Abstract
Photodynamic therapy (PDT) using indocyanine green (ICG) has gained attention as an adjunctive treatment for periodontitis due to its antimicrobial and anti-inflammatory properties and its ability to penetrate deep periodontal tissues via near-infrared light activation. We aimed to evaluate the clinical and microbiological efficacy of ICG-mediated PDT as an adjunct to conventional periodontal therapy in patients with periodontitis based on data from randomized controlled trials (RCTs). A systematic search of PubMed, Embase, Scopus, and the Cochrane Library was conducted to identify randomized controlled trials (RCTs) exclusively investigating ICG-PDT in periodontitis based on predefined eligibility criteria. Studies were selected based on predefined inclusion criteria, and methodological quality was assessed using a 14-point scoring system. Data were extracted on clinical outcomes (e.g., probing depth, clinical attachment level) and microbiological changes. Sixteen RCTs met the inclusion criteria. Most studies reported improvements in probing depth, clinical attachment level, and microbial reduction following ICG-aPDT; however, some trials found no significant differences compared to control groups. These discrepancies may be attributable to variations in laser settings, ICG concentration, treatment frequency, or initial disease severity. Microbiological benefits included significant reductions in key periodontal pathogens. The therapy was well tolerated, with no adverse effects reported. However, variability in treatment protocols and limited long-term follow-up restricted the ability to draw definitive conclusions. ICG-mediated PDT is a promising, safe, and effective adjunct in periodontal therapy. Future trials should aim for protocol standardization and long-term outcome assessment to strengthen clinical guidance.
1. Introduction
Periodontitis is a prevalent chronic inflammatory disease that affects the supporting structures of the teeth, including the periodontal ligament, cementum, and alveolar bone [1,2,3]. If left untreated, periodontitis leads to progressive tissue destruction, tooth mobility, and ultimately, tooth loss [3]. Beyond its impact on oral health, periodontitis has been increasingly linked to a range of systemic conditions, including cardiovascular diseases, diabetes mellitus, respiratory diseases, and adverse pregnancy outcomes, highlighting the importance of effective management strategies [4,5,6]. The primary etiological factor in periodontitis is the presence of a complex polymicrobial biofilm on the tooth surface and within periodontal pockets [7]. Conventional periodontal therapy, particularly scaling and root planing (SRP), remains the gold standard for mechanical disruption and removal of subgingival biofilms and calculus deposits [8,9]. However, mechanical instrumentation alone may not always achieve complete eradication of pathogenic bacteria, particularly in deep or anatomically complex periodontal pockets, furcation areas, and root concavities [10]. Residual bacterial load can contribute to persistent inflammation, disease progression, and compromised treatment outcomes [11]. In response to these limitations, adjunctive antimicrobial therapies have been explored to enhance periodontal treatment efficacy [12]. Systemic and local antibiotics have demonstrated adjunctive benefits; however, concerns regarding antibiotic resistance, allergic reactions, and disruption of the commensal microbiota have driven interest in alternative non-antibiotic antimicrobial strategies [13]. Photodynamic therapy (PDT) has emerged as a promising adjunctive modality in this context, offering targeted antimicrobial effects with minimal systemic impact and a low risk of developing resistance [14]. PDT involves the application of a photosensitizing agent, which preferentially accumulates in bacterial cells [15]. Upon activation by light of a specific wavelength, the photosensitizer undergoes a photochemical reaction, generating reactive oxygen species (ROS), such as singlet oxygen and free radicals [16]. ROS exert potent cytotoxic effects, leading to bacterial cell wall disruption, membrane damage, and ultimately bacterial cell death [17]. Importantly, PDT can also modulate the host immune response and reduce local inflammation, potentially contributing to enhanced periodontal healing. Among the various photosensitizers investigated for periodontal applications, indocyanine green (ICG) has garnered increasing attention [18,19]. ICG is a water-soluble tricarbocyanine dye approved by the U.S. Food and Drug Administration (FDA) for clinical use in medical imaging [20,21]. It exhibits favorable properties for photodynamic applications, including high photostability, low toxicity, and strong absorption of near-infrared (NIR) light around 800 nm [22]. The use of NIR light allows for deeper tissue penetration compared to visible light wavelengths, which may enable more effective targeting of subgingival pathogens located within periodontal pockets and tissues [23]. Recent studies have explored the potential of ICG-mediated PDT as an adjunct to SRP in the treatment of periodontitis [24]. Given the growing interest in PDT and the need for evidence-based guidance on its clinical application, a comprehensive synthesis of the current literature is warranted. This systematic review aims to critically evaluate and summarize the available evidence from randomized controlled trials investigating the use of indocyanine green as a photosensitizer in periodontal therapy. Specifically, it seeks to assess the effectiveness of ICG-mediated PDT in reducing bacterial load and improving periodontal outcomes compared to conventional treatments or other photosensitizers. By systematically analyzing the methodological quality, treatment protocols, and clinical outcomes reported in the included studies, this review aims to clarify the role of ICG-PDT in the contemporary management of periodontitis and identify directions for future research.
2. Materials and Methods
2.1. Focused Question
The systematic review was designed based on the PICO framework [25], structured to address the following question: In patients with periodontitis (Population), does treatment involving indocyanine green (ICG)-mediated photodynamic therapy (Intervention), compared to conventional periodontal therapies, alternative photosensitizers, or standard care without photodynamic treatment (Comparison), lead to greater improvements in bacterial reduction and periodontal outcomes (Outcome)?
2.2. Search Strategy
This systematic review, registered in PROSPERO (ID: CRD420251040973), was conducted in accordance with the PRISMA 2020 guidelines to ensure transparent and systematic reporting [26]. A comprehensive literature search was performed across major databases, PubMed/Medline, Embase, Scopus, and the Cochrane Library, to identify randomized controlled trials (RCTs) evaluating the use of indocyanine green as a photosensitizer in the treatment of periodontitis (Table 1). The complete search strategy is illustrated in Figure 1. Three independent reviewers executed the database queries using a predefined set of search terms focused on periodontitis management and photodynamic therapy with ICG. Studies were limited to those published in English, with no restrictions on publication date. The study selection process involved initial screening of titles and abstracts based on eligibility criteria (outlined in Table 2), followed by independent full-text reviews conducted by two reviewers. A snowballing method was also employed, screening the reference lists of included studies to identify any additional relevant trials. The final search was conducted on 15 March 2025 and included studies published from 1 January 2015 to 15 March 2025.

Table 1.
Search syntax used in the study.
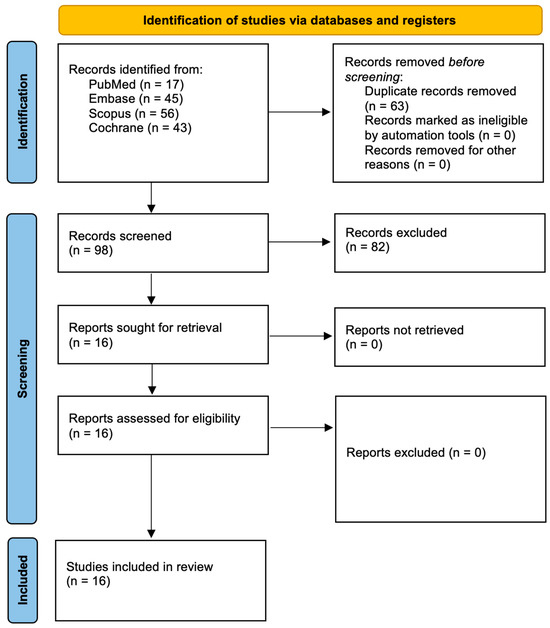
Figure 1.
PRISMA 2020 flow diagram.
Table 2.
Selection criteria used in the study.
2.3. Study Selection Process
To uphold methodological rigor and reduce potential bias, all retrieved records were subjected to a structured, independent screening process by multiple reviewers. Titles and abstracts were carefully assessed against predefined inclusion criteria. Any discrepancies in study selection were resolved through discussion to ensure consistency in decision-making. The eligibility criteria were specifically tailored to capture high-quality randomized controlled trials evaluating the antimicrobial effectiveness of indocyanine green-mediated photodynamic therapy in the treatment of periodontitis.
2.4. Risk of Bias in Individual Studies
To ensure objectivity and minimize the risk of selection bias, the initial screening of titles and abstracts identified through the search strategy was performed independently by multiple reviewers. Inter-rater agreement was assessed using Cohen’s kappa coefficient, providing a quantitative measure of consistency between reviewers [27]. In cases where discrepancies arose regarding study eligibility, they were resolved through structured discussion until full consensus was reached. This systematic and transparent approach was implemented to uphold the methodological rigor of the review and guarantee the accurate identification of relevant randomized controlled trials.
2.5. Quality Assessment
The methodological quality of the included studies was independently assessed by three reviewers, focusing on key elements related to the design, execution, and reporting of indocyanine green (ICG)-mediated photodynamic therapy (PDT) interventions. A structured scoring system was employed to evaluate risk of bias, assigning 1 point for each criterion met (“yes”) and 0 points for unmet items (“no”), across fourteen predefined domains: (1) clear reporting of ICG preparation and concentration (e.g., dye concentration, solvent, stability); (2) identification of the light source used for activation (e.g., diode laser, LED, specific manufacturer); (3) comprehensive description of the irradiation protocol, including light parameters (wavelength, power output, energy density), exposure time, and treatment area; (4) provision of full technical specifications of the light delivery system (spot size, continuous or pulsed mode, energy fluence); (5) confirmation of photosensitizer–light interaction (e.g., timing between ICG application and light exposure, verification of dye uptake); (6) inclusion of an appropriate control group (e.g., scaling and root planing only, placebo, light, or ICG alone); (7) use of valid statistical analysis for clinical (e.g., probing depth, clinical attachment level) and/or microbiological outcomes; (8) transparent outcome reporting without selective reporting or missing outcome data; (9) disclosure of conflicts of interest and funding sources; (10) randomization process (e.g., method of random sequence generation, allocation concealment); (11) lack of deviations from intended interventions (e.g., compliance with assigned interventions, blinding of participants and personnel); (12) no missing outcome data (e.g., incomplete follow-up, reasons for missing data); (13) no bias in measurement of the outcome (e.g., blinding of outcome assessors, objective outcome measurements); and (14) no bias in selection of the reported result (e.g., selective reporting of outcomes or analyses).
The scoring system was adapted from the Cochrane Risk of Bias Tool (RoB 2.0) and supplemented with technical criteria relevant to photodynamic therapy (e.g., light parameters, ICG concentration, and photosensitizer–light interaction), consistent with previous systematic reviews in dental laser therapy [28]. Each study was assigned a total score out of fourteen, and the risk of bias was categorized as high (0–5 points), moderate (6–10 points), or low (11–14 points). Discrepancies between reviewers were resolved by consensus or, if necessary, by consultation with a fourth reviewer. This evaluation process was conducted in accordance with the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions [28]. Table 3 shows the results of the quality assessment.
Table 3.
The results of the quality assessment and risk of bias across the studies.
2.6. Data Extraction
After reaching consensus on the final set of studies for inclusion, two reviewers independently performed data extraction following a predefined and standardized protocol to ensure consistency and minimize potential errors. Extracted data included essential study details such as the first author, year of publication, study design, characteristics of the participant population, descriptions of experimental and control groups, duration of follow-up (where applicable), and primary and secondary outcomes related to microbiological and periodontal measures. Special attention was given to detailed technical parameters of the indocyanine green-mediated photodynamic therapy, including the ICG concentration, light source specifications (wavelength, power output, energy density), method of application, and any adjunctive treatments combined with photodynamic therapy. Procedural aspects, such as treatment duration, irradiation technique, and frequency of application, were also systematically recorded to support comprehensive cross-study comparisons.
2.7. Study Selection
In accordance with the PRISMA 2020 guidelines, the process of study selection is outlined in Figure 1. The systematic search across multiple databases initially identified 161 records. After the removal of duplicates, 98 unique articles remained. Through screening of titles and abstracts, 16 studies were deemed potentially relevant and were selected for full-text review. All 16 studies met the inclusion criteria and were incorporated into the final analysis. These randomized controlled trials, all published within the last decade, specifically investigated the therapeutic efficacy of indocyanine green (ICG)-mediated photodynamic therapy in the management of periodontitis. Table 4 presents the geographical distribution of the included studies.
Table 4.
A geographic distribution of the included research.
3. Results
3.1. Data Presentation
The structured presentation of study data in Table 4, Table 5, Table 6 and Table 7 is intended to highlight key patterns across clinical and methodological variables. Emphasis is placed not only on outcome measures but also on contextual factors, such as geography, laser parameters, and photosensitizer characteristics, which may explain inter-study variability. Given the heterogeneity in healthcare systems, patient populations, and practice settings, geographical context is essential to understanding local feasibility and treatment outcomes. For instance, differences in clinical guidelines, availability of laser technology, and training may contribute to observed discrepancies in efficacy across countries. Presenting this data transparently enables better interpretation of generalizability and potential barriers to clinical implementation.
Table 5.
Summary of the principal results and study details.
Table 6.
Characteristics of the light source used.
Table 7.
Properties of ICG as a photosensitizer.
3.2. Overview of Study Characteristics
The geographic distribution of the included studies is not incidental; it reflects global research interest and application diversity of ICG-mediated photodynamic therapy. Studies were conducted across Europe, Asia, South America, and the Middle East, indicating broad international uptake. However, the concentration of trials in certain regions, such as India and Saudi Arabia, may influence outcomes due to differences in baseline disease prevalence, healthcare access, or operator expertise. By identifying where these studies originate, readers gain insight into both the potential applicability of findings across diverse populations and the need for further validation in underrepresented regions, such as North America and Africa. This geographic lens also helps policymakers and clinicians assess transferability to their local contexts.
3.3. Main Study Outcomes
Indocyanine green-mediated antimicrobial photodynamic therapy (ICG-aPDT) has shown varying degrees of clinical and microbiological effectiveness as an adjunct in periodontal treatment. Al-Momani et al. (2021) [29] demonstrated that ICG-aPDT significantly improved probing depth (PD), clinical attachment level (CAL), bleeding on probing (BOP), and inflammatory markers across diabetic and non-diabetic groups, with sustained benefits in non-diabetics and well-controlled type 2 diabetes mellitus (T2DM). Annunziata et al. (2023) [30] found that while both test and control groups improved following full-mouth ultrasonic debridement (FMUD), ICG-aPDT led to greater reductions in deep pocket PD and key pathogens, such as Aggregatibacter actinomycetemcomitans and Parvimonas micra. Similarly, Cetiner et al. (2024) [31] reported that adjunctive ICG-aPDT enhanced wound healing, reduced deep pocket depths, and promoted osteogenic marker expression following regenerative surgery. In maintenance patients, Chowdhury et al. (2024) [32] observed no significant benefit of ICG-aPDT over scaling and root planing (SRP) alone, whereas Costa et al. (2023) [33] found notable reductions in BOP and key pathogens despite no improvement in PD or CAL. Dalvi et al. (2019) [34] highlighted better healing and gingival outcomes with adjunctive ICG-aPDT after open flap debridement. Hayashi et al. (2023) [35] confirmed short-term bacterial reductions using transgingival ICG-aPDT, though effects were not sustained. Hill et al. (2019) [36] and Joshi et al. (2020) [37] both found modest or transient benefits, with Hill noting short-term fluid flow reduction and Joshi showing enhanced PD and CAL improvements. Monzavi et al. (2016) [38] reported significant inflammation reduction without attachment gain, while Niazi et al. (2020) [39] observed superior CAL and PD outcomes versus Salvadora persica gel or SRP alone, though BOP reduction was greater with herbal therapy. Qamar et al. (2021) [40] demonstrated ICG-aPDT’s superiority over Aloe vera gel in improving inflammatory markers and clinical parameters. Sethi et al. (2020) [41] noted strong antimicrobial effects and significant CAL/PD improvement without gingival recession. Shingnapurkar et al. (2017) [42] found enhanced relative attachment level (RAL) and PPD reduction, and Srikanth et al. (2015) [43] confirmed significantly greater CAL and PD improvements with ICG-aPDT compared to diode laser or SRP alone, with no tissue damage. Finally, Sukumar et al. (2020) [44,45,46] demonstrated consistent clinical and microbiological superiority of ICG-aPDT over SRP, including effective suppression of multiple pathogens, such as P. gingivalis and T. forsythia. These findings suggest that while clinical efficacy varies, ICG-aPDT is generally safe and may offer enhanced benefits in deep or inflamed pockets, particularly when repeated or combined with regenerative or surgical approaches.
Although several studies reported statistically significant reductions in probing depth ranging from 0.5 to 1.2 mm, only reductions ≥1.0 mm are generally considered clinically meaningful, particularly in pockets ≥5 mm [47,48,49,50,51]. Smaller improvements, while statistically significant, may not translate into tangible clinical benefit in routine practice. ICG-aPDT resulted in statistically significant PD reductions (typically 0.5–1.2 mm); however, in many studies, these changes fell below the threshold for clinical relevance (≥1.0 mm), particularly in shallow or maintenance-phase pockets. While many studies included in this review demonstrated statistically significant improvements in PD and clinical attachment level (CAL), the magnitude of change often remained modest. According to established periodontal treatment guidelines, clinically meaningful PD reductions typically start at ≥1.0 mm, especially in deep pockets (≥5 mm) [47,48,49]. Reductions below this threshold, though statistically significant, may have a limited impact on long-term periodontal stability or tooth retention. Therefore, future studies should clearly distinguish between statistical and clinical significance and report responder rates or pocket closure as more meaningful clinical endpoints [50,51].
3.4. Characteristics of Light Sources Used in PDT
Light source parameters are central to the effectiveness of photodynamic therapy and must be analyzed in detail to understand differences in clinical efficacy. While ICG has an optimal absorption peak around 800 nm, diode lasers used in the included studies varied in wavelength (from 808 to 970 nm), power output, irradiation mode (continuous vs. pulsed), and application time. These variations directly influence the generation of reactive oxygen species (ROS) and, consequently, bacterial kill rates and host tissue responses. Moreover, discrepancies in fluence and exposure duration may explain inconsistencies in short- and long-term outcomes. By explicitly summarizing these laser characteristics in Table 6, we provide a mechanistic rationale for treatment variability and highlight the pressing need for protocol standardization in future trials. Understanding these physical parameters is also crucial for clinicians seeking to replicate PDT protocols in real-world practice.
4. Discussion
4.1. Results in the Context of Other Evidence
ICG-aPDT has demonstrated significant clinical benefits as an adjunct to conventional periodontal treatments, notably improving probing depth (PD) reduction and clinical attachment level (CAL) gain in both surgical and non-surgical contexts [29,30,31,34,37]. Studies consistently report superior outcomes in deep periodontal pockets (≥6 mm) when ICG-aPDT is added to scaling and root planing (SRP), particularly in terms of PD reduction and a reduction in bleeding on probing (BOP) [30,31,33,36]. ICG-aPDT enhances antimicrobial efficacy, leading to substantial reductions in key periodontal pathogens such as P. gingivalis, A. actinomycetemcomitans, and T. forsythia in various clinical scenarios [29,30,33,39,43]. Its benefits extend to diabetic patients, where ICG-aPDT showed consistent efficacy in reducing inflammation and improving periodontal parameters, even in poorly controlled glycemic states [29]. The adjunctive use of ICG-aPDT post-regenerative surgery was associated with accelerated wound healing and increased expression of osteogenic markers, suggesting potential benefits for tissue regeneration [31]. Multiple applications of ICG-aPDT provided more pronounced clinical and microbiological improvements compared to single-use protocols, underlining the importance of treatment frequency [43]. Despite some studies finding no significant intergroup differences, ICG-aPDT was valued for its non-invasiveness, safety profile, and lack of reported adverse effects across all trials [32,35,36]. The antimicrobial effect of ICG-aPDT appears short-lived in some cases, emphasizing the need for standardized protocols and longer-term evaluations to optimize clinical outcomes [35,38]. Furthermore, ICG’s ability to perform effectively under hypoxic conditions within periodontal pockets positions it as a favorable photosensitizer compared to alternatives [29,33,39]. Overall, while heterogeneity in protocols limits broad generalizations, the evidence supports ICG-aPDT as a promising, safe, and effective adjunct in modern periodontal therapy [29,30,31,32,33,34,35,36,37,38,39,40,41,42,43].
The efficacy of ICG-mediated PDT is highly dependent on the characteristics of the light source used, particularly wavelength, power output, energy density, and exposure time. ICG exhibits peak absorption near 800 nm, making near-infrared (NIR) lasers or diode lasers ideal for optimal activation and deeper tissue penetration [25,26,27,28,29,30,31,32]. Studies suggest that light sources with lower power settings and continuous wave modes may reduce thermal effects while maintaining antimicrobial efficacy, whereas pulsed modes might enhance ROS generation without damaging host tissues [33,34,35]. Further comparative studies are warranted to determine the ideal light delivery parameters that maximize therapeutic outcomes while minimizing adverse effects. While most clinical trials to date have not stratified outcomes based on ethnicity, future investigations should consider potential differences in treatment response among diverse ethnic populations, given known genetic and immunologic variations that may influence periodontal disease progression and healing capacity [35,36,37,38,39,40,41,42,43]. Moreover, ICG-mediated PDT has shown broad-spectrum antimicrobial effects against several key periodontal pathogens, including P. gingivalis, A. actinomycetemcomitans, T. forsythia, and T. denticola. However, pathogen-specific susceptibility and resistance patterns should be further explored, as preliminary evidence suggests differential sensitivity to PDT across microbial species. Understanding these variations could support more personalized and effective antimicrobial strategies in periodontal care [35,36,37,38,39,40,41,42,43].
Photodynamic therapy (PDT) has emerged as a promising adjunctive modality for periodontal treatment, with indocyanine green (ICG) gaining significant attention as a photosensitizer in recent years [44]. Indocyanine green possesses several pharmacological properties that make it particularly suitable for periodontal photodynamic therapy [45,46]. As a water-soluble tricarbocyanine dye approved by the U.S. Food and Drug Administration for clinical use in medical imaging, ICG exhibits favorable characteristics including high photostability, low toxicity, and strong absorption of near-infrared light around 800 nm wavelength [47,48]. These properties contribute to its growing popularity in periodontal applications, where targeted antimicrobial effects are crucial for effective management of pathogenic biofilms [46,47,48]. The fundamental mechanism of ICG-mediated PDT involves the application of the photosensitizer to periodontal pockets, followed by activation with a specific wavelength of light. Upon activation, ICG undergoes a photochemical reaction that generates reactive oxygen species, which exert potent cytotoxic effects on bacterial cell walls and membranes, ultimately leading to bacterial cell death. This process offers a targeted approach to eliminating periodontal pathogens while minimizing collateral damage to surrounding tissues [48,49]. Multiple clinical studies have investigated the efficacy of ICG-mediated PDT as an adjunct to scaling and root planing (SRP) in periodontitis management.
One of the most significant advantages of ICG as a photosensitizer is its absorption spectrum in the near-infrared range around 800 nm [35,36,37,38,39,40,41,42,43]. This property allows for deeper tissue penetration compared to photosensitizers that work with visible light wavelengths, enabling more effective targeting of subgingival pathogens located within periodontal pockets and tissues [35,36,37,38,39,40,41,42,43]. Furthermore, ICG demonstrates an excellent safety profile, with minimal risk of systemic effects or adverse reactions. Unlike antibiotics, which can contribute to antimicrobial resistance and potentially disrupt the commensal microbiota, ICG-mediated PDT offers targeted antimicrobial action with a low risk of developing resistance [39]. This aspect is particularly important in contemporary periodontal care, where antibiotic stewardship is increasingly emphasized [40]. Multiple studies have demonstrated ICG’s efficacy against periodontal pathogens, including those associated with peri-implantitis [38,39,40,41,42,43,44,45,46,47,48,49,50,51,52]. Beyond its antimicrobial effects, ICG-mediated PDT may offer additional anti-inflammatory benefits. Studies have shown reductions in inflammatory biomarkers following treatment, suggesting a multifaceted therapeutic approach that addresses both the microbial and inflammatory components of periodontal disease [53,54,55].
This dual action represents a significant advantage over conventional mechanical debridement, which primarily targets the bacterial biofilm without directly modulating the host inflammatory response [53]. Despite promising results in many studies, the clinical effectiveness of ICG-mediated PDT shows some inconsistency across different investigations. The additional benefit of ICG-PDT over SRP alone was limited to a transient reduction in sulcus fluid flow rate [37]. This suggests that the adjunctive value of ICG-PDT might not always translate to substantial long-term clinical advantages compared to conventional treatment approaches.
The lack of standardized protocols represents another significant limitation in ICG-mediated PDT. Variations in ICG concentration, application method, light parameters (wavelength, power output, energy density), exposure time, and treatment area can all influence treatment outcomes. This lack of standardization makes it difficult to compare results across studies and establish definitive guidelines for clinical practice.
These requirements may present barriers to widespread adoption, particularly in resource-limited settings. Additionally, the procedure typically extends treatment time, which may impact practice workflow and patient acceptance. When comparing ICG to other photosensitizers, such as methylene blue (MB), several differences emerge. A microbiological study on phototherapy of gingivitis using MB demonstrated total suppression of pathogenic flora after a 3 min exposure to the dye solution followed by a 20 s treatment with a red light-emitting toothbrush. While this study used MB rather than ICG, it provides a useful point of comparison regarding photosensitizer efficacy. MB operates at shorter wavelengths (around 663 nm) compared to ICG (around 800 nm), resulting in different tissue penetration profiles [56,57,58,59].
The red light used with MB has less tissue penetration than the near-infrared light used with ICG, potentially limiting its effectiveness in deeper periodontal pockets. However, MB has demonstrated significant antimicrobial effects in gingivitis treatment, suggesting that both photosensitizers have valid applications depending on the specific clinical scenario. Current evidence suggests that ICG-mediated PDT offers promising adjunctive benefits in periodontal therapy, but several knowledge gaps remain. Future research should focus on establishing standardized protocols, optimizing dosage and application methods, and investigating the long-term effects of repeated applications. Additionally, comparative studies directly evaluating different photosensitizers within the same experimental design would provide valuable insights into their relative efficacy and appropriate clinical applications [60,61,62,63,64,65].
Indocyanine green as a photosensitizer in periodontal photodynamic therapy presents several advantages, including excellent tissue penetration, a favorable safety profile, effective antimicrobial action, and potential anti-inflammatory effects [35,36,37,38,39,40,41,42,43]. However, limitations such as inconsistent clinical outcomes, lack of standardized protocols, temporary effects on inflammatory biomarkers, and practical implementation challenges must be considered [35,36,37,38,39,40,41,42,43]. The current evidence suggests that ICG-mediated PDT may serve as a valuable adjunct to conventional periodontal therapy, particularly in cases where mechanical debridement alone might be insufficient. However, clinicians should approach this modality with a clear understanding of both its potential benefits and limitations. Further research with standardized protocols and long-term follow-up periods is needed to establish definitive guidelines for the optimal use of ICG in periodontal applications.
The wide variation in ICG concentration (ranging from 0.1 to 5 mg/mL) and laser power output (100–2000 mW) across studies likely contributed to the heterogeneity of outcomes observed, as these parameters critically affect the photothermal and photodynamic efficacy of treatment; however, due to insufficient stratified reporting, a direct dose–response relationship could not be formally analyzed in this review. Future trials should employ standardized or at least well-justified ICG and laser dosimetry parameters and explicitly evaluate their impact on clinical and microbiological endpoints to optimize treatment protocols.
The greater antimicrobial efficacy of ICG-aPDT against P. gingivalis and A. actinomycetemcomitans, observed across multiple studies, may be attributed to both the photochemical properties of ICG and the structural vulnerabilities of these Gram-negative pathogens [17,30,37,53]. ICG absorbs near-infrared light (~800 nm), which penetrates deeply into tissue and, upon activation, generates both reactive oxygen species (ROS) and localized heat (photothermal effect) [7,53]. These mechanisms disrupt bacterial membranes, denature proteins, and damage nucleic acids. P. gingivalis and A. actinomycetemcomitans are particularly susceptible due to their thin peptidoglycan layer and high membrane lipid content, which enhance light absorption and thermal sensitivity [30,37]. Additionally, ICG’s anionic and amphiphilic nature promotes binding to bacterial membranes and biofilm matrices, facilitating targeted phototoxic effects [53]. The short incubation time and low photobleaching tendency of ICG further support efficient ROS-mediated killing within subgingival pockets [7,53]. In contrast, Gram-positive species or facultative aerobes with thicker cell walls may be less susceptible under equivalent conditions [37].
4.2. Limitations of the Evidence
The current body of evidence supporting the use of ICG-aPDT as an adjunctive treatment for periodontitis is limited by several important factors. Despite the inclusion of only randomized controlled trials, substantial heterogeneity exists across studies in terms of ICG concentrations, laser wavelengths, power outputs, irradiation times, and treatment frequencies. This variability makes it difficult to directly compare outcomes or establish universally applicable treatment protocols. Additionally, most studies included relatively short follow-up periods, typically 1 to 6 months, limiting our understanding of the long-term effectiveness and stability of ICG-aPDT outcomes. While several trials demonstrated promising improvements in probing depth and microbial reduction, inconsistencies in reported outcomes and a lack of standardized microbiological assessment methods further weaken the generalizability of the results. Moreover, many studies lacked detailed reporting on potential confounding factors, such as smoking status, oral hygiene compliance, or systemic conditions beyond diabetes, which could have influenced treatment efficacy. Few studies directly compared ICG with other photosensitizers, making it difficult to definitively determine its relative superiority. Lastly, while safety was consistently reported, adverse effects may have been underreported due to limited sample sizes or short observation windows. Collectively, these limitations underscore the need for larger, long-term, multicenter trials with standardized protocols to more definitively assess the clinical value of ICG-aPDT in periodontal therapy.
4.3. Limitations of the Review Process
While this systematic review provides a synthesis of the available evidence on ICG-aPDT for the treatment of periodontitis, several limitations of the review process must be acknowledged. Firstly, although only randomized controlled trials (RCTs) were included to ensure methodological rigor, the clinical heterogeneity among these studies, such as differences in treatment protocols, ICG concentrations, laser parameters, application techniques, and follow-up durations, hindered the ability to perform a meta-analysis and limited the comparability of the findings. Secondly, most studies lacked long-term follow-up data, thereby restricting insights into the durability of treatment outcomes. Thirdly, language bias may have influenced the findings, as only studies published in English were considered, potentially omitting relevant trials published in other languages. Furthermore, despite the low risk of bias identified in quality assessments, reporting inconsistencies in microbiological data and selective outcome measures in some trials could have introduced a degree of reporting bias. Finally, the exclusion of the gray literature and unpublished data may have contributed to publication bias. These factors collectively highlight the need for future research to adhere to standardized methodologies and reporting frameworks to enhance comparability and strengthen clinical recommendations for ICG-aPDT in periodontal therapy.
4.4. Implications for Practice, Policy, and Future Research
The findings of this systematic review support the integration of ICG-aPDT as a safe and effective adjunct to conventional periodontal treatments, particularly in managing deep periodontal pockets and in systemically compromised patients, such as those with diabetes mellitus. In clinical practice, ICG-aPDT offers a minimally invasive, well tolerated option with demonstrated antimicrobial and anti-inflammatory effects, making it a valuable addition to periodontal maintenance and regenerative protocols. However, due to variability in treatment protocols and limited long-term data, clinicians should apply ICG-aPDT with caution and ensure patients are informed about its adjunctive role rather than a replacement for mechanical debridement. From a policy perspective, current evidence does not yet support the widespread recommendation of ICG-aPDT in clinical guidelines, largely due to the absence of standardized dosing, irradiation parameters, and frequency of application. To move toward broader clinical adoption, regulatory and professional bodies should prioritize the development of consensus-based guidelines grounded in high-quality, reproducible evidence. Future research should focus on multicenter, long-duration randomized controlled trials with clearly defined protocols and standardized outcome measures, including microbiological, inflammatory, and clinical parameters. Comparative studies evaluating ICG against other photosensitizers under uniform conditions would provide critical insights into its relative efficacy. Investigations into cost effectiveness, patient-reported outcomes, and implementation feasibility in diverse clinical settings are also essential to support evidence-based decision-making. Ultimately, addressing these research gaps will facilitate the optimization and broader clinical integration of ICG-aPDT in modern periodontal therapy.
5. Conclusions
This systematic review confirms that indocyanine green-mediated photodynamic therapy (ICG-aPDT) is a safe and effective adjunct to conventional periodontal treatments, particularly in deep pockets and systemically compromised patients. While most studies demonstrated statistically significant clinical and microbiological improvements with adjunctive ICG-aPDT, inconsistent outcomes in some trials may reflect variability in treatment protocols, photosensitizer formulation, baseline disease severity, and timing of outcome assessment, underscoring the need for standardized methodologies and stratified analyses in future research. ICG-aPDT holds strong potential as a non-invasive tool in modern periodontal therapy, especially when tailored to well-defined clinical protocols.
Author Contributions
Conceptualization, R.W., J.F.-R. and J.K.; methodology, J.F.-R., D.S. and K.L.; software, J.F.-R.; formal analysis, J.F.-R., K.B.-S., D.S. and R.W.; investigation, J.F.-R., K.L., H.F. and R.W.; writing—original draft preparation, J.F.-R., K.L., H.F. and R.W.; writing—review and editing, J.F.-R., K.B.-S., D.S. and R.W.; supervision, D.S., K.B.-S. and J.K.; funding acquisition, D.S., R.W. and K.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gasner, N.S.; Schure, R.S. Periodontal Disease. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554590/ (accessed on 3 March 2025).
- Könönen, E.; Gursoy, M.; Gursoy, U.K. Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J. Clin. Med. 2019, 8, 1135. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pragati, S.D.; Neelam, M. A Systematic Review on Periodontal Disease. J. Res. Med. Dent. Sci. 2020, 8, 153–162. [Google Scholar]
- Isola, G.; Santonocito, S.; Lupi, S.M.; Polizzi, A.; Sclafani, R.; Patini, R.; Marchetti, E. Periodontal Health and Disease in the Context of Systemic Diseases. Mediat. Inflamm. 2023, 2023, 9720947. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, J.; Amar, S. Periodontal disease and systemic conditions: A bidirectional relationship. Odontology 2006, 94, 10–21. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hashim, N.T.; Babiker, R.; Padmanabhan, V.; Ahmed, A.T.; Chaitanya, N.C.S.K.; Mohammed, R.; Priya, S.P.; Ahmed, A.; El Bahra, S.; Islam, M.S.; et al. The Global Burden of Periodontal Disease: A Narrative Review on Unveiling Socioeconomic and Health Challenges. Int. J. Environ. Res. Public Health 2025, 22, 624. [Google Scholar] [CrossRef]
- Abdulkareem, A.A.; Al-Taweel, F.B.; Al-Sharqi, A.J.B.; Gul, S.S.; Sha, A.; Chapple, I.L.C. Current concepts in the pathogenesis of periodontitis: From symbiosis to dysbiosis. J. Oral Microbiol. 2023, 15, 2197779. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shrivastava, D.; Natoli, V.; Srivastava, K.C.; Alzoubi, I.A.; Nagy, A.I.; Hamza, M.O.; Al-Johani, K.; Alam, M.K.; Khurshid, Z. Novel Approach to Dental Biofilm Management through Guided Biofilm Therapy (GBT): A Review. Microorganisms 2021, 9, 1966. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cobb, C.M. Clinical significance of non-surgical periodontal therapy: An evidence-based perspective of scaling and root planing. J. Clin. Periodontol. 2002, 29 (Suppl. S2), 22–32. [Google Scholar] [CrossRef] [PubMed]
- El Mobadder, M.; Nammour, S.; Grzech-Leśniak, K. Photodynamic Therapy with Tolonium Chloride and a Diode Laser (635 nm) in the Non-Surgical Management of Periodontitis: A Clinical Study. J. Clin. Med. 2023, 12, 5270. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Huemer, M.; Shambat, S.M.; Brugger, S.D.; Zinkernagel, A.S. Antibiotic resistance and persistence-Implications for human health and treatment perspectives. EMBO Rep. 2020, 21, e51034. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Elashiry, M.; Morandini, A.C.; Timothius, C.J.C.; Ghaly, M.; Cutler, C.W. Selective Antimicrobial Therapies for Periodontitis: Win the “Battle and the War”. Int. J. Mol. Sci. 2021, 22, 6459. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Becattini, S.; Taur, Y.; Pamer, E.G. Antibiotic-Induced Changes in the Intestinal Microbiota and Disease. Trends Mol. Med. 2016, 22, 458–478. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dąbrowska, A.; Mastalerz, J.; Wilczyński, B.; Osiecka, B.; Choromańska, A. Determinants of Photodynamic Therapy Resistance in Cancer Cells. Int. J. Mol. Sci. 2024, 25, 12069. [Google Scholar] [CrossRef] [PubMed]
- Correia, J.H.; Rodrigues, J.A.; Pimenta, S.; Dong, T.; Yang, Z. Photodynamic Therapy Review: Principles, Photosensitizers, Applications, and Future Directions. Pharmaceutics 2021, 13, 1332. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Przygoda, M.; Bartusik-Aebisher, D.; Dynarowicz, K.; Cieślar, G.; Kawczyk-Krupka, A.; Aebisher, D. Cellular Mechanisms of Singlet Oxygen in Photodynamic Therapy. Int. J. Mol. Sci. 2023, 24, 16890. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vaishampayan, A.; Grohmann, E. Antimicrobials Functioning through ROS-Mediated Mechanisms: Current Insights. Microorganisms 2021, 10, 61. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nie, M.; Zhang, P.; Pathak, J.L.; Wang, X.; Wu, Y.; Yang, J.; Shen, Y. Photodynamic therapy in periodontitis: A narrative review. Photodermatol. Photoimmunol. Photomed. 2024, 40, e12946. [Google Scholar] [CrossRef] [PubMed]
- Dudzik, T.; Domański, I.; Makuch, S. The impact of photodynamic therapy on immune system in cancer—An update. Front. Immunol. 2024, 15, 1335920. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chon, B.; Ghann, W.; Uddin, J.; Anvari, B.; Kundra, V. Indocyanine Green (ICG) Fluorescence Is Dependent on Monomer with Planar and Twisted Structures and Inhibited by H-Aggregation. Int. J. Mol. Sci. 2023, 24, 13030. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Indocyanine Green [Internet]. Elsevier. Available online: https://www.sciencedirect.com/topics/pharmacology-toxicology-and-pharmaceutical-science/indocyanine-green (accessed on 26 April 2025).
- Mytych, W.; Bartusik-Aebisher, D.; Aebisher, D. The Medical Basis for the Photoluminescence of Indocyanine Green. Molecules 2025, 30, 888. [Google Scholar] [CrossRef]
- Harris, D.M.; Sulewski, J.G. Photoinactivation and Photoablation of Porphyromonas gingivalis. Pathogens 2023, 12, 1160. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fiegler-Rudol, J.; Łopaciński, M.; Los, A.; Skaba, D.; Wiench, R. Riboflavin-Mediated Photodynamic Therapy in Periodontology: A Systematic Review of Applications and Outcomes. Pharmaceutics 2025, 17, 217. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Watson, P.F.; Petrie, A. Method agreement analysis: A review of correct methodology. Theriogenology 2010, 73, 1167–1179. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.5 (Updated August 2024); Cochrane: London, UK, 2024; Available online: https://www.cochrane.org/authors/handbooks-and-manuals/handbook (accessed on 4 April 2025).
- Al-Momani, M.M. Indocyanine-mediated antimicrobial photodynamic therapy promotes superior clinical effects in stage III and grade C chronic periodontitis among controlled and uncontrolled diabetes mellitus: A randomized controlled clinical trial. Photodiagn. Photodyn. Ther. 2021, 35, 102379. [Google Scholar] [CrossRef]
- Annunziata, M.; Donnarumma, G.; Guida, A.; Nastri, L.; Persico, G.; Fusco, A.; Sanz-Sánchez, I.; Guida, L. Clinical and microbiological efficacy of indocyanine green-based antimicrobial photodynamic therapy as an adjunct to non-surgical treatment of periodontitis: A randomized controlled clinical trial. Clin. Oral Investig. 2023, 27, 2385–2394. [Google Scholar] [CrossRef]
- Cetiner, D.O.; Isler, S.C.; Ilikci-Sagkan, R.; Sengul, J.; Kaymaz, O.; Corekci, A.U. The adjunctive use of antimicrobial photodynamic therapy, light-emitting-diode photobiomodulation and ozone therapy in regenerative treatment of stage III/IV grade C periodontitis: A randomized controlled clinical trial. Clin. Oral Investig. 2024, 28, 426. [Google Scholar] [CrossRef]
- Chowdhury, U.R.; Kamath, D.; Rao, P.; Shenoy, M.S.; Shenoy, R. Indocyanine green based antimicrobial photodynamic therapy as an adjunct to non-surgical periodontal treatment in periodontal maintenance patients: A clinico-microbiological study [version 2; peer review: 3 approved, 1 not approved]. F1000Research 2024, 12, 949. [Google Scholar] [CrossRef]
- Costa, F.O.; Lima, R.P.E.; Costa, A.M.; Costa, A.A.; Pereira, G.H.M.; Cortelli, S.C.; Cortelli, J.R.; Cyrino, R.M.; Silva, T.A.; Cota, L.O.M. Adjunctive effects of photodynamic therapy using indocyanine green in residual pockets during periodontal maintenance therapy: A split-mouth randomized controlled trial. J. Periodontol. 2023, 94, 1100–1111. [Google Scholar] [CrossRef]
- Dalvi, S.A.; Hanna, R.; Gattani, D.R. Utilisation of antimicrobial photodynamic therapy as an adjunctive tool for open flap debridement in the management of chronic periodontitis: A randomized controlled clinical trial. Photodiagn. Photodyn. Ther. 2019, 25, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, J.; Ono, K.; Iwamura, Y.; Sasaki, Y.; Ohno, T.; Goto, R.; Nishida, E.; Yamamoto, G.; Kikuchi, T.; Higuchi, N.; et al. Suppression of subgingival bacteria by antimicrobial photodynamic therapy using transgingival irradiation: A randomized clinical trial. J. Periodontol. 2024, 95, 718–728. [Google Scholar] [CrossRef] [PubMed]
- Hill, G.; Dehn, C.; Hinze, A.V.; Frentzen, M.; Meister, J. Indocyanine green-based adjunctive antimicrobial photodynamic therapy for treating chronic periodontitis: A randomized clinical trial. Photodiagn. Photodyn. Ther. 2019, 26, 29–35. [Google Scholar] [CrossRef]
- Joshi, K.; Baiju, C.S.; Khashu, H.; Bansal, S. Clinical effectiveness of indocyanine green mediated antimicrobial photodynamic therapy as an adjunct to scaling root planing in treatment of chronic periodontitis- A randomized controlled clinical trial. Photodiagn. Photodyn. Ther. 2020, 29, 101591. [Google Scholar] [CrossRef]
- Monzavi, A.; Chinipardaz, Z.; Mousavi, M.; Fekrazad, R.; Moslemi, N.; Azaripour, A.; Bagherpasand, O.; Chiniforush, N. Antimicrobial photodynamic therapy using diode laser activated indocyanine green as an adjunct in the treatment of chronic periodontitis: A randomized clinical trial. Photodiagn. Photodyn. Ther. 2016, 14, 93–97. [Google Scholar] [CrossRef]
- Niazi, F.H.; Noushad, M.; Tanvir, S.B.; Ali, S.; Al-Khalifa, K.S.; Qamar, Z.; Al-Sheikh, R. Antimicrobial efficacy of indocyanine green-mediated photodynamic therapy compared with Salvadora persica gel application in the treatment of moderate and deep pockets in periodontitis. Photodiagn. Photodyn. Ther. 2020, 29, 101665. [Google Scholar] [CrossRef]
- Qamar, Z.; Almohana, S.A.; Alanazi, A.K.; Alanazi, A.K.; Almohana, A.A.; Zeeshan, T. Clinical evaluation of the effects of topical indocyanine green-mediated photosensitiser vs aloe vera gel as adjunct therapy to scaling and root planing in chronic periodontitis patients. Oral Health Prev. Dent. 2021, 19, 489–494. [Google Scholar] [CrossRef]
- Sethi, K.S.; Raut, C.P. Antimicrobial photodynamic therapy using indocyanine green as a photosensitizer in treatment of chronic periodontitis: A clinico-microbial study. Indian J. Dent. Res. 2019, 30, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Shingnapurkar, S.H.; Mitra, D.K.; Kadav, M.S.; Shah, R.A.; Rodrigues, S.V.; Prithyani, S.S. The effect of indocyanine green-mediated photodynamic therapy as an adjunct to scaling and root planing in the treatment of chronic periodontitis: A comparative split-mouth randomized clinical trial. Indian J. Dent. Res. 2016, 27, 609–617. [Google Scholar] [CrossRef]
- Kura, S.; Viswa, C.R.; Amarender, R.A.; Harish, R.B.; Chakravarthy, R.; Anumala, N. Effect of a single session of antimicrobial photodynamic therapy using indocyanine green in the treatment of chronic periodontitis: A randomized controlled pilot trial. Quintessence Int. 2015, 46, 391–400. [Google Scholar] [CrossRef]
- Sukumar, K.; Tadepalli, A.; Parthasarathy, H.; Ponnaiyan, D. Evaluation of combined efficacy of photodynamic therapy using indocyanine green photosensitizer and non-surgical periodontal therapy on clinical and microbial parameters in the management of chronic periodontitis subjects: A randomized split-mouth design. Photodiagn. Photodyn. Ther. 2020, 31, 101949. [Google Scholar] [CrossRef] [PubMed]
- Raut, C.P.; Sethi, K.S.; Kohale, B.R.; Mamajiwala, A.; Warang, A. Indocyanine green-mediated photothermal therapy in treatment of chronic periodontitis: A clinico-microbiological study. J. Indian Soc. Periodontol. 2018, 22, 221–227. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Karmakar, S.; Prakash, S.; Jagadeson, M.; Namachivayam, A.; Das, D.; Sarkar, S. Clinico-microbiological Efficacy of Indocyanine Green as a Novel Photosensitizer for Photodynamic Therapy among Patients with Chronic Periodontitis: A Split-mouth Randomized Controlled Clinical Trial. J. Pharm. Bioallied Sci. 2021, 13 (Suppl. S1), S143–S148. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yamashita, A.; Jang, P.; Bao, K.; Kashiwagi, S.; Frangioni, J.V.; Choi, H.S. Indocyanine Blue (ICB) as a Functional Alternative to Indocyanine Green (ICG) for Enhanced 700 nm NIR Imaging. Int. J. Mol. Sci. 2024, 25, 13547. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schweigert, T.B.M.O.; Afonso, J.P.R.; da Palma, R.K.; Oliveira-Silva, I.; Silva, C.H.M.; Jirjos, E.I.; Júnior, W.R.F.; Insalaco, G.; Guedes, O.A.; Oliveira, L.V.F. Influence of Photosensitizer on Photodynamic Therapy for Peri-Implantitis: A Systematic Review. Pharmaceutics 2024, 16, 307. [Google Scholar] [CrossRef]
- Kikuchi, T.; Mogi, M.; Okabe, I.; Okada, K.; Goto, H.; Sasaki, Y.; Fujimura, T.; Fukuda, M.; Mitani, A. Adjunctive Application of Antimicrobial Photodynamic Therapy in Nonsurgical Periodontal Treatment: A Review of Literature. Int. J. Mol. Sci. 2015, 16, 24111–24126. [Google Scholar] [CrossRef]
- Labban, N.; Al Shibani, N.; Al-Kattan, R.; Alfouzan, A.F.; Binrayes, A.; Assery, M.K. Clinical, bacterial, and inflammatory outcomes of indocyanine green-mediated photodynamic therapy for treating periimplantitis among diabetic patients: A randomized controlled clinical trial. Photodiagn. Photodyn. Ther. 2021, 35, 102350. [Google Scholar] [CrossRef] [PubMed]
- Alsayed, H.; Bukhari, I.A.; Alsaif, R.; Vohra, F. Efficacy of indocyanine green and methylene blue mediated-photodynamic therapy on peri-implant outcomes among diabetics with peri-implant mucositis. Photodiagn. Photodyn. Ther. 2023, 42, 103344. [Google Scholar] [CrossRef] [PubMed]
- Fiegler-Rudol, J.; Zięba, N.; Turski, R.; Misiołek, M.; Wiench, R. Hypericin-Mediated Photodynamic Therapy for Head and Neck Cancers: A Systematic Review. Biomedicines 2025, 13, 181. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bashir, N.Z.; Singh, H.-A.; Virdee, S.S. Indocyanine green-mediated antimicrobial photodynamic therapy as an adjunct to periodontal therapy: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 5699–5710. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chiang, C.-P.; Hsieh, O.; Tai, W.-C.; Chen, Y.-J.; Chang, P.-C. Clinical outcomes of adjunctive indocyanine green-diode lasers therapy for treating refractory periodontitis: A randomized controlled trial with in vitro assessment. J. Formos. Med. Assoc. 2020, 119, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, K.K.; Pavaskar, R.; Cappetta, E.G.; Drew, H.J. Effectiveness of adjunctive use of low-level laser therapy and photodynamic therapy after scaling and root planing in patients with chronic periodontitis. Int. J. Periodontics Restor. Dent. 2019, 39, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.-H.; Zhang, X.-J. Indocyanine green combined with methylene blue versus methylene blue alone for sentinel lymph node biopsy in breast cancer: A retrospective study. BMC Surg. 2023, 23, 133. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guo, J.; Yang, H.; Wang, S.; Cao, Y.; Liu, M.; Xie, F.; Liu, P.; Zhou, B.; Tong, F.; Cheng, L.; et al. Comparison of sentinel lymph node biopsy guided by indocyanine green, blue dye, and their combination in breast cancer patients: A prospective cohort study. World J. Surg. Oncol. 2017, 15, 196. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yang, R.; Dong, C.; Jiang, T.; Zhang, X.; Zhang, F.; Fan, Z. Indocyanine Green and Methylene Blue Dye Guided Sentinel Lymph Node Biopsy in Early Breast Cancer: A Single-Center Retrospective Survival Study in 1574 Patients. Clin. Breast Cancer 2023, 23, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Łopaciński, M.; Fiegler-Rudol, J.; Niemczyk, W.; Skaba, D.; Wiench, R. Riboflavin- and Hypericin-Mediated Antimicrobial Photodynamic Therapy as Alternative Treatments for Oral Candidiasis: A Systematic Review. Pharmaceutics 2024, 17, 33. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, Y.; Sun, G.; Xie, J.; Xiao, S.; Lin, C. Antimicrobial photodynamic therapy against oral biofilm: Influencing factors, mechanisms, and combined actions with other strategies. Front. Microbiol. 2023, 14, 1192955. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The oral microbiota: Dynamic communities and host interactions. Nat. Rev. Microbiol. 2018, 16, 745–759. [Google Scholar] [CrossRef]
- Houthoofd, S.; Vuylsteke, M.; Mordon, S.; Fourneau, I. Photodynamic therapy for atherosclerosis. The potential of indocyanine green. Photodiagn. Photodyn. Ther. 2020, 29, 101568. [Google Scholar] [CrossRef]
- Kruczek-Kazibudzka, A.; Lipka, B.; Fiegler-Rudol, J.; Tkaczyk, M.; Skaba, D.; Wiench, R. Toluidine Blue and Chlorin-e6 Mediated Photodynamic Therapy in the Treatment of Oral Potentially Malignant Disorders: A Systematic Review. Int. J. Mol. Sci. 2025, 26, 2528. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Warakomska, A.; Fiegler-Rudol, J.; Kubizna, M.; Skaba, D.; Wiench, R. The Role of Photodynamic Therapy Mediated by Natural Photosensitisers in the Management of Peri-Implantitis: A Systematic Review. Pharmaceutics 2025, 17, 443. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fiegler-Rudol, J.; Kapłon, K.; Kotucha, K.; Moś, M.; Skaba, D.; Kawczyk-Krupka, A.; Wiench, R. Hypocrellin-Mediated PDT: A Systematic Review of Its Efficacy, Applications, and Outcomes. Int. J. Mol. Sci. 2025, 26, 4038. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).