
Coil Embolization Is Not Justified for Treating Patients with Veno-Occlusive Dysfunction: Case Series and Narrative Literature Review


 ,
,
Abstract
1. Introduction
2. Methods
Case Series of Five Patients
3. Results
Literature Review of Endovascular Coil Embolization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burnett, A.L.; Nehra, A.; Breau, R.H. Erectile Dysfunction: AUA Guideline (2018). American Urological Association Website. Available online: https://www.auanet.org/guidelines/erectile-dysfunction-aua-guideline-(2018) (accessed on 6 June 2018).
- Calzo, J.P.; Austin, S.B.; Charlton, B.M.; Missmer, S.A.; Kathrins, M.; Gaskins, A.J.; Chavarro, J.E. Erectile Dysfunction in a Sample of Sexually Active Young Adult Men from a U.S. Cohort: Demographic, Metabolic and Mental Health Correlates. J. Urol. 2021, 205, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Kessler, A.; Sollie, S.; Challacombe, B.; Briggs, K.; Van Hemelrijck, M. The global prevalence of erectile dysfunction: A review. BJU Int. 2019, 124, 587–599. [Google Scholar] [CrossRef] [PubMed]
- Fang, D.; Peng, J.; Liao, S.; Tang, Y.; Cui, W.; Yuan, Y.; Wu, D.; Hu, B.; Wang, R.; Song, W.; et al. An Online Questionnaire Survey on the Sexual Life and Sexual Function of Chinese Adult Men During the Coronavirus Disease 2019 Epidemic. Sex. Med. 2021, 9, 100293. [Google Scholar] [CrossRef] [PubMed]
- Sansone, A.; Mollaioli, D.; Ciocca, G.; Colonnello, E.; Limoncin, E.; Balercia, G.; Jannini, E.A. “Mask up to keep it up”: Preliminary evidence of the association between erectile dysfunction and COVID-19. Andrology 2021, 18, 35–49. [Google Scholar] [CrossRef]
- Andersson, K.E.; Wagner, G. Physiology of penile erection. Physiol. Rev. 1995, 75, 191–218. [Google Scholar] [CrossRef]
- Kaminetsky, J. Epidemiology and pathophysiology of male sexual dysfunction. Int. J. Impot. Res. 2008, 20, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. FDA approves oral therapy for erectile dysfunction. Am. J. Health Syst. Pharm. 1998, 55, 981–984. [Google Scholar] [CrossRef] [PubMed]
- Dans les champs de l’observation le hasard ne favorise que les esprits préparés. Lecture: University of Lille, 7 December 1854; France.
- Papagiannopoulos, D.; Khare, N.; Nehra, A. Evaluation of young men with organic erectile dysfunction. Asian J. Androl. 2015, 17, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, A.M.; Mehringer, C.M.; Rajfer, J. Anatomy of penile venous drainage in potent and impotent men during cavernosography. J. Urol. 1989, 141, 1353–1356. [Google Scholar] [CrossRef]
- Elhanbly, S.; Abdel-Gaber, S.; Fathy, H.; El-Bayoumi, Y.; Wald, M.; Niederberger, C.S. Erectile dysfunction in smoker. A penile dynamic and vascular study. J. Androl. 2004, 25, 991–995. [Google Scholar] [CrossRef]
- Hatzimouratidis, K.; Giuliano, F.; Moncada, I.; Muneer, A.; Salonia, A.; Verze, P. EAU Guidelines on Erectile Dysfunction, Premature Ejaculation, Penile Curvature and Priapism. 2018. Available online: https://d56bochluxqnz.cloudfront.net/media/16-Male-Sexual-Dysfunction_2017_web.pdf (accessed on 15 March 2018).
- Vardi, Y.; Appel, B.; Kilchevsky, A.; Gruenwald, I. Does low intensity extracorporeal shock wave therapy have a physiological effect on erectile function? Short-term results of a randomized, double-blind, sham controlled study. J. Urol. 2012, 187, 1769–1775. [Google Scholar] [CrossRef] [PubMed]
- Frydman, V.; Pinar, U.; Abdessater, M.; Akakpo, W.; Grande, P.; Audouin, M.; Mozer, P.; Chartier-Kastler, E.; Seisen, T.; Roupret, M. Long-term outcomes after penile prosthesis placement for the Management of Erectile Dysfunction: A single-Centre experience. Basic Clin. Androl. 2021, 31, 34. [Google Scholar] [CrossRef] [PubMed]
- Bettocchi, C.; Ditonno, P.; Palumbo, F.; Lucarelli, G.; Garaffa, G.; Giammusso, B.; Battaglia, M. Penile Prosthesis: What Should We Do about Complications? Adv. Urol. 2008, 2008, 573560. [Google Scholar] [CrossRef] [PubMed]
- Shishehbor, M.H.; Philip, F. Endovascular treatment for erectile dysfunction: An old paradigm revisited. J. Am. Coll. Cardiol. 2012, 60, 2628–2630. [Google Scholar] [CrossRef] [PubMed]
- Kutlu, R.; Soylu, A. Deep dorsal vein embolization with N-butyl-2-cyanoacrylate and lipiodol mixture in venogenic erectile dysfunction: Early and late result. Radiol. Oncol. 2009, 43, 17–25. [Google Scholar] [CrossRef]
- Kim, E.D.; Owen, R.C.; White, G.S.; Elkelany, O.O.; Rahnema, C.D. Endovascular treatment of vasculogenic erectile dysfunction. Asian J. Androl. 2015, 17, 40–43. [Google Scholar]
- Huang, P.-C.; Hsu, G.-L. Vascular Surgery for Erectile Dysfunction. In Encyclopedia of Reproduction; Skinner, M.K., Ed.; Academic Press: Cambridge, MA, USA; Elsevier: Amsterdam, The Netherlands, 2018; Volume 4, pp. 427–436. [Google Scholar] [CrossRef]
- Hsu, G.L. Physiological Approach to Penile Venous Stripping Surgical Procedure for Patients with Erectile Dysfunction. U.S. Patent 8,240,313 B2, 14 August 2012. Available online: https://www.google.com/patents/US20110271966 (accessed on 10 November 2011).
- Schultz, S.G. William Harvey and the Circulation of the Blood: The Birth of a Scientific Revolution and Modern Physiology. N. Physiol. Sci. 2002, 17, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Pardi, N.; Hogan, M.J.; Porter, F.W.; Weissman, D. mRNA vaccines—A new era in vaccinology. Nat. Rev. Drug Discov. 2018, 17, 261–279. [Google Scholar] [CrossRef] [PubMed]
- Wickham, J.E.A.; Fitzpatrick, J.M. Minimally Invasive Surgery. Br. J. Surg. 1990, 77, 721–722. [Google Scholar] [CrossRef]
- Vitek, J. Idiopathic intractable epistaxis: Endovascular therapy. Radiology 1991, 181, 113–116. [Google Scholar] [CrossRef]
- White, R.I., Jr. Embolotherapy in vascular disease. AJR Am. J. Roentgenol. 1984, 142, 27–30. [Google Scholar] [CrossRef]
- Coldwell, D.M.; Stokes, K.R.; Yakes, W.F. Embolotherapy: Agents, clinical applications, and techniques. Radiographics 1994, 14, 623–643. [Google Scholar] [CrossRef]
- Guglielmi, G. History of the genesis of detachable coils. J. Neurosurg. 2009, 111, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kroese, A.C.; de Lange, N.M.; Collins, J.A.; Evers, J.L. Varicocele surgery, new evidence. Hum. Reprod. Update 2013, 19, 317. [Google Scholar] [CrossRef] [PubMed]
- Kaidar-Person, O.; Person, B.; Wexner, S.D. Hemorrhoidal disease: A comprehensive review. J. Am. Coll. Surg. 2007, 204, 102–117. [Google Scholar] [CrossRef]
- Courtheoux, P.; Maiza, D.; Henriet, J.P.; Alachkar, F.; Solassol, A.; Maiza, C.; Théron, J. Correction des insuffisances érectiles d’origine veineuse par ballonnets largables et coils. J. Radiol. 1985, 66, 535–539. [Google Scholar]
- Courtheoux, P.; Maiza, D.; Henriet, J.P.; Vaislic, C.D.; Evrard, C.; Theron, J. Erectile dysfunction caused by venous leakage: Treatment with detachable balloons and coils. Radiology 1986, 161, 807–809. [Google Scholar] [CrossRef]
- Courtheoux, P.; Maiza, D.; Henriet, J.P.; Maiza, C.; Mani, J.; Pelouze, G.; Theron, J. Exploration et traitement par voie endovasculaire des insuffisances érectiles d’origine veineuse [Study and treatment using an endovascular approach of erectile insufficiency of venous origin]. J. Urol. 1987, 93, 37–40. [Google Scholar]
- Courtheoux, P. Embolisation des insuffisances érectiles par fuite veineuse [Embolization in venous erectile insufficiency]. Ann. Urol. 1991, 25, 79–81. (In French) [Google Scholar] [PubMed]
- Schild, H.H.; Mildenberger, P.; Kersjes, W. Effectiveness of platinum wire microcoils for venous occlusion: A study on patients treated for venogenic impotence. Cardiovasc. Intervent. Radiol. 1994, 17, 170–172. [Google Scholar] [CrossRef] [PubMed]
- Malossini, G.; Ficarra, V.; Cavalleri, S.; Morana, G.; Zanon, G.; Mansueto, G.C. Risultati a lungo termine del trattamento percutaneo veno-occlusivo della disfunzione erettile di origine venosa [Long-term results of the veno-occlusive percutaneous treatment of erectile disorders of venous origin]. Arch. Ital. Urol. Androl. 1998, 70, 203–209. (In Italian) [Google Scholar] [PubMed]
- Rebonato, A.; Auci, A.; Sanguinetti, F.; Maiettini, D.; Rossi, M.; Brunese, L.; Carrafiello, G.; Torri, T. Embolization of the periprostatic venous plexus for erectile dysfunction resulting from venous leakage. J. Vasc. Interv. Radiol. 2014, 25, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Carrino, M.; Pucci, P.; Chiancone, F.; Battaglia, G.; Meccariello, C. Embolization of the deep dorsal vein using aethoxysklerol in the treatment of erectile dysfunction resulting from venous leakage. Analysis of our experience with 171 patients. In XXIII Congresso Nationale Auro.it; National Institutes of Health: Stapleton, NY, USA, 2016; Volume 13, pp. 1–12. [Google Scholar]
- Bechara, C.F.; Weakley, S.M.; Kougias, P.; Athamneh, H.; Duffy, P.; Khera, M.; Kobayashi, K.; Lin, P.H. Percutaneous treatment of varicocele with micro-coil embolization: Comparison of treatment outcome with laparoscopic varicocelectomy. Vascular 2009, 17 (Suppl. 3), S129–S136. [Google Scholar] [CrossRef] [PubMed]
- Ficarra, V.; Novara, G.; Artibani, W.; Cestari, A.; Galfano, A.; Graefen, M.; Guazzoni, G.; Guillonneau, B.; Menon, M.; Montorsi, F.; et al. Retropubic, laparoscopic, and robot-assisted radical prostatectomy: A systematic review and cumulative analysis of comparative studies. Eur. Urol. 2009, 55, 1037–1063. [Google Scholar] [CrossRef] [PubMed]
- Makris, G.C.; Efthymiou, E.; Little, M.; Boardman, P.; Anthony, S.; Uberoi, R.; Tapping, C. Safety and effectiveness of the different types of embolic materials for the treatment of testicular varicoceles: A systematic review. Br. J. Radiol. 2018, 91, 20170445. [Google Scholar] [CrossRef]
- Babiker, M.H.; Gonzalez, L.F.; Albuquerque, F.; Collins, D.; Elvikis, A.; Zwart, C.; Roszelle, B.; Frakes, D.H. An In Vitro Study of Pulsatile Fluid Dynamics in Intracranial Aneurysm Models Treated with Embolic Coils and Flow Diverters. IEEE Trans. Biomed. Eng. 2013, 60, 1150–1159. [Google Scholar] [CrossRef] [PubMed]
- Helps, E.P.; McDonald, D.A. Observations on laminar flow in veins. J. Physiol. 1954, 124, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Karia, N.; Balmforth, D.; Lall, K.; Gupta, S.; Bhattacharyya, S. Migration of a Varicocele Coil to the Right Heart. JACC 2020, 15, 2312–2317. [Google Scholar] [CrossRef] [PubMed]
- Moriel, E.Z.; Mehringer, C.M.; Schwartz, M.; Rajfer, J. Pulmonary migration of coils inserted for treatment of erectile dysfunction caused by venous leakage. J. Urol. 1993, 149, 1316–1318. [Google Scholar] [CrossRef]
- Hsu, G.L.; Chang, Y.K.; Chiang, I.N.; Hsu, C.-Y.; Chang, H.-C.; Chueh, S.C.J. A case report of right cardiac ventricle perforation by uncontrolled embolization coil inserted for treating penile veno-occlusive dysfunction. Urol. Case Rep. 2022, 44, 102166. [Google Scholar] [CrossRef]
- Hsu, G.L.; Chang, H.C.; Molodysky, E.; Hsu, C.Y.; Tsai, M.H.; Yin, J.H.; Chen, M.T. The penile fibro-vascular assembly is the last remaining independent vascular compartment to be elucidated in the entire human body. In Proceedings of the 22nd International Society of Sexual Medicine World Webinar Meeting, Virtual, 19–21 November 2021. Zorgniotti-Newman prize-winning paper. [Google Scholar]
- Hsu, G.-L.; Lu, H.-C. Penis Structure—Erection. In Encyclopedia of Reproduction; Skinner, M.K., Ed.; Academic Press: Cambridge, MA, USA; Elsevier: Amsterdam, The Netherlands, 2018; Volume 1, pp. 367–375. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Occurred Time | Symptoms | Signs |
|---|---|---|---|
| ED a | 2008 | Early detumescence of rigid erection, position-dependent | A multiplanar diagnosis workup showed a veno-occlusive dysfunction. |
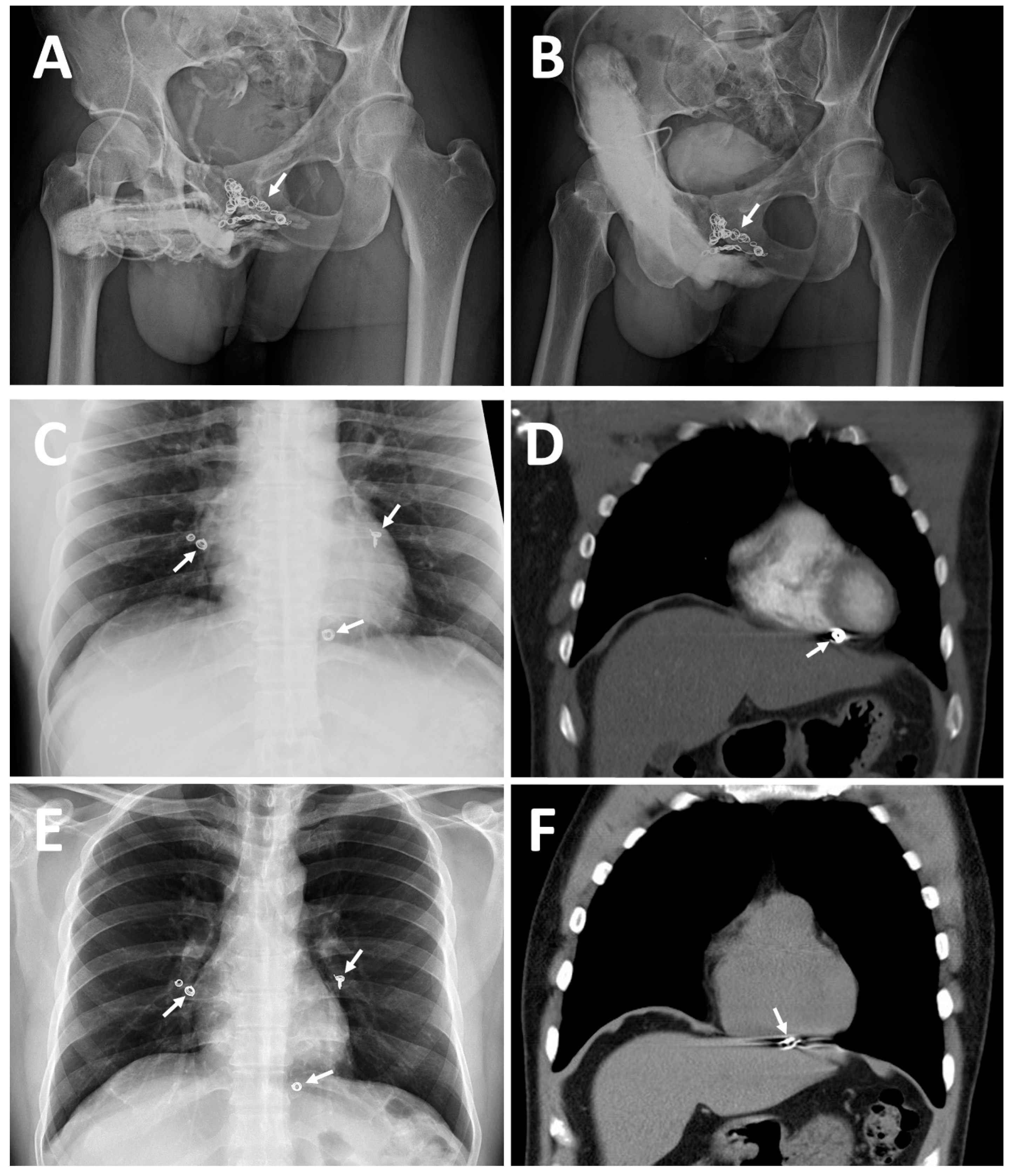
| CE(I) b | 2010 | Same | Acute chest pain was caused by the migration of a dumbbell-shaped coil to the right pulmonary artery. |
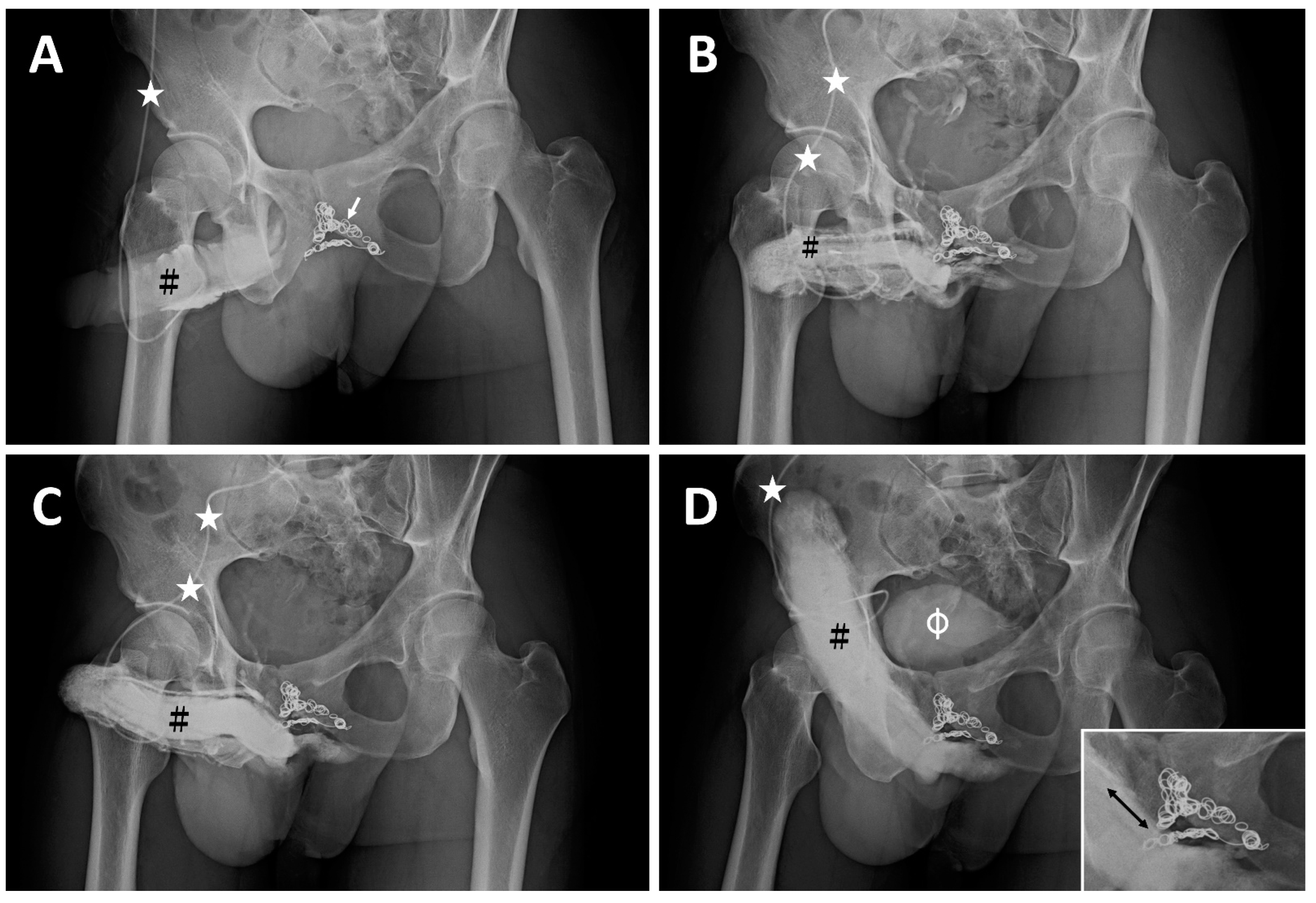
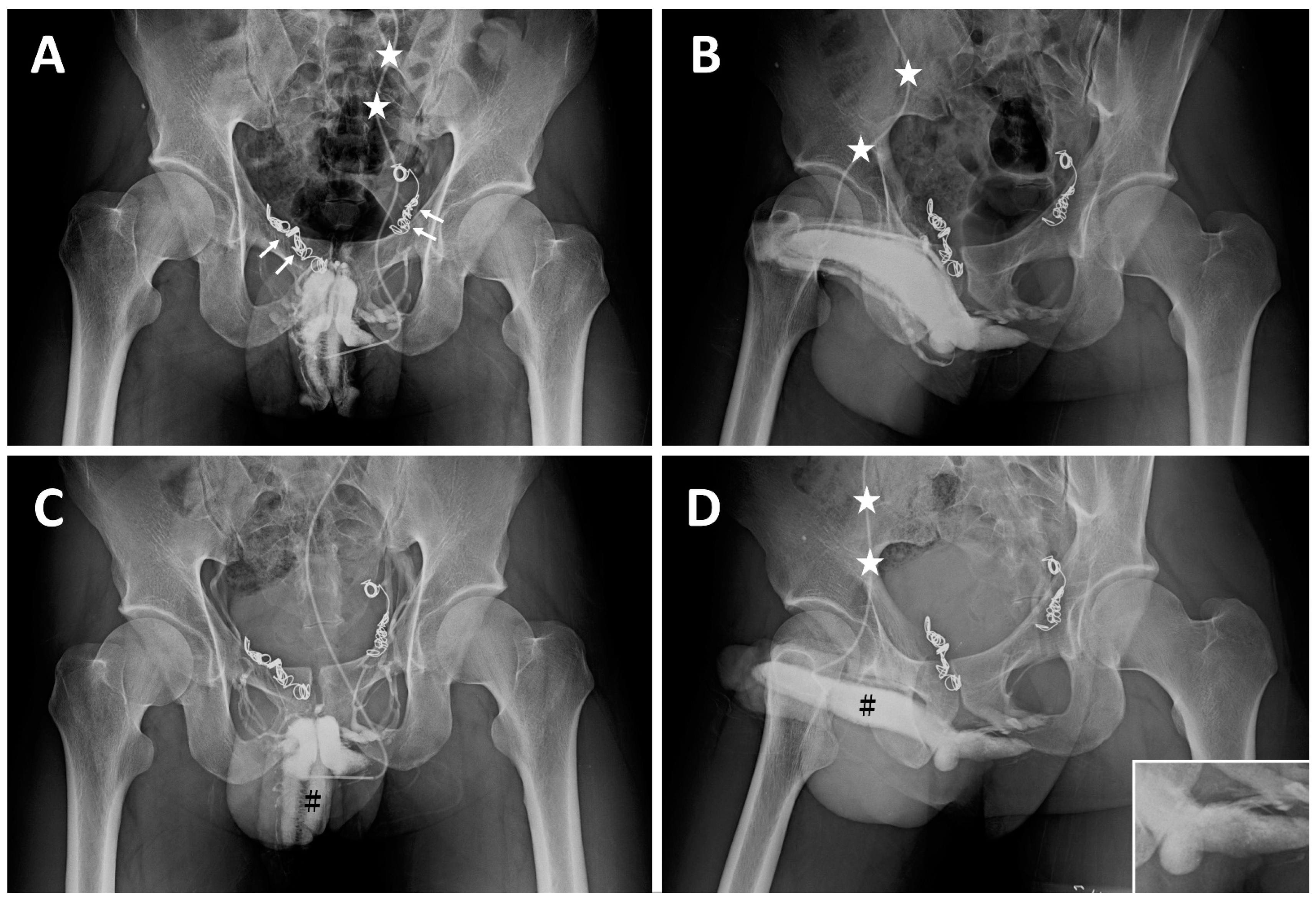
| CE(II) c | November 2012 | Same | A tapeworm-shaped coil was noted in the region of the right iliac vein at 90 degrees to the venous channel. |
| CE(III) d | May 2014 | Same | A pigtail-shaped coil was shown at the left internal pudendal vein level at 90 degrees to the venous channel. |
| Author/Publication (Reference Number) | Patient No. VL/Varicocele | Therapy Method | Follow-Up (Months) | Success Rate %/Follow Available |
|---|---|---|---|---|
| Courtheoux/1985 [31] | 17 | VL a (CE) b | ? | 83.3 (15/18) |
| Courtheoux/1986 [32] | 40 | VL(CE) b | ? | 65.0 (26) |
| Courtheoux/1991 [34] | 46 | VL(CE) b | 8 | 57 |
| Schild/1994 [35] | 19 | VL(CE) b | 25 | 22.2 (24) |
| Malossini/1998 [36] | 17 | VL CR c | NA | 73.4 (11/15) |
| Bechara/2009 [39] | 41 | Varicocele (CE) | 39.3 | 95 |
| Kutlu/2009 [19] | 32 | Varicocele (CE) | ? | Migration |
| Makris/2018 [41] | 898 | Varicocele | ? | 90.9 (9.1) |
| Total | 139/971 | ? | ? | ? |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, K.-S.; Chung, C.-H.; Chang, Y.-K.; Hsu, G.-L.; Tsai, M.-H.; Chueh, J.S. Coil Embolization Is Not Justified for Treating Patients with Veno-Occlusive Dysfunction: Case Series and Narrative Literature Review. Life 2024, 14, 911. https://doi.org/10.3390/life14070911
Chang K-S, Chung C-H, Chang Y-K, Hsu G-L, Tsai M-H, Chueh JS. Coil Embolization Is Not Justified for Treating Patients with Veno-Occlusive Dysfunction: Case Series and Narrative Literature Review. Life. 2024; 14(7):911. https://doi.org/10.3390/life14070911
Chicago/Turabian StyleChang, Ko-Shih, Cho-Hsing Chung, Yi-Kai Chang, Geng-Long Hsu, Mang-Hung Tsai, and Jeff SC Chueh. 2024. "Coil Embolization Is Not Justified for Treating Patients with Veno-Occlusive Dysfunction: Case Series and Narrative Literature Review" Life 14, no. 7: 911. https://doi.org/10.3390/life14070911
APA StyleChang, K.-S., Chung, C.-H., Chang, Y.-K., Hsu, G.-L., Tsai, M.-H., & Chueh, J. S. (2024). Coil Embolization Is Not Justified for Treating Patients with Veno-Occlusive Dysfunction: Case Series and Narrative Literature Review. Life, 14(7), 911. https://doi.org/10.3390/life14070911