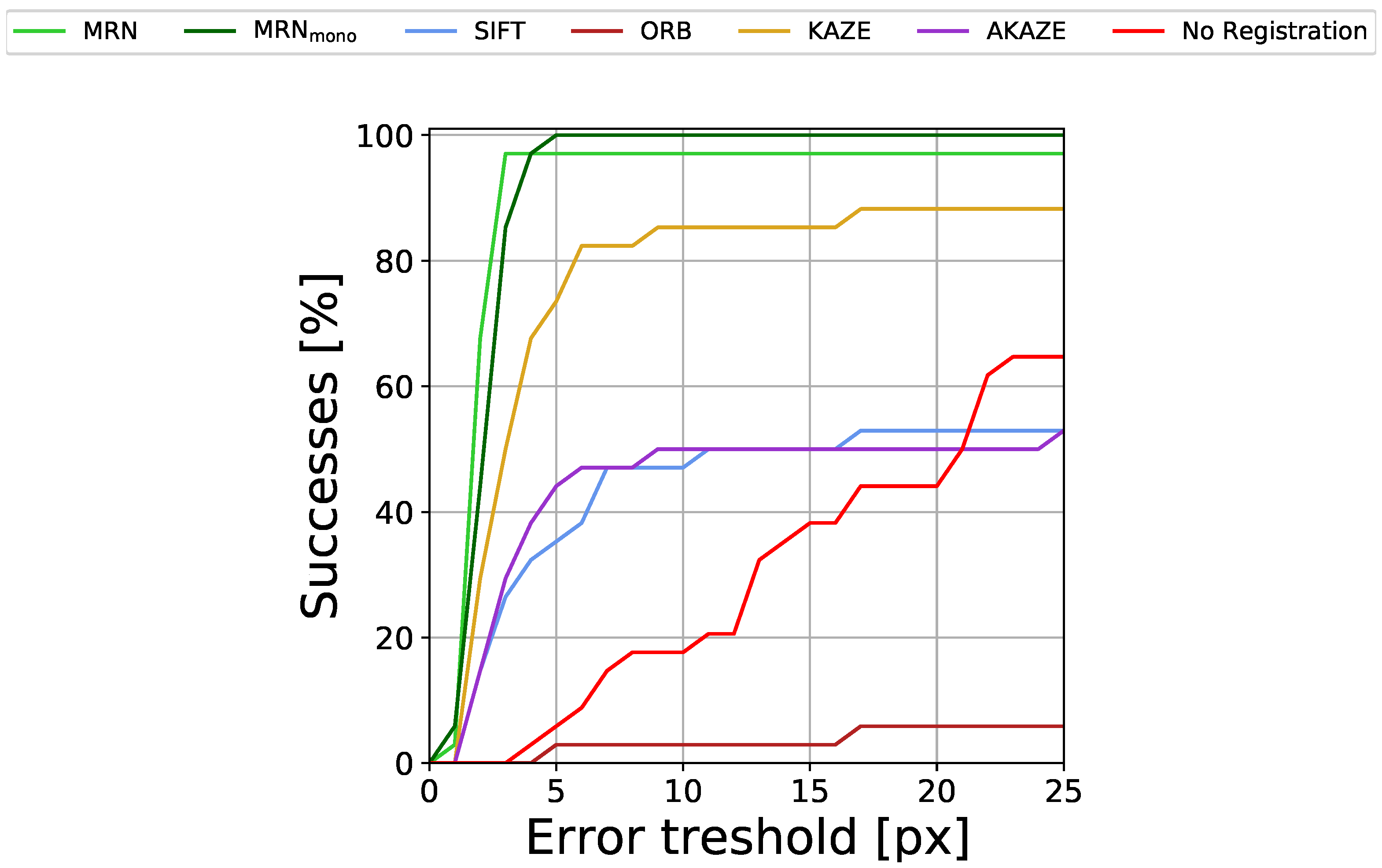
3.2. Registration Network
4. Technical Discussion
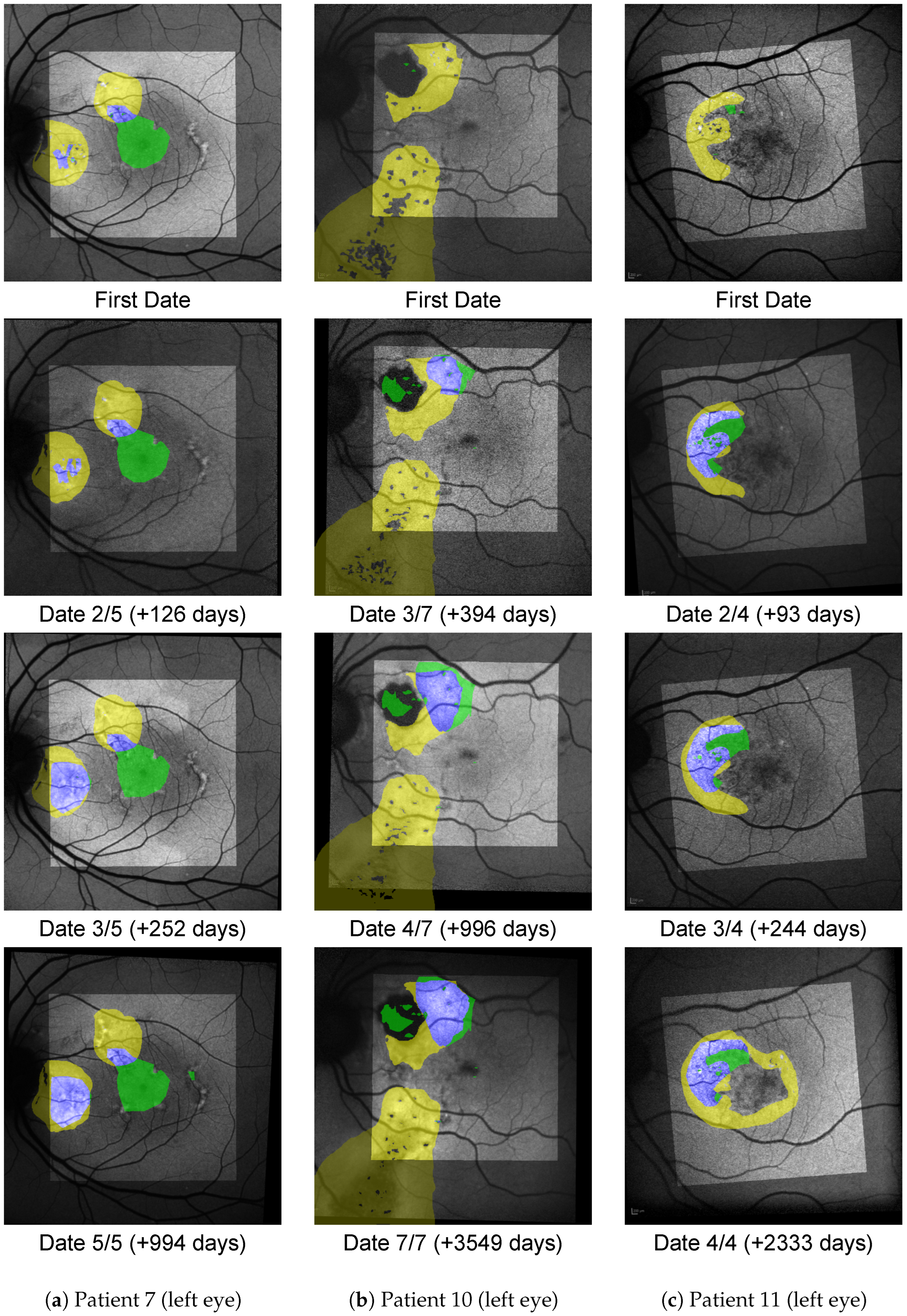
5. Medical Analysis
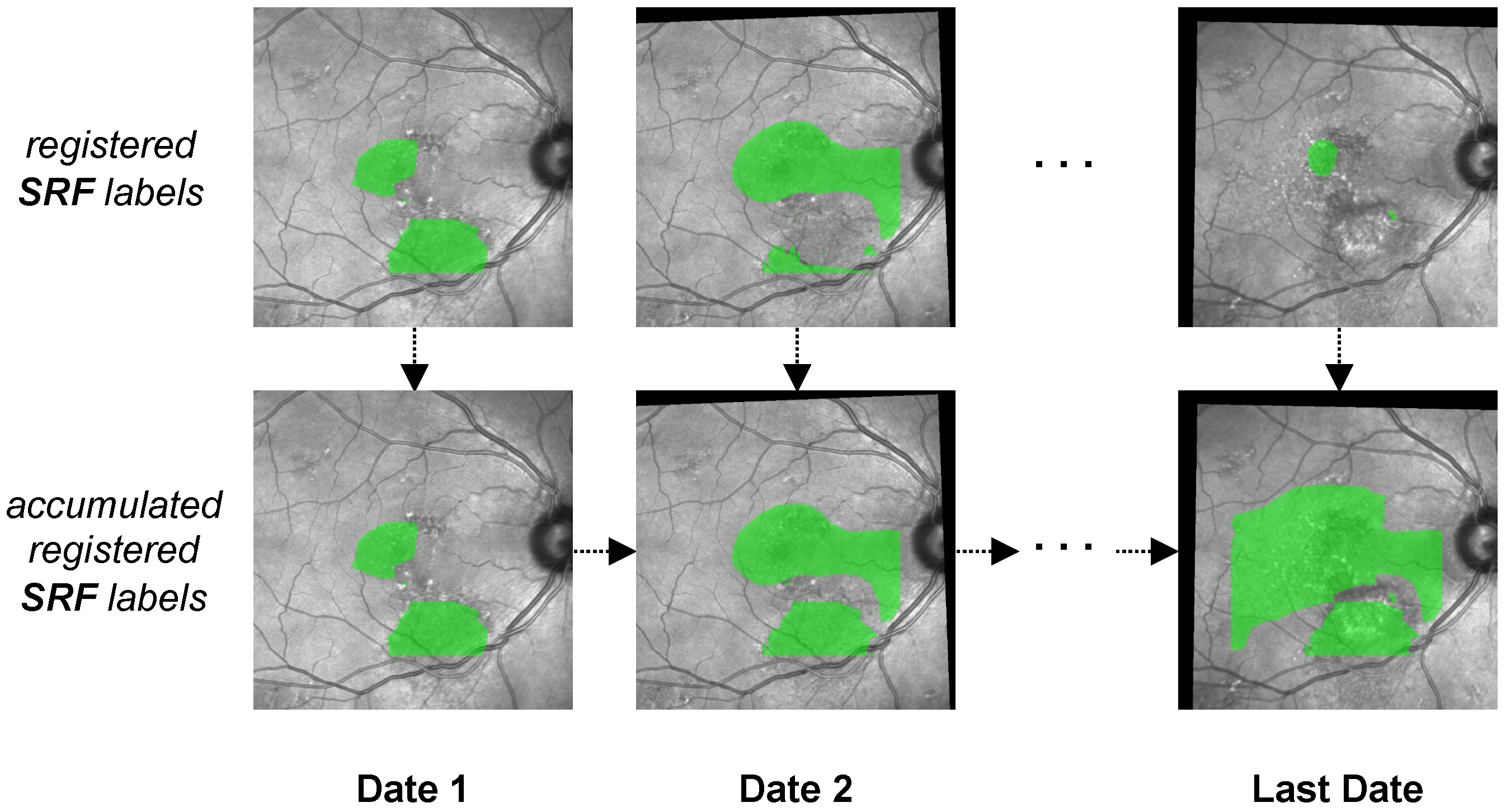
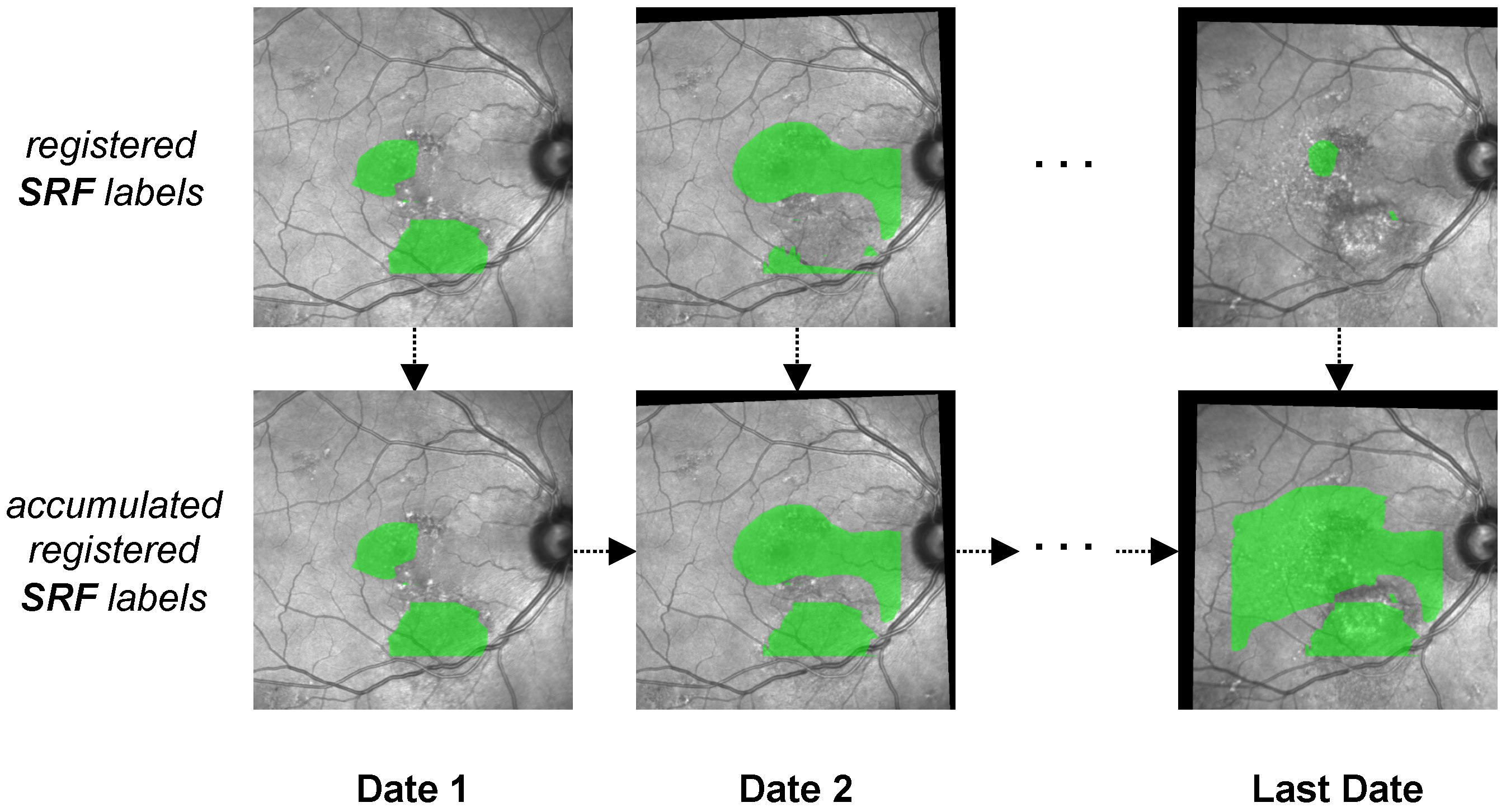
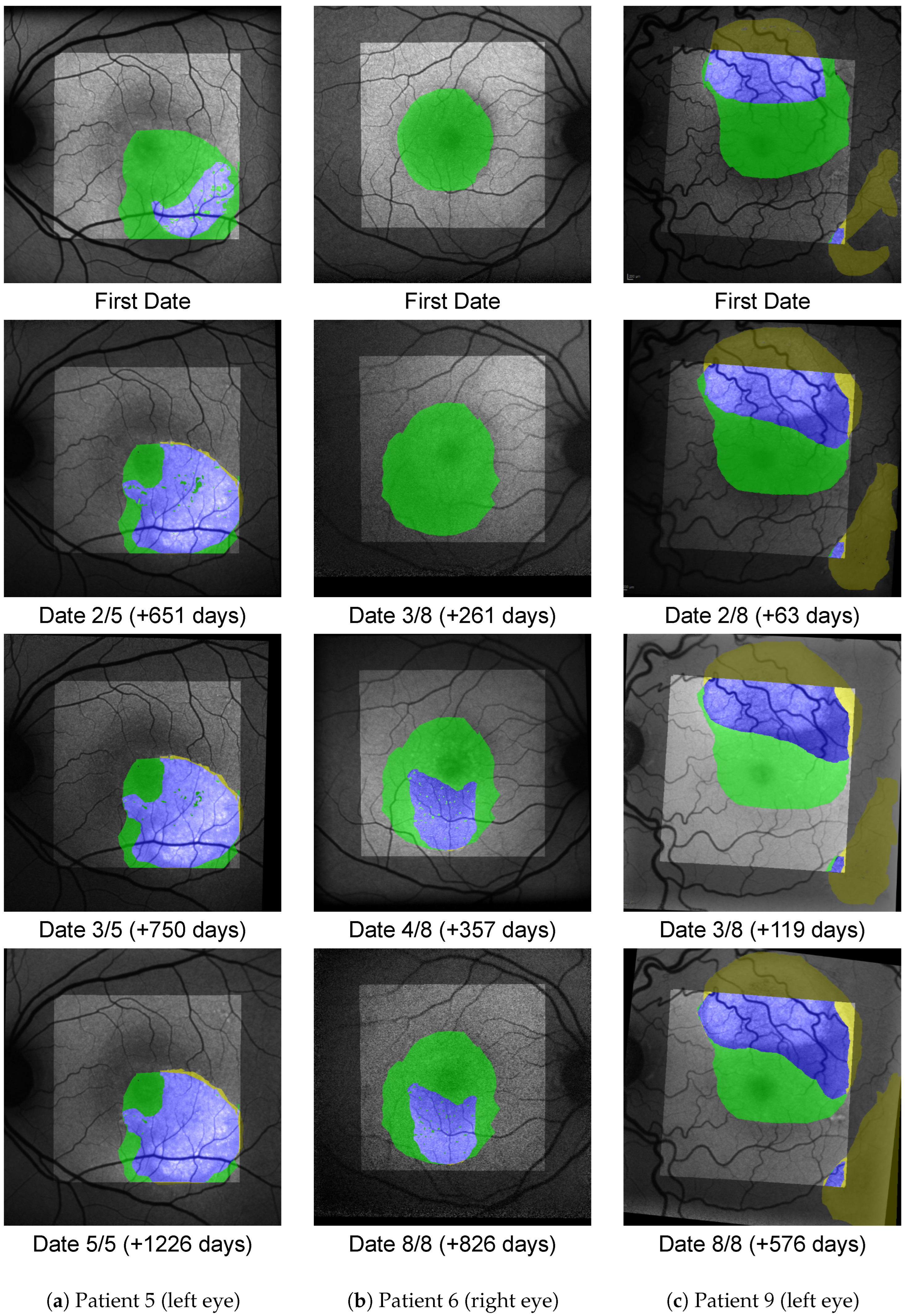
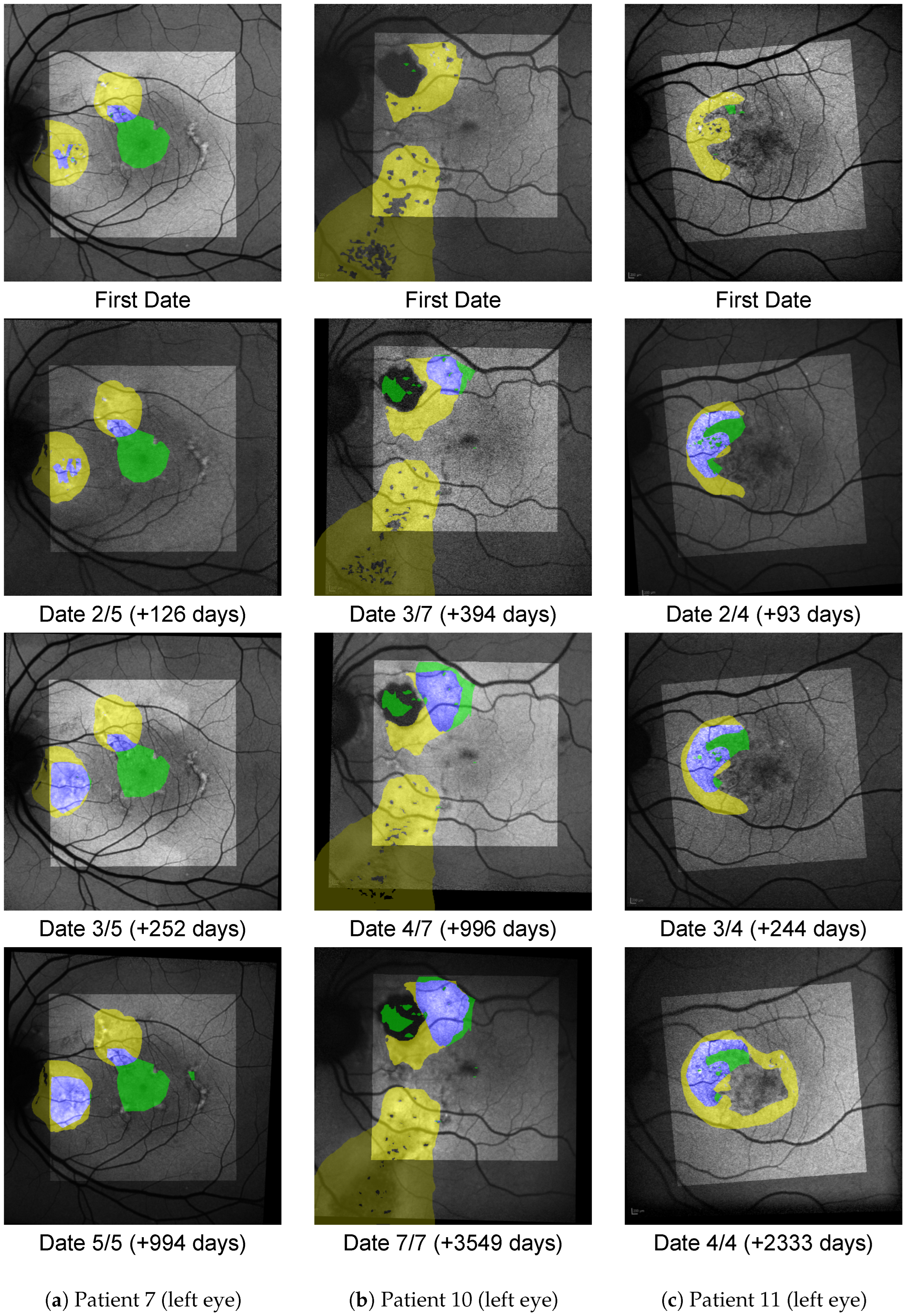
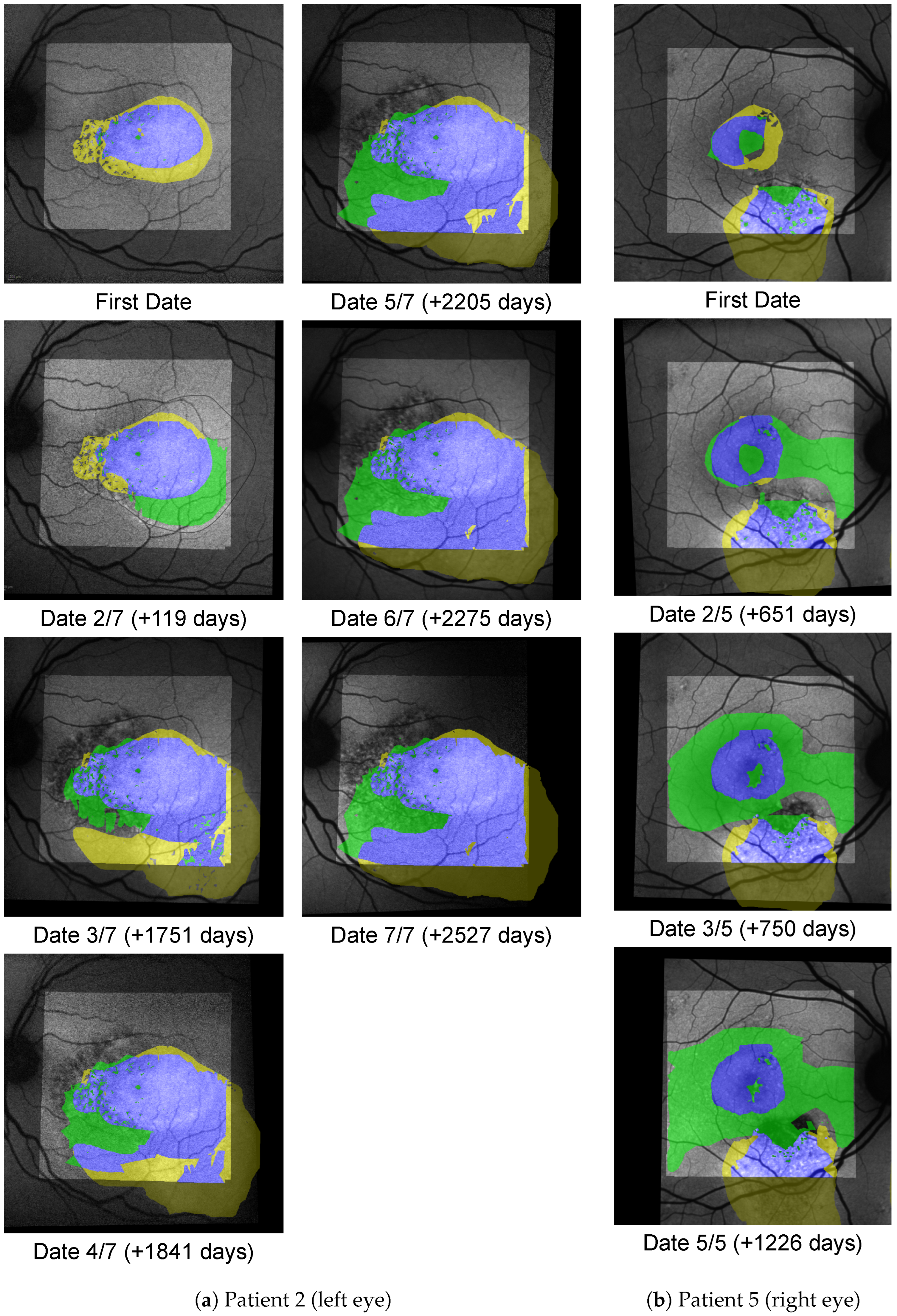
5.1. Visualisation Method
6. Medical Discussion
7. Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


References
- Manayath, G.J.; Ranjan, R.; Shah, V.S.; Karandikar, S.S.; Saravanan, V.R.; Narendran, V. Central serous chorioretinopathy: Current update on pathophysiology and multimodal imaging. Oman J. Ophthalmol. 2018, 11, 103. [Google Scholar] [PubMed]
- Spaide, R.F.; Campeas, L.; Haas, A.; Yannuzzi, L.A.; Fisher, Y.L.; Guyer, D.R.; Slakter, J.S.; Sorenson, J.A.; Orlock, D.A. Central serous chorioretinopathy in younger and older adults. Ophthalmology 1996, 103, 2070–2080. [Google Scholar] [CrossRef]
- Sekiryu, T.; Iida, T.; Maruko, I.; Saito, K.; Kondo, T. Infrared fundus autofluorescence and central serous chorioretinopathy. Investig. Ophthalmol. Vis. Sci. 2010, 51, 4956–4962. [Google Scholar] [CrossRef] [Green Version]
- Han, J.; Cho, N.S.; Kim, K.; Kim, E.S.; Kim, J.M.; Yu, S.Y. Fundus autofluorescence patterns in central serous chorioretinopathy. Retina 2020, 40, 1387. [Google Scholar] [CrossRef]
- Kitzmann, A.S.; Pulido, J.S.; Diehl, N.N.; Hodge, D.O.; Burke, J.P. The incidence of central serous chorioretinopathy in Olmsted County, Minnesota, 1980–2002. Ophthalmology 2008, 115, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Kido, A.; Miyake, M.; Tamura, H.; Hiragi, S.; Kimura, T.; Ohtera, S.; Takahashi, A.; Ooto, S.; Kawakami, K.; Kuroda, T.; et al. Incidence of central serous chorioretinopathy (2011–2018): A nationwide population-based cohort study of Japan. Br. J. Ophthalmol. 2021. [Google Scholar] [CrossRef]
- Rudnicka, A.R.; Kapetanakis, V.V.; Jarrar, Z.; Wathern, A.K.; Wormald, R.; Fletcher, A.E.; Cook, D.G.; Owen, C.G. Incidence of late-stage age-related macular degeneration in American whites: Systematic review and meta-analysis. Am. J. Ophthalmol. 2015, 160, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Santarossa, M.; Kilic, A.; von der Burchard, C.; Schmarje, L.; Zelenka, C.; Reinhold, S.; Koch, R.; Roider, J. MedRegNet: Unsupervised multimodal retinal-image registration with GANs and ranking loss. In Proceedings of the Medical Imaging 2022: Image Processing, San Diego, CA, USA, 20–24 February 2022; Volume 12032, pp. 321–333. [Google Scholar]
- Told, R.; Reiter, G.S.; Orsolya, A.; Mittermüller, T.J.; Eibenberger, K.; Schlanitz, F.G.; Arikan, M.; Pollreisz, A.; Sacu, S.; Schmidt-Erfurth, U. Swept source optical coherence tomography angiography, fluorescein angiography, and indocyanine green angiography comparisons revisited: Using a novel deep-learning-assisted approach for image registration. Retina 2020, 40, 2010–2017. [Google Scholar] [CrossRef]
- Noh, K.J.; Kim, J.; Park, S.J.; Lee, S. Multimodal registration of fundus images With fluorescein angiography for fine-scale vessel segmentation. IEEE Access 2020, 8, 63757–63769. [Google Scholar] [CrossRef]
- Luo, G.; Chen, X.; Shi, F.; Peng, Y.; Xiang, D.; Chen, Q.; Xu, X.; Zhu, W.; Fan, Y. Multimodal affine registration for ICGA and MCSL fundus images of high myopia. Biomed. Opt. Express 2020, 11, 4443–4457. [Google Scholar] [CrossRef]
- Lee, J.A.; Liu, P.; Cheng, J.; Fu, H. A deep step pattern representation for multimodal retinal image registration. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Seoul, Korea, 27 October–2 November 2019; pp. 5077–5086. [Google Scholar]
- Truong, P.; Apostolopoulos, S.; Mosinska, A.; Stucky, S.; Ciller, C.; Zanet, S.D. Glampoints: Greedily learned accurate match points. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Seoul, Korea, 27 October–2 November 2019; pp. 10732–10741. [Google Scholar]
- Hervella, Á.S.; Rouco, J.; Novo, J.; Ortega, M. Multimodal registration of retinal images using domain-specific landmarks and vessel enhancement. Procedia Comput. Sci. 2018, 126, 97–104. [Google Scholar] [CrossRef]
- Stewart, C.V.; Tsai, C.L.; Roysam, B. The dual-bootstrap iterative closest point algorithm with application to retinal image registration. IEEE Trans. Med. Imaging 2003, 22, 1379–1394. [Google Scholar] [CrossRef]
- Szeskin, A.; Yehuda, R.; Shmueli, O.; Levy, J.; Joskowicz, L. A column-based deep learning method for the detection and quantification of atrophy associated with AMD in OCT scans. Med. Image Anal. 2021, 72, 102130. [Google Scholar] [CrossRef] [PubMed]
- Tuerksever, C.; Pruente, C.; Hatz, K. High frequency SD-OCT follow-up leading to up to biweekly intravitreal ranibizumab treatment in neovascular age-related macular degeneration. Sci. Rep. 2021, 11, 1–10. [Google Scholar] [CrossRef]
- Vogl, W.D.; Waldstein, S.M.; Gerendas, B.S.; Schmidt-Erfurth, U.; Langs, G. Predicting macular edema recurrence from spatio-temporal signatures in optical coherence tomography images. IEEE Trans. Med. Imaging 2017, 36, 1773–1783. [Google Scholar] [CrossRef]
- Gorgi Zadeh, S.; Wintergerst, M.W.; Wiens, V.; Thiele, S.; Holz, F.G.; Finger, R.P.; Schultz, T. CNNs enable accurate and fast segmentation of drusen in optical coherence tomography. In Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support; Springer: Berlin/Heidelberg, Germany, 2017; pp. 65–73. [Google Scholar]
- Mokhtari, M.; Rabbani, H.; Mehri-Dehnavi, A. Alignment of optic nerve head optical coherence tomography B-scans in right and left eyes. In Proceedings of the 2017 IEEE International Conference on Image Processing (ICIP), Beijing, China, 17–20 September 2017; pp. 2279–2283. [Google Scholar]
- Padmasini, N.; Umamaheswari, R. Detection of neovascularisation using K-means clustering through registration of peripapillary OCT and fundus retinal images. In Proceedings of the 2016 IEEE International Conference on Computational Intelligence and Computing Research (ICCIC), Tamil Nadu, India, 15–17 December 2016; pp. 1–4. [Google Scholar]
- Niu, S.; Chen, Q.; Shen, H.; de Sisternes, L.; Rubin, D.L. Registration of SD-OCT en-face images with color fundus photographs based on local patch matching. In Ophthalmic Medical Image Analysis International Workshop; University of Iowa: Iowa City, IA, USA, 2014; pp. 25–32. [Google Scholar]
- Golabbakhsh, M.; Rabbani, H. Vessel-based registration of fundus and optical coherence tomography projection images of retina using a quadratic registration model. IET Image Process. 2013, 7, 768–776. [Google Scholar] [CrossRef]
- Golabbakhsh, M.; Rabbani, H.; Esmaeili, M. Detection and registration of vessels of fundus and OCT images using curevelet analysis. In Proceedings of the 2012 IEEE 12th International Conference on Bioinformatics & Bioengineering (BIBE), Larnaca, Cyprus, 11–13 November 2012; pp. 594–597. [Google Scholar]
- Li, Y.; Gregori, G.; Knighton, R.W.; Lujan, B.J.; Rosenfeld, P.J. Registration of OCT fundus images with color fundus photographs based on blood vessel ridges. Opt. Express 2011, 19, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Kolar, R.; Tasevsky, P. Registration of 3D retinal optical coherence tomography data and 2D fundus images. In International Workshop on Biomedical Image Registration; Springer: Berlin/Heidelberg, Germany, 2010; pp. 72–82. [Google Scholar]
- Golkar, E.; Rabbani, H.; Dehghani, A. Hybrid registration of retinal fluorescein angiography and optical coherence tomography images of patients with diabetic retinopathy. Biomed. Opt. Express 2021, 12, 1707–1724. [Google Scholar] [CrossRef]
- Almasi, R.; Vafaei, A.; Ghasemi, Z.; Ommani, M.R.; Dehghani, A.R.; Rabbani, H. Registration of fluorescein angiography and optical coherence tomography images of curved retina via scanning laser ophthalmoscopy photographs. Biomed. Opt. Express 2020, 11, 3455–3476. [Google Scholar] [CrossRef]
- Pan, L.; Chen, X. Retinal OCT Image Registration: Methods and Applications. IEEE Rev. Biomed. Eng. 2021. [Google Scholar] [CrossRef]
- Zola, M.; Chatziralli, I.; Menon, D.; Schwartz, R.; Hykin, P.; Sivaprasad, S. Evolution of fundus autofluorescence patterns over time in patients with chronic central serous chorioretinopathy. Acta Ophthalmol. 2018, 96, e835–e839. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Lee, J.; Lee, B. Fundus autofluorescence imaging patterns in central serous chorioretinopathy according to chronicity. Eye 2016, 30, 1336–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; Springer: Cham, Switerland, 2015; pp. 234–241. [Google Scholar]
- Siebert, H.; Hansen, L.; Heinrich, M.P. Learning a Metric for Multimodal Medical Image Registration without Supervision Based on Cycle Constraints. Sensors 2022, 22, 1107. [Google Scholar] [CrossRef] [PubMed]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Sudre, C.H.; Li, W.; Vercauteren, T.; Ourselin, S.; Jorge Cardoso, M. Generalised Dice Overlap as a Deep Learning Loss Function for Highly Unbalanced Segmentations. In Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support; Springer: Berlin/Heidelberg, Germany, 2017; pp. 240–248. [Google Scholar]
- Schenk, A.; Prause, G.; Peitgen, H.O. Efficient semiautomatic segmentation of 3D objects in medical images. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Pittsburgh, PA, USA, 11–14 October 2000; Springer: Berlin/Heidelberg, Germany, 2000; pp. 186–195. [Google Scholar]
- Lowe, D.G. Distinctive image features from scale-invariant keypoints. Int. J. Comput. Vis. 2004, 60, 91–110. [Google Scholar] [CrossRef]
- Fischler, M.A.; Bolles, R.C. Random sample consensus: A paradigm for model fitting with applications to image analysis and automated cartography. Commun. ACM 1981, 24, 381–395. [Google Scholar] [CrossRef]
- Cen, L.P.; Ji, J.; Lin, J.W.; Ju, S.T.; Lin, H.J.; Li, T.P.; Wang, Y.; Yang, J.F.; Liu, Y.F.; Tan, S.; et al. Automatic detection of 39 fundus diseases and conditions in retinal photographs using deep neural networks. Nat. Commun. 2021, 12, 1–13. [Google Scholar] [CrossRef]
- 1000 Fundus Images with 39 Categories V.4. Joint Shantou International Eye Centre (JSIEC). 2019. Available online: .https://www.kaggle.com/linchundan/fundusimage1000 (accessed on 6 December 2021).
- Pizer, S.M.; Amburn, E.P.; Austin, J.D.; Cromartie, R.; Geselowitz, A.; Greer, T.; ter Haar Romeny, B.; Zimmerman, J.B.; Zuiderveld, K. Adaptive histogram equalization and its variations. Comput. Vision Graph. Image Process. 1987, 39, 355–368. [Google Scholar] [CrossRef]
- Zijdenbos, A.P.; Dawant, B.M.; Margolin, R.A.; Palmer, A.C. Morphometric analysis of white matter lesions in MR images: Method and validation. IEEE Trans. Med. Imaging 1994, 13, 716–724. [Google Scholar] [CrossRef] [Green Version]
- Dice, L.R. Measures of the amount of ecologic association between species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Sorensen, T.A. A method of establishing groups of equal amplitude in plant sociology based on similarity of species content and its application to analyses of the vegetation on Danish commons. Biol. Skar. 1948, 5, 1–34. [Google Scholar]
- Hernandez-Matas, C.; Zabulis, X.; Triantafyllou, A.; Anyfanti, P.; Douma, S.; Argyros, A.A. FIRE: Fundus image registration dataset. Model. Artif. Intell. Ophthalmol. 2017, 1, 16–28. [Google Scholar] [CrossRef]
- Rublee, E.; Rabaud, V.; Konolige, K.; Bradski, G. ORB: An efficient alternative to SIFT or SURF. In Proceedings of the 2011 International Conference on Computer Vision, Barcelona, Spain, 6–13 November 2011; pp. 2564–2571. [Google Scholar]
- Alcantarilla, P.F.; Bartoli, A.; Davison, A.J. KAZE features. In Proceedings of the European Conference on Computer Vision, Florence, Italy, 7–13 October 2012; Springer: Berlin/Heidelberg, Germany, 2012; pp. 214–227. [Google Scholar]
- Alcantarilla, P.F.; Solutions, T. Fast explicit diffusion for accelerated features in nonlinear scale spaces. IEEE Trans. Patt. Anal. Mach. Intell 2011, 34, 1281–1298. [Google Scholar]
- Rao, T.N.; Girish, G.; Kothari, A.R.; Rajan, J. Deep learning based sub-retinal fluid segmentation in central serous chorioretinopathy optical coherence tomography scans. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 978–981. [Google Scholar]
- Hu, J.; Chen, Y.; Yi, Z. Automated segmentation of macular edema in OCT using deep neural networks. Med. Image Anal. 2019, 55, 216–227. [Google Scholar] [CrossRef]
- Bogunović, H.; Venhuizen, F.; Klimscha, S.; Apostolopoulos, S.; Bab-Hadiashar, A.; Bagci, U.; Beg, M.F.; Bekalo, L.; Chen, Q.; Ciller, C.; et al. RETOUCH: The retinal OCT fluid detection and segmentation benchmark and challenge. IEEE Trans. Med. Imaging 2019, 38, 1858–1874. [Google Scholar] [CrossRef]
- Sappa, L.B.; Okuwobi, I.P.; Li, M.; Zhang, Y.; Xie, S.; Yuan, S.; Chen, Q. RetFluidNet: Retinal Fluid Segmentation for SD-OCT Images Using Convolutional Neural Network. J. Digit. Imaging 2021, 34, 691–704. [Google Scholar] [CrossRef]
- Ehlers, J.P.; Wang, K.; Vasanji, A.; Hu, M.; Srivastava, S.K. Automated quantitative characterisation of retinal vascular leakage and microaneurysms in ultra-widefield fluorescein angiography. Br. J. Ophthalmol. 2017, 101, 696–699. [Google Scholar] [CrossRef]
- Zhou, C.; Zhang, T.; Wen, Y.; Chen, L.; Zhang, L.; Chen, J. Cross-Modal Guidance for Hyperfluorescence Segmentation in Fundus Fluorescein Angiography. In Proceedings of the 2021 IEEE International Conference on Multimedia and Expo (ICME), Shenzhen, China, 5–9 July 2021; pp. 1–6. [Google Scholar]
- Li, W.; Fang, W.; Wang, J.; He, Y.; Deng, G.; Ye, H.; Hou, Z.; Chen, Y.; Jiang, C.; Shi, G. A Weakly Supervised Deep Learning Approach for Leakage Detection in Fluorescein Angiography Images. Transl. Vis. Sci. Technol. 2022, 11, 9. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Used in | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 |
| seg. train | . | ✓ | ✓ | . | . | . | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | . | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| seg. eval | ✓ | . | . | ✓ | ✓ | ✓ | . | . | . | . | . | . | ✓ | . | . | . | . | . | . | . | . |
| reg. train | . | ✓ | . | ✓ | ✓ | . | . | . | . | . | ✓ | ✓ | . | . | . | . | ✓ | . | ✓ | . | . |
| reg. eval | . | . | ✓ | . | . | ✓ | ✓ | ✓ | ✓ | ✓ | . | . | . | . | ✓ | ✓ | . | ✓ | . | . | . |
| SRF prediction | . | . | . | . | . | . | ✓ | . | ✓ | . | . | . | . | . | . | . | . | . | . | . | . |
| med. analysis | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | . | . | . | . | . | . | . | . | . |
| Method | TP Matches | AuC | |
|---|---|---|---|
| MRN | 1715 | (34%) | 0.902 |
| MRN | 606 | (13%) | 0.913 |
| SIFT | 55 | (1%) | 0.434 |
| ORB | 29 | (0.3%) | 0.034 |
| KAZE | 205 | (8%) | 0.760 |
| AKAZE | 60 | (3%) | 0.438 |
| No registration | - | 0.288 | |
| Patient ID and Eye | Follow Up Time (Years) | Area of HF/SRF Overlap | Area Where SRF Precedes | Area Where HF Precedes | Area Where Chronology Is Unknown | Last VA (logMAR) |
|---|---|---|---|---|---|---|
| Pattern A: SRF Precedes | ||||||
| 5 L | 3.3 | 68k px | 67% | 0% | 33% | 0.1 |
| 6 R | 2.3 | 30k px | 100% | 0% | 0% | 0.6 |
| 8 L | 2.5 | 11k px | 98% | 0% | 2% | 0 |
| 9 L | 6.4 | 74k px | 40% | 1% | 59% | 0 |
| 11 R | 6.4 | 39k px | 100% | 0% | 0% | 0 |
| Pattern B: HF Precedes | ||||||
| 1 R | 2.6 | 105k px | 50% | 41% | 9% | 0.4 |
| 3 R | 7.6 | 0.4k px | 1% | 46% | 53% | −0.1 |
| 4 L | 6.0 | 74k px | 37% | 63% | 0% | 0.2 |
| 7 L | 2.7 | 16k px | 5% | 71% | 24% | 0.1 |
| 9 R | 6.4 | 76k px | 28% | 52% | 20% | 0.9 |
| 10 L | 9.7 | 20k px | 24% | 74% | 1% | 0.4 |
| 10 R | 9.7 | 81k px | 6% | 73% | 21% | 0.2 |
| 11 L | 6.4 | 15k px | 14% | 82% | 4% | 0.2 |
| 12 L | 7.5 | 31k px | 1% | 72% | 27% | 0.2 |
| Excluded: No chronological order | ||||||
| 1 L | 2.6 | 85k px | 4% | 19% | 77% | 0.2 |
| 2 L | 7.9 | 132k px | 20% | 44% | 36% | 0.8 |
| 5 R | 3.3 | 55k px | 11% | 21% | 68% | 1.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santarossa, M.; Tatli, A.; von der Burchard, C.; Andresen, J.; Roider, J.; Handels, H.; Koch, R. Chronological Registration of OCT and Autofluorescence Findings in CSCR: Two Distinct Patterns in Disease Course. Diagnostics 2022, 12, 1780. https://doi.org/10.3390/diagnostics12081780
Santarossa M, Tatli A, von der Burchard C, Andresen J, Roider J, Handels H, Koch R. Chronological Registration of OCT and Autofluorescence Findings in CSCR: Two Distinct Patterns in Disease Course. Diagnostics. 2022; 12(8):1780. https://doi.org/10.3390/diagnostics12081780
Chicago/Turabian StyleSantarossa, Monty, Ayse Tatli, Claus von der Burchard, Julia Andresen, Johann Roider, Heinz Handels, and Reinhard Koch. 2022. "Chronological Registration of OCT and Autofluorescence Findings in CSCR: Two Distinct Patterns in Disease Course" Diagnostics 12, no. 8: 1780. https://doi.org/10.3390/diagnostics12081780
APA StyleSantarossa, M., Tatli, A., von der Burchard, C., Andresen, J., Roider, J., Handels, H., & Koch, R. (2022). Chronological Registration of OCT and Autofluorescence Findings in CSCR: Two Distinct Patterns in Disease Course. Diagnostics, 12(8), 1780. https://doi.org/10.3390/diagnostics12081780