
Echocardiographic Calcium Score of Aortic Valve Correlates with Coronary Artery Calcium Score in Heterozygous Familial Hypercholesterolemia


 ,
,  , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. ACS Measurement by Coronary Calcium CT Scan
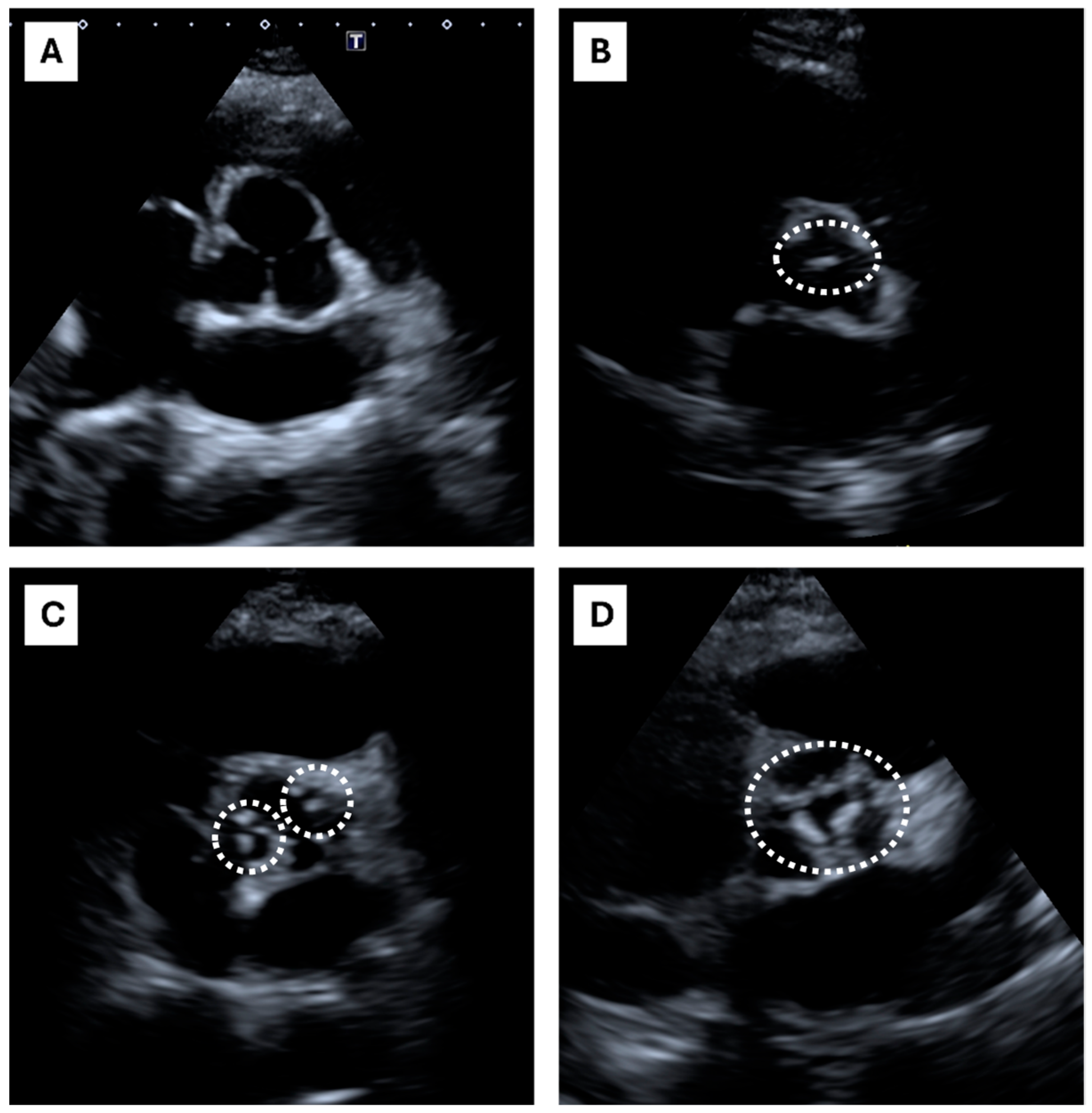
2.2. Echocardiographic Calcium Score (ECS)
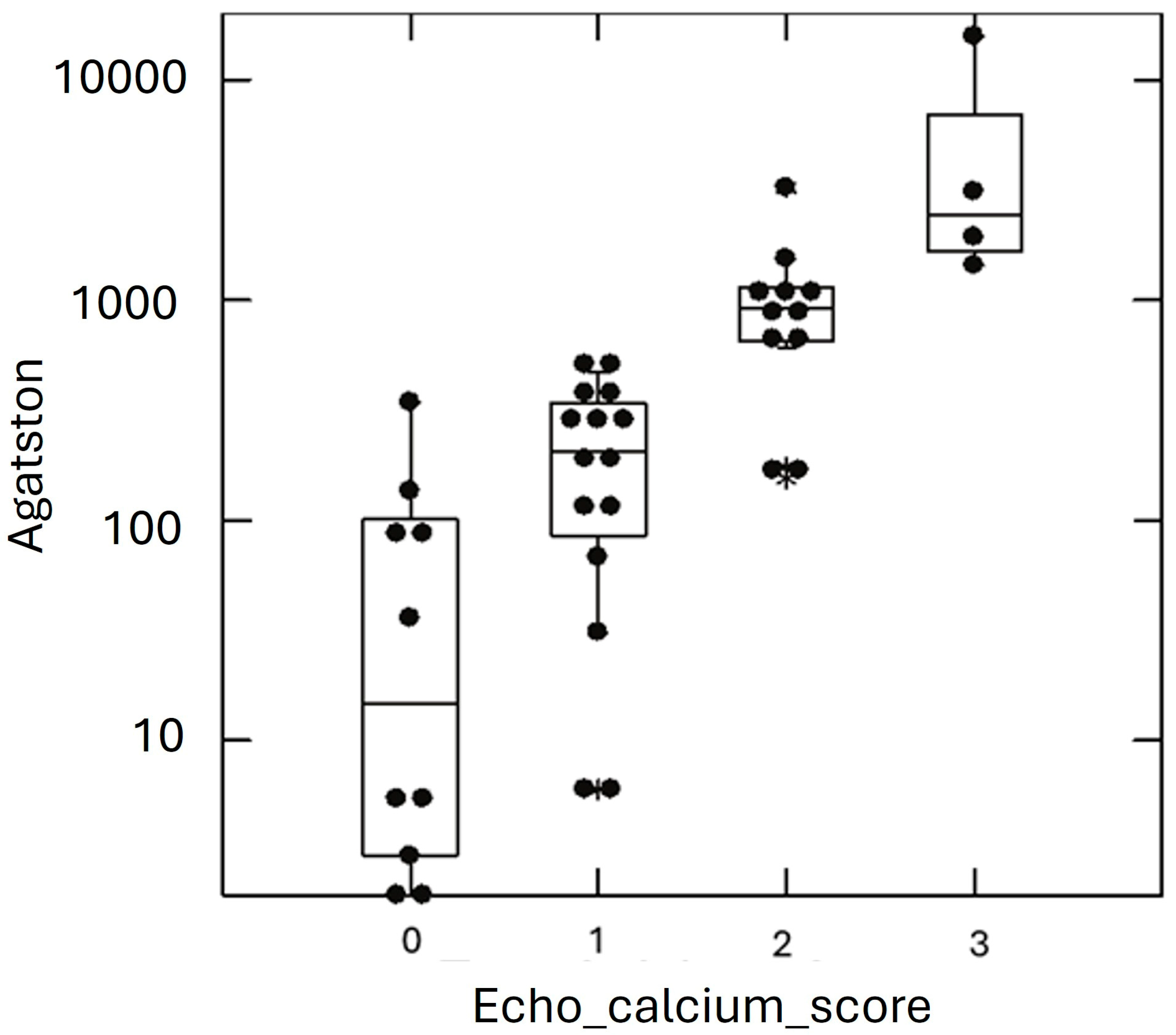
2.3. Statistics
3. Results
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HeFH | Heterozygous familial hypercholesterolemia |
| HoFH | Homozygous familial hypercholesterolemia |
| ASCVD | Atherosclerotic cardiovascular disease |
| AVC | Aortic valve calcifications |
| CV | Cardiovascular |
| CAC score | Coronary artery calcium score |
| CT | Computed tomography |
| MACE | Major adverse cardiovascular event |
| ACS | Agatston calcium score |
| ECS | Echocardiographic calcium score |
References
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; ESC Scientific Document Group. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Beheshti, S.O.; Madsen, C.M.; Varbo, A.; Nordestgaard, B.G. Worldwide Prevalence of Familial Hypercholesterolemia: Meta-Analyses of 11 Million Subjects. J. Am. Coll. Cardiol. 2020, 75, 2553–2566. [Google Scholar] [CrossRef]
- Völzke, H.; Haring, R.; Lorbeer, R.; Wallaschofski, H.; Reffelmann, T.; Empen, K.; Rettig, R.; John, U.; Felix, S.B.; Dörr, M. Heart valve sclerosis predicts all-cause and cardiovascular mortality. Atherosclerosis 2010, 209, 606–610. [Google Scholar] [CrossRef]
- Shah, P.K. Screening asymptomatic subjects for subclinical atherosclerosis: Can we, does it matter, and should we? J. Am. Coll. Cardiol. 2010, 56, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Elias-Smale, S.E.; Proença, R.V.; Koller, M.T.; Kavousi, M.; van Rooij, F.J.; Hunink, M.G.; Steyerberg, E.W.; Hofman, A.; Oudkerk, M.; Witteman, J.C. Coronary calcium score improves classification of coronary heart disease risk in the elderly: The Rotterdam study. J. Am. Coll. Cardiol. 2010, 56, 1407–1414. [Google Scholar] [CrossRef]
- Kälsch, H.; Lehmann, N.; Berg, M.H.; A Mahabadi, A.; Mergen, P.; Möhlenkamp, S.; Bauer, M.; Kara, K.; Dragano, N.; Hoffmann, B.; et al. Coronary artery calcification outperforms thoracic aortic calcification for the prediction of myocardial infarction and all-cause mortality: The Heinz Nixdorff Recall Study. Eur. J. Prev. Cardiol. 2014, 21, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Khera, A.; Budoff, M.J.; O’donnell, C.J.; Ayers, C.A.; Locke, J.; de Lemos, J.A.; Massaro, J.M.; McClelland, R.L.; Taylor, A.; Levine, B.D. Astronaut Cardiovascular Health and Risk Modification (Astro-CHARM) coronary calcium atherosclerotic cardiovascular disease risk calculator. Circulation 2018, 138, 1819–1827. [Google Scholar] [CrossRef]
- Liew, G.; Chow, C.; van Pelt, N.; Younger, J.; Jelinek, M.; Chan, J.; Hamilton-Craig, C. Cardiac Society of Australia and New Zealand Position Statement: Coronary Artery Calcium Scoring. Heart Lung Circ. 2017, 26, 1239–1251. [Google Scholar] [CrossRef] [PubMed]
- van der Zant, F.M.; Wondergem, M.; Lazarenko, S.V.; Geenen, R.W.; Umans, V.A.; Cornel, J.-H.; Knol, R.J. Ruling out coronary artery disease in women with atypical chest pain: Results of calcium score combined with coronary computed tomography angiography and associated radiation exposure. J. Women Health 2015, 24, 550–556. [Google Scholar] [CrossRef]
- Santos, R.D.; Gidding, S.S.; Hegele, R.A.; Cuchel, M.A.; Barter, P.J.; Watts, G.F.; Baum, S.J.; Catapano, A.L.; Chapman, M.J.; International Atherosclerosis Society Severe Familial Hypercholesterolemia Panel; et al. Defining severe familial hypercholesterolaemia and the implications for clinical management: A consensus statement from the International Atherosclerosis Society Severe Familial Hypercholesterolemia Panel. Lancet Diabetes Endocrinol. 2016, 4, 850–861. [Google Scholar] [CrossRef]
- Gallo, A.; Mszar, R.; Miname, M.H. Updates on the Use of Subclinical Atherosclerosis to Predict Risk of Cardiovascular Events in Heterozygous Familial Hypercholesterolemia. Curr. Atheroscler. Rep. 2022, 24, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Moreo, A.; Gaibazzi, N.; Faggiano, P.; Mohammed, M.; Carerj, S.; Mureddu, G.; Pigazzani, F.; Muiesan, L.; Salvetti, M.; Cesana, F.; et al. Multiparametric carotid and cardiac ultrasound compared with clinical risk scores for the prediction of a angiographic coronary artery disease: A multicenter prospective study. J. Hypertens. 2015, 33, 1291–1300. [Google Scholar] [CrossRef] [PubMed]
- Faggiano, P.; Dasseni, N.; Gaibazzi, N.; Rossi, A.; Henein, M.; Pressman, G. Cardiac calcification as a marker of subclinical atherosclerosis and predictor of cardiovascular events: A review of the evidence. Eur. J. Prev. Cardiol. 2019, 26, 1191–1204. [Google Scholar] [CrossRef] [PubMed]
- Cuchel, M.; Raal, F.J.; Hegele, R.A.; Al-Rasadi, K.; Arca, M.; Averna, M.; Bruckert, E.; Freiberger, T.; Gaudet, D.; Harada-Shiba, M.; et al. 2023 Update on European Atherosclerosis Society Consensus Statement on Homozygous Familial Hypercholesterolaemia: New treatments and clinical guidance. Eur. Heart J. 2023, 44, 2277–2291. [Google Scholar] [CrossRef]
- Noto, D.; Spina, R.; Giammanco, A.; Barbagallo, C.M.; Ganci, A.; Scrimali, C.; Brucato, F.; Misiano, G.; Ciaccio, M.; Caldarella, R.; et al. Diagnosis of familial hypercholesterolemia in a large cohort of Italian genotyped hypercholesterolemic patients. Atherosclerosis 2022, 347, 63–67. [Google Scholar] [CrossRef]
- Agatston, A.S.; Janowitz, W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef]
- Corciu, A.I.; Siciliano, V.; Poggianti, E.; Petersen, C.; Venneri, L.; Picano, E. Cardiac calcification by transthoracic echocardiography in patients with known or suspected coronary artery disease. Int. J. Cardiol. 2010, 142, 288–295. [Google Scholar] [CrossRef]
- Gaibazzi, N.; Baldari, C.; Faggiano, P.; Albertini, L.; Faden, G.; Pigazzani, F.; Rossi, C.; Reverberi, C. Cardiac calcium score on 2D echo: Correlations with cardiac and coronary calcium at multi-detector computed tomography. Cardiovasc. Ultrasound 2014, 12, 43. [Google Scholar] [CrossRef]
- Casula, M.; Olmastroni, E.; Pirillo, A.; Catapano, A.L.; Members of The Lipigen Steering Commettee. Evaluation of the performance of Dutch Lipid Clinic Network score in an Italian FH population: The LIPIGEN study. Atherosclerosis 2018, 277, 413–418. [Google Scholar] [CrossRef]
- Corral, P.; Aguilar Salinas, C.A.; Matta, M.G.; Zago, V.; Schreier, L. Stratification in Heterozygous Familial Hypercholesterolemia: Imaging, Biomarkers, and Genetic Testing. Curr. Atheroscler. Rep. 2023, 25, 899–909. [Google Scholar] [CrossRef]
- Iadecola, C.; Parikh, N.S. Framingham General Cardiovascular Risk Score and Cognitive Impairment: The Power of Foresight. J. Am. Coll. Cardiol. 2020, 75, 2535–2537. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D'Agostino, R.B., Sr.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 63, 2935–2959. [Google Scholar] [CrossRef] [PubMed]
- Conroy, R.M.; Pyörälä, K.; Fitzgerald, A.P.; Sans, S.; Menotti, A.; De Backer, G.; De Bacquer, D.; Ducimetière, P.; Jousilahti, P.; Keil, U.; et al. SCORE project group: Estimation of ten-year risk of fatal cardiovascular disease in Europe: The SCORE project. Eur. Heart J. 2003, 24, 987–1003. [Google Scholar] [CrossRef] [PubMed]
- Tarugi, P.; Bertolini, S.; Calandra, S.; Arca, M.; Angelico, F.; Casula, M.; Cefalù, A.B.; D'Erasmo, L.; Fortunato, G.; Perrone-Filardi, P.; et al. Consensus document on diagnosis and management of familial hypercholesterolemia from the Italian Society for the Study of Atherosclerosis (SISA). Nutr. Metab. Cardiovasc. Dis. 2024, 34, 1819–1836. [Google Scholar] [CrossRef]
- Paquette, M.; Brisson, D.; Dufour, R.; Khoury, É.; Gaudet, D.; Baass, A. Cardiovascular disease in familial hypercholesterolemia: Validation and refinement of the Montreal-FH-SCORE. J. Clin. Lipidol. 2017, 11, 1161–1167.e3. [Google Scholar] [CrossRef]
- Brunham, L.R.; Ruel, I.; Aljenedil, S.; Rivière, J.-B.; Baass, A.; Tu, J.V.; Mancini, G.J.; Raggi, P.; Gupta, M.; Couture, P.; et al. Canadian Cardiovascular Society Position Statement on Familial Hypercholesterolemia: Update 2018. Can. J. Cardiol. 2018, 34, 1553–1563. [Google Scholar] [CrossRef] [PubMed]
- Rosenhek, R.; Klaar, U.; Schemper, M.; Scholten, C.; Heger, M.; Gabriel, H.; Binder, T.; Maurer, G.; Baumgartner, H. Mild and moderate aortic stenosis. Natural history and risk stratification by echocardiography. Eur. Heart J. 2004, 25, 199–205. [Google Scholar] [CrossRef]
- Ortega, M.A.; De Leon-Oliva, D.; Gimeno-Longas, M.J.; Boaru, D.L.; Fraile-Martinez, O.; García-Montero, C.; de Castro, A.V.; Barrena-Blázquez, S.; López-González, L.; Amor, S.; et al. Vascular Calcification: Molecular Networking, Pathological Implications and Translational Opportunities. Biomolecules 2024, 14, 275. [Google Scholar] [CrossRef]
- Christensen, J.L.; Tan, S.; Chung, H.E.; Ghosalkar, D.S.; Qureshi, R.; Chu, A.; Yu, W.; Berus, J.; Shah, N.R.; Wu, W.-C.; et al. Aortic valve calcification predicts all-cause mortality independent of coronary calcification and severe stenosis. Atherosclerosis 2020, 307, 16–20. [Google Scholar] [CrossRef]
- Pressman, G.S.; Crudu, V.; Parameswaran-Chandrika, A.; Romero-Corral, A.; Purushottam, B.; Figueredo, V.M. Can total cardiac calcium predict the coronary calcium score? Int. J. Cardiol. 2011, 146, 202–206. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Parameters | ACS ≤ 100 | ACS > 100 | p-Value 1 |
|---|---|---|---|
| Cardiovascular risk based on CAC score | Low | High | - |
| Number of subjects | 52 | 29 | - |
| Age (yrs) | 45.77 ± 12.29 | 62.69 ± 8.55 | <0.001 |
| Gender (M/F) | (24/28) | (11/18) | 0.475 |
| Smoking (No/Former/Active) | (9/3/17) | (14/10/28) | 0.576 |
| Age of FH diagnosis (yrs) | 22.08 ± 13.62 | 33.57 ± 14.06 | <0.001 |
| Family history of CVD (Y/N) | (25/27) | (14/15) | 0.927 |
| Hypertension (Y/N) | (6/46) | (13/16) | 0.297 |
| Diabetes (Y/N) | (2/50) | (3/26) | 0.729 |
| Age at start of LLT (yrs) | 26.21 ± 12.63 | 37.52 ± 14.66 | <0.001 |
| Clinical examination | |||
| BMI (kg/m2) | 26.36 ± 5.27 | 29.16 ± 4.73 | 0.007 |
| Waist circumference (cm) | 92.84 ± 15.9 | 99.24 ± 11.1 | 0.024 |
| S.B.P. (mm/Hg) | 121.81 ± 14.26 | 137.86 ± 23.97 | <0.001 |
| D.B.P. (mm/Hg) | 73.38 ± 10.47 | 77.21 ± 13.11 | 0.083 |
| Tendon xanthoma (Y/N) | (4/48) | (8/21) | 0.260 |
| Corneal arcus (Y/N) | (4/48) | (15/14) | 0.128 |
| Biochemical parameters | |||
| Total cholesterol (mmol/L) | 6.06 ± 1.83 | 5.69 ± 1.77 | 0.292 |
| Triglyceride (mmol/L) | 1.20 ± 0.57 | 1.22 ± 0.58 | 0.821 |
| HDL cholesterol (mmol/L) | 1.41 ± 0.36 | 1.49 ± 0.35 | 0.267 |
| LDL cholesterol (mmol/L) | 4.11 ± 1.65 | 3.65 ± 1.62 | 0.153 |
| Lipid-lowering therapy | |||
| Statins (Y/N) | (41/10) | (27/2) | 0.407 |
| Statins + Ezetimibe (Y/N) | (41/10) | (27/2) | 0.407 |
| PCSK9i Mab (Y/N) | (4/48) | (9/20) | 0.493 |
| Instrumental measures | |||
| Coronary calcium CT scan | |||
| ACS (range) | 0 (0–80) | 384 (101–15 k) | <0.001 2 |
| Echocardiography | |||
| ECS > 0 (Y/N) | (8/44) | (26/3) | <0.001 |
| V_max 3 | 1.38 ± 0.05 | 1.61 ± 0.07 | 0.022 |
| Specificity | 0.846 |
| Sensitivity | 0.897 |
| Accuracy | 0.864 |
| Precision | 0.765 |
| False positive rate | 0.154 |
| True positive rate | 0.897 |
| False negative rate | 0.103 |
| True negative rate | 0.846 |
| Parameters | ECS = 0 and ACS ≤ 100 | ECS = 0 and ACS > 100 | ECS > 0 and ACS ≤ 100 | ECS > 0 and ACS > 100 | p-Value 1 |
|---|---|---|---|---|---|
| Risk according to ACS | Low | High | Low | High | - |
| Risk according to ECS | Low | Low | High | High | - |
| N of subjects | 44 | 8 | 3 | 26 | - |
| Age (years) | 43.52 ± 11.80 | 58.12 ± 6.40 | 58.33 ± 3.05 | 63.12 ± 8.86 * | 0.005 |
| Male gender | 0.45 | 0.50 | 1.00 | 0.30 | 0.995 |
| BMI (kg/m2) | 26.16 ± 5.09 | 28.87 ± 2.02 | 27.61 ± 6.6 | 29.19 ± 4.98 ** | 0.005 |
| WC (cm) | 102.73 ± 10.68 | 106.33 ± 7.37 | 101.57 ± 9.61 | 107.19 ± 12.35 * | 0.033 |
| S.B.P. (mm/Hg) | 119.86 ± 13.62 | 135.33 ± 17.47 * | 132.5 ± 13.68 | 138.15 ± 24.87 ** | <0.001 |
| D.B.P. (mm/Hg) | 72.25 ± 10.16 | 88 ± 24.25 * | 79.63 ± 10.54 * | 75.96 ± 11.4 | 0.071 |
| Hypertension | 0.068 | 0.333 * | 0.375 | 0.462 * | 0.002 |
| Diabetes mellitus | 0.045 | 0 | 0 | 0.115 | 0.529 |
| Tendon xanthoma | 0.045 | 0 | 0.25 | 0.308 * | 0.018 |
| Corneal arcus | 0.091 | 0 | 0 | 0.577 | <0.001 |
| CVD Family history | 0.545 | 0.333 | 0.125 | 0.5 | 0.165 |
| Age of FH diagnosis (yrs) | 19.59 ± 12.72 | 23 ± 3.46 * | 35.75 ± 10.25 | 34.84 ± 14.35 * | <0.001 |
| TC (mmol/L) | 236.68 ± 74.47 | 249.67 ± 84.71 | 231 ± 52.21 | 218.12 ± 67.95 | 0.264 |
| TG (mmol/L) | 102.64 ± 46.53 | 104.67 ± 33.53 | 119.25 ± 66.78 | 107.68 ± 52.99 | 0.768 |
| HDL- C (mmol/L) | 55.2 ± 14.24 | 59.33 ± 8.02 | 53.63 ± 13.33 | 57.76 ± 14.13 | 0.271 |
| LDL- C (mmol/L) | 160.95 ± 66.61 | 169.4 ± 73.88 | 153.53 ± 51.42 | 138.82 ± 62.46 | 0.132 |
| Parameters | Odd Ratio (95% CI Interval) | p-Value 1 |
|---|---|---|
| Age (×10 years) 2 | 14.48 (3.78–86.8) | 0.003 |
| Echocardiographic calcium score > 0 | 0.8 (1–4.42) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cefalù, A.B.; Nardi, E.; Giammanco, A.; Gagliardo, C.M.; Barbagallo, C.M.; La Grutta, L.; Toia, P.; Brucato, F.; Scrimali, C.; Fasciana, T.M.G.; et al. Echocardiographic Calcium Score of Aortic Valve Correlates with Coronary Artery Calcium Score in Heterozygous Familial Hypercholesterolemia. Life 2025, 15, 506. https://doi.org/10.3390/life15030506
Cefalù AB, Nardi E, Giammanco A, Gagliardo CM, Barbagallo CM, La Grutta L, Toia P, Brucato F, Scrimali C, Fasciana TMG, et al. Echocardiographic Calcium Score of Aortic Valve Correlates with Coronary Artery Calcium Score in Heterozygous Familial Hypercholesterolemia. Life. 2025; 15(3):506. https://doi.org/10.3390/life15030506
Chicago/Turabian StyleCefalù, Angelo Baldassare, Emilio Nardi, Antonina Giammanco, Carola Maria Gagliardo, Carlo Maria Barbagallo, Ludovico La Grutta, Patrizia Toia, Federica Brucato, Chiara Scrimali, Teresa Maria Grazia Fasciana, and et al. 2025. "Echocardiographic Calcium Score of Aortic Valve Correlates with Coronary Artery Calcium Score in Heterozygous Familial Hypercholesterolemia" Life 15, no. 3: 506. https://doi.org/10.3390/life15030506
APA StyleCefalù, A. B., Nardi, E., Giammanco, A., Gagliardo, C. M., Barbagallo, C. M., La Grutta, L., Toia, P., Brucato, F., Scrimali, C., Fasciana, T. M. G., Spina, R., Lanza, M., Vitale, F., Noto, D., & Averna, M. (2025). Echocardiographic Calcium Score of Aortic Valve Correlates with Coronary Artery Calcium Score in Heterozygous Familial Hypercholesterolemia. Life, 15(3), 506. https://doi.org/10.3390/life15030506