
Impact of Three Different Algorithms for the Screening of SSc-PAH and Comparison with the Decisions of a Multidisciplinary Team

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Follow-Up
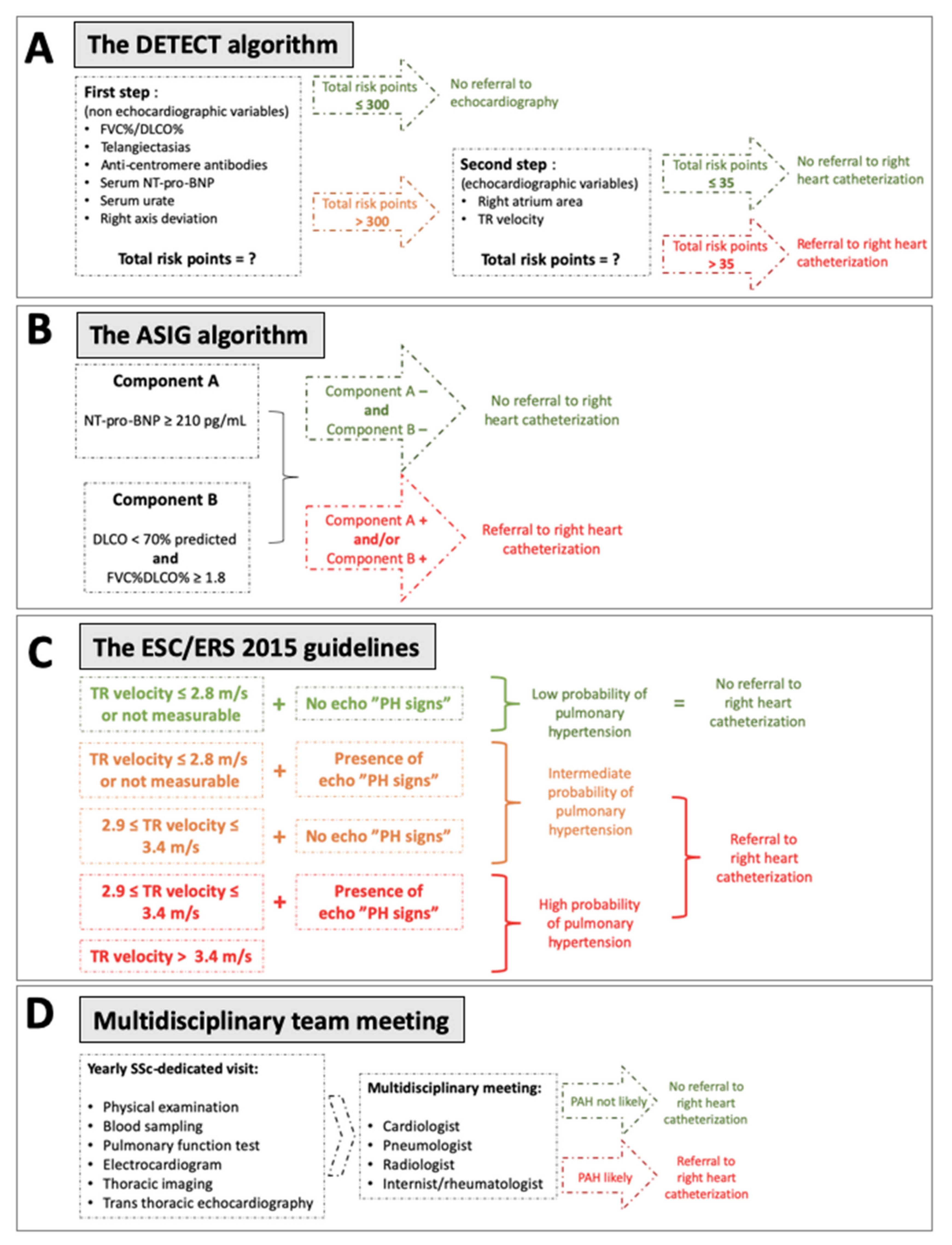
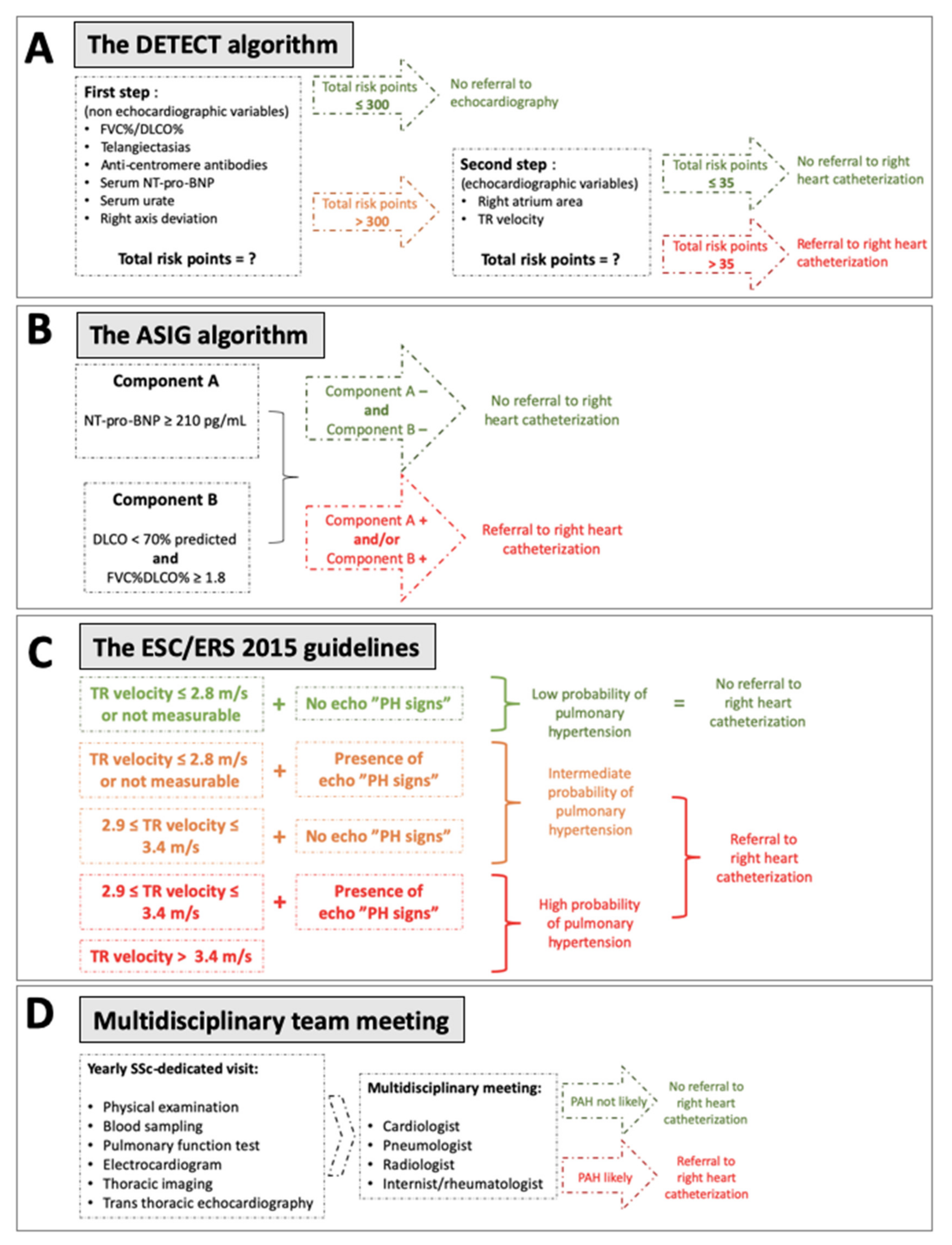
2.2. PAH Algorithms
2.3. Multidisciplinary Team (MDT)
2.4. PAH Definitions
2.5. Data Collection
2.6. Statistics
3. Results
3.1. Population Characteristics at Baseline
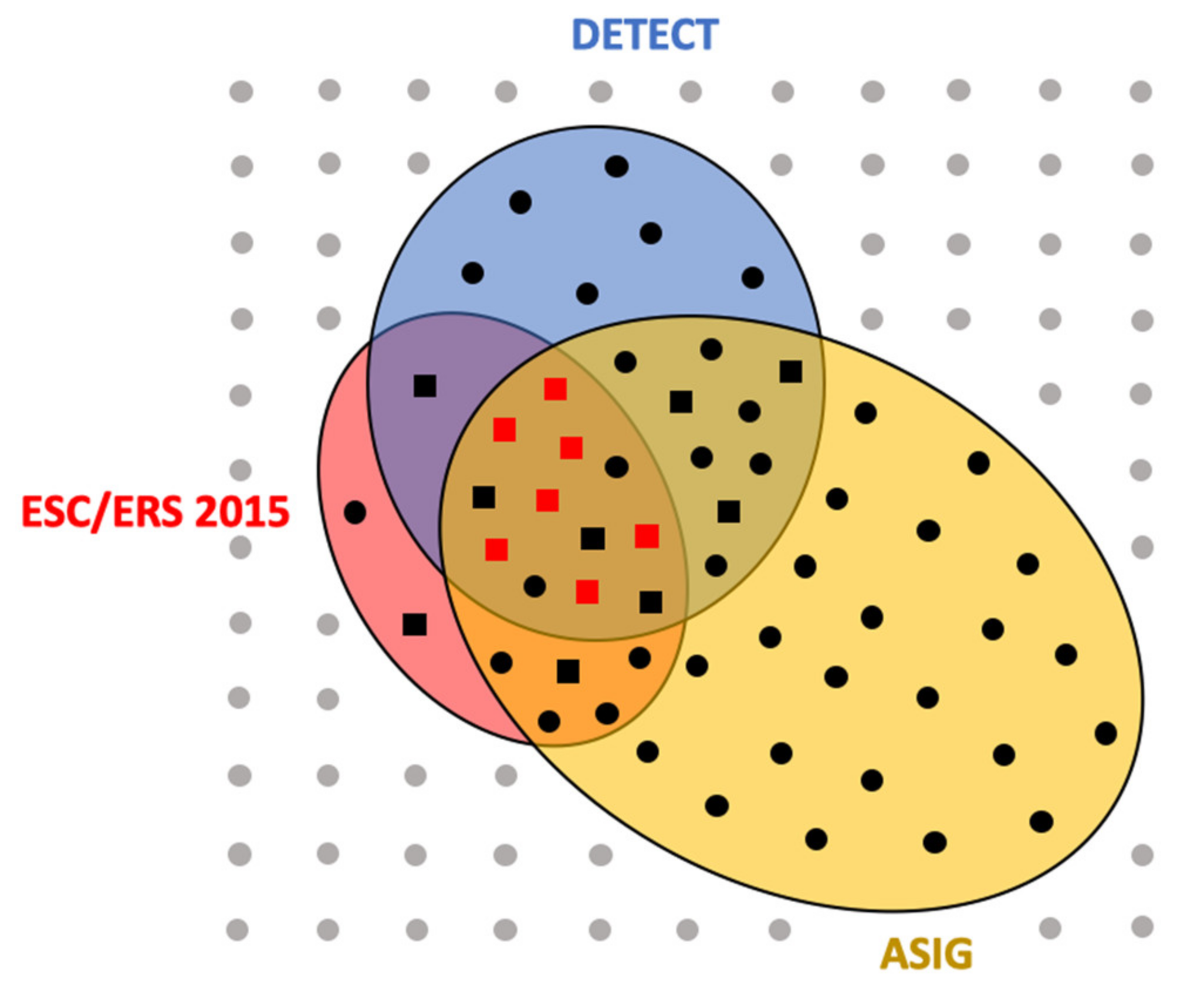
3.2. Recommendations According to Algorithms and MDT Based on Baseline Data
3.3. SSc-PAH Diagnosis
3.4. Three-Year Follow-Up
3.5. Impact of the New PH Definition
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Denton, C.P.; Khanna, D. Systemic sclerosis. Lancet 2017, 390, 1685–1699. [Google Scholar] [CrossRef]
- Ciprandi, G.; Murdaca, G.; Colombo, B.M.; De Amici, M.; Marseglia, G.L. Serum vascular endothelial growth factor in allergic rhinitis and systemic lupus erythematosus. Hum. Immunol. 2008, 69, 510–512. [Google Scholar] [CrossRef] [PubMed]
- Murdaca, G.; Colombo, B.M.; Puppo, F. The role of Th17 lymphocytes in the autoimmune and chronic inflammatory diseases. Intern. Emerg. Med. 2011, 6, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Costa, P.; Rusconi, S.; Mavilio, D.; Fogli, M.; Murdaca, G.; Pende, D.; Mingari, M.C.; Galli, M.; Moretta, L.; De Maria, A. Differential disappearance of inhibitory natural killer cell receptors during HAART and possible impairment of HIV-1-specific CD8 cytotoxic T lymphocytes. AIDS 2001, 15, 965–974. [Google Scholar] [CrossRef]
- Steen, V.D.; Medsger, T.A. Changes in causes of death in systemic sclerosis, 1972–2002. Ann. Rheum. Dis. 2007, 66, 940–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyndall, A.J.; Bannert, B.; Vonk, M.; Airò, P.; Cozzi, F.; Carreira, P.E.; Bancel, D.F.; Allanore, Y.; Müller-Ladner, U.; Distler, O.; et al. Causes and risk factors for death in systemic sclerosis: A study from the EULAR Scleroderma Trials and Research (EUSTAR) database. Ann. Rheum. Dis. 2010, 69, 1809–1815. [Google Scholar] [CrossRef] [Green Version]
- Avouac, J.; Airò, P.; Meune, C.; Beretta, L.; Dieude, P.; Caramaschi, P.; Tiev, K.; Cappelli, S.; Diot, E.; Vacca, A.; et al. Prevalence of Pulmonary Hypertension in Systemic Sclerosis in European Caucasians and Metaanalysis of 5 Studies. J. Rheumatol. 2010, 37, 2290–2298. [Google Scholar] [CrossRef] [PubMed]
- Morrisroe, K.; the Australian Scleroderma Interest Group (ASIG); Stevens, W.; Sahhar, J.; Rabusa, C.; Nikpour, M.; Proudman, S. Epidemiology and disease characteristics of systemic sclerosis-related pulmonary arterial hypertension: Results from a real-life screening programme. Arthritis Res. 2017, 19, 42. [Google Scholar] [CrossRef] [Green Version]
- Strange, G.; Gabbay, E.; Kermeen, F.; Williams, T.; Carrington, M.J.; Stewart, S.; Keogh, A. Time from Symptoms to Definitive Diagnosis of Idiopathic Pulmonary Arterial Hypertension: The Delay Study. Pulm. Circ. 2013, 3, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Humbert, M.; Yaici, A.; de Groote, P.; Montani, D.; Sitbon, O.; Launay, D.; Gressin, V.; Guillevin, L.; Clerson, P.; Simonneau, G.; et al. Screening for pulmonary arterial hypertension in patients with systemic sclerosis: Clinical characteristics at diagnosis and long-term survival. Arthritis Rheum. 2011, 63, 3522–3530. [Google Scholar] [CrossRef]
- Chung, L.; Domsic, R.T.; Lingala, B.; Alkassab, F.; Bolster, M.; Csuka, M.E.; Derk, C.; Fischer, A.; Frech, T.; Furst, D.E.; et al. Survival and Predictors of Mortality in Systemic Sclerosis-Associated Pulmonary Arterial Hypertension: Outcomes from the Pulmonary Hypertension Assessment and Recognition of Outcomes in Scleroderma Registry. Arthritis Rheum. 2013, 66, 489–495. [Google Scholar] [CrossRef] [Green Version]
- Kiely, D.G.; Lawrie, A.; Humbert, M. Screening strategies for pulmonary arterial hypertension. Eur. Heart J. Suppl. 2019, 21, K9–K20. [Google Scholar] [CrossRef] [Green Version]
- Hachulla, E.; Gressin, V.; Guillevin, L.; Carpentier, P.; Diot, E.; Sibilia, J.; Kahan, A.; Cabane, J.; Francès, C.; Launay, D.; et al. Early detection of pulmonary arterial hypertension in systemic sclerosis: A French nationwide prospective multicenter study. Arthritis Rheum. 2005, 52, 3792–3800. [Google Scholar] [CrossRef]
- Coghlan, J.G.; Denton, C.P.; Grünig, E.; Bonderman, D.; Distler, O.; Khanna, D.; Müller-Ladner, U.; E Pope, J.; Vonk, M.C.; Doelberg, M.; et al. Evidence-based detection of pulmonary arterial hypertension in systemic sclerosis: The DETECT study. Ann. Rheum. Dis. 2014, 73, 1340–1349. [Google Scholar] [CrossRef] [Green Version]
- Galiè, N.; Humbert, M.; Vachiéry, J.-L.; Gibbs, S.; Lang, I.M.; Kaminski, K.A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2015, 37, 67–119. [Google Scholar] [CrossRef]
- Simonneau, G.; Montani, D.; Celermajer, D.; Denton, C.P.; Gatzoulis, M.A.; Krowka, M.; Williams, P.G.; Souza, R. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801913. [Google Scholar] [CrossRef]
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef] [PubMed]
- Leroy, E.C.; Medsger, T.A. Criteria for the classification of early systemic sclerosis. J. Rheumatol. 2001, 28, 1573–1576. [Google Scholar] [PubMed]
- Thakkar, V.; Stevens, W.M.; Prior, D.; A Moore, O.; Byron, J.; Liew, D.; Patterson, K.; Hissaria, P.; Roddy, J.; Zochling, J.; et al. N-terminal pro-brain natriuretic peptide in a novel screening algorithm for pulmonary arterial hypertension in systemic sclerosis: A case-control study. Arthritis Res. Ther. 2012, 14, R143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Home. Available online: https://detect-pah.com/ (accessed on 21 March 2020).
- Hachulla, P.E.; Mouthon, P.L. Ce PNDS a été Actualisé sous la Coordination des; Haute Autorité de Santé: Saint-Denis, France, 2017; p. 140. [Google Scholar]
- Coirier, V.; Lescoat, A.; Fournet, M.; Cazalets, C.; Coiffier, G.; Jouneau, S.; Chabanne, C.; Jégo, P. Dépistage de l’hypertension artérielle pulmonaire au cours de la sclérodermie systémique: Comparaison de l’algorithme DETECT à une discussion pluridisciplinaire en centre de compétence. Rev. Med. Interne 2017, 38, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American College of Rheumatology/European League against Rheumatism collaborative initiative. Arthritis. Rheum. 2013, 65, 2737–2747. [Google Scholar] [CrossRef] [Green Version]
- Hoeper, M.M.; Lee, S.H.; Voswinckel, R.; Palazzini, M.; Jais, X.; Marinelli, A.; Barst, R.J.; Ghofrani, A.; Jing, Z.-C.; Opitz, C.; et al. Complications of Right Heart Catheterization Procedures in Patients with Pulmonary Hypertension in Experienced Centers. J. Am. Coll. Cardiol. 2006, 48, 2546–2552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandecasteele, E.; Drieghe, B.; Melsens, K.; Thevissen, K.; De Pauw, M.; Deschepper, E.; Decuman, S.; Bonroy, C.; Piette, Y.; De Keyser, F.; et al. Screening for pulmonary arterial hypertension in an unselected prospective systemic sclerosis cohort. Eur. Respir. J. 2017, 49, 1602275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hao, Y.; Thakkar, V.; Stevens, W.; Morrisroe, K.; Prior, D.; Rabusa, C.; Youssef, P.; Gabbay, E.; Roddy, J.; Walker, J.; et al. A comparison of the predictive accuracy of three screening models for pulmonary arterial hypertension in systemic sclerosis. Arthritis Res. Ther. 2015, 17, 7. [Google Scholar] [CrossRef] [Green Version]
- Young, A.; Moles, V.M.; Jaafar, S.; Visovatti, S.; Huang, S.; Vummidi, D.; Nagaraja, V.; McLaughlin, V.; Khanna, D. Performance of the DETECT Algorithm for Pulmonary Hypertension Screening in a Systemic Sclerosis Cohort. Arthritis Rheumatol. 2021, 73, 1731–1737. [Google Scholar] [CrossRef] [PubMed]
- Castillo, A.G.-D.; Callejas-Moraga, E.L.; García, G.; Rodríguez-Palomares, J.F.; Román, A.; Berastegui, C.; López-Meseguer, M.; Domingo, E.; Fonollosa-Plá, V.; Simeón-Aznar, C.P. High sensitivity and negative predictive value of the DETECT algorithm for an early diagnosis of pulmonary arterial hypertension in systemic sclerosis: Application in a single center. Arthritis Res. 2017, 19, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valerio, C.J.; Schreiber, B.E.; Handler, C.E.; Denton, C.P.; Coghlan, J.G. Borderline Mean Pulmonary Artery Pressure in Patients with Systemic Sclerosis: Transpulmonary Gradient Predicts Risk of Developing Pulmonary Hypertension. Arthritis Rheum. 2013, 65, 1074–1084. [Google Scholar] [CrossRef]
- Bae, S.; Saggar, R.; Bolster, M.B.; Chung, L.; Csuka, M.E.; Derk, C.; Domsic, R.; Fischer, A.; Frech, T.; Goldberg, A.; et al. Baseline characteristics and follow-up in patients with normal haemodynamics versus borderline mean pulmonary arterial pressure in systemic sclerosis: Results from the PHAROS registry. Ann. Rheum. Dis. 2012, 71, 1335–1342. [Google Scholar] [CrossRef]
- Maron, B.A.; Hess, E.; Maddox, T.M.; Opotowsky, A.R.; Tedford, R.J.; Lahm, T.; Joynt, K.E.; Kass, D.J.; Stephens, T.; Stanislawski, M.; et al. Association of Borderline Pulmonary Hypertension with Mortality and Hospitalization in a Large Patient Cohort: Insights from the Veterans Affairs Clinical Assessment, Reporting, and Tracking Program. Circulation 2016, 133, 1240–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann-Vold, A.-M.; Fretheim, H.; Midtvedt, Ø.; Kilian, K.; Angelshaug, M.; Chaudhary, A.; Gunnarsson, R.; Brunborg, C.; Garen, T.; Andreassen, A.K.; et al. Frequencies of borderline pulmonary hypertension before and after the DETECT algorithm: Results from a prospective systemic sclerosis cohort. Rheumatology 2018, 57, 480–487. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, G.; Berghold, A.; Scheidl, S.; Olschewski, H. Pulmonary arterial pressure during rest and exercise in healthy subjects: A systematic review. Eur. Respir. J. 2009, 34, 888–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaafar, S.; Visovatti, S.; Young, A.; Huang, S.; Cronin, P.; Vummidi, D.; McLaughlin, V.; Khanna, D. Impact of the revised haemodynamic definition on the diagnosis of pulmonary hypertension in patients with systemic sclerosis. Eur. Respir. J. 2019, 54, 1900586. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, G.; Olschewski, H. Debating the new haemodynamic definition of pulmonary hypertension: Much ado about nothing? Eur. Respir. J. 2019, 54, 1901278. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.A.; Brittain, E.L.; Hess, E.; Waldo, S.W.; E Barón, A.; Huang, S.; Goldstein, R.H.; Assad, T.; Wertheim, B.M.; Alba, G.A.; et al. Pulmonary vascular resistance and clinical outcomes in patients with pulmonary hypertension: A retrospective cohort study. Lancet Respir. Med. 2020, 8, 873–884. [Google Scholar] [CrossRef]
- Kowal-Bielecka, O.; Fransen, J.; Avouac, J.; Becker, M.; Kulak, A.; Allanore, Y.; Distler, O.; Clements, P.J.; Cutolo, M.; Czirjak, L.; et al. Update of EULAR recommendations for the treatment of systemic sclerosis. Ann. Rheum. Dis. 2017, 76, 1327–1339. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| n (%) or Median (IQR) | Baseline (n = 117) | End of FU (n = 99) |
|---|---|---|
| Age at diagnosis (years old) | 55 (46–66) | 54 (46–63) |
| Disease duration (years) | 6 (3–11) | 9 (6–15) |
| Sex ratio | 0.3 | 0.29 |
| ACR/EULAR 2013 criteria | 105 (90%) | 89 (90%) |
| Telangiectasia | 83 (71%) | 67 (68%) |
| Right axis deviation on ECG | 8 (7%) | 5 (5%) |
| Positive anti-centromere antibody | 65 (56%) | 56 (57%) |
| NT-pro-BNP (pg/mL) | 94 (50–164) | 103 (59–173) |
| Serum urate (mmol/L) | 274 (238–357) | 270 (224–345) |
| DLCO (% of predicted value) | 64 (52–72) | 63 (53–72) |
| FVC/DLCO ratio | 1.68 (1.44–1.86) | 1.63 (1.41–1.84) |
| Interstitial lung disease | 46 (39%) | 40 (40%) |
| Estimated sPAP (mmHg) | 25 (20–30) | 30 (26–35) |
| Right atrium surface (cm2) | 14 (12–16) | 13 (12–15) |
| Death during the study period | 10/117 (9%) |
| n (%) or Median (IQR) | DETECT + n = 28/117 | ESC 2015 + n = 20/117 | ASIG + n = 48/117 | MDT Decision + n = 16/117 | p-Value |
|---|---|---|---|---|---|
| Age at diagnosis | 56 (47–65) | 64 (53–70) | 64 (54–68) | 64 (53–70) | 0.297 |
| Disease duration | 9 (6–14) | 9 (4–19) | 6 (4–13) | 7 (4–19) | 0.562 |
| Sex ratio | 0.22 | 0.43 | 0.37 | 0.23 | 0.786 |
| ACR/EULAR 2013 criteria (n [%]) | 27 (96%) | 19 (95%) | 45 (94%) | 15 (94%) | 0.970 |
| Telangiectasia (n [%]) | 27 (96%) | 19 (95%) | 40 (83%) | 15 (94%) | 0.213 |
| Right axis deviation on ECG | 4 (14%) | 4 (20%) | 5 (10%) | 3 (19%) | 0.757 |
| Anti-centromere antibody (n [%]) | 15 (54%) | 12 (60%) | 26 (54%) | 8 (50%) | 0.944 |
| NT-pro-BNP (pg/mL) | 137 (97–390) | 318 (126–705) | 240 (77–497) | 323 (101–1125) | 0.361 |
| Serum urate (mmol/L) | 297 (241–416) | 354 (297–476) | 297 (238–416) | 357 (297–520) | 0.081 |
| DLCO (% of predicted value) | 50 (32–55) | 47 (30–64) | 53 (40–64) | 39 (30–57) | 0.178 |
| FVC (% of predicted value) | 93 (79–107) | 90 (77–101) | 98 (82–116) | 90 (79–101) | 0.160 |
| FVC/DLCO ratio | 2.12 (1.73–2.52) | 2.16 (1.53–2.62) | 2.02 (1.81–2.40) | 2.28 (1.70–2.62) | 0.744 |
| Interstitial lung disease on HRCT (n [%]) | 15 (54%) | 9 (45%) | 19 (40%) | 9 (56%) | 0.553 |
| Tricuspid regurgitation velocity(m/s) | 2.8 (2.6–3.2) | 3.1 (2.9–3.4) | 2.8 (2.5–3) | 3.2 (2.9–3.4) | 0.002 * |
| Estimated sPAP (mmHg) | 35 (25–48) | 45 (38–50) | 30 (25–44) | 47 (36–50) | 0.002 * |
| Right atrium surface (cm2) | 15 (12–19) | 16 (14–21) | 14 (12–19) | 17 (14–22) | 0.194 |
| DETECT + | 28 (100%) | 13 (65%) | 21 (44%) | 14 (88%) | NA |
| ASIG + | 21 (75%) | 17 (85%) | 48 (100%) | 14 (88%) | NA |
| ESC 2015 + | 13 (46%) | 20 (100%) | 17 (35%) | 13 (81%) | NA |
| MDT decision + | 14 (50%) | 13 (65%) | 14 (29%) | 16 (100%) | NA |
| n (%) or Median (IQR) | SSc-PAH + n = 7 | SSc-PAH − n = 9 | p-Value |
|---|---|---|---|
| Age at diagnosis | 62 (51–67) | 65 (53–73) | p = 0.668 |
| Disease duration | 11 (6–20) | 5 (4–14) | p = 0.235 |
| Sex ratio (M/F) | 0 | 0.5 | p = 0.192 |
| ACR/EULAR 2013 criteria (n [%]) | 7 (100%) | 8 (89%) | p = 1.000 |
| Telangiectasia (n [%]) | 7 (100%) | 8 (89%) | p = 1.000 |
| Right axis on electrocardiogram | 2 (29%) | 1 (11%) | p = 0.550 |
| Anti-centromere antibody (n [%]) | 6 (86%) | 2 (22%) | p = 0.041 * |
| NT-pro-BNP (pg/mL) | 700 (240–1834) | 122 (71–858) | p = 0.174 |
| Serum urate (mmol/L) | 476 (268–773) | 333 (297–470) | p = 0.483 |
| WHO-functional classification | 3 (2–3) | 2 (2–3) | p = 0.215 |
| DLCO (% of predicted value) | 31 (28–38) | 54 (38–61) | p = 0.071 |
| FVC (% of predicted value) | 82 (69–102) | 90 (81–102) | p = 0.607 |
| FVC/DLCO ratio | 2.63 (2.23–2.93) | 2.07 (1.43–2.42) | p = 0.012 * |
| Interstitial lung disease (n [%]) | 2 (29%) | 7 (78%) | p = 0.126 |
| Tricuspid regurgitation velocity(m/s) | 3.2 (3.0–3.6) | 3.0 (2.6–3.3) | p = 0.208 |
| Estimated sPAP (mmHg) | 50 (40–65) | 40 (26–49) | p = 0.073 |
| Right atrium surface (cm2) | 19 (16–28) | 15 (14–20) | p = 0.072 |
| TAPSE (mm) | 18 (16–24) | 21 (16–22) | p = 0.940 |
| Tricuspid S wave (cm/s) | 12 (10–15) | 14 (10–16) | p = 0.691 |
| LVEF (%) | 65 (60–65) | 65 (60–70) | p = 1.000 |
| 6MWD (m) | 336 (247–501) | 444 (419–523) | p = 0.295 |
| Pulse oximetry before 6MWT (%) | 98 (96–99) | 99 (98–100) | p = 0.304 |
| Pulse oximetry after 6MWT (%) | 88 (79–93) | 96 (91–98) | p = 0.067 |
| DETECT + | 7 (100%) | 7 (78%) | NA |
| ASIG + | 7 (100%) | 7 (78%) | NA |
| ESC 2015 + | 7 (100%) | 6 (67%) | NA |
| Mean pulmonary arterial pressure (mmHg) | 32 (28–39) | 18 (18–23) | p = 0.002 * |
| Pulmonary capillary wedge pressure (mmHg) | 11 (4–12) | 9 (6–13) | p = 0.865 |
| Pulmonary vascular resistance (WU) | 6.0 (1.9–7.5) | 1.5 (1.2–2.2) | p = 0.016 * |
| Cardiac output (L/min) | 5.1 (4.0–7.4) | 7.1 (5.4–9.1) | p = 0.095 |
| Cardiac index (L/min/m2) | 3.2 (2.1–4.3) | 4.1 (3.2–4.3) | p = 0.350 |
| PH group I | 7 (100%) | 0 | NA |
| PH group II | 0 | 2 (22%) | NA |
| PH group III | 0 | 0 | NA |
| PH group IV | 0 | 0 | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coirier, V.; Chabanne, C.; Jouneau, S.; Belhomme, N.; Ballerie, A.; Cazalets, C.; Sobanski, V.; Hachulla, É.; Jégo, P.; Lescoat, A. Impact of Three Different Algorithms for the Screening of SSc-PAH and Comparison with the Decisions of a Multidisciplinary Team. Diagnostics 2021, 11, 1738. https://doi.org/10.3390/diagnostics11101738
Coirier V, Chabanne C, Jouneau S, Belhomme N, Ballerie A, Cazalets C, Sobanski V, Hachulla É, Jégo P, Lescoat A. Impact of Three Different Algorithms for the Screening of SSc-PAH and Comparison with the Decisions of a Multidisciplinary Team. Diagnostics. 2021; 11(10):1738. https://doi.org/10.3390/diagnostics11101738
Chicago/Turabian StyleCoirier, Valentin, Céline Chabanne, Stéphane Jouneau, Nicolas Belhomme, Alice Ballerie, Claire Cazalets, Vincent Sobanski, Éric Hachulla, Patrick Jégo, and Alain Lescoat. 2021. "Impact of Three Different Algorithms for the Screening of SSc-PAH and Comparison with the Decisions of a Multidisciplinary Team" Diagnostics 11, no. 10: 1738. https://doi.org/10.3390/diagnostics11101738
APA StyleCoirier, V., Chabanne, C., Jouneau, S., Belhomme, N., Ballerie, A., Cazalets, C., Sobanski, V., Hachulla, É., Jégo, P., & Lescoat, A. (2021). Impact of Three Different Algorithms for the Screening of SSc-PAH and Comparison with the Decisions of a Multidisciplinary Team. Diagnostics, 11(10), 1738. https://doi.org/10.3390/diagnostics11101738