Abstract
Guaranteeing the safety of swimming pools is a paramount concern worldwide. Robust risk assessment and management practices are crucial for ensuring public safety. A comprehensive understanding of the chemical equilibrium required in pool water and a thorough assessment of the associated physicochemical, microbiological, operational, and maintenance risks have become prerequisites for effective swimming pool management. The aim of the present study was to identify, for the first time in Greece, all the possible hazards at different swimming pools as a first step of the scientific-based risk assessment procedure. Six distinct swimming pools, comprising two open sports pools, two indoor pools, and two children’s pools designed for baby swimming, were included. Water samples were collected for physicochemical and microbiological analyses, and on-site inspections were conducted across the swimming pools. A detailed evaluation of potential identified hazards categorized risks based on their level of impact and likelihood of occurrence; mitigation measures were proposed. Comprehensive risk assessments are essential for swimming pools, as they need to address the specific hazards and vulnerabilities of each facility.
1. Introduction
Swimming pools constitute artificially constructed aquatic environments intended for diverse applications, including recreational, competitive athletic events, and therapeutic purposes. Swimming pools encompass a wide spectrum of structures, ranging from residential pools to large, complex aquatic centers. On a global level, there are around 13 million swimming pools, approximately 4.4 million (29%) of which are found in Europe [1]. The global swimming pool construction market size was valued at USD 8315.8 million in 2023 and is projected to reach USD 12,282.5 million by 2032, growing at a compound annual growth rate (CAGR) of 4.1% during the forecast period (2024–2032). Swimming pool construction market growth is attributed to the rising health awareness among people and the growing tourism business, increasing the demand for hotel accommodations [2].
In Greece, there is currently no national organization responsible for a unified, comprehensive, and systematic monitoring of pool operations. Instead, pools are monitored in a fragmented and inconsistent manner, if at all, by various entities, resulting in poor attendance data. Since Greece is among the leading touristic destinations in the world and tourism is one of the country’s most important economic sectors, there is a corresponding increase in hotel swimming pools; however, all other kinds of swimming pools are also accommodated in the country [3,4].
The successful design, construction, and ongoing maintenance of swimming pools necessitate a multifaceted integration of engineering principles, water chemistry expertise, and public health considerations. Despite swimming pool use benefits, the concurrent use of swimming pools by heterogeneous groups presents significant public health and safety challenges. Foremost among these is microbial contamination, which remains a persistent issue despite advancements in water quality control and the implementation of rigorous disinfectant monitoring protocols [5,6]. Suboptimal disinfection practices can facilitate the transmission of waterborne pathogens, thereby posing considerable risks to public health. Additionally, the chemical agents employed in water treatment, such as chlorine, can interact with natural organic matter to generate disinfection by-products (DBPs), some of which are linked to both carcinogenic and non-carcinogenic health outcomes [7]. These concerns are exacerbated in indoor aquatic facilities, where airborne volatile compounds can adversely affect the respiratory health of both swimmers and personnel [8]. Physical safety is another critical dimension requiring attention. Non-compliance with safety protocols can lead to accidents, ranging from minor injuries to severe incidents such as spinal cord trauma or fatalities. Such occurrences have far-reaching implications, disrupting societal stability and imposing significant economic burdens. Indoor pools, in particular, exhibit higher rates of accidents, necessitating targeted interventions to enhance safety [9].
The implementation of rigorous health and safety frameworks is imperative for mitigating these risks. Pivotal to these frameworks is risk assessment, a systematic process that evaluates the likelihood and consequences of potential hazards. Risk assessment serves as the foundation for informed decision-making, enabling stakeholders to identify vulnerabilities, prioritize safety measures, and allocate resources effectively. By quantifying the probability and severity of adverse events, risk assessments provide actionable insights that guide the development of prevention strategies and contingency plans. This proactive approach not only reduces the occurrence of incidents but also fosters a safer and more resilient operational environment [10].
Effective risk management, as defined by the International Organization for Standardization, involves identifying potential hazards, assessing their likelihood and severity, and implementing measures to minimize adverse outcomes. Risk assessment is pivotal to this process, enabling stakeholders to prioritize safety objectives and allocate resources efficiently. This is especially applicable in the case of swimming pools, where hazard identification—including microbial threats, chemical risks, and structural vulnerabilities—is the cornerstone of any comprehensive safety program [11].
Various studies underscore the critical role of proactive safety measures in pool management. For instance, assessments have shown that maintaining water quality is as vital as ensuring physical safety, as both factors are interdependent in creating a secure aquatic environment [12]. Research further indicates that robust inspection protocols and compliance monitoring are essential for addressing persistent safety gaps. In practice, this involves regular microbial testing, monitoring of chemical concentrations, and ensuring adherence to structural and operational standards [13,14].
In conclusion, even though swimming pools epitomize the intersection of health promotion, recreation, and economic utility, their benefits are contingent upon effective health and safety management. By integrating rigorous risk assessment methodologies and fostering a culture of safety, stakeholders can ensure that pools remain safe, enjoyable, and sustainable environments. This commitment to excellence in pool management not only protects public health but also strengthens the socioeconomic fabric of communities worldwide.
Swimming pool regulations differ across countries due to varying approaches by health authorities, influenced by each nation’s unique social, economic, and cultural context. Greek legislation governing swimming pool operations and water quality remains severely outdated, dating back to 1973 [15]. Despite several amendments over the years, these changes have not modernized the standards for water quality parameters or microbiological hygiene (Table 1).

Table 1.
Summarized requirements of Greek legislation for the Operation of Swimming Pools, ensuring water quality and safety for users [15].
In contrast, modern international standards, including the European framework since 2008 and WHO Guidelines [9,16,17], emphasize risk assessment approaches. Risk assessment in this context is scientifically defined as “a systematic process encompassing the following stages: (i) hazard identification, (ii) hazard characterization, (iii) exposure assessment, and (iv) risk characterization”. This structured methodology informs the formulation and refinement of effective risk management protocols. To optimize waterborne pathogen management, the World Health Organization (WHO) advocates for a risk analysis paradigm increasingly recognized as best practice in water utility sectors, including drinking water management [9,18].
The failure of Greek legislation to integrate modern risk-based methodologies highlights an urgent need for legislative reform. Current practices lag far behind international benchmarks, risking public health and undermining effective pool water management. The aim of the present study was to identify, for the first time in Greece, all the possible hazards—physical, chemical, microbiological, construction, and operational—at various types of swimming pools as a first step of the scientific-based risk assessment procedure. Our approach involved demonstrating the methodology’s utility in common settings, using a high-volume sampling strategy within each pool. We intended to thoroughly map risk factors across select environments. The analysis of a large number of samples within each pool allowed for a detailed and robust evaluation of the methodology’s effectiveness and its ability to capture variations in water quality over time. In response to the limitations of the existing legislative framework, established in 1973 and lacking a comprehensive risk-based approach, this study proposes a novel paradigm shift. This innovative methodology facilitates the identification and mitigation of emerging hazards, including novel pathogens and chemical contaminants, which may be overlooked by traditional monitoring techniques.
2. Materials and Methods
This analytical-observational study was conducted across six distinct swimming pools, comprising two open sports pools, two indoor pools, and two children’s pools designed for baby swimming. A total of 168 water samples were collected and microbiologically analyzed. The water samples were collected from September 2023 to July 2024 on different days and times for each swimming pool to ensure representativeness. Sampling was performed according to ISO 19458 guidelines [19]. The samples were collected from strategic points within the pool basins, focusing on areas near outlets such as skimmers or gutters. Specific sampling locations included the water entry point, the water exit point, the center of the pool (20 cm below the water surface), and areas before and after filtration systems. The water samples were collected in sterile 1 L containers, each containing 20 mg of sodium thiosulfate to neutralize any residual chlorine or other oxidizing biocides. The samples were promptly labeled and stored temporarily in a cold box at a temperature of 5 ± 3 °C shielded from direct light and transported to the laboratory within 24 h after collection.
The enumeration of E. coli, total coliform bacteria, Pseudomonas aeruginosa, and intestinal enterococci was performed using the membrane filtration method. Briefly, the membrane filtration method involved passing 100 mL of a water sample through a sterile membrane filter composed of cellulose esters, with a 0.45 µm pore size (Whatman ME25/21 47 mm Sterile Mixed Cellulose Ester Filter, Cytiva, Marlborough, MA, USA, https://www.cytivalifesciences.com/en/us), which effectively retained microorganisms present in the sample. Subsequently, the membrane was aseptically transferred onto the selective or differential culture medium within a Petri dish, as described in the relative ISO methods; after incubation at 36 ± 2 °C for 21–24 h, typical colonies were enumerated. Confirmation procedures were implemented according to ISO methods. Enumeration of culturable microorganisms was carried out by inoculation in a nutrient agar culture medium, all according to relative ISO standards [20,21,22,23]. Measurements for total coliforms, E. coli, and culturable microorganisms were considered ‘compliant’ based on the Greek regulatory framework (Table 1) [15]. For Pseudomonas aeruginosa, a compliance limit of <1 CFU/100 mL was adopted, as recommended by the WHO [9]. Enterococci were selected as an alternative indicator of fecal contamination, given the demonstrated greater resistance of the enterococcus group to environmental stresses and water disinfectants compared to E. coli [24,25,26]. A limit of <1 CFU/100 mL was also adopted for enterococci, consistent with the criterion established for the primary fecal indicator, E. coli.
Field measurements were obtained using calibrated instruments to ensure accuracy. Temperature measurements were taken using a calibrated thermometer. Free and total chlorine, pH, alkalinity, and cyanuric acid levels were determined using a microprocessor-based portable photometer (Hanna Instruments, Woonsocket, RI, USA: HI97104 Portable Photometer, with a measurement range/accuracy of 6.5 to 8.5 pH/±0.1 pH at 25 °C, an alkalinity of 0 to 500 mg/L (as CaCO3)/±5 mg/L at 25 °C, a chlorine level of 0.00 to 5.00 mg/L (as Cl2)/±0.03 mg/L ±3% of reading, and a cyanuric acid level of 0 to 80 mg/L/±1 mg/L ±15% of reading at 25 °C).
In total, 360 residual chlorine, 300 total chlorine, 380 pH, 360 alkalinity, and 48 cyanuric acid measurements were performed. Comprehensive data were documented during the sampling process, which included details such as the date and time of sampling, descriptive information about the location of the facility, prevailing weather conditions, the exact sampling points, and the parameters slated for analysis.
A total of 72 on-site inspections were conducted across the swimming pools, including 32 inspections for outdoor athletic pools evenly distributed throughout the year, 20 for indoor pools, and 20 for baby swimming pools. These inspections were carried out during the operational phase to assess compliance with Greek legislation, as well as environmental health guidelines, particularly those established by the WHO and Pool Water Treatment Advisory Group (PWTAG) Code of Practice [9,15,27]. Assessments were performed to evaluate the structural integrity and hygienic state of changing rooms and toilets. Further insights were gathered on self-monitoring practices, risk assessment processes, and regulations governing swimmer behavior. Hazard identification was carried out using environmental health checklists aligned with international standards. This study reviewed all stages of pool design, development, and operation.
All statistical analyses were conducted using the free electronic version of the MedCalc Relative Risk Statistical Calculation Software (Version 23.1.7) [28] and IBM SPSS Statistics Version 24, Epi Info 2000 Version 7.2.5.0 (Centers for Disease Control and Prevention, Atlanta, GA, USA). The relative risk (RR) was calculated, along with a 95% confidence interval (CI). Categorical risk variables were analyzed in relation to water distribution systems. Statistical significance was defined as a p-value of less than 0.05. Pearson’s correlation coefficient (r) was applied to evaluate linear relationships.
Historically, risk assessment and management in swimming pools have primarily focused on epidemiological data and immediate health impacts [29,30,31]. Building on our measurement results, findings from 72 on-site inspections, and the relevant literature (a comprehensive literature search was conducted from June 2023 to December 2024, encompassing PubMed, Scopus, and Web of Science Core Collection), the first stage of risk assessment—hazard identification and risk evaluation—was conducted. This process involved identifying, analyzing, and assessing hazards; evaluating risk levels; and identifying the population at risk. Additionally, it entailed determining the likelihood and severity of potential negative outcomes. A hazard is defined as the combination of the probability of an adverse event occurring and the magnitude and severity of harm caused if the event takes place. Accordingly, potential health and safety hazards were identified by examining various factors, such as health-related issues, water treatment processes, ventilation systems, equipment performance, and human error. Both direct and indirect hazards were systematically included in a comprehensive hazard list. After compiling the initial list, each hazard underwent critical evaluation—drawing on literature and international experience—to assess its likelihood and severity. A detailed Risk Assessment Matrix table was developed to categorize identified risks based on their impact, likelihood, risk level, and control measures. Data from 72 on-site inspections were used to evaluate risks associated with open pools, indoor pools, and baby swimming pools. Each risk was rated based on likelihood, severity, and the resultant risk level, with proposed control measures provided for mitigation. The likelihood of risks, severity levels, and risk levels were categorized into distinct levels (Table 2, Table 3 and Table 4).
Table 2.
Categorization of risk likelihood levels: classification of risk likelihood based on observations from inspections or measurements. Each category represents the frequency with which a specific risk or hazard was identified during the inspection process. This structured approach helps assess the probability of a risk occurring, facilitating better risk management and prioritization.
Table 3.
Categorization of severity levels: classification of severity into three distinct levels based on the potential impact of a hazard. Each category defines the seriousness of the consequences if the hazard materializes. This classification helps prioritize risks and determine the appropriate level of response or mitigation measures required. This categorization ensures a structured evaluation of hazards, enabling informed decision-making and effective resource allocation to manage risks appropriately.
Table 4.
Categorization of risk levels: classification of the identified risks into different levels, based on their potential impact and likelihood of occurrence. Each risk level is associated with specific control measures to guide appropriate actions. The categories range from “Critical” to “Low”, helping to prioritize risks and determine the urgency of interventions required. This categorization ensures that resources and efforts are focused on addressing the highest risks first while maintaining ongoing management of lower-level hazards. This structured approach ensures that risks are managed in a way that reduces harm while optimizing resource allocation.
Corrective actions prompted by risk assessment findings were reviewed and communicated to pool managers to facilitate further improvements. The inspections utilized a structured checklist (Inspection/Safety Plan Checklist) to systematically record key information, including the classification of the swimming pool (e.g., public/private, indoor/outdoor/mixed), as well as associated facilities such as sports centers, gyms, and spas. Additional data collected included pool dimensions and volumes, types of disinfectants used, water recirculation systems, and treatment methods.
3. Results
3.1. Physicochemical Parameters
3.1.1. Residual Chlorine
According to current national legislation, free residual chlorine should be maintained between 0.4 and 0.7 mg/L. A total of 168 water samples were analyzed, revealing residual chlorine values with a maximum of 5.0 mg/L, a minimum of 0.00 mg/L, a mean of 1.64 mg/L, and a median of 2.34 mg/L. Of these 168 water samples, only 22 (13.09%) complied with the national legislation limits, while 122 (86.90%) exceeded these limits (Table 5 and Figure 1).
Table 5.
Distribution of residual chlorine levels in different pool types.
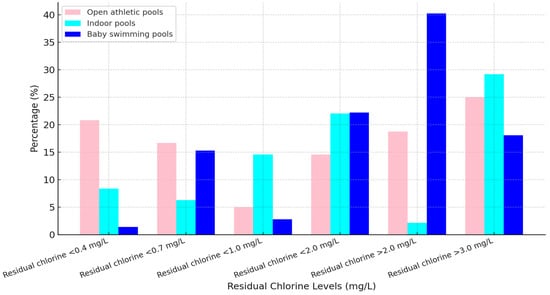
Figure 1.
Distribution of residual chlorine levels in different pool types. Graphical presentation of residual chlorine levels across different pool types, namely, open athletic pools (pink), indoor pools (cyan), and baby swimming pools (blue). Each bar represents a specific chlorine concentration category, with the highest concentrations (>2.0 mg/L and >3.0 mg/L) being most common in baby swimming pools.
3.1.2. pH Parameter Measurements
Maintaining the chemical quality of swimming pool water is crucial for ensuring user safety and effective disinfection. According to Greek legislation, pH levels should range between 7.2 and 8.2 (with an optimal range of 7.2–7.8). However, 78.5% of swimming pools failed to systematically monitor pH levels as required, with 48.5% of measurements falling outside the legal range of 7.2–8.2 and 42% outside the optimal range of 7.2–7.8. Additionally, 37.8% of measurements showed pH levels > 8, which severely impairs disinfection efficacy, while 10.7% of measurements indicated pH levels < 7, increasing the risks of microbial contamination and discomfort for swimmers. Regarding the impact of improper pH levels on the efficacy of chlorination, the relative risk (RR) was determined to be high (RR = 7.28; p = 0.02) (Figure 2).
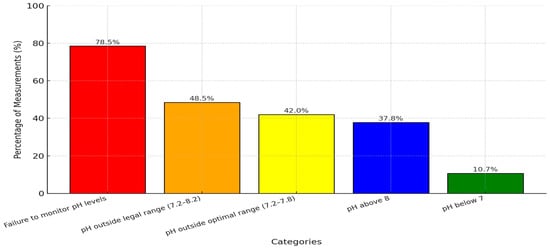
Figure 2.
pH monitoring and level distribution in swimming pools. Percentage distribution of pH level measurements in swimming pools, highlighting non-compliance with legal and optimal ranges.
3.1.3. Total Alkalinity and Cyanuric Acid
Total alkalinity and cyanuric acid are essential parameters for maintaining swimming pool water quality and ensuring users’ safety. According to Greek legislation requirements, total alkalinity should be at least 50 mg/L, ideally between 80 and 120 mg/L; there is no requirement for cyanuric acid; however, chemical suppliers recommend that the optimal range for cyanuric acid should be 30–50 mg/L. However, 98.5% of pools failed to measure alkalinity, and 45.8% of samples recorded levels below the recommended 80 mg/L, averaging just 42 mg/L. A total of 99.5% of pools did not monitor cyanuric acid, and 37.8% of samples exceeded the recommended threshold.
3.1.4. Compliance After Recommendations
Follow-up inspections, conducted after identifying and evaluating risks and notifying pool managers, revealed significant improvements in pool water management. Among open athletic pools, 45% achieved compliance by reducing chlorine concentrations to below 1 mg/L, while 58% of indoor pools similarly met the recommended limits. Notably, 85% of baby swimming pools, where over-chlorination poses the greatest risks, successfully reduced chlorine levels to safe ranges. Furthermore, systematic daily pH monitoring was implemented across all pools, with 60% also initiating regular assessments of alkalinity and cyanuric acid levels, contributing to enhanced water quality and safety (Figure 3).
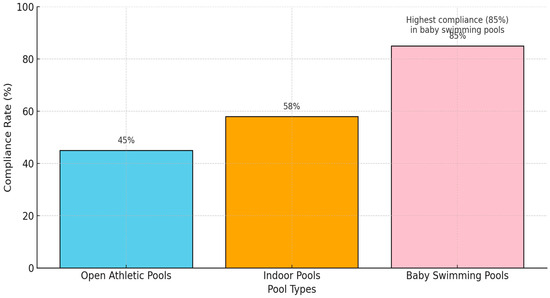
Figure 3.
Compliance rates after follow-up inspections. Compliance rates for each pool type, emphasizing the highest compliance observed in baby swimming pools (85%). The systematic daily pH monitoring was implemented across all pools and an additional 60% of pools, and alkalinity and cyanuric acid assessments were initiated.
3.2. Microbiological Parameters
Microbiological parameters were assessed using the following limits for comparison: E. coli, P. aeruginosa, and Enterococci (<1 CFU/100 mL); total microbial flora (<200 CFU/mL); and total coliforms (<15 CFU/100 mL).
P. aeruginosa: Out of 168 tested samples, 130 (77.68%) were within acceptable limits, while 38 samples (22.61%) exceeded the permissible levels. The distribution of non-compliant samples was as follows: 27.08% in outdoor athletic pools, 14.58% in indoor pools, and 25% in baby swimming pools (Figure 4 and Figure 5). These samples displayed a high mean value of 14.33 CFU/100 mL, with significant variation ranging from 1 to 65 CFU/100 mL. The relative risk (RR) for the presence of P. aeruginosa due to non-compliance with residual chlorine requirements was 3.50 (p = 0.0004). A statistically significant correlation (r = 0.04, p = 0.0001) was observed between ineffective chlorination (<0.4 mg/L) and the presence of P. aeruginosa (Figure 4).
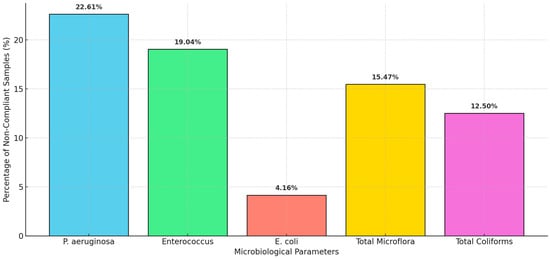
Figure 4.
Non-compliance rates for various microbiological parameters in swimming pool samples.
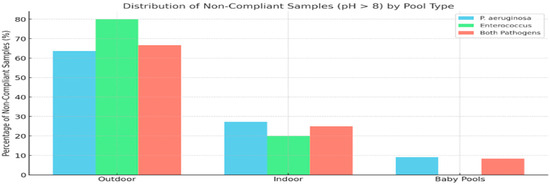
Figure 5.
Number of positive findings for Pseudomonas aeruginosa, Enterococci, and both pathogens among water samples with a pH greater than 8 across different pool types (outdoor, indoor, and baby pools).
Enterococci: Of the tested samples, 32 (19.04%) exceeded the limit of <1 CFU/100 mL, with the following distribution of ‘non-compliance’: 25% in outdoor athletic pools, 22.91% in indoor pools, and 12.50% in baby swimming pools (Figure 5 and Figure 6). The samples had a high mean concentration of 9.04 CFU/100 mL, with variations ranging from 1 to 40 CFU/100 mL (Figure 4).
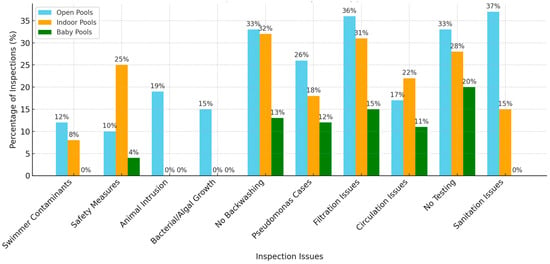
Figure 6.
Percentage of inspections identifying various issues across the following three pool types: Open Pools, Indoor Pools, and Baby Pools. Key issues include “No Backwashing”, “Filtration Issues”, and “No Testing”, which are particularly prominent in open and indoor pools. Baby pools show fewer problems overall, but some issues like “No Testing” and “Filtration Issues” remain significant. Each bar represents the percentage of inspections where the specific issue was observed, with color-coded bars distinguishing the pool types.
Among the positive samples for P. aeruginosa, 62.33% in outdoor athletic pools, 57.14% in indoor pools, and 55.55% in baby swimming pools showed no exceedances for other microbiological parameters based on Greek legislation. Similarly, of the Enterococci-positive samples, 58.33% in outdoor athletic pools, 36.36% in indoor pools, and 33.33% in baby swimming pools were within limits for E. coli, total microbial flora, and total coliforms.
Total Microbial Flora and Total Coliforms: Deviations from legal requirements were observed in 26 samples (15.47%) for total microbial flora (>200 CFU/mL) and in 21 samples (12.50%) for total coliforms (>15 CFU/100 mL) (Figure 4). These deviations displayed significant variability in concentrations. The lack of effective chlorination was associated with a high RR of 3.8 for total microbial flora and 6.28 for total coliforms across all pool types (Figure 4).
E. coli: Among the 168 samples tested, 7 (4.16%) exceeded permissible limits. Non-compliance with residual chlorine levels significantly increased the presence of E. coli, with an RR of 8.20 (p = 0.0002) (Figure 4).
In the samples with insufficient free residual chlorine concentrations (0.00–0.3 mg/L), P. aeruginosa was detected with concentrations ranging from 10 to 65 CFU/100 mL, along with Enterococci (25–40 CFU/100 mL), total microbial flora (>200 CFU/mL), and total coliforms (>15 CFU/100 mL). Notably, 40% of these samples also tested positive for E. coli.
For the 63 out of 168 samples (37.5%), where pH levels were >8, 44 samples (69.84%) revealed microbiological findings, including P. aeruginosa and Enterococci, without exceeding other microbiological parameters such as total microbial flora (<200 CFU/mL), total coliforms (>15 CFU/100 mL), and E. coli (<1 CFU/100 mL), as stipulated by Greek legislation. Among these 44 microbiologically non-compliant samples, 22 samples (50%) were positive for P. aeruginosa, with the distribution as follows: 14/22 (63.63%) in outdoor athletic pools, 6/22 (27.27%) in indoor pools, and 2/22 (9.09%) in baby pools (Figure 5). Ten samples (22.72%) tested positive for Enterococci, distributed as follows: 8/10 (80%) in outdoor athletic pools, 2/10 (20%) in indoor pools, and 0/10 (0%) in baby pools. Moreover, 12 samples (27.27%) were positive for both P. aeruginosa and Enterococci, distributed as follows: 8/12 (66.66%) in outdoor athletic pools, 3/12 (25%) in indoor pools, and 1/12 (8.33%) in baby pools.
3.3. On-Site Inspections
The analysis of data from 72 on-site inspections of swimming pools (32 outdoor athletic pools, 20 indoor pools, and 20 baby swimming pools) identified critical deficiencies across multiple operational and maintenance areas, posing significant risks to public health and safety. Inadequate sanitation practices and poor cleaning protocols were observed in 38/72 (open pools: 27/38, indoor pools: 11/38, and baby swimming pools: 0/38) inspections, with insufficient cleaning of pool surroundings such as decks and surfaces, which harbor bacteria, fungi, and viruses, while unattended organic debris exacerbated microbial contamination risks. Alarmingly, no regular microbial testing or daily physicochemical testing was conducted in 58/72 inspections (open pools 24/58, indoor pools 20/58, and baby swimming pools: 14/58), highlighting a serious lapse in water quality monitoring. Circulation issues, including stagnant water in “dead zones” fostering pathogen growth and uneven disinfectant distribution causing microbial blooms, were found in 33/72 (open pools: 12/38, indoor pools: 13/38, and baby swimming pools: 8/38) inspections, while filtration and circulation deficiencies were more widespread, noted in 59/72 (open pools: 26/59, indoor pools: 22/59, and baby swimming pools: 11/59) inspections, with delayed filter replacements, insufficient water circulation, and biofilm formation in pipes and filters harboring harmful microorganisms such as Pseudomonas species in 39/72 (open pools: 19/39, indoor pools: 11/39, and baby swimming pools: 9/39) cases. Furthermore, 56/72 (open pools: 24/56, indoor pools: 23/56, and baby swimming pools: 19/56) case inspections revealed the absence of regular backwashing or cleaning, leading to equipment failure and water quality degradation, while bacterial and algal proliferation, compromising water clarity and safety, was documented in 11/72 (open pools: 11/11, indoor pools: 0/11, and baby swimming pools: 0/11) case inspections. Animal and bird intrusion was another concern, noted in 14/72 (open pools: 14/14, indoor pools: 0/14, and baby swimming pools: 0/14) case inspections, with birds, rodents, insects, or pets accessing pool areas due to a lack of pool covers, perimeter fencing, or regular debris removal. Safety measures were inadequate in 28/72 (open pools: 7/28, indoor pools: 18/28, and baby swimming pools: 1/18) case inspections, with essential equipment like life buoys and rescue poles unavailable, while swimmer-related contaminants, including sweat, urine, feces, and skin pathogens, were reported in 18/72 (open pools: 12/18, indoor pools: 6/18, and baby swimming pools: 0/18) case inspections, reflecting insufficient enforcement of pre-swim showers, hygiene education, and water testing protocols (Figure 6).
3.4. Risk Assessment Matrix for Swimming Pool Safety
Table 6 provides a detailed evaluation of potential hazards, their impact, likelihood, and mitigation measures, categorizing identified risks for open pools, indoor pools, and baby swimming pools. In Table 6, each hazard is assessed in terms of likelihood, severity, and overall risk level and proposes targeted control measures to mitigate public health and safety concerns. The matrix includes specific categories of risks, such as microbial contamination, equipment failures, and swimmer-related issues, while outlining their likelihood of occurrence and severity of impact. Suggested mitigation measures address critical areas such as water quality testing, equipment maintenance, and hygiene protocols.
Table 6.
Comprehensive Risk Assessment Matrix for Swimming Pool Water Quality, building on measurement results. Detailed evaluation of potential hazards associated with swimming pool water quality, categorizing risks based on their level of impact, likelihood of occurrence, and proposed mitigation measures. Critical hazards such as microbial contamination, chemical imbalances, and improper disinfection are identified, emphasizing the population at risk and recommending actionable control strategies.
Based on the data from 72 on-site inspections, this risk assessment matrix evaluates each category of risks. Each risk is rated for likelihood, severity, and the resultant risk level. Control measures are provided for mitigation, and a matrix diagram visually represents the risk levels with color coding (Table 7 and Table 8 and Figure 7).
Table 7.
Risk Assessment Matrix for Swimming Pool Operations. Key risks associated with swimming pool operations, categorized by sanitation, water quality, filtration, safety, and swimmer hygiene. Each risk is evaluated based on likelihood, severity, and the resulting risk level. To mitigate these risks, specific control measures are recommended. This assessment emphasizes the importance of regular maintenance, monitoring, and compliance to ensure safe and hygienic swimming conditions.
Table 8.
Risk Assessment Matrix categorizing the identified risks for open pools, indoor pools, and baby swimming pools, along with their likelihood, severity, risk level, and control measures.
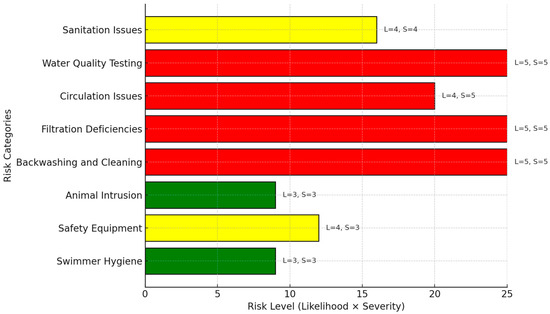
Figure 7.
Risk levels for swimming pool management. This horizontal bar chart illustrates the risk levels (calculated as Likelihood × Severity) for various categories in swimming pool management. The categories are color-coded to highlight their urgency: Red (critical risk: 20–25): Categories such as Inadequate Sanitation, Lack of Microbial Testing, Circulation Issues, and Filtration Deficiencies have the highest risk level (25). These require immediate corrective actions to prevent health hazards. Yellow (moderate risk: 10–19): Swimmer contaminants and safety equipment issues pose moderate risks with a level of 12, requiring regular monitoring and preventive measures. Green (low risk: 1–9): Animal Intrusion has a relatively low risk level (9) but still needs attention to prevent contamination. The numerical annotations on each bar provide precise risk levels, aiding stakeholders in prioritizing interventions for improving safety and water quality in swimming pools. (L: Likelihood, S: Severity).
4. Discussion
Ensuring the safety of swimming pools is a global priority, particularly in countries like Greece, where tourism forms a cornerstone of the economy. Effective risk assessment and management strategies are essential for safeguarding public health, enhancing the tourist experience, and maintaining the reputation of recreational water facilities. However, achieving and sustaining optimal safety standards presents significant challenges that require systematic evaluation and intervention.
4.1. Microbiological Hazards and Chemical Imbalances
Analysis of monitoring data highlights two critical threats to pool safety: microbial hazards due to underdisinfection and chemical risks stemming from over-chlorination. Chlorination remains the most widely employed method for microbial control in swimming pools. However, deviations in residual chlorine levels were observed, with only 13.09% of samples adhering to national standards (0.4–0.7 mg/L). Over 77% exceeded the upper limit, posing risks such as eye and skin irritation and exposure to disinfection by-products (DBPs). Conversely, 9% of samples demonstrated insufficient chlorine levels (<0.4 mg/L), increasing vulnerability to microbial hazards.
Deviations from recommended chlorine levels compromise water safety. Insufficient chlorine allows microbial contaminants to proliferate, while excessive chlorine concentrations can irritate swimmers and pose additional health risks.
During the COVID-19 pandemic, Greek legislation raised permissible residual chlorine thresholds for hotel swimming pools in accordance with WHO and CDC recommendations, aiming to mitigate microbiological threats [32]. Although this measure enhanced protection during the pandemic, it led to a post-pandemic trend where elevated chlorine levels were maintained as a precaution, often without addressing the risks associated with over-chlorination.
Equally important is the regulation of pH levels, which directly impacts chlorine efficacy and water quality. Studies have consistently shown that effective disinfection requires maintaining free chlorine levels within appropriate ranges, particularly when pH is controlled between 7.2 and 7.8. In this study, nearly 49% of pools exhibited pH values outside the legal range, with 37.8% exceeding 8.0, impairing chlorine’s disinfecting efficacy. Such conditions elevate the risk of bacterial proliferation, highlighting the critical role of risk assessment in maintaining optimal chemical balance. High pH levels (above 8) reduce chlorine’s bactericidal effectiveness, while low pH levels (<7) cause water to become corrosive, leading to infrastructure damage and swimmer discomfort. Insufficient monitoring of these parameters has resulted in heightened risks of microbial contamination and suboptimal disinfection.
Despite alkalinity’s importance and its inclusion in mandatory monitoring under Greek law, 98.5% of pools failed to measure alkalinity, and 45.8% of samples recorded levels below the recommended 80 mg/L, averaging just 42 mg/L. This neglect increases risks to both users and pool infrastructure. Similarly, cyanuric acid, used in outdoor pools to reduce chlorine loss from UV radiation, must be maintained between 30 and 50 mg/L, as excessive levels (>50 mg/L) reduce chlorine’s disinfection efficiency and increase water turbidity, compromising safety and visibility. A total of 99.5% of pools did not monitor cyanuric acid, and 37.8% of samples exceeded the recommended threshold, leading to reduced disinfection efficiency and potential water clarity issues.
4.2. Microbial Contamination and Public Health Risks
This study revealed alarming rates of microbial contamination; pathogens such as Pseudomonas aeruginosa (22%) and also fecal indicators Enterococcus spp. (19%) and E. coli (4.16%) were frequently detected in non-compliant samples. These findings underscore the necessity of regular microbial testing, as inadequate chlorine levels and elevated pH values create environments conducive to pathogen survival. Notably, baby swimming pools, which cater to highly vulnerable populations, exhibited disproportionately high rates of contamination. This highlights the need for stricter monitoring and risk mitigation measures in facilities frequented by children. Effective risk assessment frameworks can identify such high-risk areas and prioritize interventions.
Swimming pools and spas are frequently colonized by Pseudomonas aeruginosa, a Gram-negative pathogen associated with waterborne infections. Known for its ability to form biofilms and resist chemical disinfectants, P. aeruginosa poses significant challenges in treated water environments [30,33,34]. The detection of this pathogen often results in pool closures, increased maintenance costs, and diminished user confidence.
The global risk analysis of pool water is indispensable for devising targeted control strategies to prevent P. aeruginosa contamination. Key measures include routine microbiological testing to detect pathogens early, thorough cleaning protocols for surfaces and materials prone to microbial growth, mandatory pre-entry showering to minimize microbial introduction by users, and regulated pool occupancy levels to prevent overuse and maintain water quality.
4.3. Chemical Risks and Disinfection By-Products (DBPs).
Chemical disinfection, while essential, can create additional risks through the formation of disinfection by-products (DBPs). These are formed when chlorine reacts with natural organic matter (NOM) in water [35]. Studies have linked DBPs to carcinogenic and non-carcinogenic health effects, including bladder cancer [36]. Indoor environments exacerbate exposure risks through inhalation of volatile DBPs, highlighting the need for careful chemical management. Risk assessment plays a pivotal role in identifying and mitigating hazards associated with swimming pools. It enables systematic evaluations of potential risks, ensuring proactive measures are in place to protect users. The current study highlights the interplay between inadequate chemical management and microbial contamination, emphasizing the need for vigilant monitoring and control.
4.4. Operational Challenges and Compliance
This study also identified significant gaps in operational compliance, with 78.5% of pools failing to monitor pH systematically and 98.5% neglecting alkalinity checks. Such lapses compromise water quality and disinfection efficacy, emphasizing the need for targeted training and education for pool operators. Proper risk assessment ensures that these deficiencies are systematically addressed, reducing the likelihood of non-compliance.
4.5. Structured Risk Management Framework
From a risk assessment perspective, these findings underscore the necessity of robust monitoring systems and adherence to chemical and microbiological standards. A structured risk management framework should incorporate routine monitoring of chlorine, pH, total alkalinity, and cyanuric acid to ensure water quality; advanced monitoring technologies for real-time data collection and analysis; training programs to enhance the expertise of pool operators; and strict enforcement of legislative standards to ensure compliance.
Improper behaviors among swimming pool users are widespread, reflecting limited awareness of the importance of pool rules in mitigating health risks [37]. Greek swimming pool regulations mandate specific obligations for swimmers, including showering before pool entry, refraining from swimming when experiencing dermatological conditions or other infections, and adhering to established safety and hygiene protocols [15]. Despite regulations and preventive measures, swimming pool attendance remains a significant risk factor for molluscum contagiosum (MC) and warts, particularly among children. Studies indicate high incidence rates of these infections in Greek swimmers, with MC occurrence nearly quadrupling compared to earlier findings [38]. These infections are often linked to moist surfaces in pool environments, such as floors, or the shared use of items and equipment [6].
Facility operators hold primary responsibility for the safe operation and comprehensive maintenance of swimming facilities. Their duties include implementing rigorous cleaning and disinfection protocols, controlling the bathing load to prevent overcrowding, and ensuring compliance with hygiene standards. Such measures are essential for minimizing the transmission of contagious diseases, including viral and dermatological infections. The Greek swimming pool regulations also outline preventive measures, such as limiting swimmer capacity, continuous water disinfection, enhanced cleaning of sanitary installations, and regular maintenance of technical equipment like filters. Operators must ensure the proper operation of facilities to avoid issues such as poor water and air quality, overcrowding, and equipment malfunctions, which can contribute to viral, dermatological, and other infections. Swimmers, too, bear responsibilities to ensure the safe use of facilities. Mandatory actions include showering before entering the pool, wearing a swimming cap, and refraining from swimming if affected by infectious diseases. These practices, coupled with enhanced hygiene protocols, can significantly reduce the transmission of infections.
4.6. Implications for Public Health and Tourism
By addressing chemical imbalances and microbial hazards comprehensively, pool operators can minimize risks and enhance safety for all users, particularly vulnerable populations such as children. Such measures also strengthen public confidence in recreational water facilities, supporting the sustainability of tourism and protecting public health.
Safety in swimming pools is a critical concern due to its potential impacts on public health, societal well-being, and the environment. Addressing these challenges requires the consistent implementation of robust risk and safety management strategies. These strategies should emphasize proactive measures, continuous monitoring, and effective response mechanisms to create a low-risk environment that prioritizes user safety.
WHO underscores the importance of education in promoting safer behaviors among swimmers. Educating users about pool rules and the significance of compliance fosters a culture of safety and responsibility. Facility operators, swimming clubs, and public health organizations play a crucial role in this effort by disseminating clear, accessible information on safety signage and through educational campaigns [9]. In conclusion, creating a safe swimming environment requires a collaborative approach involving facility operators, regulatory authorities, and swimmers. By adhering to established guidelines and promoting education and awareness, the health risks associated with swimming pools can be minimized, ensuring a safer and more enjoyable experience for all users.
The integration of structured risk assessment methodologies, as advocated by the WHO and CDC, is essential for modern pool management. Key components are as follows:
Routine Monitoring: Frequent testing of chemical and microbial parameters to ensure compliance with safety standards.
Targeted Mitigation Strategies: Identifying high-risk scenarios, such as elevated pH or insufficient chlorine, and implementing corrective actions.
Stakeholder Education: Equipping pool operators with the knowledge and tools necessary to maintain water quality and protect public health.
This study’s findings highlight the importance of proactive safety measures, such as adjusting disinfection protocols, maintaining proper chemical balances, and enforcing hygiene rules for bathers. These efforts are particularly critical in enclosed aquatic facilities, where inadequate ventilation can exacerbate exposure to DBPs and other contaminants.
5. Conclusions
This study demonstrates the necessity of integrating risk assessment into swimming pool management to address the multifaceted challenges of pool safety. By systematically identifying and mitigating risks, stakeholders can ensure safer recreational environments for all users. The findings call for stricter regulatory frameworks, enhanced monitoring systems, and continuous operator training. Emphasizing risk-based approaches aligns with international best practices, fostering a culture of safety and compliance. Through diligent application of risk assessment methodologies, swimming pools can fulfill their dual roles as venues for recreation and public health promotion, ensuring both user safety and satisfaction. To effectively protect public health, Greece should prioritize the modernization of its legislative framework for the operation and maintenance of swimming pools, moving from an outdated legislation to a proactive, risk-based approach. This shift enables the identification and mitigation of emerging hazards like new pathogens and chemical contaminants, which traditional monitoring misses. By implementing contemporary risk models like the one suggested based on our study, Greece aims to improve public health, adapt to changing environmental conditions, and align with international standards, ensuring safer swimming environments for everyone.
This study serves as a valuable pilot demonstrating the feasibility and utility of our risk assessment approach; therefore, future research endeavors should prioritize expanding the pool selection to validate and enhance the generalizability of our findings. This broader approach will be crucial for confirming the initial trends observed and for providing a more comprehensive understanding of the risk factors under investigation.
Author Contributions
Conceptualization, A.M. (Athina Mplougoura), G.D.M. and A.M. (Athena Mavridou); methodology, A.M. (Athina Mplougoura) and K.K.; software, A.M. (Athina Mplougoura); validation, A.M. (Athina Mplougoura), G.D.M. and A.M. (Athena Mavridou); formal analysis, A.M. (Athina Mplougoura), G.D.M. and A.M. (Athena Mavridou); investigation, A.M. (Athina Mplougoura) and K.K.; resources, G.D.M.; data curation, A.M. (Athina Mplougoura) and G.D.M.; writing—original draft preparation, A.M. (Athina Mplougoura), G.D.M. and A.M. (Athena Mavridou); writing—review and editing, A.M. (Athina Mplougoura), G.D.M. and A.M. (Athena Mavridou); visualization, A.M. (Athina Mplougoura) and G.D.M.; supervision, G.D.M.; project administration, G.D.M.; funding acquisition, G.D.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Dataset available on request from the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Final Report Summary—POOLSAFE (A Novel Swimming Pool Water Treatment for the Detection and Elimination of Excess Cyanuric Acid). 2024. Available online: https://cordis.europa.eu/project/id/604884/reporting (accessed on 10 January 2025).
- Swimming Pool Construction Market Size, Share & Trends Analysis Report By Material (Concrete, Fiberglass, Steel Frame, Vinyl Liner), By Construction Type (Above-Ground, In-Ground), By End User (Residential, Commercial) and By Region(North America, Europe, APAC, Middle East and Africa, LATAM) Forecasts, 2024-2032. 2024. Available online: https://straitsresearch.com/report/swimming-pool-construction-market (accessed on 10 January 2025).
- Mavridou, A.; Pappa, O.; Papatzitze, O.; Mplougoura, A.; Drossos, P. An overview of pool and spa regulations in Mediterranean countries with a focus on the tourist industry. J. Water Health 2014, 12, 359–371. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidou, S.; Anestis, A.; Bartzoki, S.-F.; Lampropoulou, E.; Dardavesis, T.; Haidich, A.-B.; Tirodimos, I.; Tsimtsiou, Z. Microbiological water quality assessment of swimming pools and jacuzzis in Northern Greece: A retrospective study. Int. J. Environ. Health Res. 2024, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mavridou, A.; Pappa, O.; Papatzitze, O.; Dioli, C.; Kefala, A.M.; Drossos, P.; Beloukas, A. Exotic Tourist Destinations and Transmission of Infections by Swimming Pools and Hot Springs—A Literature Review. Int. J. Environ. Res. Public Health 2018, 15, 2730. [Google Scholar] [CrossRef] [PubMed]
- Sfyri, E.; Kefala, V.; Papageorgiou, E.; Mavridou, A.; Beloukas, A.; Rallis, E. Viral Cutaneous Infections in Swimmers: A Preliminary Study. Water 2021, 13, 3401. [Google Scholar] [CrossRef]
- Carter, R.A.A.; Joll, C.A. Occurrence and formation of disinfection by-products in the swimming pool environment: A critical review. J. Environ. Sci. 2017, 58, 19–50. [Google Scholar] [CrossRef] [PubMed]
- Johannesson, S.; Eriksson, K.; Wastensson, G.; Westerlund, J.; Graff, P. Airborne trichloramine in indoor swimming pools in Sweden. J. Occup. Environ. Hyg. 2024, 21, 805–816. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for Safe Recreational-Water Environments Final Draft for Consultation Vol. 2: Swimming Pools, Spas and Similar Recreational-Water Environments. 2006. Available online: https://apps.who.int/iris/handle/10665/43336 (accessed on 10 January 2025).
- Brecher, R.W. Risk Assessment. Toxicol. Pathol. 1997, 25, 23–26. [Google Scholar] [CrossRef] [PubMed]
- ISO 31000: 2018; Risk Management-Guidelines. ISO: London, UK, 2018.
- Hesami Arani, M.; Jaafarzadeh, N.; Dehabadi, P.; Mostafaii, G.; Tazik, M.; Karimi, Z.; Etesam, A.; Mohammadzadeh, M. Health and safety hazards identification and risk assessment in the swimming pools using combined HAZID and ALARP. Environ. Health Eng. Manag. 2020, 7, 151–160. [Google Scholar] [CrossRef]
- Berg, A.; Fang, T.-A.; Tang, H. Variability of residual chlorine in swimming pool water and determination of chlorine consumption for maintaining hygienic safety of bathers with a simple mass balance model. J. Water Health 2018, 17, 227–236. [Google Scholar] [CrossRef]
- Norlin, J.I. Public health investigation of swimming pool chlorine gas disinfection systems. Environ. Health Rev. 2019, 62, 53–58. [Google Scholar] [CrossRef]
- Sanitary Order Γ1/443/1973—Government Gazette B-87/24-1-1973, About Swimming Pools Following Instructions for Their Construction and Operation. 1973. Available online: https://www.elinyae.gr/ethniki-nomothesia/ya-g14431973-fek-87b-2411973 (accessed on 10 January 2025).
- EN 15288-1; Swimming Pools—Part 1: Safety Requirements for Design. CEN—European Committee for Standardization: Brussels, Belgium, 2018.
- EN 15288-2; Swimming Pools—Part 2: Safety Requirements for Operation. CEN—European Committee for Standardization: Brussels, Belgium, 2018.
- Bartram, J.; Fewtrell, L.; Stenström, T. Harmonised Assessment of Risk and Risk Management for Water-related Infectious Disease: An overview. In Water Quality: Guidelines, Standards and Health; WHO: Geneva, Switzerland, 2001; pp. 1–16. [Google Scholar]
- ISO 19458:2006; Water Quality—Sampling for Microbiological Analysis. ISO: London, UK, 2006.
- ISO 9308-1:2014; Water Quality—Enumeration of Escherichia Coli and Coliform Bacteria Part 1: Membrane Filtration Method for Waters with Low Bacterial Background Flora. ISO: London, UK, 2014.
- ISO 16266:2006; Water Quality—Detection and Enumeration of Pseudomonas Aeruginosa—Method by Membrane Filtration. ISO: London, UK, 2006.
- ISO/DIS 7899-3; Water Quality—Enumeration of Intestinal Enterococci—Part 3: Most Probable Number Method. ISO: London, UK, 2023.
- ISO 6222:1999; Water Quality—Enumeration of Culturable Micro-Organisms—Colony Count by Inoculation in a Nutrient Agar Culture Medium. ISO: London, UK, 1999.
- Guidelines on Recreational Water Quality: Volume 1 Coastal and Fresh Waters. 2021. Available online: https://iris.who.int/bitstream/handle/10665/342625/9789240031302-eng.pdf?sequence=1 (accessed on 10 January 2025).
- Canadian Recreational Water Quality Guidelines—Indicators of Fecal Contamination: E. coli and Enterococci in Recreational Waters. 2023. Available online: https://www.canada.ca/en/health-canada/services/publications/healthy-living/recreational-water-quality-guidelines-indicators-fecal-contamination/e-coli-enterococci.html (accessed on 10 January 2025).
- Guidance on the Use of Enterococci as an Indicator in Canadian Drinking Water Supplies. 2020. Available online: https://www.canada.ca/en/health-canada/services/publications/healthy-living/guidance-use-enterococci-indicator-canadian-drinking-water-supplies.html (accessed on 10 January 2025).
- Pool Water Treatment Advisory Group (PWTAG) Code of Practice: The Management and Treatment of Swimming Pool Water. 2024. Available online: http://www.pwtag.org/code-of-practice/ (accessed on 10 January 2025).
- MedCalc. MedCalc's Relative Risk Calculator; MedCalc Software Ltd.: Ostend, Belgium, 2023. [Google Scholar]
- Barwick, R.S.; Levy, D.A.; Craun, G.F.; Beach, M.J.; Calderon, R.L. Surveillance for waterborne-disease outbreaks--United States, 1997–1998. MMWR. CDC Surveill. Summ. 2000, 49, 1–21. [Google Scholar] [PubMed]
- Craun, G.F.; Calderon, R.L.; Craun, M.F. Outbreaks associated with recreational water in the United States. Int. J. Environ. Health Res. 2005, 15, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Craun, G.F.; Calderon, R.L.; Wade, T.J. Assessing waterborne risks: An introduction. J Water Health 2006, 4 (Suppl. 2), 3–18. [Google Scholar] [CrossRef] [PubMed]
- Mellou, K.; Mplougoura, A.; Mandilara, G.; Papadakis, A.; Chochlakis, D.; Psaroulaki, A.; Mavridou, A. Swimming Pool Regulations in the COVID-19 Era: Assessing Acceptability and Compliance in Greek Hotels in Two Consecutive Summer Touristic Periods. Water 2022, 14, 796. [Google Scholar] [CrossRef]
- Guida, M.; Di Onofrio, V.; Gallè, F.; Gesuele, R.; Valeriani, F.; Liguori, R.; Romano Spica, V.; Liguori, G. Pseudomonas aeruginosa in Swimming Pool Water: Evidences and Perspectives for a New Control Strategy. Int. J. Environ. Res. Public Health 2016, 13, 90919. [Google Scholar] [CrossRef] [PubMed]
- Rice, S.A.; van den Akker, B.; Pomati, F.; Roser, D. A risk assessment of Pseudomonas aeruginosa in swimming pools: A review. J. Water Health 2012, 10, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.J.; Conrad, D.; Kothawala, D.N.; Baulch, H.M. Selective removal of dissolved organic matter affects the production and speciation of disinfection byproducts. Sci. Total Environ. 2019, 652, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Diana, M.; Felipe-Sotelo, M.; Bond, T. Disinfection byproducts potentially responsible for the association between chlorinated drinking water and bladder cancer: A review. Water Res. 2019, 162, 492–504. [Google Scholar] [CrossRef] [PubMed]
- Pasquarella, C.; Veronesi, L.; Napoli, C.; Castaldi, S.; Pasquarella, M.; Saccani, E.; Colucci, M.; Auxilia, F.; Gallè, F.; Di Onofrio, V.; et al. What about behaviours in swimming pools? Results of an Italian multicentre study. Microchem. J. 2014, 112, 190–195. [Google Scholar] [CrossRef]
- Kyriakis, K.P.; Palamaras, I.; Terzoudi, S.; Emmanuelides, S.; Michailides, C. Case detection rates of molluscum contagiosum in childhood. Pediatr. Dermatol. 2007, 24, 198–199. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).