
NTRK Fusions in 1113 Solid Tumors in a Single Institution

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Selection
2.2. Tissue Microarrays (TMA)
2.3. IHC Assay
2.4. NGS Analysis
3. Results
3.1. Prevalence of NTRK Fusions in 1113 Solid Tumors
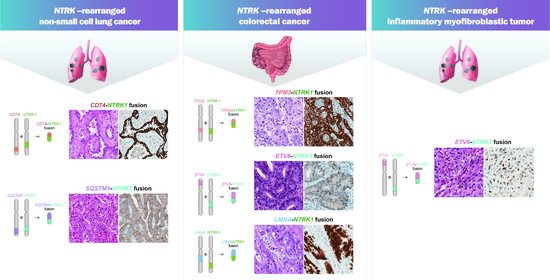
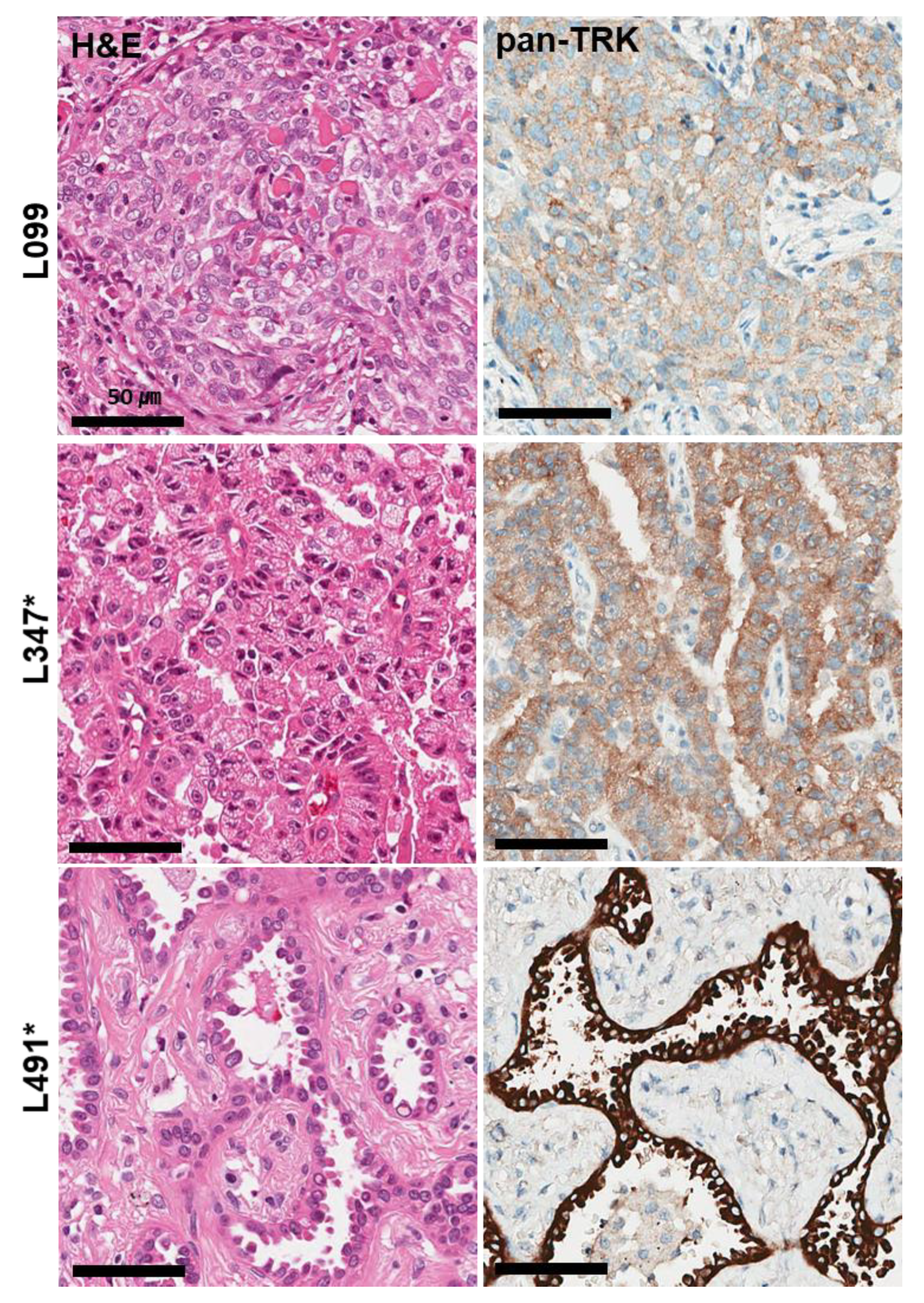
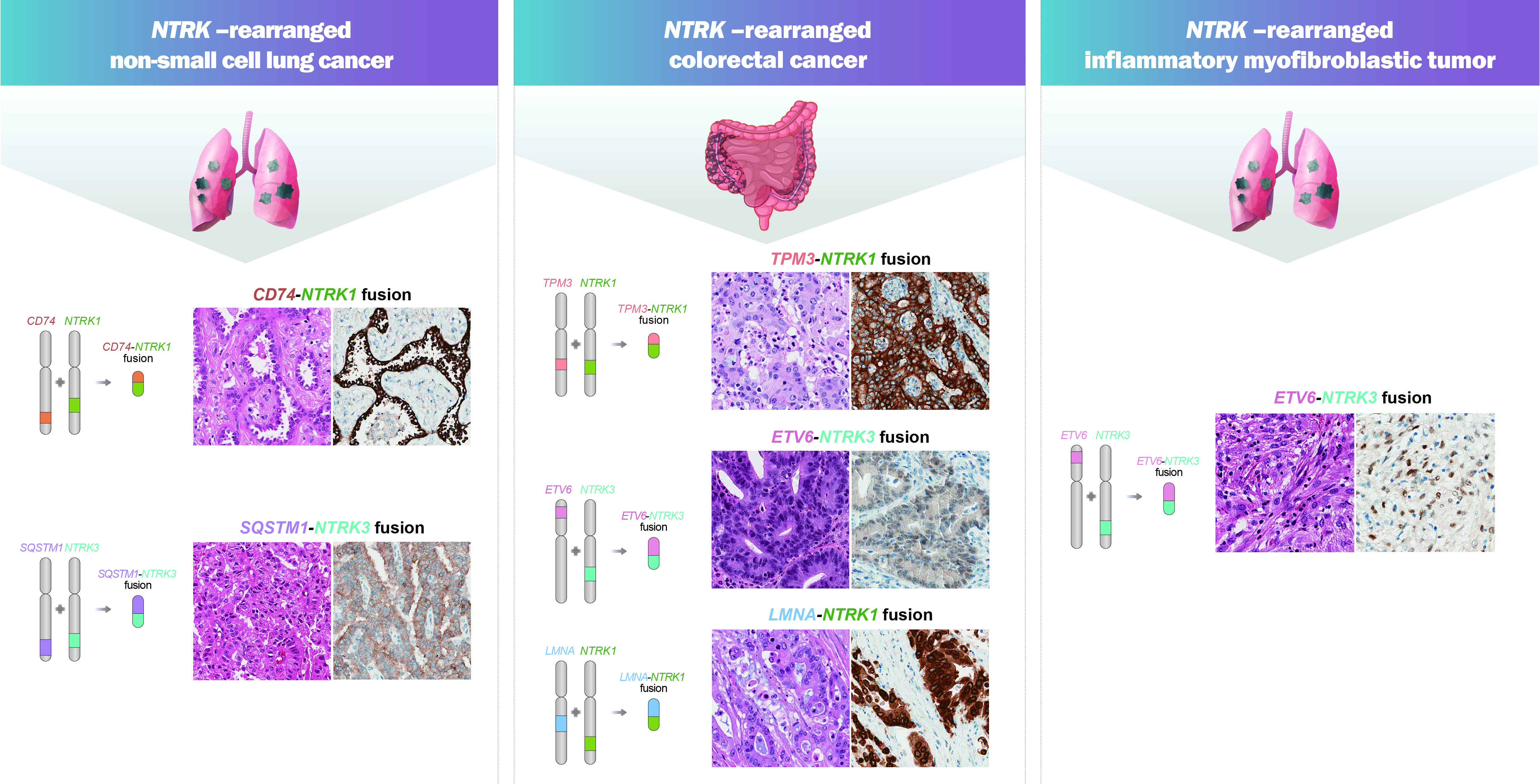
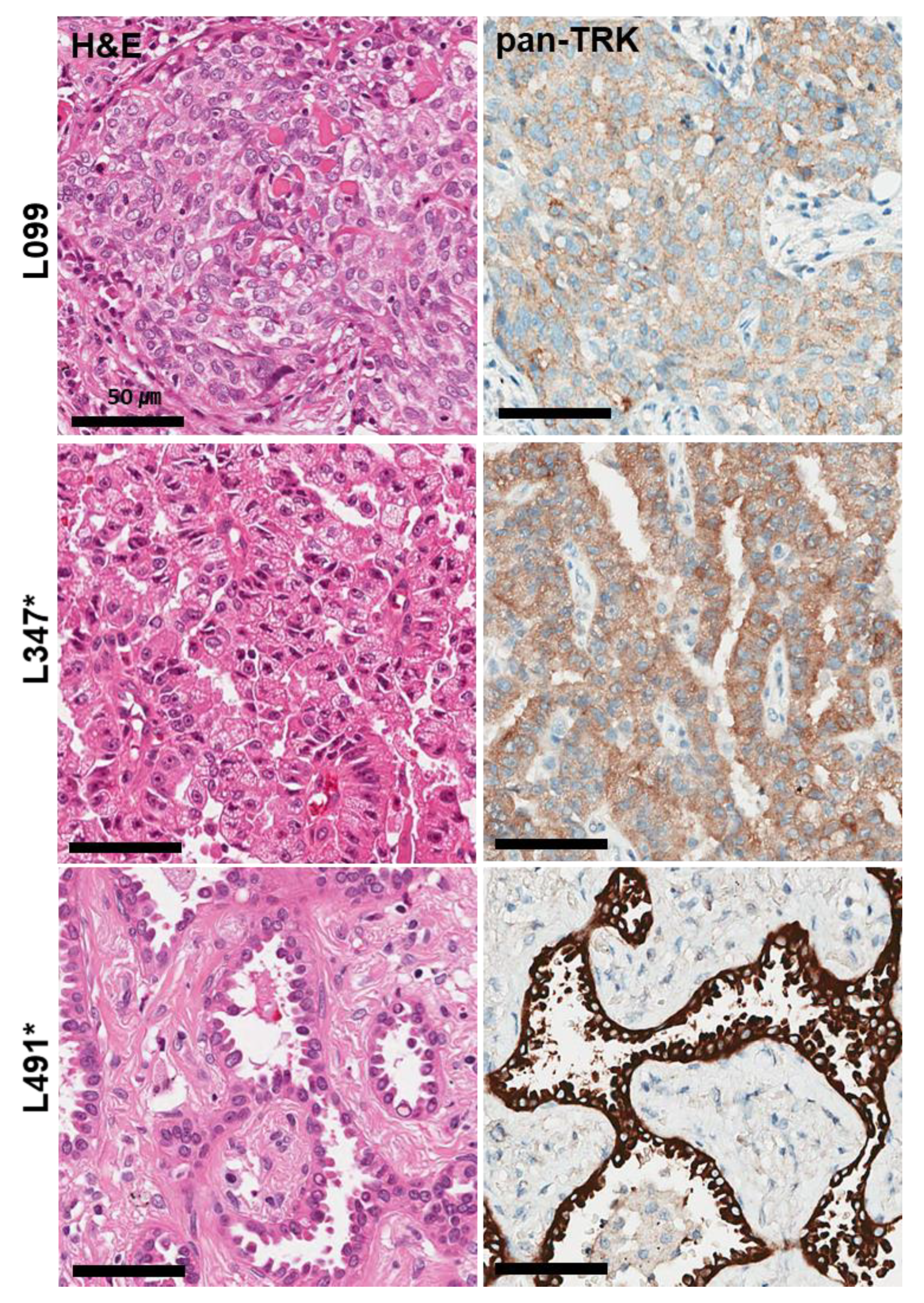
3.2. Non-Small Cell Lung Cancer
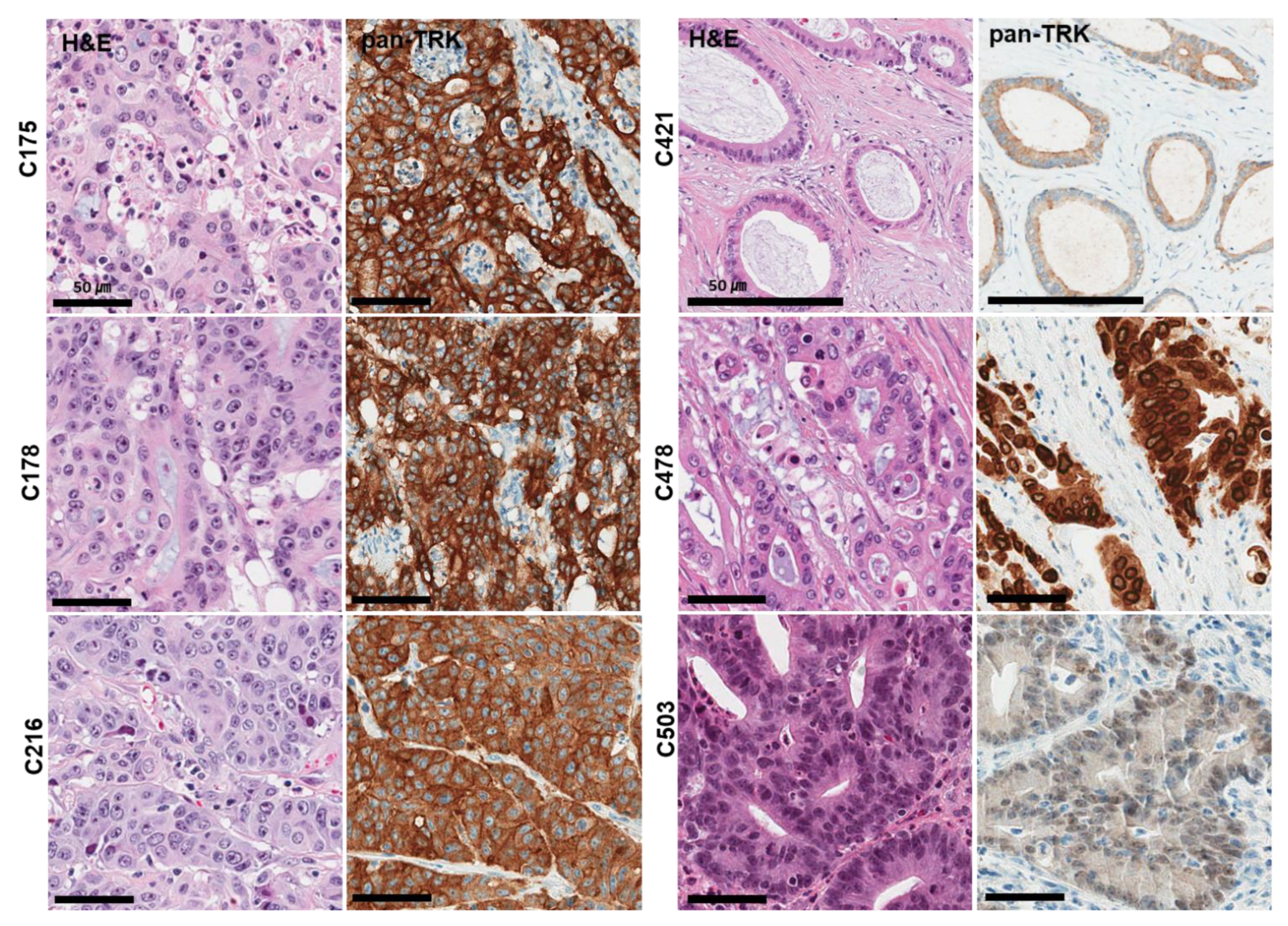
3.3. Colorectal Cancer
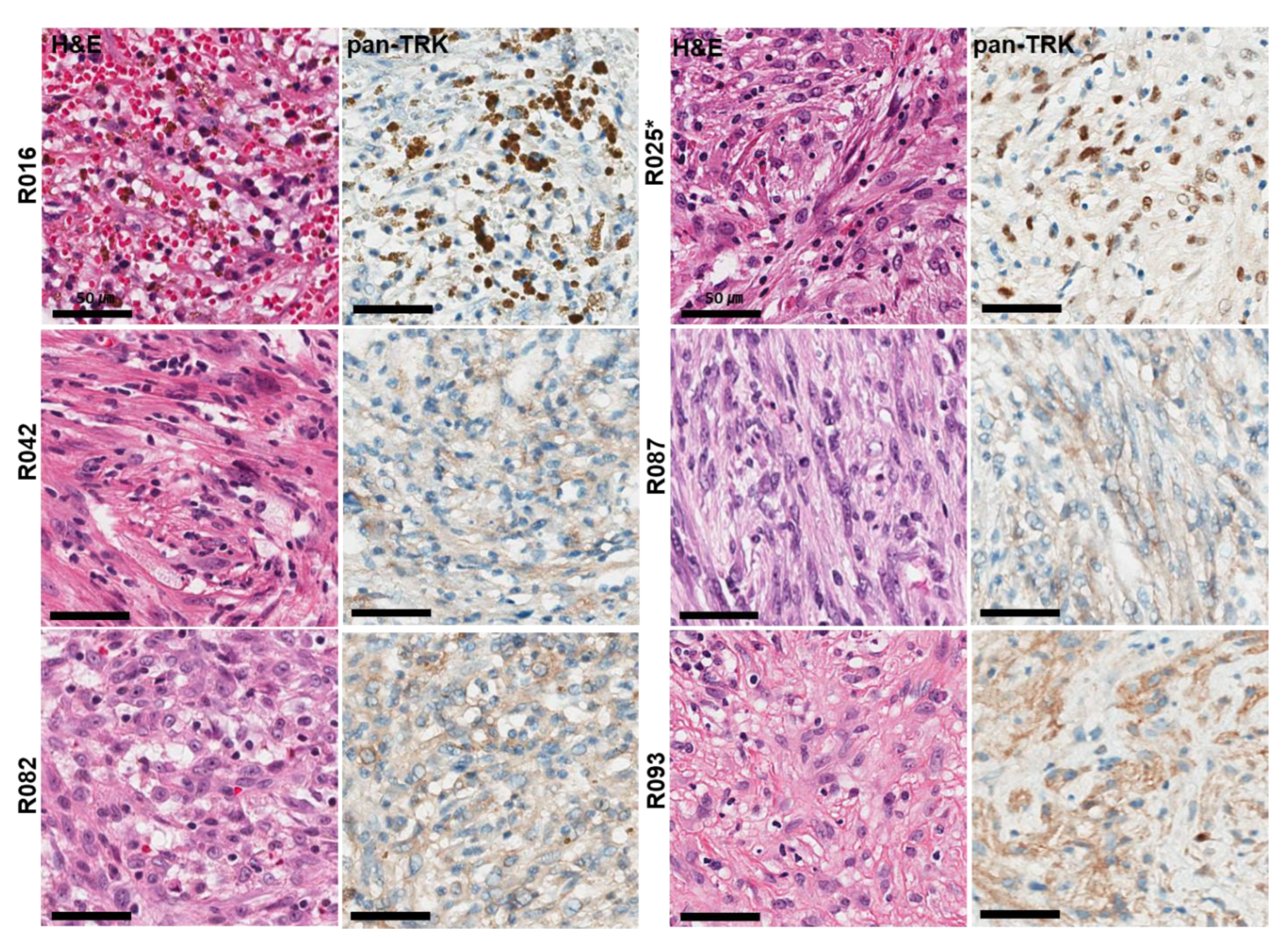
3.4. Inflammatory Myofibroblastic Tumor
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Vaishnavi, A.; Le, A.T.; Doebele, R.C. TRKing down an old oncogene in a new era of targeted therapy. Cancer Discov. 2015, 5, 25–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solomon, J.P.; Benayed, R.; Hechtman, J.F.; Ladanyi, M. Identifying patients with NTRK fusion cancer. Ann. Oncol. 2019, 30, viii16–viii22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocco, E.; Scaltriti, M.; Drilon, A. NTRK fusion-positive cancers and TRK inhibitor therapy. Nat. Rev. Clin. Oncol. 2018, 15, 731–747. [Google Scholar] [CrossRef]
- Drilon, A. TRK inhibitors in TRK fusion-positive cancers. Ann. Oncol. 2019, 30, viii23–viii30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farago, A.F.; Le, L.P.; Zheng, Z.; Muzikansky, A.; Drilon, A.; Patel, M.; Bauer, T.M.; Liu, S.V.; Ou, S.H.; Jackman, D.; et al. Durable Clinical Response to Entrectinib in NTRK1-Rearranged Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2015, 10, 1670–1674. [Google Scholar] [CrossRef] [Green Version]
- Drilon, A.; Siena, S.; Ou, S.I.; Patel, M.; Ahn, M.J.; Lee, J.; Bauer, T.M.; Farago, A.F.; Wheler, J.J.; Liu, S.V.; et al. Safety and Antitumor Activity of the Multitargeted Pan-TRK, ROS1, and ALK Inhibitor Entrectinib: Combined Results from Two Phase I Trials (ALKA-372-001 and STARTRK-1). Cancer Discov. 2017, 7, 400–409. [Google Scholar] [CrossRef] [Green Version]
- Drilon, A.; Laetsch, T.W.; Kummar, S.; DuBois, S.G.; Lassen, U.N.; Demetri, G.D.; Nathenson, M.; Doebele, R.C.; Farago, A.F.; Pappo, A.S.; et al. Efficacy of Larotrectinib in TRK Fusion-Positive Cancers in Adults and Children. N. Engl. J. Med. 2018, 378, 731–739. [Google Scholar] [CrossRef]
- Davis, J.L.; Lockwood, C.M.; Albert, C.M.; Tsuchiya, K.; Hawkins, D.S.; Rudzinski, E.R. Infantile NTRK-associated Mesenchymal Tumors. Pediatr. Dev. Pathol. 2018, 21, 68–78. [Google Scholar] [CrossRef] [Green Version]
- Bourgeois, J.M.; Knezevich, S.R.; Mathers, J.A.; Sorensen, P.H. Molecular detection of the ETV6-NTRK3 gene fusion differentiates congenital fibrosarcoma from other childhood spindle cell tumors. Am. J. Surg. Pathol. 2000, 24, 937–946. [Google Scholar] [CrossRef]
- Rubin, B.P.; Chen, C.J.; Morgan, T.W.; Xiao, S.; Grier, H.E.; Kozakewich, H.P.; Perez-Atayde, A.R.; Fletcher, J.A. Congenital mesoblastic nephroma t(12;15) is associated with ETV6-NTRK3 gene fusion: Cytogenetic and molecular relationship to congenital (infantile) fibrosarcoma. Am. J. Pathol. 1998, 153, 1451–1458. [Google Scholar] [CrossRef]
- Skalova, A.; Vanecek, T.; Sima, R.; Laco, J.; Weinreb, I.; Perez-Ordonez, B.; Starek, I.; Geierova, M.; Simpson, R.H.; Passador-Santos, F.; et al. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: A hitherto undescribed salivary gland tumor entity. Am. J. Surg. Pathol. 2010, 34, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Farago, A.F.; Taylor, M.S.; Doebele, R.C.; Zhu, V.W.; Kummar, S.; Spira, A.I.; Boyle, T.A.; Haura, E.B.; Arcila, M.E.; Benayed, R.; et al. Clinicopathologic Features of Non-Small-Cell Lung Cancer Harboring an NTRK Gene Fusion. JCO Precis Oncol. 2018, 2, 1–12. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Di Nicolantonio, F.; Schrock, A.B.; Lee, J.; Tejpar, S.; Sartore-Bianchi, A.; Hechtman, J.F.; Christiansen, J.; Novara, L.; Tebbutt, N.; et al. ALK, ROS1, and NTRK Rearrangements in Metastatic Colorectal Cancer. J. Natl. Cancer Inst. 2017, 109, djx089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, S.; Cotzia, P.; Hyman, D.M.; Drilon, A.; Tap, W.D.; Zhang, L.; Hechtman, J.F.; Frosina, D.; Jungbluth, A.A.; Murali, R.; et al. NTRK Fusions Define a Novel Uterine Sarcoma Subtype With Features of Fibrosarcoma. Am. J. Surg. Pathol. 2018, 42, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Lezcano, C.; Shoushtari, A.N.; Ariyan, C.; Hollmann, T.J.; Busam, K.J. Primary and Metastatic Melanoma with NTRK Fusions. Am. J. Surg. Pathol. 2018, 42, 1052–1058. [Google Scholar] [CrossRef]
- Racanelli, D.; Brenca, M.; Baldazzi, D.; Goeman, F.; Casini, B.; De Angelis, B.; Guercio, M.; Milano, G.M.; Tamborini, E.; Busico, A.; et al. Next-Generation Sequencing Approaches for the Identification of Pathognomonic Fusion Transcripts in Sarcomas: The Experience of the Italian ACC Sarcoma Working Group. Front. Oncol. 2020, 10, 489. [Google Scholar] [CrossRef] [Green Version]
- Lasota, J.; Chlopek, M.; Lamoureux, J.; Christiansen, J.; Kowalik, A.; Wasag, B.; Felisiak-Golabek, A.; Agaimy, A.; Biernat, W.; Canzonieri, V.; et al. Colonic Adenocarcinomas Harboring NTRK Fusion Genes: A Clinicopathologic and Molecular Genetic Study of 16 Cases and Review of the Literature. Am. J. Surg. Pathol. 2020, 44, 162–173. [Google Scholar] [CrossRef]
- Ardini, E.; Bosotti, R.; Borgia, A.L.; De Ponti, C.; Somaschini, A.; Cammarota, R.; Amboldi, N.; Raddrizzani, L.; Milani, A.; Magnaghi, P.; et al. The TPM3-NTRK1 rearrangement is a recurring event in colorectal carcinoma and is associated with tumor sensitivity to TRKA kinase inhibition. Mol. Oncol. 2014, 8, 1495–1507. [Google Scholar] [CrossRef]
- Lasota, J.; Chlopek, M.; Wasag, B.; Kowalik, A.; Christiansen, J.; Lamoureux, J.; Kuzniacka, A.; Felisiak-Golabek, A.; Liu, Y.; Reyes, T.A.R.; et al. Colorectal Adenocarcinomas Harboring ALK Fusion Genes: A Clinicopathologic and Molecular Genetic Study of 12 Cases and Review of the Literature. Am. J. Surg. Pathol. 2020, 44, 1224–1234. [Google Scholar] [CrossRef]
- Kim, J.H.; Hong, J.H.; Choi, Y.L.; Lee, J.A.; Seo, M.K.; Lee, M.S.; An, S.B.; Sung, M.J.; Cho, N.Y.; Kim, S.S.; et al. NTRK oncogenic fusions are exclusively associated with the serrated neoplasia pathway in the colorectum and begin to occur in sessile serrated lesions. J. Pathol. 2021, 255, 399–411. [Google Scholar] [CrossRef]
- Gatalica, Z.; Xiu, J.; Swensen, J.; Vranic, S. Molecular characterization of cancers with NTRK gene fusions. Mod. Pathol. 2019, 32, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Solomon, J.P.; Linkov, I.; Rosado, A.; Mullaney, K.; Rosen, E.Y.; Frosina, D.; Jungbluth, A.A.; Zehir, A.; Benayed, R.; Drilon, A.; et al. NTRK fusion detection across multiple assays and 33,997 cases: Diagnostic implications and pitfalls. Mod. Pathol. 2020, 33, 38–46. [Google Scholar] [CrossRef]
- Koopman, B.; Kuijpers, C.; Groen, H.J.M.; Timens, W.; Schuuring, E.; Willems, S.M.; van Kempen, L.C. Detection of NTRK Fusions and TRK Expression and Performance of pan-TRK Immunohistochemistry in Routine Diagnostics: Results from a Nationwide Community-Based Cohort. Diagnostics 2022, 12, 668. [Google Scholar] [CrossRef] [PubMed]
- Sato, K.; Kawazu, M.; Yamamoto, Y.; Ueno, T.; Kojima, S.; Nagae, G.; Abe, H.; Soda, M.; Oga, T.; Kohsaka, S.; et al. Fusion Kinases Identified by Genomic Analyses of Sporadic Microsatellite Instability-High Colorectal Cancers. Clin. Cancer Res. 2019, 25, 378–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amatu, A.; Sartore-Bianchi, A.; Siena, S. NTRK gene fusions as novel targets of cancer therapy across multiple tumour types. ESMO Open 2016, 1, e000023. [Google Scholar] [CrossRef] [Green Version]
- Gleason, B.C.; Hornick, J.L. Inflammatory myofibroblastic tumours: Where are we now? J. Clin. Pathol. 2008, 61, 428–437. [Google Scholar] [CrossRef] [Green Version]
- Lovly, C.M.; Gupta, A.; Lipson, D.; Otto, G.; Brennan, T.; Chung, C.T.; Borinstein, S.C.; Ross, J.S.; Stephens, P.J.; Miller, V.A.; et al. Inflammatory myofibroblastic tumors harbor multiple potentially actionable kinase fusions. Cancer Discov. 2014, 4, 889–895. [Google Scholar] [CrossRef] [Green Version]
- Antonescu, C.R.; Suurmeijer, A.J.; Zhang, L.; Sung, Y.S.; Jungbluth, A.A.; Travis, W.D.; Al-Ahmadie, H.; Fletcher, C.D.; Alaggio, R. Molecular characterization of inflammatory myofibroblastic tumors with frequent ALK and ROS1 gene fusions and rare novel RET rearrangement. Am. J. Surg. Pathol. 2015, 39, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Hornick, J.L.; Sholl, L.M.; Dal Cin, P.; Childress, M.A.; Lovly, C.M. Expression of ROS1 predicts ROS1 gene rearrangement in inflammatory myofibroblastic tumors. Mod. Pathol. 2015, 28, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, H.; Yoshida, A.; Taguchi, K.; Kohashi, K.; Hatanaka, Y.; Yamashita, A.; Mori, D.; Oda, Y. ALK, ROS1 and NTRK3 gene rearrangements in inflammatory myofibroblastic tumours. Histopathology 2016, 69, 72–83. [Google Scholar] [CrossRef]
- Debonis, S.A.; Bongiovanni, A.; Pieri, F.; Fausti, V.; De Vita, A.; Riva, N.; Gurrieri, L.; Vanni, S.; Diano, D.; Mercatali, L.; et al. ALK-negative lung inflammatory myofibroblastic tumor in a young adult: A case report and literature review of molecular alterations. Medicine 2021, 100, e25972. [Google Scholar] [CrossRef] [PubMed]
- Recine, F.; De Vita, A.; Fausti, V.; Pieri, F.; Bongiovanni, A.; Franchini, E.; Casadei, R.; Falasconi, M.C.; Oboldi, D.; Matteucci, F.; et al. Case Report: Adult NTRK-Rearranged Spindle Cell Neoplasm: Early Tumor Shrinkage in a Case With Bone and Visceral Metastases Treated With Targeted Therapy. Front. Oncol. 2021, 11, 740676. [Google Scholar] [CrossRef] [PubMed]
- Siozopoulou, V.; Smits, E.; De Winne, K.; Marcq, E.; Pauwels, P. NTRK Fusions in Sarcomas: Diagnostic Challenges and Clinical Aspects. Diagnostics 2021, 11, 478. [Google Scholar] [CrossRef] [PubMed]
- Dang, X.; Xiang, T.; Zhao, C.; Tang, H.; Cui, P. EML4-NTRK3 Fusion Cervical Sarcoma: A Case Report and Literature Review. Front. Med. 2022, 9, 832376. [Google Scholar] [CrossRef] [PubMed]
- Hung, Y.P.; Fletcher, C.D.M.; Hornick, J.L. Evaluation of pan-TRK immunohistochemistry in infantile fibrosarcoma, lipofibromatosis-like neural tumour and histological mimics. Histopathology 2018, 73, 634–644. [Google Scholar] [CrossRef]
- Brodeur, G.M.; Minturn, J.E.; Ho, R.; Simpson, A.M.; Iyer, R.; Varela, C.R.; Light, J.E.; Kolla, V.; Evans, A.E. Trk receptor expression and inhibition in neuroblastomas. Clin. Cancer Res. 2009, 15, 3244–3250. [Google Scholar] [CrossRef] [Green Version]
- Solomon, J.P.; Hechtman, J.F. Detection of NTRK Fusions: Merits and Limitations of Current Diagnostic Platforms. Cancer Res. 2019, 79, 3163–3168. [Google Scholar] [CrossRef]
- Hsiao, S.J.; Zehir, A.; Sireci, A.N.; Aisner, D.L. Detection of Tumor NTRK Gene Fusions to Identify Patients Who May Benefit from Tyrosine Kinase (TRK) Inhibitor Therapy. J. Mol. Diagn. 2019, 21, 553–571. [Google Scholar] [CrossRef] [Green Version]
- Hechtman, J.F.; Benayed, R.; Hyman, D.M.; Drilon, A.; Zehir, A.; Frosina, D.; Arcila, M.E.; Dogan, S.; Klimstra, D.S.; Ladanyi, M.; et al. Pan-Trk Immunohistochemistry Is an Efficient and Reliable Screen for the Detection of NTRK Fusions. Am. J. Surg. Pathol. 2017, 41, 1547–1551. [Google Scholar] [CrossRef]
- Xu, B.; Haroon Al Rasheed, M.R.; Antonescu, C.R.; Alex, D.; Frosina, D.; Ghossein, R.; Jungbluth, A.A.; Katabi, N. Pan-Trk immunohistochemistry is a sensitive and specific ancillary tool for diagnosing secretory carcinoma of the salivary gland and detecting ETV6-NTRK3 fusion. Histopathology 2020, 76, 375–382. [Google Scholar] [CrossRef]
- Yamashiro, Y.; Kurihara, T.; Hayashi, T.; Suehara, Y.; Yao, T.; Kato, S.; Saito, T. NTRK fusion in Japanese colorectal adenocarcinomas. Sci. Rep. 2021, 11, 5635. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor Type | Case No. | Age at Diagnosis | Sex | Final Diagnosis | MSI Status |
|---|---|---|---|---|---|
| Non-small cell lung carcinoma (NSCLC) | L099 | 68 | M | Adenocarcinoma, poorly differentiated (solid pattern) | |
| L347 * | 42 | M | Adenocarcinoma, moderately differentiated (papillary pattern) | ||
| L491 * | 54 | F | Adenocarcinoma, moderately differentiated (acinar pattern) | ||
| Colorectal carcinoma (CRC) | C175 * | 78 | F | Mucinous adenocarcinoma | MSI-high |
| C178 * | 75 | F | Adenocarcinoma, poorly differentiated | MSI-high | |
| C216 * | 73 | F | Adenocarcinoma, poorly differentiated | MSI-high | |
| C421 * | 68 | F | Adenocarcinoma, moderately differentiated | MSI-high | |
| C478 * | 65 | F | Metastatic Adenocarcinoma | MSI-high | |
| C503 * | 60 | M | Adenocarcinoma, moderately differentiated | MSI-high | |
| Inflammatory myofibroblastic tumor (IMT) | R016 | 72 | M | Inflammatory myofibroblastic tumor | |
| R025 * | 41 | F | Inflammatory myofibroblastic tumor | ||
| R042 | 28 | M | Inflammatory myofibroblastic tumor | ||
| R082 | 33 | M | Inflammatory myofibroblastic tumor | ||
| R087 | 5 | F | Inflammatory myofibroblastic tumor | ||
| R093 | 45 | M | Inflammatory myofibroblastic tumor |
| Tumor Type | Case No. | TRK IHC Staining Intensity | TRK IHC Staining Pattern | Fusion Type | Exon # of BP | ChrA | GeneA | Break Point A | ChrB | GeneB | Break Point B | Supporting Reads |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Non-small cell lung carcinoma (NSCLC) | L099 | 1–2 | C, M | |||||||||
| L347 * | 2 | C, M | SQSTM1-NTRK3 | S(6)N(14) | chr5 | SQSTM1 | chr5: 179252226 | chr15 | NTRK3 | chr15: 88576276 | 6584 | |
| L491 * | 3 | C, M | CD74-NTRK1 | C(7)N(10) | chr5 | CD74 | chr5: 149782684 | chr1 | NTRK1 | chr1: 156844362 | 214 | |
| C(6)N(10) | chr5 | CD74 | chr5: 149784243 | chr1 | NTRK1 | chr1: 156844361 | 1199 | |||||
| Colorectal carcinoma (CRC) | C175 * | 3 | C, M | TPM3-NTRK1 | T(7)N(10) | chr1 | TPM3 | chr1: 154142876 | chr1 | NTRK1 | chr1: 156844361 | 318 |
| C178 * | 3 | C, M | TPM3-NTRK1 | T(7)N(10) | chr1 | TPM3 | chr1: 154142876 | chr1 | NTRK1 | chr1: 156844361 | 673 | |
| C216 * | 3 | C, M | TPM3-NTRK1 | T(7)N(10) | chr1 | TPM3 | chr1: 154142876 | chr1 | NTRK1 | chr1: 156844361 | 50 | |
| C421 * | 1-2 | C, M | TPM3-NTRK1 | T(7)N(10) | chr1 | TPM3 | chr1: 154142876 | chr1 | NTRK1 | chr1: 156844361 | 258 | |
| C478 * | 3 | NM | LMNA-NTRK1 | L(13)N(12) | chr1 | LMNA | chr1: 156108546 | chr1 | NTRK1 | chr1: 156845310 | 9 | |
| L(13)N(12) | chr1 | LMNA | chr1: 156109604 | chr1 | NTRK1 | chr1: 156845310 | 663 | |||||
| C503 * | 2 | N | ETV6-NTRK3 | E(5)N(15) | chr12 | ETV6 | chr12: 12022900 | chr15 | NTRK3 | chr15: 88483984 | 217 | |
| Inflammatory myofibroblastic tumor (IMT) | R016 | 2 | C | |||||||||
| R025 * | 2 | N | ETV6-NTRK3 | E(5)N(15) | chr12 | ETV6 | chr12: 12022900 | chr15 | NTRK3 | chr15: 88483984 | 31 | |
| R042 | 1–2 | C | ||||||||||
| R082 | 1–2 | C | ||||||||||
| R087 | 1–2 | C | ||||||||||
| R093 | 2 | C |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bang, H.; Lee, M.-S.; Sung, M.; Choi, J.; An, S.; Kim, S.-H.; Lee, S.E.; Choi, Y.-L. NTRK Fusions in 1113 Solid Tumors in a Single Institution. Diagnostics 2022, 12, 1450. https://doi.org/10.3390/diagnostics12061450
Bang H, Lee M-S, Sung M, Choi J, An S, Kim S-H, Lee SE, Choi Y-L. NTRK Fusions in 1113 Solid Tumors in a Single Institution. Diagnostics. 2022; 12(6):1450. https://doi.org/10.3390/diagnostics12061450
Chicago/Turabian StyleBang, Heejin, Mi-Sook Lee, Minjung Sung, Juyoung Choi, Sungbin An, Seok-Hyung Kim, Seung Eun Lee, and Yoon-La Choi. 2022. "NTRK Fusions in 1113 Solid Tumors in a Single Institution" Diagnostics 12, no. 6: 1450. https://doi.org/10.3390/diagnostics12061450
APA StyleBang, H., Lee, M.-S., Sung, M., Choi, J., An, S., Kim, S.-H., Lee, S. E., & Choi, Y.-L. (2022). NTRK Fusions in 1113 Solid Tumors in a Single Institution. Diagnostics, 12(6), 1450. https://doi.org/10.3390/diagnostics12061450