Abstract
Repetitive Facilitation Exercise (RFE) is known as an effective rehabilitation method that can elicit brain plasticity. In our previous study, we developed a hemiplegic upper limb rehabilitation system that can train the elbow and shoulder based on RFE theory. The system consists of a selective Arm-DoF constrainable mechanism and a multiple facilitative stimulus timing and duration control system. The selective Arm-DoF constrainable mechanism has three DoF, making it possible to selectively restrict a DoF of the shoulder or elbow. The multiple facilitative stimulation timing and duration control system only has an electrical stimulation source and a vibrator and no large actuators to perform the training exercise. In this study, we undertook an evaluation of the short-term clinical effects of a proposed elbow training program using the hemiplegic upper limb rehabilitation system. The training method consists of two sets, each involving 50 repetitions of the elbow extension exercise programmed in our system. We evaluated the short-term training effects through clinical trials for five stroke patients using the above method. In the evaluation, 10 repetitions of pre/post-tests without any facilitative stimulus were performed before and after the two sets of training. As a result, the maximum angular velocities or the average angular velocities of the elbow extensions improved significantly in most subjects. These results indicate that the quickness or the smoothness of elbow extension movements in the hemiplegic limb improved. Therefore, our clinical experiments support the short-term clinical benefits of the proposed method as well as the practicality of quantitative evaluation using our system.
1. Introduction
Hemiplegia is paralysis that affects only one side of the body, and it is caused by brain damage after a stroke. It is a common condition, and the number of affected patients continues to increase. Conventionally, it has been considered that if damaged nerve cells in the brain are not recovered, the treatment of paralysis is impossible. However, a level of “brain plasticity” has been found, aiding in the effectiveness of rehabilitation. This is a phenomenon in which the surrounding brain neurons make a new neural network, acting in place of the dead ones [1,2,3,4].
Functional recovery in a hemiplegic stroke patient is directly related to the improvement of quality of life (QOL) and activities of daily living (ADL). Training involving upper extremity exercises is particularly important in sub-acute rehabilitation after stroke [5]. In particular, the training of elbow extension directly improves ADL, such as drinking water, pushing a button, and changing clothes [4,5,6,7].In order to improve paralysis in the hemiplegic limb, “Repetitive Facilitation Exercise” (RFE; Kawahira method) is considered an effective rehabilitation method that can elicit brain plasticity [8,9,10,11]. The aim of RFE is to induce brain plasticity; it involves two stages: separating the targeted movement from synergic movement with the application of facilitative stimulations and performing 100 repetitions. Facilitative stimulations include the stretch reflex, the skin muscular reflex, shrinkable electrical stimulation (SES) [12], vibratory stimulation (VS), auditory stimulation, and visual stimulation. However, there are some issues that make it difficult to train therapists in RFE techniques; accordingly, there is a shortage of therapists who can perform RFE treatment. Therefore, improving both the quality and the quantity of treatment applications is necessary by developing rehabilitation devices that can perform RFE treatment [5,13,14].
Concerning the research on rehabilitation training using RFE, Amano et al. [15] assessed the feasibility of applying a robot to improve the motor control and function of the hemiparetic upper extremity in patients who had suffered a chronic stroke, with neuromuscular electrical stimulation and vibratory stimulation applied to facilitate agonist muscle contraction. However, this rehabilitation method cannot completely separate the synergic movements between the elbow and shoulder joints.
Previously, most rehabilitation devices have employed passive power assistance provided by actuators, such as motors or artificial muscles [16,17,18,19]. There are a few studies that have focused on separating voluntary movement from the synergic movement of hemiplegic limbs. Although our rehabilitation system does not use actuators such as power-assist robots, it can separate the synergic movement and thus isolate the joint movements of the hemiplegic upper limb [4,5,6]. Because we set the RFE training posture as a supine position, our device does not require any actuators because the passive elbow flexion required to trigger the stretch reflex can be assisted by gravity acting on the patient’s arm [4,6].
Rehabilitation training is most effective when it promotes voluntary movements. It is necessary for post-stroke patients with upper limb hemiplegia to have specific synergic movements separated from voluntary movements in their individual joints. In order to be able to perform coordinated movement, it is important for hemiplegic patients to achieve this separation [4]. However, when a hemiplegic patient is training alone, voluntary movement tends to be accompanied by synergic movement. Training that does not separate these movements will cause adverse effects. Therefore, it is important for hemiplegic patients to separate voluntary from synergic movements in their training [7].
Hence, in our previous research, a selective Arm-DoF constrainable mechanism (Figure 1) and multiple facilitative stimulation timing and duration control systems for hemiplegic upper limb rehabilitation were developed, as introduced in [4,6]. Our rehabilitation system facilitates deliberate, voluntary movements in the patient using the two aforementioned devices. Moreover, preliminary clinical experiments on hemiplegic patients using this system were reported in [5]. In this paper, we report on the short-term clinical effects of a newly proposed training program using this system for hemiplegic elbow extension rehabilitation.
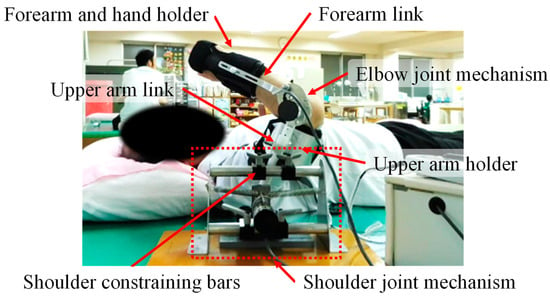
Figure 1.
Selective Arm-DoF constrainable mechanism.
2. A Selective Arm-DoF Constrainable Mechanism and Multiple Facilitative Stimulation Control System
2.1. Selective Arm-DoF Constrainable Mechanism
Figure 1 shows the device mounted on the right arm of a patient. This device includes two link mechanisms that can only move in the DoF of purposeful movements of the shoulder and elbow joints. The upper arm and forearm are held by these links. The main structural materials of this device are an aluminum alloy and non-metallic materials, meaning the device is lightweight and not oppressive on the arm of the user [4]. The selective Arm-DoF constrainable mechanism is adjustable so that it can fit the width and length of the upper limb of any patient, and it is able to limit the movement direction and range depending on the training being given, besides being able to aid the movement of the elbow joint. In fixing the forearm to the link mechanism, a brace is used to establish an appropriate position for training [4]. The range of shoulder movement is adjustable in intervals set on the shoulder-constraining bar, and this bar can be fixed or adjusted. The range of movement of the elbow joint is constrained by the elbow joint mechanism [4].
2.2. Elbow Joint Mechanism
The elbow joint mechanism enables elbow rotation, and the range of motion of the elbow joint can be set independently. An encoder is built into the rotation axis of the elbow joint mechanism [4]. Figure 2 shows the movements applied in the elbow extension–flexion exercise. The elbow joint has only one DoF, either flexion or extension. To avoid damage of the elbow joint, the rotational angle of the elbow should be limited to within -10° extension to 100° flexion. This mechanism can aid in the training of both the right and left arms [4]. The training posture is the same as that used in manual RFE training; in this training posture, the weight of the upper arm accelerates the flexion motion of the elbow, which can induce a stretch reflex in the triceps’ brachii muscle without any actuators.
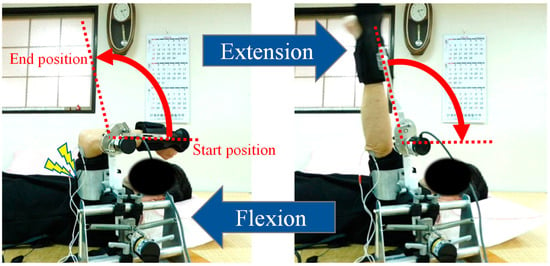
Figure 2.
Elbow extension-flexion training exercise. SES and VS are given at predetermined timings during extension-flexion movements.
2.3. Multiple Facilitative Stimulation Timing and Duration Control System
An overview of the system configuration is shown in Figure 3. The encoder counter is connected to a laptop computer via a USB cable. The software on the laptop processes the count data provided by the rotary encoders set at each joint axis of the selective Arm-DoF constrainable mechanism. The computer records data on the joint angle and angular velocity. Based on the data regarding joint angle and angular velocity, it is possible to control the timing and duration of the SES and VS.
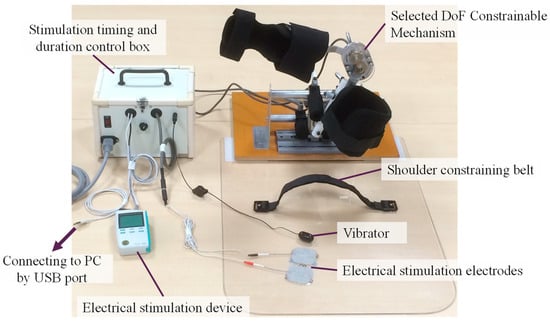
Figure 3.
Configuration of the timing and duration control system for the SES and VS.
The points of stimulation of the SES and VS applied in the elbow extension training program are shown in Figure 4. Two electrodes are placed over the tricep brachii muscle [5]. The intervention timing and duration of the SES and VS are outlined in [5].
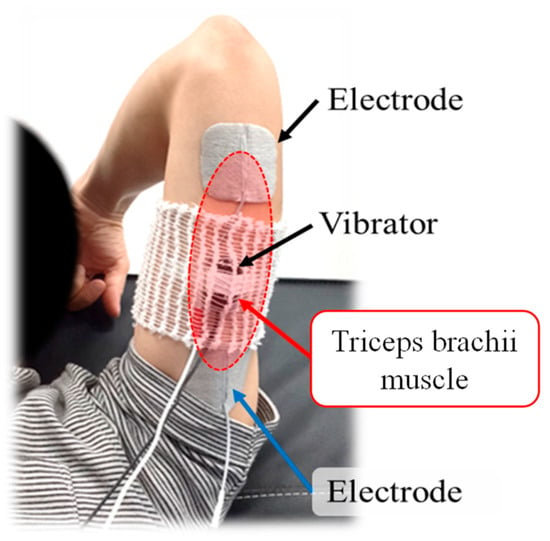
Figure 4.
Stimulation points of the SES and VS.
In this study, the conditions of the SES were as follows: The pulse width was 150 μs, and the pulse frequency was 50 Hz. The current intensity was set at different values optimized for each patient so as to avoid pain and muscle stiffness, with reference to the SES method outlined in [5,10]. The intervening end angle of the SES was set to 95% of the maximum movement range in order to prevent muscle cramps. The frequency of the VS was approximately 100 Hz.
2.4. Method of Rehabilitation Training and Evaluation
Figure 5 shows the values of the parameters applied when evaluating the training effects. The maximum angular velocity refers to the celerity of the training exercise, while the average angular velocity refers to the smoothness of the training exercise. Because the first and last points of the exercise training data are not stable, they were not used for the evaluation of the training effects. As such, when the training exercise was carried out 10 times, the maximum angular velocity data were only collected for the second repetition to the ninth. The method applied to evaluate the training effects involved a comparison of the median values of the maximum angular velocity, recorded pre-training and post-training [5]. The average angular velocity is defined as follows:
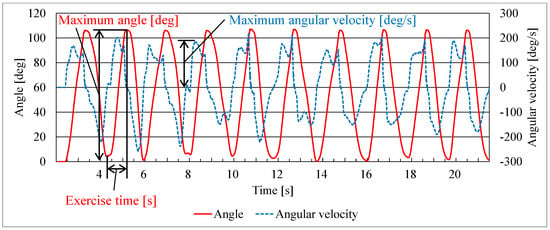
Figure 5.
Definition of parameters on evaluations.
3. Clinical Experiments of Training
3.1. Aim of the Clinical Experiment
Our previous study showed that a combination of SES and VS is more effective than training without either. Furthermore, the study suggests that undertaking more than three sets of 10 repetitions, combined with SES and VS, significantly improved the training effects [5]. However, in previous studies, the number of repetitions of the training movement was as low as 10; thus, the effects of performing 100 repetitions, as in RFE, are unclear. Accordingly, in this study, we proposed a training program that involved a total of 100 repetitions of the training exercise, with repetitions increasing per set in combination with SES and VS, as inspired by RFE theory. The 100-repetition exercise was divided into two sets of 50 repetitions each to maintain the patient’s concentration and prevent muscle fatigue. In these experiments, the number of training exercises in combination with SES and VS was set at 50 repetitions in each training set, and two sets were performed to determine the effects of repeated RFE training.
All study participants, or their legal guardians, provided informed written consent prior to study enrollment. In addition, we obtained approval from the Institutional Ethics Committee of the cooperating medical institution.
3.2. Methods of the Clinical Experiment
The configuration of the clinical experiment is shown in Table 1. The proposed training method comprises two training sets; one set comprises 50 repetitions of the purposeful training movement, as programmed into our system. In order to evaluate the effects of training, 10 repetitions were performed pre/post-test without any facilitative stimulations before and after the two sets of training. In the test set, for each set of 10 repetitions, the data regarding the maximum angular velocities and average angular velocities were collected from the second repetition to the ninth. In the training set, the data regarding the maximum angular velocities and average angular velocities were collected from the 2nd repetition to the 49th. The method applied for the evaluation of the effects of training was a comparison of the median values of the maximum and average angular velocities yielded in the test set before versus after the training set.

Table 1.
Configuration of the clinical experiment.
3.3. Subjects of the Clinical Experiment
We evaluated the short-term training effects through clinical trials involving five stroke patients using the above method. These subjects comprised two convalescent stroke patients and three chronic stroke patients. The details of these subjects are shown in Table 2.
Table 2.
Details of the subjects used in the clinical experiment.
3.4. Results of the Clinical Experiment
The results of the experiment for subjects A–E are shown in Table 3. Figure 6, Figure 7, Figure 8, Figure 9 and Figure 10 show the results for the maximum angular velocities and average angular velocities in each set. These results show that the maximum angular velocities of elbow extension improved significantly in most subjects after training with a combination of SES and VS. In addition, in almost all cases, we observed significant improvements in terms of the change observed in the rate of average angular velocities between the pre-test and post-test periods. As these results show, the improvements in the maximum angular velocity in the first set are greater than those in the second set. The change rate of the maximum angular velocity between the mid-test and post-test periods did not improve much, even over 50 repetitions. In some cases (for example, in subjects D and E), improvements in either the maximum angular velocity or average angular velocity were seen, but not both. Interestingly, in subject C, we saw no significant change in the maximum angular velocity. However, in the results for the average angular velocity, we can note a significant difference in the improvement rate of the average angular velocity in the evaluation test from before to after the first training set.
Table 3.
The result of clinical experiments.
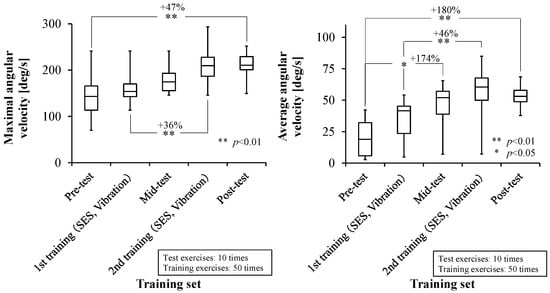
Figure 6.
Maximum angular velocities (Left) and average angular velocities (Right) of subject A.
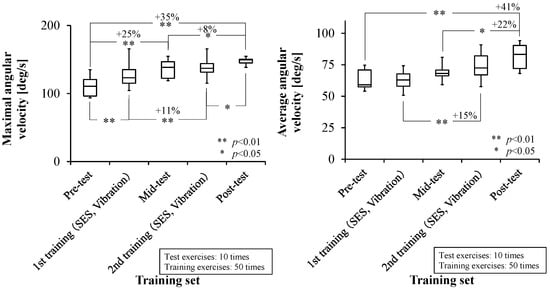
Figure 7.
Maximum angular velocities (Left) and average angular velocities (Right) of subject B.
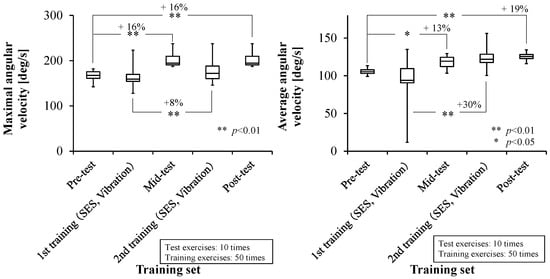
Figure 8.
Maximum angular velocities (Left) and average angular velocities (Right) of subject C.
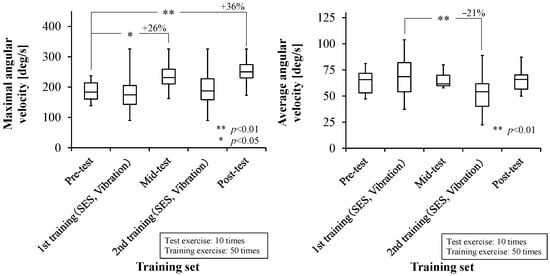
Figure 9.
Maximum angular velocities (Left) and average angular velocities (Right) of subject D.
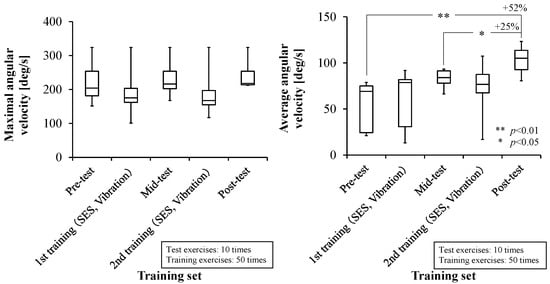
Figure 10.
Maximum angular velocities (Left) and average angular velocities (Right) of subject E.
Surprisingly, large effects of the training were observed in chronic patients (over 6 months from stroke onset).
4. Discussion
As the results of these clinical experiments show, the combination of SES and VS yielded good effects, as seen in previous studies [4,5,6]. This demonstrates the effectiveness of the VS and SES combination when used as a facilitative stimulus applied in the hemiplegic rehabilitation of elbow extensions. These results also show that a tonic vibration reflex (TVR) related to VS was easily induced by increasing the biopotential excitation level of the target muscle attributed to SES. TVR is the phenomenon whereby a muscle contracts due to a spinal reflex, itself arising when a muscle spindle senses a stimulus resulting from a change in muscle length and shrinkage rate due to vibration [5,20]. Besides this, it is also considered that the training posture employed could induce a stretch reflex in the triceps’ brachii muscle without the use of any actuator; this is due to the weight of the upper arm accelerating the flexion of the elbow.
In addition, it was suggested that increasing the number of repetitions per set could produce consistent improvements in the motion velocity after training. In manual RFE, the training movements are usually repeated 100 times; therefore, it was theorized that a greater training effect could be yielded by employing the RFE training method. Another significant aspect of the above results reveals that by automating RFE training using mechatronics, it is possible to not only statistically verify the effectiveness of the training method itself but also to quantitatively evaluate the training’s immediate effects, with a focus on the individual patient.
In most cases, when assessing the change rate of the maximum or average angular velocity pre-test versus post-test, we observed significant improvements. It is assumed that improvements in the maximum angular velocity indicate improved agility; on the other hand, improvements in the maximum angular velocity indicate improved smoothness of movement. However, there are some cases that showed no significant improvement in the maximum angular velocity. In these cases, we saw significant improvements in average angular velocity, and so these results suggest that only the smoothness of movement was improved. Thus, these results indicate that the speed of movement was broadly improved. As such, after observing both the maximum angular velocities and average angular velocities, we can infer the quality of the effects of training.
As shown by most of the results, the improvements in the maximum and average angular velocities achieved in the first training are greater than those achieved in the second training. This result suggests that the ratios of the training effects are not greatly improved over the 50 training exercises. Based on these facts, it seems that around 100 repetitions would be appropriate, and increasing the number of training repetitions to over 100 would be inefficient.
Furthermore, interestingly enough, large training effects were observed in patients in the chronic phase group for whom over 6 months had elapsed from stroke onset. This suggests that automatic training employing SES and VS in addition to RFE is effective even in chronic patients.
These results only indicate short-term training effects, and thus, we have yet to verify the more long-term training effects. Even if the effects imparted by the training increase movement momentarily, it is unclear what the long-term effects might be when training is continued daily for some weeks. A study by Amano et al. [15] showed medium-term training effects over two weeks derived from robotic rehabilitation using a combination of electrical stimulation and VS. Therefore, the approach in this study could yield not only short-term training effects but also medium- to long-term effects.
5. Conclusions
In this study, we proposed a hemiplegic upper limb rehabilitation system that can train the elbow and shoulder independently. The system consists of a selective Arm-DoF constrainable mechanism and a multiple facilitative stimulation timing and duration control system. The selective Arm-DoF constrainable mechanism enables the separation of synergic movements during elbow extension training by constraining each individual joint throughout the training exercise. Furthermore, this system permits control of the timings of the interventions and the duration of SES and VS according to the angle and angular velocity in the elbow joint. This system employs no actuators, such as power-assist robots, which improves safety and lowers costs.
Our previous study showed that using a combination of SES and VS is more effective than using neither. Furthermore, this study suggests that undertaking more than three training sets of 10 repetitions, combined with SES and VS, improved the training effects. Accordingly, in this study, we have proposed a training program comprising a total of 100 repetitions of the training exercise using the hemiplegic upper limb rehabilitation system. The proposed training method consists of two sets; each set comprises 50 repetitions of the elbow extension exercise, as programmed into our system. We evaluated the short-term training effects through clinical trials on five stroke patients using the above method. In order to evaluate the training effect, 10 repetitions of pre/post-tests without any facilitative stimuli were performed before and after the two sets of training.
Focusing on the evaluation of the instrumentation, the maximum angular velocities of elbow extensions improved significantly in most subjects. These results indicate that the speed of the elbow extension movements in the hemiplegic limb improved. In addition, in most cases, we observed significant improvements in the change rate of the average angular velocities between the pre-test and post-test periods. These results indicate that the smoothness of the elbow extension movements in the hemiplegic limb improved. In particular, in some cases (for example, in subjects D and E), improvements in either the maximum angular velocities or average angular velocities were seen, but not both. These results demonstrate the value of the training, both in terms of the maximum angular velocity and average angular velocity. Interestingly, significant training effects were observed in chronic patients for whom over 6 months had elapsed since the stroke onset. The clinical experiments demonstrated the short-term clinical effects of the proposed method, as well as the practicality of the quantitative evaluations using our system.
In future research, it will be necessary to verify more long-term training effects, such as those for when training is continued daily for a number of weeks. Moreover, it is thought that quantitative evaluations of this system could be made more effective by evaluating correlations with data provided by existing rehabilitation evaluation methods, such as FMA (Fugl-Meyer Assessment), FIM (Functional Independence Measure), or ARAT (Action Research Arm Test).
Author Contributions
Conceptualization, K.T. and Y.Y.; methodology, K.T. and Y.Y.; software, K.T.; validation, K.T.; formal analysis, K.T.; investigation, K.T.; resources, K.T.; data curation, K.T.; writing—original draft preparation, K.T.; writing—review and editing, K.T. and Y.Y.; visualization, K.T.; supervision, Y.Y.; project administration, Y.Y.; funding acquisition, K.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Japan Society for the Promotion of Science KAKENHI Grant Numbers JP26917020, and JP15H00331.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to perspective of personal information protection.
Acknowledgments
The authors would like to thank Tomokazu Noma, Megumi Shimodozono and Kazumi Kawahira for their clinical experiment supports and advices to this research. We are also grateful to the anonymous reviewers of this article for their very constructive contributions.
Conflicts of Interest
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Bach-y-Rita, P. Brain plasticity as a basis for recovery of function in humans. Neuropsychologia 1990, 28, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Yukihiro, H. Brain Plasticity and Rehabilitation in Stroke Patients. J. Nippon. Med. Sch. 2015, 82, 4–13. [Google Scholar]
- Kawahira, K.; Shimodozono, M.; Etoh, S.; Kamada, K.; Noma, T.; Tanaka, N. Effects of Intensive Repetition of a New Facilitation Technique on Motor Functional Recovery of the Hemiplegic Upper Limb and Hand. Brain Inj. 2010, 24, 1202–1213. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, K.; Yu, Y.; Noma, T.; Hayash, R.; Matsumoto, S.; Shimodozono, M.; Kawahira, K. Research of Rehabilitation Aid System by DOF Constraintable Mechanism and NMES for Hemiplegic Upper Limbs. In Proceedings of the 2015 IEEE/ASME International Conference on Advanced Intelligent Mechatronics, Busan, Republic of Korea, 7–11 July 2015. [Google Scholar]
- Taniguchi, K.; Yu, Y.; Noma, T.; Yamanaka, H.; Fukuda, I.; Matsumoto, S.; Shimodozono, M.; Kawahira, K. Training Condition Research on Selective DOF Constrainable Rehabilitation Unit with Shrinkable Electrical and VS Timing and Duration Control System for Hemiplegic Shoulder-Flexion and Elbow-Extension. In Proceedings of the IEEE International Conference on Robotics and Biomimetics, Qingdao, China, 3–7 December 2016. [Google Scholar]
- Taniguchi, K.; Yu, Y.; Noma, T.; Hayash, R.; Matsumoto, S.; Shimodozono, M.; Kawahira, K. Research of Training and Evaluation Aid Device with DOF Selective Constraint Mechanism for Hemiplegic Upper Limbs Rehabilitation. In Proceedings of the 2015 IEEE International Conference on Mechatronics, Nagoya, Japan, 6–8 March 2015. [Google Scholar]
- Noma, T.; Matsumoto, S.; Shimodozono, M.; Iwase, Y.; Kawahira, K. Novel neuromuscular electrical stimulation system for the upper limbs in chronic stroke patients: A feasibility study. Am. J. Phys. Med. Rehabil. 2014, 93, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Kawahira, K.; Shimodozono, M.; Ogata, A.; Tanaka, N. Addition of Intensive Repetition of Facilitation Exercise to Multidisciplinary Rehabilitation Promotes Motor Functional Recovery of the Hemiplegic Lower Limb. J. Rehabil. Med. 2004, 36, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Kawahira, K.; Noma, T.; Iiyama, J.; Etoh, S.; Ogata, A.; Shimodozono, M. Improvements in Limb Kinetic Apraxia by Repetition of a Newly Designed Facilitation Exercise in a Patient with Corticobasal Degeneration. Int. J. Rehabil. Res. 2009, 32, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Shimodozono, M.; Noma, T.; Nomoto, Y.; Hisamatsu, N.; Kamada, K.; Miyata, R.; Matsumoto, S.; Ogata, A.; Etoh, S.; Basford, J.R.; et al. Benefits of a Repetitive Facilitative Exercise Program for the Upper Paretic Extremity after Subacute Stroke: A Randomized Controlled Trial. Neurorehabilit. Neural Repair. 2013, 27, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, K.; Etoh, S.; Tanoue, A.; Kamezawa, T.; Shimodozono, M. Repetitive facilitative exercise and task-oriented training in a subacute stroke patient with moderate upper paralysis: A case study. Jpn. Occup. Ther. Res. 2022, 41, 113–122. (In Japanese) [Google Scholar]
- Yu, Y.; Tomiyama, D.; Shimodozono, M.; Ooe, K.; Hayashi, R.; Kawahira, K. Shrinkable Electrical Stimulation and Characterization for Prompting Effective Stretch Reflex in Repetitive Facilitation Exercise to the Hemiplegic Finger. In Proceedings of the 15th SICE System Integration Division Annual Conference, Tokyo, Japan, 15–17 December 2014. (In Japanese). [Google Scholar]
- Yu, Y.; Nagai, M.; Matsuda, J.; Kawahira, K.; Hayashi, R. Control Strategy of an Active Arm Weight-Bearing Unit for Hemiplegic Arm Rehabilitation. In Proceedings of the 2014 IEEE International Conference on Information and Automation, Hulunbuir, China, 28–30 July 2014. [Google Scholar]
- Yu, Y.; Iwashita, H.; Kawahira, K.; Hayashi, R. Development of Rehabilitation Device for Hemiplegic Fingers by Finger-Expansion Facilitation Exercise with Stretch Reflex. In Proceedings of the 2013 IEEE International Conference on Robotics and Biomimetics, Shenzhen, China, 12–14 December 2013. [Google Scholar]
- Amano, Y.; Noma, T.; Etoh, S.; Miyata, R.; Kawamura, K.; Shimodozono, M. Reaching exercise for chronic paretic upper extremity after stroke using a novel rehabilitation robot with arm-weight support and concomitant electrical stimulation and vibration: Before-and-after feasibility trial. Biomed. Eng. Online 2020, 19, 28. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, A.; Chin, T.; Oyabu, H. Robotic Arm Orthosis using Pneumatic Artificial Rubber Muscle for Rehabilitation Training. J. Jpn. Fluid. Power Syst. Soc. 2007, 38, 194–198. (In Japanese) [Google Scholar]
- Mita, M.; Suzumori, K.; Kudo, D.; Saito, K.; Chida, S.; Hatakeyama, K.; Shimada, Y.; Miyakoshi, N. Utility of a wearable robot for the fingers that uses pneumatic artificial muscles for patients with post-stroke spasticity. Jpn. J. Compr. Rehabil. Sci. 2022, 13, 12–16. (In Japanese) [Google Scholar] [CrossRef] [PubMed]
- Koizumi, S.; Chang, T.-H.; Nabae, H.; Endo, G.; Suzumori, K.; Mita, M.; Saitoh, K.; Hatakeyama, K.; Chida, S.; Shimada, Y. Soft Robotic Gloves with Thin McKibben Muscles for Hand Assist and Rehabilitation. In Proceedings of the 2020 IEEE/SICE International Symposium on System Integration (SII), Honolulu, HI, USA, 12–15 January 2020; pp. 93–98. [Google Scholar]
- Mendoza, M.J.; Gollob, S.D.; Lavado, D.; Koo, B.H.B.; Cruz, S.; Roche, E.T.; Vela, E.A. A Vacuum-Powered Artificial Muscle Designed for Infant Rehabilitation. Micromachines 2021, 12, 971. [Google Scholar] [CrossRef] [PubMed]
- Eklund, G.; Hagbarth, K.E. Normal variability of tonic vibration reflexes in man. Exp. Neurol. 1966, 16, 80–92. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).