
Optimal Conspicuity of Liver Metastases in Virtual Monochromatic Imaging Reconstructions on a Novel Photon-Counting Detector CT—Effect of keV Settings and BMI

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Scan Protocol and Reconstruction Settings
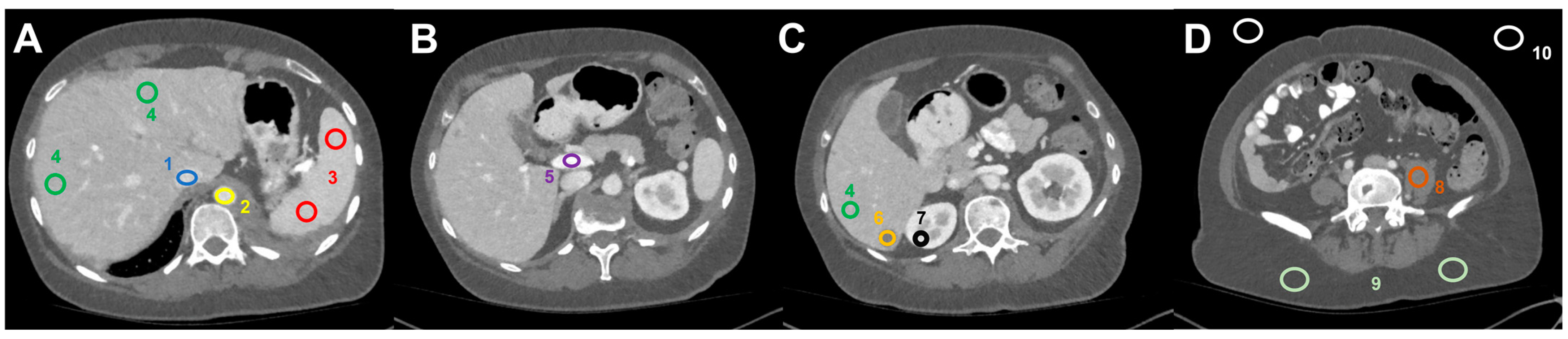
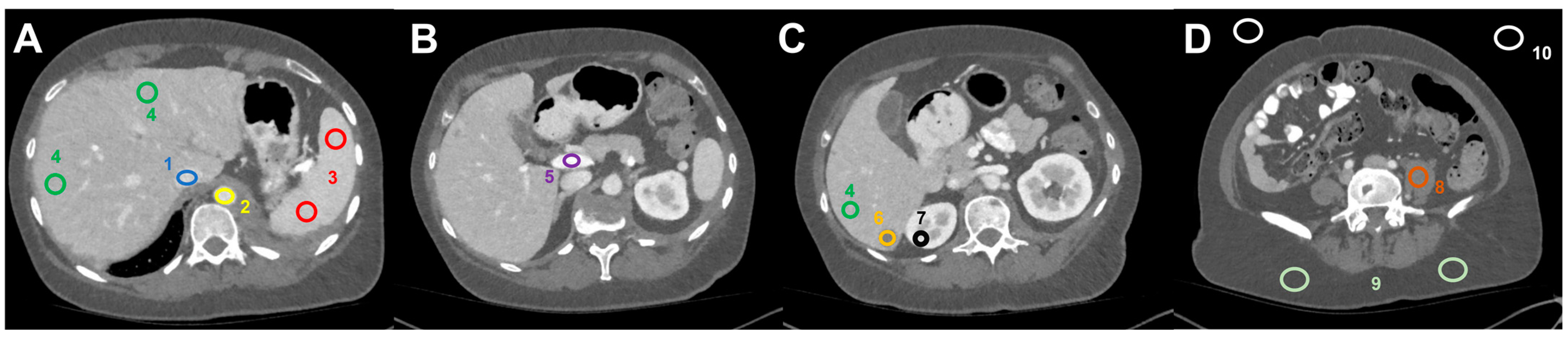
2.2. Image Postprocessing and Analysis
2.3. Weight- and BMI-Dependent Analyses
2.4. Statistical Analysis
3. Results
3.1. Patient Population
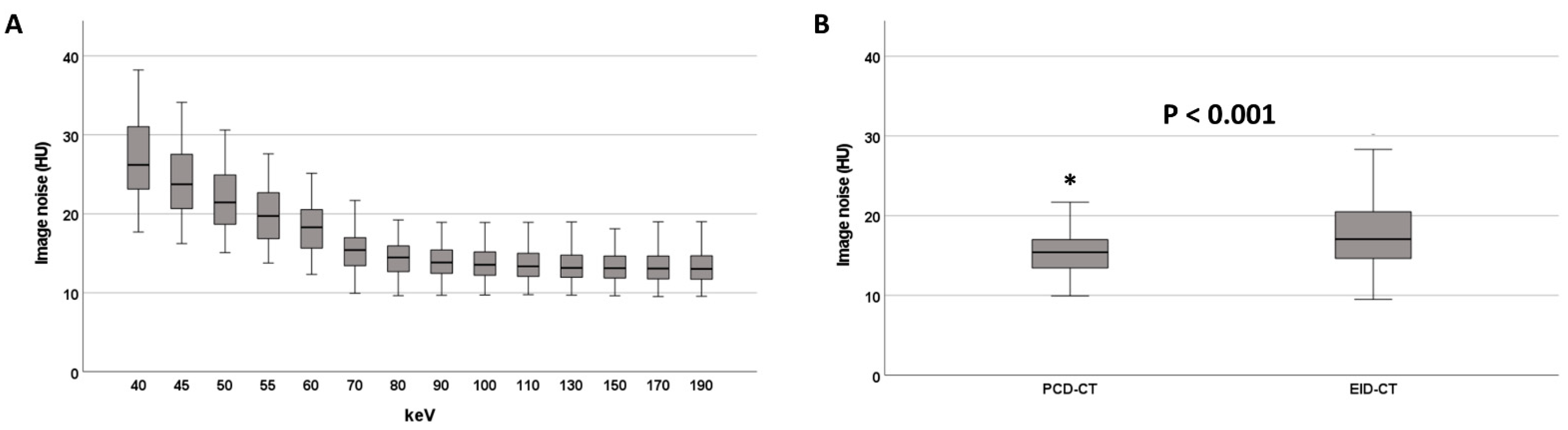
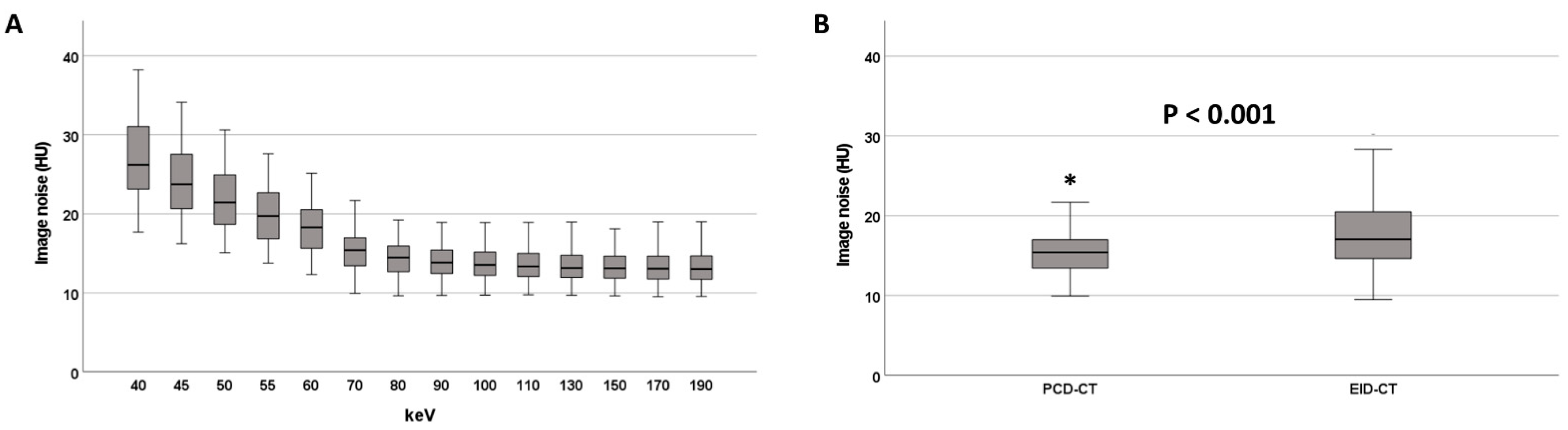
3.2. Image Noise
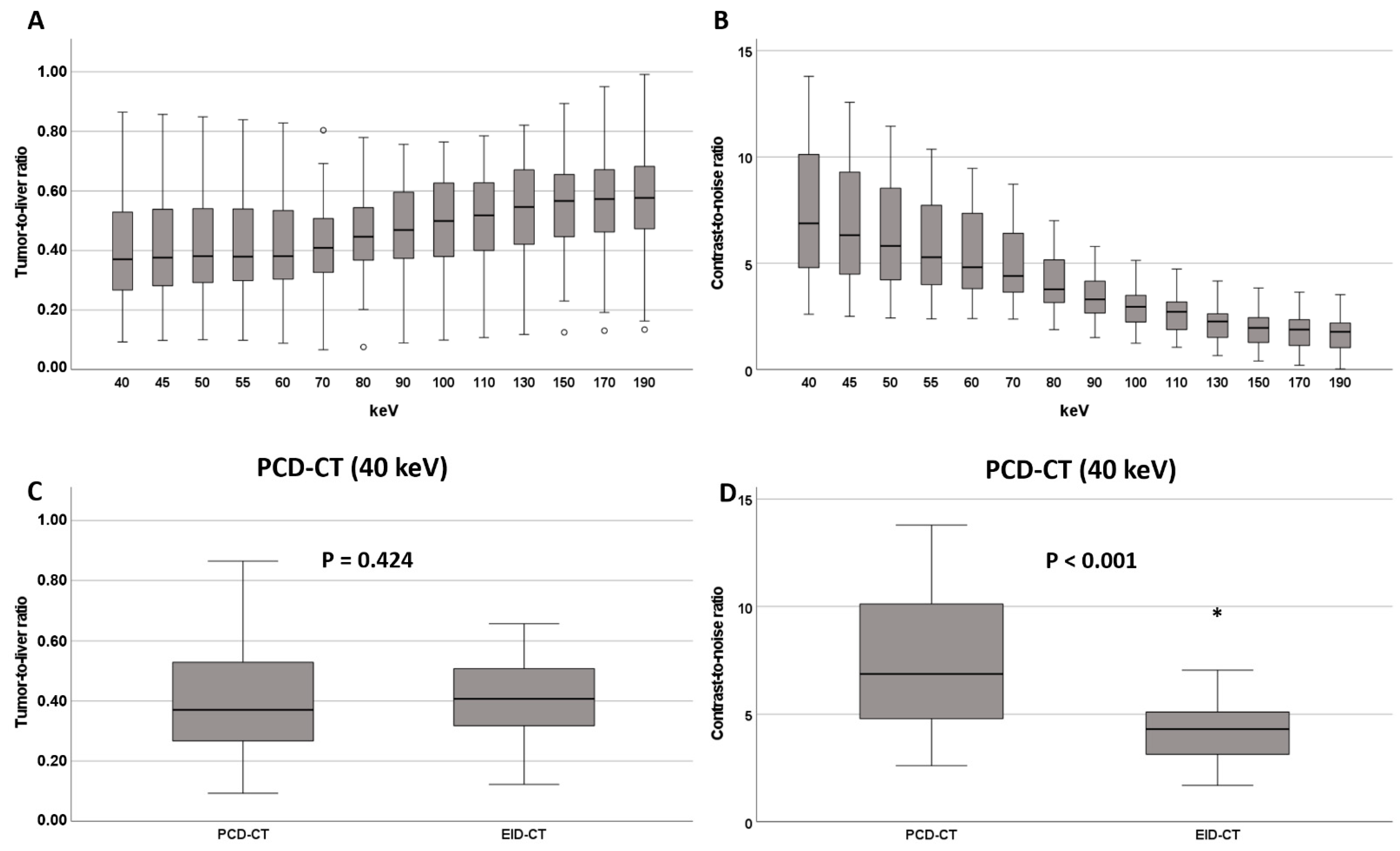
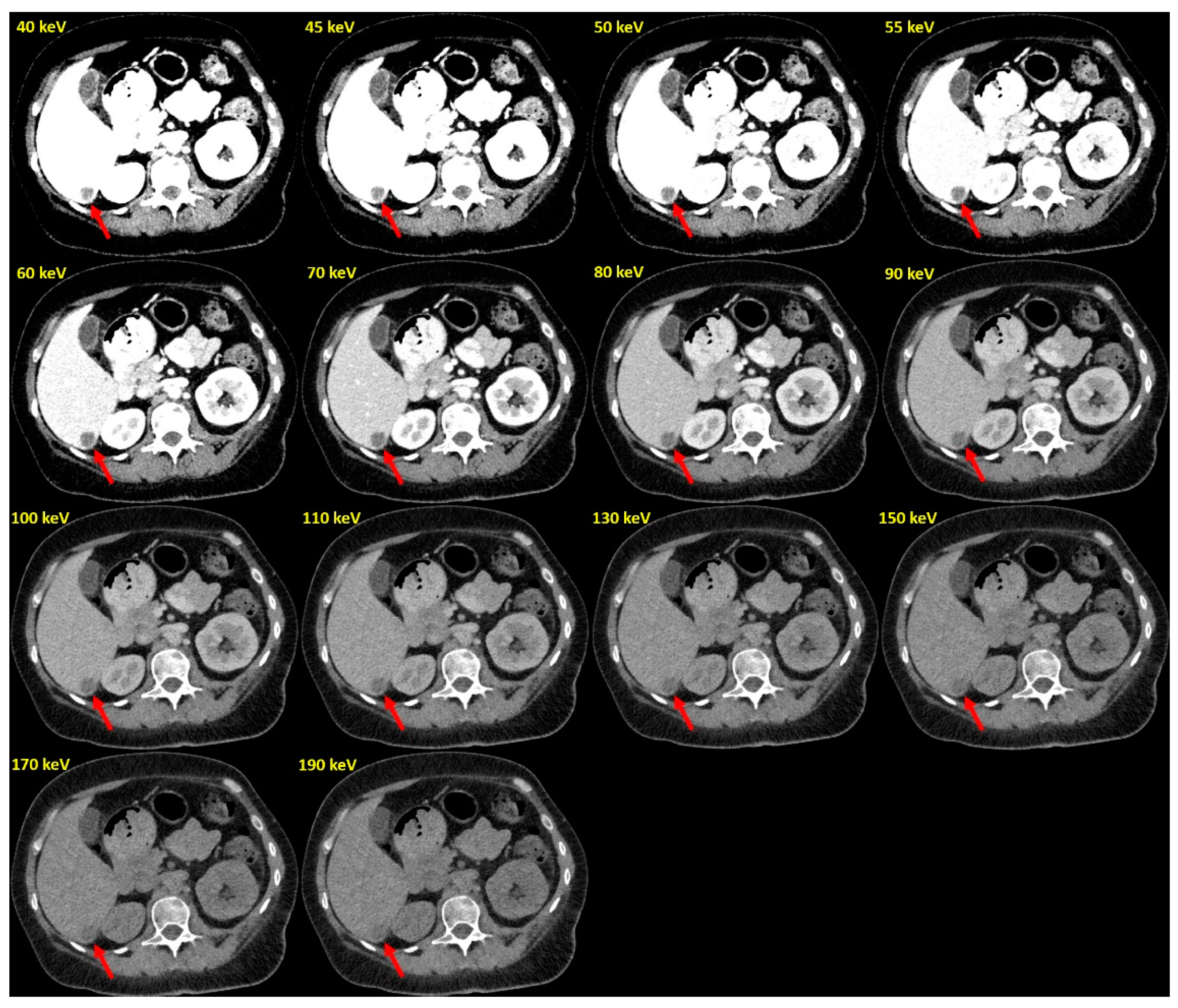
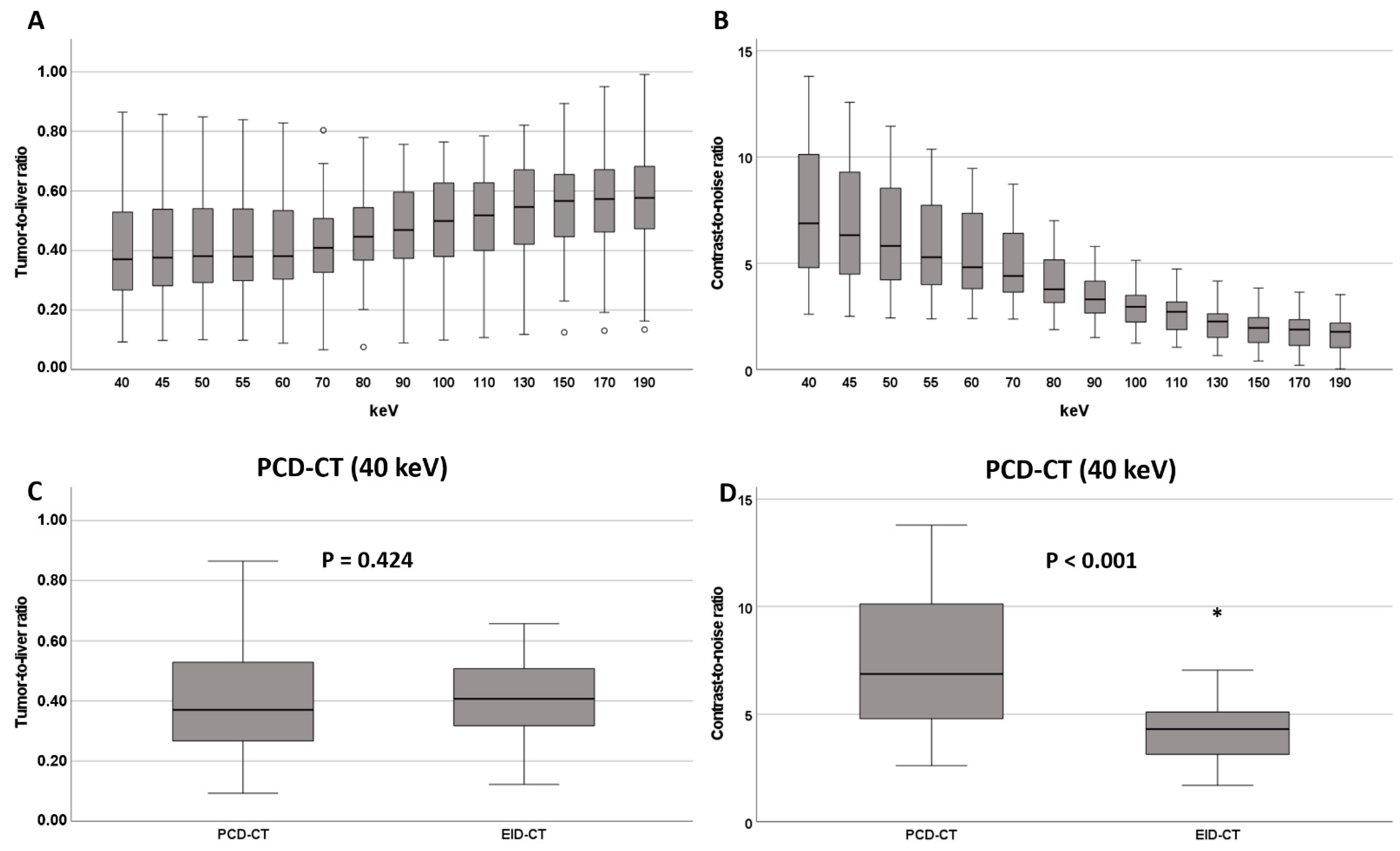
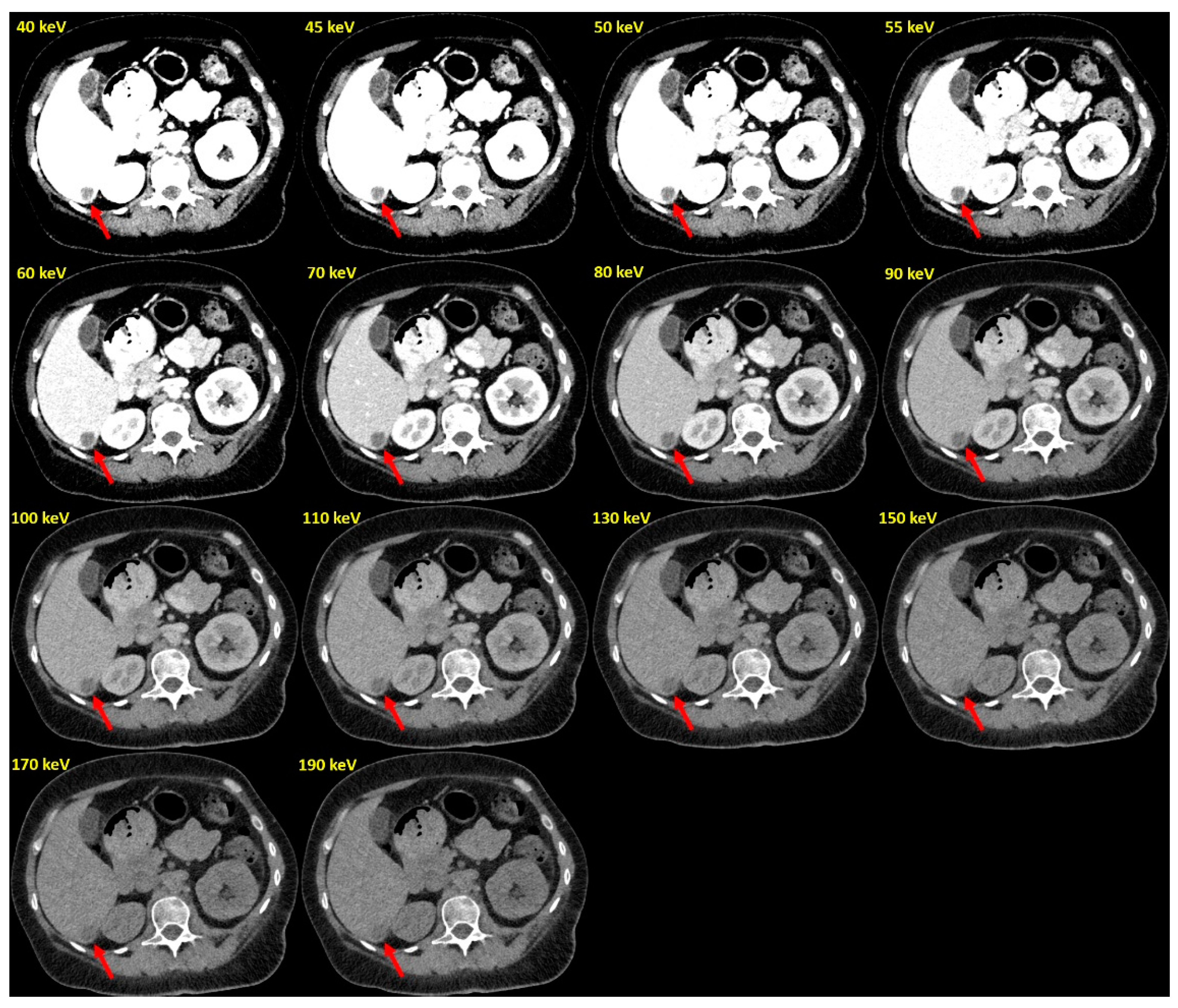
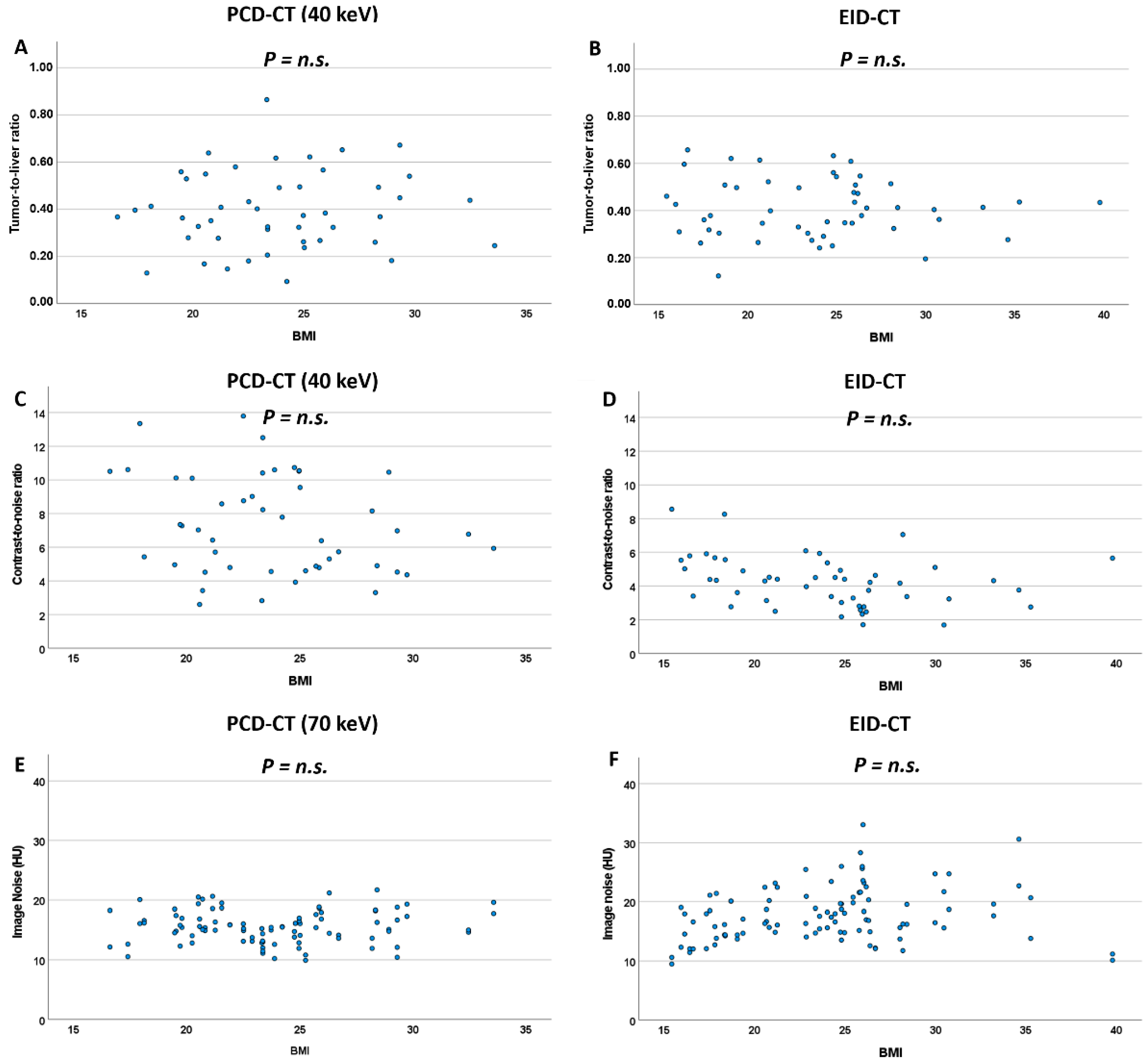
3.3. Tumor-to-Liver Ratio (TLR)
3.4. Contrast-to-Noise Ratio (CNR)
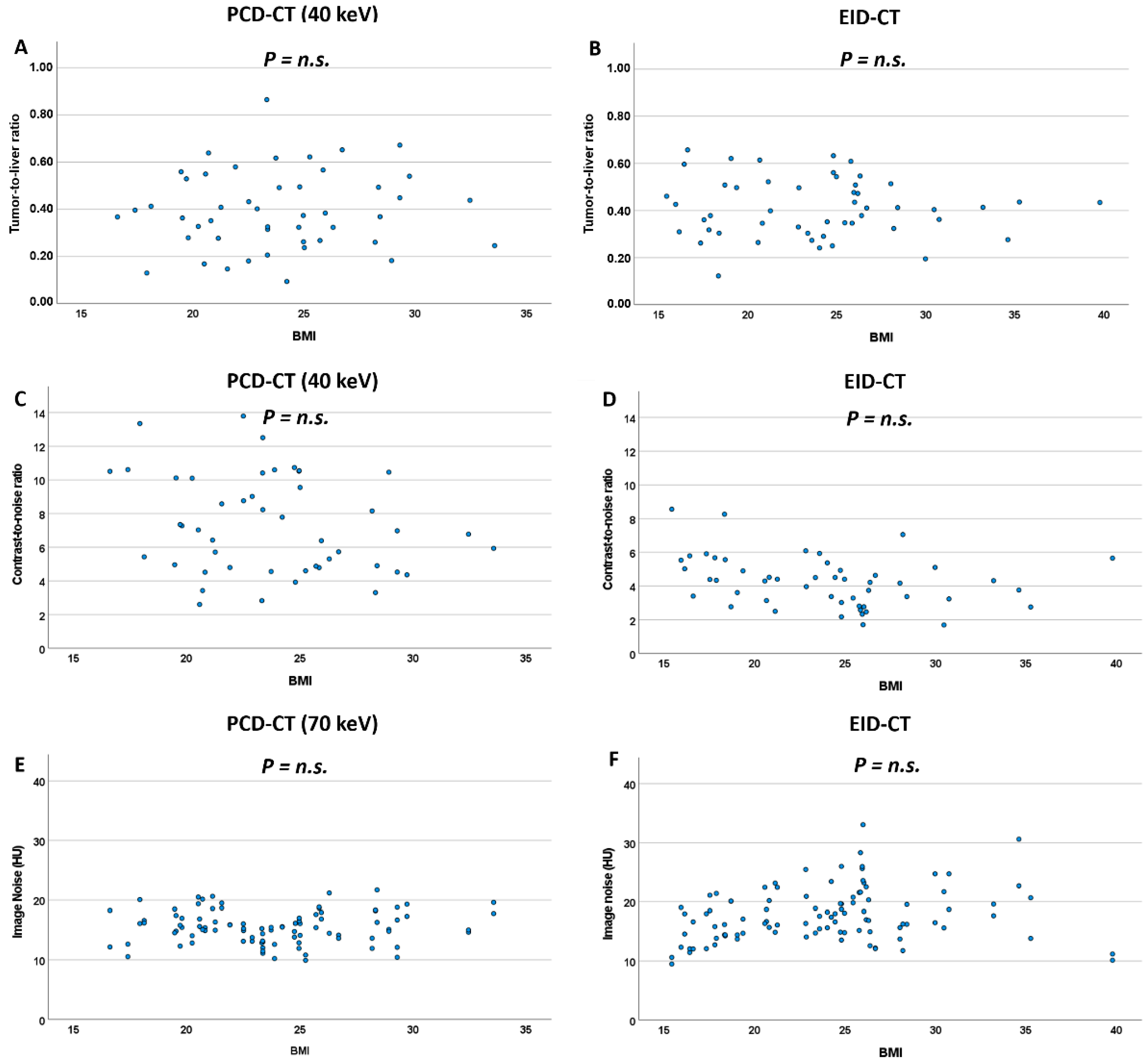
3.5. Effect of BMI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agrawal, M.D.; Pinho, D.F.; Kulkarni, N.M.; Hahn, P.F.; Guimaraes, A.R.; Sahani, D.V. Oncologic Applications of Dual-Energy CT in the Abdomen. Radiographics 2014, 34, 589–612. [Google Scholar] [CrossRef] [PubMed]
- Hanson, G.J.; Michalak, G.J.; Childs, R.; McCollough, B.; Kurup, A.N.; Hough, D.M.; Frye, J.M.; Fidler, J.L.; Venkatesh, S.K.; Leng, S.; et al. Low KV versus Dual-Energy Virtual Monoenergetic CT Imaging for Proven Liver Lesions: What Are the Advantages and Trade-Offs in Conspicuity and Image Quality? A Pilot Study. Abdom. Radiol. 2018, 43, 1404–1412. [Google Scholar] [CrossRef] [PubMed]
- Lenga, L.; Lange, M.; Arendt, C.T.; Yel, I.; Booz, C.; Durden, J.; Leithner, D.; Vogl, T.J.; Albrecht, M.H.; Martin, S.S. Can Dual-Energy CT-Based Virtual Monoenergetic Imaging Improve the Assessment of Hypodense Liver Metastases in Patients with Hepatic Steatosis? Acad. Radiol. 2021, 28, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Lenga, L.; Czwikla, R.; Wichmann, J.L.; Leithner, D.; Albrecht, M.H.; Booz, C.; Arendt, C.T.; Yel, I.; D’Angelo, T.; Vogl, T.J.; et al. Dual-Energy CT in Patients with Colorectal Cancer: Improved Assessment of Hypoattenuating Liver Metastases Using Noise-Optimized Virtual Monoenergetic Imaging. Eur. J. Radiol. 2018, 106, 184–191. [Google Scholar] [CrossRef]
- de Cecco, C.N.; Caruso, D.; Schoepf, U.J.; Wichmann, J.L.; ter Louw, J.R.; Perry, J.D.; Picard, M.M.; Schaefer, A.R.; Parker, L.W.; Hardie, A.D. Optimization of Window Settings for Virtual Monoenergetic Imaging in Dual-Energy CT of the Liver: A Multi-Reader Evaluation of Standard Monoenergetic and Advanced Imaged-Based Monoenergetic Datasets. Eur. J. Radiol. 2016, 85, 695–699. [Google Scholar] [CrossRef]
- Lenga, L.; Lange, M.; Arendt, C.T.; Booz, C.; Yel, I.; Bodelle, B.; D’Angelo, T.; Hammerstingl, R.M.; Huizinga, N.A.; Vogl, T.J.; et al. Measurement Reliability and Diagnostic Accuracy of Virtual Monoenergetic Dual-Energy CT in Patients with Colorectal Liver Metastases. Acad. Radiol. 2020, 27, e168–e175. [Google Scholar] [CrossRef]
- Große Hokamp, N.; Obmann, V.C.; Kessner, R.; Gilkeson, R.C.; Gupta, A.; Persigehl, T.; Haneder, S.; Ramaiya, N. Virtual Monoenergetic Images for Diagnostic Assessment of Hypodense Lesions Within the Liver: Semiautomatic Estimation of Window Settings Using Linear Models. J. Comput. Assist. Tomogr. 2018, 42, 925–931. [Google Scholar] [CrossRef]
- Große Hokamp, N.; Obmann, V.C.; Kessner, R.; Laukamp, K.R.; Persigehl, T.; Haneder, S.; Ramaiya, N. Improved Visualization of Hypodense Liver Lesions in Virtual Monoenergetic Images from Spectral Detector CT: Proof of Concept in a 3D-Printed Phantom and Evaluation in 74 Patients. Eur. J. Radiol. 2018, 109, 114–123. [Google Scholar] [CrossRef]
- Caruso, D.; de Cecco, C.N.; Schoepf, U.J.; Schaefer, A.R.; Leland, P.W.; Johnson, D.; Laghi, A.; Hardie, A.D. Can Dual-Energy Computed Tomography Improve Visualization of Hypoenhancing Liver Lesions in Portal Venous Phase? Assessment of Advanced Image-Based Virtual Monoenergetic Images. Clin. Imaging 2017, 41, 118–124. [Google Scholar] [CrossRef]
- Nagayama, Y.; Iyama, A.; Oda, S.; Taguchi, N.; Nakaura, T.; Utsunomiya, D.; Kikuchi, Y.; Yamashita, Y. Dual-Layer Dual-Energy Computed Tomography for the Assessment of Hypovascular Hepatic Metastases: Impact of Closing k-Edge on Image Quality and Lesion Detectability. Eur. Radiol. 2019, 29, 2837–2847. [Google Scholar] [CrossRef]
- Yu, L.; Christner, J.A.; Leng, S.; Wang, J.; Fletcher, J.G.; McCollough, C.H. Virtual Monochromatic Imaging in Dual-Source Dual-Energy CT: Radiation Dose and Image Quality. Med. Phys. 2011, 38, 6371–6379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, Y.; Gao, S.-Y.; Wang, Z.-L.; Li, X.-T.; Sun, Y.-S.; Tang, L.; Zhang, X.-P. Which Should Be the Routine Cross-Sectional Reconstruction Mode in Spectral CT Imaging: Monochromatic or Polychromatic? Br. J. Radiol. 2012, 85, e887–e890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leng, S.; Bruesewitz, M.; Tao, S.; Rajendran, K.; Halaweish, A.F.; Campeau, N.G.; Fletcher, J.G.; McCollough, C.H. Photon-Counting Detector CT: System Design and Clinical Applications of an Emerging Technology. Radiographics 2019, 39, 729–743. [Google Scholar] [CrossRef] [PubMed]
- Willemink, M.J.; Persson, M.; Pourmorteza, A.; Pelc, N.J.; Fleischmann, D. Photon-Counting CT: Technical Principles and Clinical Prospects. Radiology 2018, 289, 293–312. [Google Scholar] [CrossRef]
- Flohr, T.; Petersilka, M.; Henning, A.; Ulzheimer, S.; Ferda, J.; Schmidt, B. Photon-Counting CT Review. Phys. Med. 2020, 79, 126–136. [Google Scholar] [CrossRef]
- Bette, S.J.; Braun, F.M.; Haerting, M.; Decker, J.A.; Luitjens, J.H.; Scheurig-Muenkler, C.; Kroencke, T.J.; Schwarz, F. Visualization of Bone Details in a Novel Photon-Counting Dual-Source CT Scanner-Comparison with Energy-Integrating CT. Eur. Radiol. 2021, 32, 2930–2936. [Google Scholar] [CrossRef]
- Jungblut, L.; Kronenberg, D.; Mergen, V.; Higashigaito, K.; Schmidt, B.; Euler, A.; Alkadhi, H.; Frauenfelder, T.; Martini, K. Impact of Contrast Enhancement and Virtual Monoenergetic Image Energy Levels on Emphysema Quantification: Experience with Photon-Counting Detector Computed Tomography. Investig. Radiol. 2022. [Google Scholar] [CrossRef]
- Chappard, C.; Abascal, J.; Olivier, C.; Si-Mohamed, S.; Boussel, L.; Piala, J.B.; Douek, P.; Peyrin, F. Virtual Monoenergetic Images from Photon-Counting Spectral Computed Tomography to Assess Knee Osteoarthritis. Eur. Radiol. Exp. 2022, 6, 10. [Google Scholar] [CrossRef]
- Euler, A.; Higashigaito, K.; Mergen, V.; Sartoretti, T.; Zanini, B.; Schmidt, B.; Flohr, T.G.; Ulzheimer, S.; Eberhard, M.; Alkadhi, H. High-Pitch Photon-Counting Detector Computed Tomography Angiography of the Aorta: Intraindividual Comparison to Energy-Integrating Detector Computed Tomography at Equal Radiation Dose. Investig. Radiol. 2022, 57, 115–121. [Google Scholar] [CrossRef]
- Higashigaito, K.; Euler, A.; Eberhard, M.; Flohr, T.G.; Schmidt, B.; Alkadhi, H. Contrast-Enhanced Abdominal CT with Clinical Photon-Counting Detector CT: Assessment of Image Quality and Comparison with Energy-Integrating Detector CT. Acad. Radiol. 2022, 29, 689–697. [Google Scholar] [CrossRef]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An Open-Source Platform for Biological-Image Analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacCallum, R.C.; Zhang, S.; Preacher, K.J.; Rucker, D.D. On the Practice of Dichotomization of Quantitative Variables. Psychol. Methods 2002, 7, 19–40. [Google Scholar] [CrossRef] [PubMed]
- Curtin, F.; Schulz, P. Multiple Correlations and Bonferroni’s Correction. Biol. Psychiatry 1998, 44, 775–777. [Google Scholar] [CrossRef]
- Marin, D.; Ramirez-Giraldo, J.C.; Gupta, S.; Fu, W.; Stinnett, S.S.; Mileto, A.; Bellini, D.; Patel, B.; Samei, E.; Nelson, R.C. Effect of a Noise-Optimized Second-Generation Monoenergetic Algorithm on Image Noise and Conspicuity of Hypervascular Liver Tumors: An In Vitro and In Vivo Study. AJR Am. J. Roentgenol. 2016, 206, 1222–1232. [Google Scholar] [CrossRef] [PubMed]
- Qurashi, A.A.; Rainford, L.A.; Alshamrani, K.M.; Foley, S.J. The Impact of Obesity on Abdominal CT Radiation Dose and Image Quality. Radiat. Prot. Dosim. 2019, 185, 17–26. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | PCD-CT | EID-CT | p-Value |
|---|---|---|---|
| Age, years | 65.0 ± 12.4 (32–85) | 65.7 ± 11.8 (32–88) | 0.597 |
| Sex, male | 29/50 | 28/50 | 0.693 |
| BMI, kg/m2 | 23.3 [20.6; 25.9] | 24.4 [19.0; 26.3] | 0.934 |
| CTDI, mGy | 6.7 [5.9; 8.1] | 6.4 [4.9; 8.4] | 0.128 |
| DLP, mGy*cm | 402.0 [339.0; 491.0] | 378.9 [274.4; 492.9] | 0.362 |
| Primary Malignancy | |||
| ● Colorectal cancer | 13 | 17 | |
| ● Pancreatic cancer | 11 | 8 | |
| ● Lung cancer | 5 | 3 | |
| ● Other | 21 | 22 |
| keV Level | Tumor-to-Liver Ratio (TLR) | Contrast-to-Noise Ratio (CNR) | ||||
|---|---|---|---|---|---|---|
| PCD-CT | EID-CT | p-Value | PCD-CT | EID-CT | p-Value | |
| 40 | 0.37 (0.27–0.53) | 0.41 (0.32–0.51) | 0.42 | 6.88 (4.79–10.19) | 4.31 (3.11–5.17) | <0.001 |
| 45 | 0.38 (0.28–0.54) | 0.54 | 6.32 (4.46–9.30) | <0.001 | ||
| 50 | 0.38 (0.29–0.54) | 0.67 | 5.81 (4.22–8.59) | <0.001 | ||
| 55 | 0.38 (0.30–0.54) | 0.79 | 5.28 (3.98–7.76) | <0.001 | ||
| 60 | 0.38 (0.30–0.54) | 0.85 | 4.82 (3.79–7.35) | 0.006 | ||
| 70 | 0.41 (0.33–0.52) | 0.76 | 4.41 (3.64–6.45) | 0.054 | ||
| 80 | 0.45 (0.36–0.55) | 0.12 | 3.78 (3.13–5.23) | 0.788 | ||
| 90 | 0.47 (0.37–0.60) | 0.02 | 3.30 (2.65–4.24) | 0.014 | ||
| 100 | 0.50 (0.38–0.63) | 0.003 | 2.96 (2.21–3.56) | <0.001 | ||
| 110 | 0.52 (0.40–0.63) | <0.001 | 2.72 (1.87–3.21) | <0.001 | ||
| 130 | 0.55 (0.42–0.67) | <0.001 | 2.26 (1.51–2.67) | <0.001 | ||
| 150 | 0.57 (0.45–0.66) | <0.001 | 1.96 (1.26–2.48) | <0.001 | ||
| 170 | 0.57 (0.46–0.68) | <0.001 | 1.88 (1.11–2.36) | <0.001 | ||
| 190 | 0.58 (0.47–0.69) | <0.001 | 1.78 (1.02–2.22) | <0.001 | ||
| PCD-CT | EID-CT | |||||
|---|---|---|---|---|---|---|
| keV | Noise, HU | p-Value | Noise, HU | p-Value | ||
| BMI ≤ 23.9 kg/m2 | BMI > 23.9 kg/m2 | BMI ≤ 23.9 kg/m2 | BMI > 23.9 kg/m2 | |||
| 40 | 24.2 [22.4; 27.6] | 27.9 [24.5; 32.1] | 0.002 | 16.1 [14.2; 18.9] | 18.3 [15.5; 21.9] | 0.011 |
| 45 | 21.8 [20.1; 24.9] | 24.8 [21.6; 28.4] | 0.006 | |||
| 50 | 19.9 [18.2; 22.6] | 22.5 [19.6; 25.6] | 0.006 | |||
| 55 | 18.6 [16.4; 21.0] | 20.7 [17.9; 23.2] | 0.025 | |||
| 60 | 17.9 [15.2; 19.4] | 19.3 [16.4; 21.6] | 0.074 | |||
| 70 | 15.3 [13.1; 16.8] | 15.8 [14.1; 17.8] | 0.382 | |||
| 80 | 14.0 [12.3; 15.3] | 15.1 [13.4; 16.4] | 0.067 | |||
| 90 | 13.6 [11.9; 14.7] | 14.6 [12.9; 16.1] | 0.022 | |||
| 100 | 13.2 [11.7; 14.2] | 14.5 [12.9; 16.1] | 0.009 | |||
| 110 | 13.0 [11.6; 14.1] | 14.5 [12.9; 16.2] | 0.007 | |||
| 130 | 12.9 [11.4; 13.9] | 14.3 [12.8; 16.1] | 0.004 | |||
| 150 | 12.7 [11.4; 13.9] | 14.3 [12.7; 16.1] | 0.003 | |||
| 170 | 12.6 [11.3; 13.8] | 14.3 [12.7; 16.1] | 0.002 | |||
| 190 | 12.5 [11.3; 13.8] | 14.3 [12.7; 16.1] | 0.002 | |||
| PCD-CT | ||||||
|---|---|---|---|---|---|---|
| keV | Tumor-to-Liver Ratio (TLR) | p | Contrast-to-Noise Ratio (CNR) | p | ||
| BMI ≤ 23.9 | BMI > 23.9 | BMI ≤ 23.9 | BMI > 23.9 | |||
| 40 | 0.38 [0.28; 0.53] | 0.37 [0.26; 0.52] | 0.98 | 7.79 [4.92; 10.44] | 5.93 [4.70; 8.86] | 0.22 |
| 45 | 0.38 [0.29; 0.54] | 0.38 [0.27; 0.53] | 0.98 | 7.28 [4.56; 9.41] | 5.46 [4.40; 7.88] | 0.21 |
| 50 | 0.39 [0.30; 0.55] | 0.38 [0.29; 0.53] | 0.97 | 6.65 [4.31; 8.61] | 5.04 [4.13; 7.88] | 0.22 |
| 55 | 0.38 [0.30; 0.55] | 0.38 [0.30; 0.54] | 0.95 | 6.08 [4.18; 7.95] | 4.62 [3.86; 7.25] | 0.18 |
| 60 | 0.38 [0.29; 0.54] | 0.38 [0.30; 0.53] | 0.80 | 5.60 [4.11; 7.64] | 4.25 [3.64; 7.05] | 0.20 |
| 70 | 0.41 [0.30; 0.52] | 0.41 [0.33; 0.55] | 0.73 | 4.92 [3.79; 6.81] | 3.98 [3.55; 6.33] | 0.18 |
| 80 | 0.45 [0.33; 0.54] | 0.45 [0.38; 0.58] | 0.56 | 4.02 [3.41; 5.93] | 3.27 [2.85; 5.01] | 0.11 |
| 90 | 0.45 [0.35; 0.60] | 0.49 [0.39; 0.63] | 0.55 | 3.55 [2.83; 5.06] | 2.84 [2.32; 4.10] | 0.08 |
| 100 | 0.50 [0.38; 0.63] | 0.52 [0.40; 0.68] | 0.44 | 3.12 [2.23; 4.48] | 2.53 [2.00; 3.44] | 0.10 |
| 110 | 0.52 [0.40; 0.63] | 0.54 [0.43; 0.71] | 0.40 | 2.84 [2.03; 4.06] | 2.30 [1.75; 2.93] | 0.06 |
| 130 | 0.54 [0.42; 0.64] | 0.56 [0.47; 0.75] | 0.35 | 2.47 [1.83; 3.48] | 2.00 [1.33; 2.40] | 0.03 |
| 150 | 0.56 [0.44; 0.65] | 0.59 [0.50; 0.77] | 0.30 | 2.23 [1.65; 3.05] | 1.82 [1.06; 2.10] | 0.02 |
| 170 | 0.57 [0.45; 0.64] | 0.59 [0.52; 0.79] | 0.27 | 2.08 [1.53; 2.76] | 1.63 [0.89; 1.93] | 0.02 |
| 190 | 0.57 [0.46; 0.64] | 0.60 [0.53; 0.81] | 0.27 | 1.98 [1.45; 2.58] | 1.48 [0.77; 1.81] | 0.02 |
| EID-CT | ||||||
| Tumor-to-Liver Ratio (TLR) | p | Contrast-to-Noise Ratio (CNR) | p | |||
| BMI ≤ 23.9 | BMI > 23.9 | BMI ≤ 23.9 | BMI > 23.9 | |||
| 0.38 [0.30; 0.51] | 0.41 [0.35; 0.51] | 0.69 | 4.52 [3.96; 5.79] | 3.37 [2.76; 4.51] | 0.003 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bette, S.; Decker, J.A.; Braun, F.M.; Becker, J.; Haerting, M.; Haeckel, T.; Gebhard, M.; Risch, F.; Woźnicki, P.; Scheurig-Muenkler, C.; et al. Optimal Conspicuity of Liver Metastases in Virtual Monochromatic Imaging Reconstructions on a Novel Photon-Counting Detector CT—Effect of keV Settings and BMI. Diagnostics 2022, 12, 1231. https://doi.org/10.3390/diagnostics12051231
Bette S, Decker JA, Braun FM, Becker J, Haerting M, Haeckel T, Gebhard M, Risch F, Woźnicki P, Scheurig-Muenkler C, et al. Optimal Conspicuity of Liver Metastases in Virtual Monochromatic Imaging Reconstructions on a Novel Photon-Counting Detector CT—Effect of keV Settings and BMI. Diagnostics. 2022; 12(5):1231. https://doi.org/10.3390/diagnostics12051231
Chicago/Turabian StyleBette, Stefanie, Josua A. Decker, Franziska M. Braun, Judith Becker, Mark Haerting, Thomas Haeckel, Michael Gebhard, Franka Risch, Piotr Woźnicki, Christian Scheurig-Muenkler, and et al. 2022. "Optimal Conspicuity of Liver Metastases in Virtual Monochromatic Imaging Reconstructions on a Novel Photon-Counting Detector CT—Effect of keV Settings and BMI" Diagnostics 12, no. 5: 1231. https://doi.org/10.3390/diagnostics12051231
APA StyleBette, S., Decker, J. A., Braun, F. M., Becker, J., Haerting, M., Haeckel, T., Gebhard, M., Risch, F., Woźnicki, P., Scheurig-Muenkler, C., Kroencke, T. J., & Schwarz, F. (2022). Optimal Conspicuity of Liver Metastases in Virtual Monochromatic Imaging Reconstructions on a Novel Photon-Counting Detector CT—Effect of keV Settings and BMI. Diagnostics, 12(5), 1231. https://doi.org/10.3390/diagnostics12051231