
Coexistence of Cor Triatriatum Sinister, Fibroelastoma and Pulmonary Veins Ostial Anatomy Variant as Incidental Findings in Coronary Computed Tomography Angiography




Abstract
:Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Loeffler, E. Unusual Malformation of the Left Atrium; Pulmonary Sinus. Arch. Pathol. 1949, 48, 371–376. [Google Scholar]
- Lam, C.R.; Green, E.; Drake, E. Diagnosis and Surgical Correction of 2 Types of Triatrial Heart. Surgery 1962, 51, 127–137. [Google Scholar] [PubMed]
- Marín-García, J.; Tandon, R.; Lucas, R.V.; Edwards, J.E. Cor Triatriatum: Study of 20 Cases. Am. J. Cardiol. 1975, 35, 59–66. [Google Scholar] [CrossRef]
- Abdel Razek, A.; Al-Marsafawy, H.; Elmansy, M.; El-Latif, M.A.; Sobh, D. Computed Tomography Angiography and Magnetic Resonance Angiography of Congenital Anomalies of Pulmonary Veins. J. Comput. Assist. Tomogr. 2019, 43, 399–405. [Google Scholar] [CrossRef]
- Alphonso, N.; Nørgaard, M.A.; Newcomb, A.; d’Udekem, Y.; Brizard, C.P.; Cochrane, A. Cor Triatriatum: Presentation, Diagnosis and Long-Term Surgical Results. Ann. Thorac. Surg. 2005, 80, 1666–1671. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
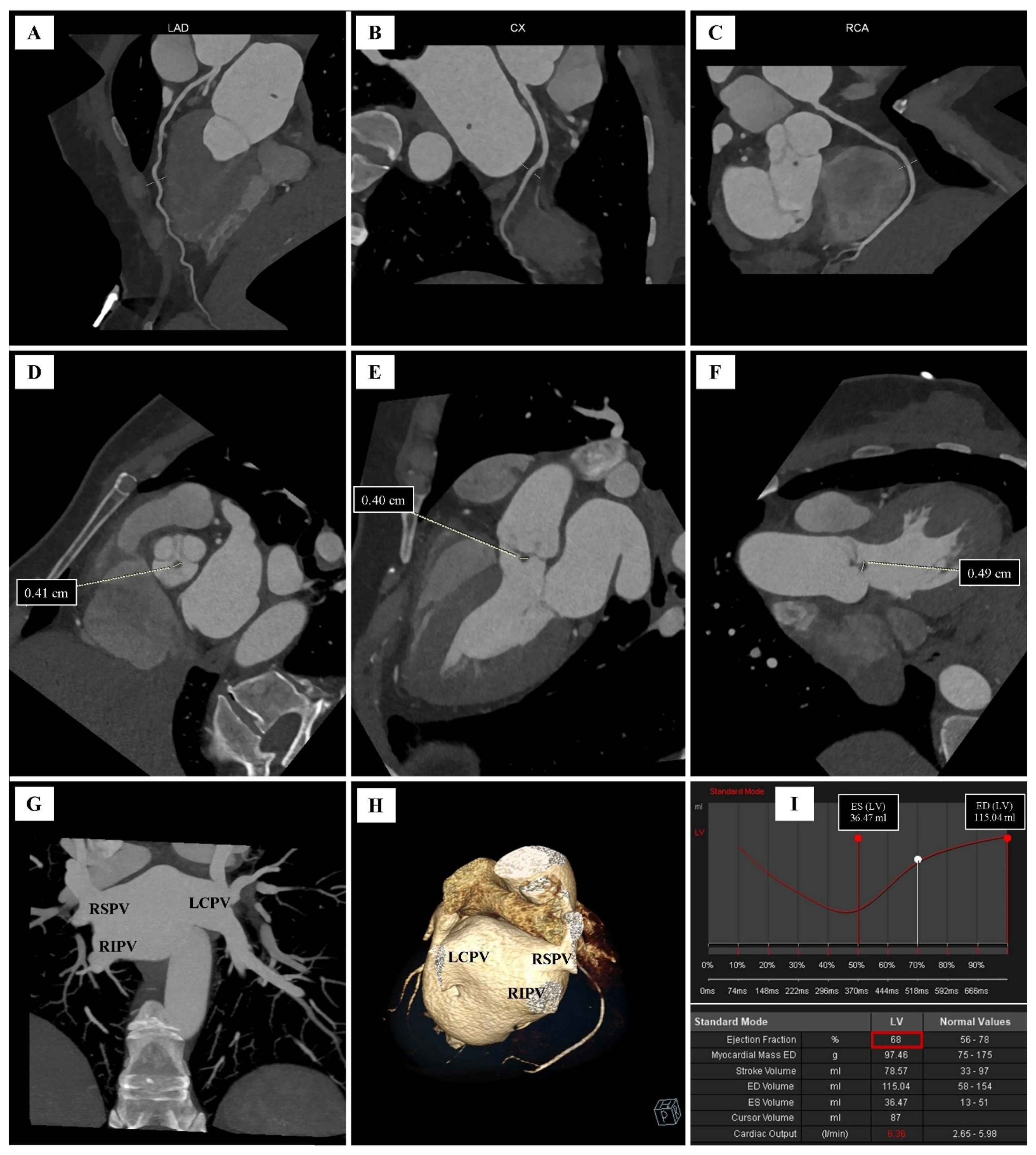
| Parameter | Value |
|---|---|
| Left ventricular mass (LVM) | 97.46 g |
| End-diastolic volume (EDV) | 115.04 mL |
| End-systolic volume (ESV) | 36.47 mL |
| Stroke volume (SV) | 78.57 mL |
| Ejection fraction (EF) | 68% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gać, P.; Martuszewski, A.; Paluszkiewicz, P.; Poręba, R. Coexistence of Cor Triatriatum Sinister, Fibroelastoma and Pulmonary Veins Ostial Anatomy Variant as Incidental Findings in Coronary Computed Tomography Angiography. Diagnostics 2022, 12, 1449. https://doi.org/10.3390/diagnostics12061449
Gać P, Martuszewski A, Paluszkiewicz P, Poręba R. Coexistence of Cor Triatriatum Sinister, Fibroelastoma and Pulmonary Veins Ostial Anatomy Variant as Incidental Findings in Coronary Computed Tomography Angiography. Diagnostics. 2022; 12(6):1449. https://doi.org/10.3390/diagnostics12061449
Chicago/Turabian StyleGać, Paweł, Adrian Martuszewski, Patrycja Paluszkiewicz, and Rafał Poręba. 2022. "Coexistence of Cor Triatriatum Sinister, Fibroelastoma and Pulmonary Veins Ostial Anatomy Variant as Incidental Findings in Coronary Computed Tomography Angiography" Diagnostics 12, no. 6: 1449. https://doi.org/10.3390/diagnostics12061449
APA StyleGać, P., Martuszewski, A., Paluszkiewicz, P., & Poręba, R. (2022). Coexistence of Cor Triatriatum Sinister, Fibroelastoma and Pulmonary Veins Ostial Anatomy Variant as Incidental Findings in Coronary Computed Tomography Angiography. Diagnostics, 12(6), 1449. https://doi.org/10.3390/diagnostics12061449