
Workup and Clinical Assessment for Allergen Immunotherapy Candidates

 ,
,  ,
, 
Abstract
:1. Introduction
2. Tests Confirming IgE-Mediated Allergy and Monitoring the Severity of the Allergic Reaction
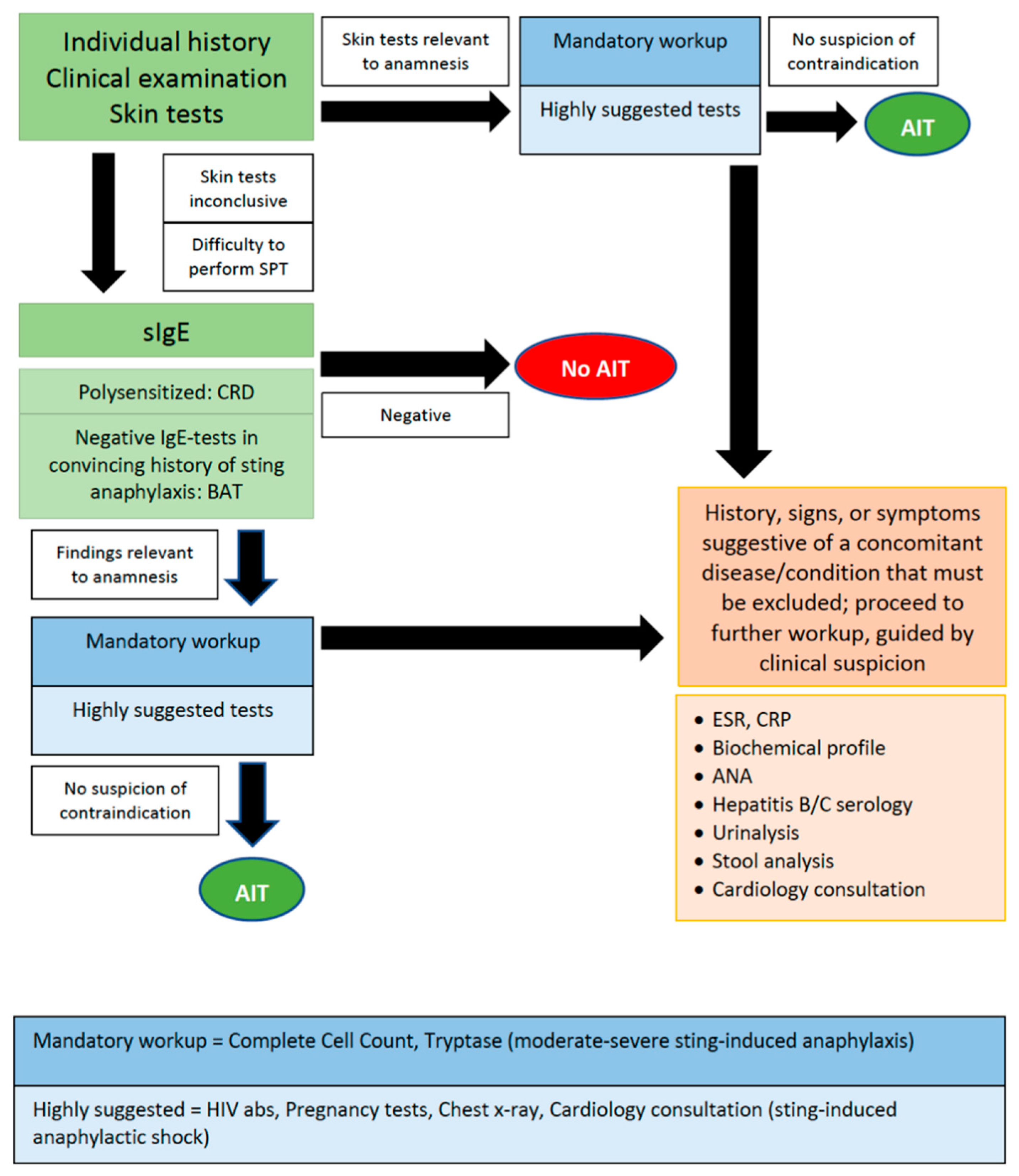
2.1. Skin Tests
2.2. Serum-IgE Tests
2.3. Component-Resolved Diagnostics (CRD)
2.4. Tryptase
2.5. Basophil-Activation Test
2.6. Complete Blood Count (CBC)
3. Cardiovascular Checkup
4. Neoplasias
- Unexplained paleness and loss of energy
- Unusual lump, mass, or swelling
- Sudden unexplained weight loss
- Unexplained persisting fever or illness
- Easy bruising or bleeding
- Prolonged or ongoing pain in one or more areas of the body
- Limping
- Frequent headaches, particularly in the morning and associated with vomiting
- Sudden eye or vision changes
- Unexplained changes in bowel and urination habits
- Obvious changes in existing skin lesions
- Persistent cough or hoarseness
- Observation for general health appearance, central and peripheral skin color, nutritional status, respiratory rate and effort, sweating, venous distention, and edema
- Examination of the chest wall
- Examination of the breasts, including assessment of pubertal stage in females and assessment for gynecomastia in males.
- Examination of the lungs
- Examination of the heart including palpation and auscultation
- Examination of the abdomen
- Examination of nose, mouth and neck
5. Autoimmune Rheumatic Diseases
6. HIV Infection
7. Pregnancy
8. Chronic Diseases
9. Asthma
10. Conclusions and Unmet Needs
Author Contributions
Funding
Conflicts of Interest
References
- Dhami, S.; Kakourou, A.; Asamoah, F.; Agache, I.; Lau, S.; Jutel, M.; Muraro, A.; Roberts, G.; Akdis, C.A.; Bonini, M.; et al. Allergen immunotherapy for allergic asthma: A systematic review and meta-analysis. Allergy 2017, 72, 1825–1848. [Google Scholar] [CrossRef]
- Bousquet, J.; van Cauwenberge, P.; Khaltaev, N. Allergic Rhinitis and Its Impact on Asthma. J. Allergy Clin. Immunol. 2001, 108, S147–S334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nurmatov, U.; Dhami, S.; Arasi, S.; Roberts, G.; Pfaar, O.; Muraro, A.; Ansotegui, I.J.; Calderon, M.; Cingi, C.; Durham, S.; et al. Allergen immunotherapy for allergic rhinoconjunctivitis: A systematic overview of systematic reviews. Clin. Transl. Allergy 2017, 7, 1–16. [Google Scholar] [CrossRef]
- Dhami, S.; Zaman, H.; Varga, E.-M.; Sturm, G.J.; Muraro, A.; Akdis, C.A.; Antolín-Amérigo, D.; Bilò, M.B.; Bokanovic, D.; Calderon, M.A.; et al. Allergen immunotherapy for insect venom allergy: A systematic review and meta-analysis. Allergy Eur. J. Allergy Clin. Immunol. 2017, 72, 342–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, G.; Pfaar, O.; Akdis, C.A.; Ansotegui, I.J.; Durham, S.R.; Van Wijk, R.G.; Halken, S.; Linnemann, D.L.; Pawankar, R.; Pitsios, C.; et al. EAACI Guidelines on Allergen Immunotherapy: Allergic rhinoconjunctivitis. Allergy 2017, 73, 765–798. [Google Scholar] [CrossRef] [Green Version]
- Cox, L.; Nelson, H.; Lockey, R.; Calabria, C.; Chacko, T.; Finegold, I.; Nelson, M.; Weber, R.; Bernstein, D.I.; Blessing-Moore, J.; et al. Allergen immunotherapy: A practice parameter third update. J. Allergy Clin. Immunol. 2011, 127, S1–S55. [Google Scholar] [CrossRef]
- Sturm, G.J.; Varga, E.-M.; Roberts, G.; Mosbech, H.; Bilò, M.B.; Akdis, C.A.; Antolín-Amérigo, D.; Cichocka-Jarosz, E.; Gawlik, R.; Jakob, T.; et al. EAACI guidelines on allergen immunotherapy: Hymenoptera venom allergy. Allergy 2017, 73, 744–764. [Google Scholar] [CrossRef] [Green Version]
- Alvaro-Lozano, M.; Akdis, C.A.; Akdis, M.; Alviani, C.; Angier, E.; Arasi, S.; Arzt-Gradwohl, L.; Barber, D.; Bazire, R.; Cavkaytar, O.; et al. Allergen Immunotherapy in Children User’s Guide. Pediatr. Allergy Immunol. 2020, 31, 1–101. [Google Scholar] [CrossRef]
- Calderón, M.A.; Vidal, C.; del Río, P.R.; Just, J.; Pfaar, O.; Tabar, A.I.; Sánchez-Machín, I.; Bubel, P.; Borja, J.; Eberle, P.; et al. European Survey on Adverse Systemic Reactions in Allergen Immunotherapy (EASSI): A real-life clinical assessment. Allergy 2016, 72, 462–472. [Google Scholar] [CrossRef]
- Pitsios, C.; Tsoumani, M.; Bilò, M.B.; Sturm, G.J.; del Rio, P.R.; Gawlik, R.; Ruëff, F.; Paraskevopoulos, G.; Valovirta, E.; Pfaar, O.; et al. Contraindications to immunotherapy: A global approach. Clin. Transl. Allergy 2019, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Del Rio, P.R.; Pitsios, C.; Tsoumani, M.; Pfaar, O.; Paraskevopoulos, G.; Gawlik, R.; Valovirta, E.; Larenas-Linnemann, D.; Demoly, P.; Calderón, M.A. Physicians’ experience and opinion on contraindications to allergen immunotherapy: The CONSIT survey. Ann. Allergy Asthma Immunol. 2017, 118, 621–628.e1. [Google Scholar] [CrossRef] [PubMed]
- Heinzerling, L.; Mari, A.; Bergmann, K.C.; Bresciani, M.; Burbach, G.; Darsow, U.; Durham, S.; Fokkens, W.; Gjomarkaj, M.; Haahtela, T.; et al. The skin prick test—European standards. Clin. Transl. Allergy 2013, 3, 3. [Google Scholar] [CrossRef] [Green Version]
- Jakob, T.; Rafei-Shamsabadi, D.; Spillner, E.; Müller, S. Diagnostics in Hymenoptera venom allergy: Current concepts and developments with special focus on molecular allergy diagnostics. Allergo J. Int. 2017, 26, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Oppenheimer, J.; Durham, S.; Nelson, H.; Wolthers, O.D. World Allergy Organization Website. Allergy Diagnostic Testing. Available online: https://www.worldallergy.org/education-and-programs/education/allergic-disease-resource-center/professionals/allergy-diagnostic-testing (accessed on 1 December 2021).
- Ansotegui, I.J.; Melioli, G.; Canonica, G.W.; Caraballo, L.; Villa, E.; Ebisawa, M.; Passalacqua, G.; Savi, E.; Ebo, D.; Gómez, R.M.; et al. IgE allergy diagnostics and other relevant tests in allergy, a World Allergy Organization position paper. World Allergy Organ. J. 2020, 13, 100080, Erratum in 2021, 14, 100557. [Google Scholar] [CrossRef] [PubMed]
- Pitsios, C. Allergen Immunotherapy: Biomarkers and Clinical Outcome Measures. J. Asthma Allergy 2021, 14, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Matricardi, P.M.; Kleine-Tebbe, J.; Hoffmann, H.J.; Valenta, R.; Hilger, C.; Hofmaier, S.; Aalberse, R.C.; Agache, I.; Asero, R.; Ballmer-Weber, B.; et al. EAACI Molecular Allergology User’s Guide. Pediatr. Allergy Immunol. 2016, 27 (Suppl. 2), 1–250. [Google Scholar] [CrossRef]
- Matricardi, P.M.; Dramburg, S.; Potapova, E.; Skevaki, C.; Renz, H. Molecular diagnosis for allergen immunotherapy. J. Allergy Clin. Immunol. 2019, 143, 831–843. [Google Scholar] [CrossRef]
- Bonadonna, P.; Bonifacio, M.; Lombardo, C.; Zanotti, R. Hymenoptera Allergy and Mast Cell Activation Syndromes. Curr. Allergy Asthma Rep. 2015, 16, 5. [Google Scholar] [CrossRef]
- Van Anrooij, B.; van der Veer, E.; de Monchy, J.G.R.; van der Heide, S.; Kluin-Nelemans, J.C.; Van Voorst Vader, P.C.; van Doormaal, J.J.; Oude Elberink, J.N.G. Higher mast cell load decreases the risk of Hymenoptera venom–induced anaphylaxis in patients with mastocytosis. J. Allergy Clin. Immunol. 2013, 132, 125–130. [Google Scholar] [CrossRef]
- Valent, P.; Horny, H.P.; Li, C.Y.; Longley, J.B.; Metcalfe, D.D.; Parwaresch, R.M.; Bennett, J.M. Mastocytosis (Mast Cell Disease), 4th ed.; Swerdlow, S.H., Campo, E., Harris, N.L., Jaffe, E.S., Pileri, S.A., Stein, H., Thiele, J., Vardiman, J.W., Eds.; World Health Organization (WHO) Classification of Tumours; Pathology & Genetics; Tumours of Haematopoietic and Lymphoid Tissues; IARC Press: Lyon, France, 2008; pp. 54–63. [Google Scholar]
- Korosec, P.; Erzen, R.; Silar, M.; Bajrovic, N.; Kopac, P.; Kosnik, M. Basophil responsiveness in patients with insect sting allergies and negative venom-specific immunoglobulin E and skin prick test results. Clin. Exp. Allergy 2009, 39, 1730–1737. [Google Scholar] [CrossRef]
- Bonadonna, P.; Zanotti, R.; Melioli, G.; Antonini, F.; Romano, I.; Lenzi, L.; Caruso, B.; Passalacqua, G. The role of basophil activation test in special populations with mastocytosis and reactions to hymenoptera sting. Allergy 2012, 67, 962–965. [Google Scholar] [CrossRef] [PubMed]
- George-Gay, B.; Parker, K. Understanding the complete blood count with differential. J. PeriAnesth. Nurs. 2003, 18, 96–117. [Google Scholar] [CrossRef] [PubMed]
- Roufosse, F.; Weller, P.F. Practical approach to the patient with hypereosinophilia. J. Allergy Clin. Immunol. 2010, 126, 39–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, K.W.; Milner, J.D.; Freeman, A.F. Eosinophilia Associated with Disorders of Immune Deficiency or Immune Dysregulation. Immunol. Allergy Clin. N. Am. 2015, 35, 523–544. [Google Scholar] [CrossRef] [Green Version]
- Pitsios, C.; Demoly, P.; Bilò, M.B.; Van Wijk, R.G.; Pfaar, O.; Sturm, G.J.; del Rio, P.R.; Tsoumani, M.; Gawlik, R.; Paraskevopoulos, G.; et al. Clinical contraindications to allergen immunotherapy: An EAACI position paper. Allergy 2015, 70, 897–909. [Google Scholar] [CrossRef]
- Greenberger, P.A.; Rotskoff, B.D.; Lifschultz, B. Fatal anaphylaxis: Postmortem findings and associated comorbid diseases. Ann. Allergy Asthma Immunol. 2007, 98, 252–257. [Google Scholar] [CrossRef]
- Wagdi, P.; Mehan, V.K.; Bürgi, H.; Salzmann, C. Acute myocardial infarction after wasp stings in a patient with normal coronary arteries. Am. Heart J. 1994, 128, 820–823. [Google Scholar] [CrossRef]
- Golden, D.B. What is anaphylaxis? Curr. Opin. Allergy Clin. Immunol. 2007, 7, 331–336. [Google Scholar] [CrossRef]
- Marone, G.; Bova, M.; Detoraki, A.; Onorati, A.M.; Rossi, F.W.; Spadaro, G. The Human Heart As a Shock Organ in Anaphylaxis. Allergo J. Int. 2004, 257, 133–156. [Google Scholar] [CrossRef] [Green Version]
- Simons, F.E.R.; Ardusso, L.R.; Bilò, M.B.; El-Gamal, Y.M.; Ledford, D.K.; Ring, J.; Sanchez-Borges, M.; Senna, G.E.; Sheikh, A.; Thong, B.Y.; et al. World Allergy Organization Guidelines for the Assessment and Management of Anaphylaxis. World Allergy Organ. J. 2011, 4, 13–37. [Google Scholar] [CrossRef] [Green Version]
- Westfall, T.C.; Westfall, D.P. Adrenergic agonists and antagonists. In Goodman & Gilman’s: The Pharmacological Basis of Therapeutics, 12th ed.; Brunton, L.L., Chabner, B.A., Knollmann, B.C., Eds.; McGraw-Hill Companies: New York, NY, USA, 2011; pp. 277–334. Available online: https://accessmedicine.mhmedical.com/content.aspx?bookid=1613§ionid=102158209 (accessed on 18 December 2021).
- Vadas, P.; Perelman, B. Effect of epinephrine on platelet-activating factor–stimulated human vascular smooth muscle cells. J. Allergy Clin. Immunol. 2012, 129, 1329–1333. [Google Scholar] [CrossRef] [PubMed]
- Caviglia, A.G.; Passalacqua, G.; Senna, G. Risk of severe anaphylaxis for patients with Hymenoptera venom allergy: Are angiotensin-receptor blockers comparable to angiotensin-converting enzyme inhibitors? J. Allergy Clin. Immunol. 2010, 125, 1171. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Hess, E.P.; Nestler, D.M.; Athmaram, V.R.B.; Bellolio, F.; Decker, W.W.; Li, J.T.; Hagan, J.B.; Manivannan, V.; Vukov, S.C.; et al. Antihypertensive medication use is associated with increased organ system involvement and hospitalization in emergency department patients with anaphylaxis. J. Allergy Clin. Immunol. 2013, 131, 1103–1108. [Google Scholar] [CrossRef]
- Ruëff, F.; Przybilla, B.; Biló, M.B.; Müller, U.; Scheipl, F.; Aberer, W.; Birnbaum, J.; Bodzenta-Lukaszyk, A.; Bonifazi, F.; Bucher, C.; et al. Predictors of side effects during the buildup phase of venom immunotherapy for Hymenoptera venom allergy: The importance of baseline serum tryptase. J. Allergy Clin. Immunol. 2010, 126, 105–111.e5. [Google Scholar] [CrossRef] [PubMed]
- Ruëff, F.; Przybilla, B.; Biló, M.B.; Müller, U.; Scheipl, F.; Aberer, W.; Birnbaum, J.; Lukaszyk, A.B.; Bonifazi, F.; Bucher, C.; et al. Predictors of severe systemic anaphylactic reactions in patients with Hymenoptera venom allergy: Importance of baseline serum tryptase—a study of the European Academy of Allergology and Clinical Immunology Interest Group on Insect Venom Hypersensitivity. J. Allergy Clin. Immunol. 2009, 124, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Linneberg, A.; Jacobsen, R.K.; Jespersen, L.; Abildstrøm, S.Z. Association of subcutaneous allergen-specific immunotherapy with incidence of autoimmune disease, ischemic heart disease, and mortality. J. Allergy Clin. Immunol. 2011, 129, 413–419. [Google Scholar] [CrossRef]
- El-Qutob, D.; Letrán, A.; Matheu, V.; Fernandez-Caldas, E. Cancer: Still a contraindication for allergen immunotherapy? World Allergy Organ. J. 2021, 14, 100597. [Google Scholar] [CrossRef]
- World Health Organization International Agency for Research on Cancer. Cancer Today. Available online: http://gco.iarc.fr/today/data/factsheets/populations/900-worldfact-sheets.pdf (accessed on 18 December 2021).
- Crosswell, J.M.; Brawley, O.W.; Kramer, B.S. Prevention and early detection of cancer. In Harrison’s Principles of Internal Medicine, 20th ed.; Jameson, J.L., Kasper, D.L., Longo, D.L., Fauci, A.S., Hauser, S.L., Loscalzo, J.L., Eds.; McGraw Hill: New York, NY, USA, 2018; Available online: https://accessmedicine.mhmedical.com/content.aspx?bookid=2129§ionid=192014692 (accessed on 19 December 2018).
- Chan, R.; Nekhlyudov, L. Overview of Cancer Survivorship Care for Primary Care and Oncology Providers; Shah, S., Ed.; UptoDate: Waltham, MA, USA, 2021. [Google Scholar]
- Ziogas, A.; Horick, N.K.; Kinney, A.; Lowery, J.T.; Domchek, S.M.; Isaacs, C.; Griffin, C.A.; Moorman, P.G.; Edwards, K.L.; Hill, D.A.; et al. Clinically Relevant Changes in Family History of Cancer Over Time. JAMA 2011, 306, 172–178. [Google Scholar] [CrossRef] [Green Version]
- Steuber, P.C. Overview of Common Presenting Signs and Symptoms of Childhood Cancer; Pappo, A.S., Armsby, C., Eds.; UptoDate: Waltham, MA, USA, 2021. [Google Scholar]
- Kelly, N.R. Screening Tests in Children and Adolescents; Drutz, J.E., Torchia, M.M., Eds.; UptoDate: Waltham, MA, USA, 2021. [Google Scholar]
- Krishna, M.T.; Subramanian, A.; Adderley, N.; Zemedikun, D.T.; Gkoutos, G.V.; Nirantharakumar, K. Allergic diseases and long-term risk of autoimmune disorders: Longitudinal cohort study and cluster analysis. Eur. Respir. J. 2019, 54, 1900476. [Google Scholar] [CrossRef]
- Lu, Z.; Zeng, N.; Cheng, Y.; Chen, Y.; Li, Y.; Lu, Q.; Xia, Q.; Luo, D. Atopic dermatitis and risk of autoimmune diseases: A systematic review and meta-analysis. Allergy, Asthma Clin. Immunol. 2021, 17, 1–9. [Google Scholar] [CrossRef]
- Rudwaleit, M.; Andermann, B.; Alten, R.; Sörensen, H.; Listing, J.; Zink, A.; Sieper, J.; Braun, J. Atopic disorders in ankylosing spondylitis and rheumatoid arthritis. Ann. Rheum. Dis. 2002, 61, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Karatay, S.; Yildirim, K.; Ugur, M.; Senel, K.; Erdal, A.; Durmus, B.; Baysal, O.; Altay, Z.; Sarac, A.J.; Gur, A.; et al. Prevalence of atopic disorders in rheumatic diseases. Mod. Rheumatol. 2012, 23, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Solomon, D.H.; Kavanaugh, A.J.; Schur, P.H. American College of Rheumatology Ad Hoc Committee on Immunologic Testing Guidelines Evidence-based guidelines for the use of immunologic tests: Antinuclear antibody testing. Arthritis Care Res. 2002, 47, 434–444. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.M.; Feltkamp, T.E.W.; Smolen, J.S.; Butcher, B.; Dawkins, R.; Fritzler, M.J.; Gordon, T.; Hardin, J.A.; Kalden, J.R.; Lahita, R.G.; et al. Range of antinuclear antibodies in “healthy” individuals. Arthritis Care Res. 1997, 40, 1601–1611. [Google Scholar] [CrossRef]
- Kurbacheva, O.M.; Pavlova, K.S.; A Galitzkaya, M. Allergen-specific immunotherapy. Analytic review of current international and Russian federal position papers. Russ. J. Allergy 2017, 14, 24–32. [Google Scholar] [CrossRef]
- Larenas-Linnemann, D.E.; Hauswirth, D.W.; Calabria, C.W.; Sher, L.D.; Rank, M.A. American Academy of Allergy, Asthma & Immunology membership experience with allergen immunotherapy safety in patients with specific medical conditions. Allergy Asthma Proc. 2016, 37, 112–122. [Google Scholar] [CrossRef]
- Calabria, C.W.; Hauswirth, D.W.; Rank, M.; Sher, L.; Larenas-Linnemann, D. American Academy of Asthma, Allergy & Immunology membership experience with venom immunotherapy in chronic medical conditions and pregnancy, and in young children. Allergy Asthma Proc. 2017, 38, 121–129. [Google Scholar] [CrossRef]
- 1993 Revised Classification System for HIV Infection and Expanded Surveillance Case Definition for AIDS Among Adolescents and Adults. JAMA 1993, 269, 729–730. [CrossRef]
- Johnson, S.C. Antiretroviral Therapy for HIV Infection: When to Initiate Therapy, Which Regimen to Use, and How to Monitor Patients on Therapy. Top. Antivir. Med. 2016, 23, 161–167. [Google Scholar]
- Cox, L.; Li, J.T.; Nelson, H.; Lockey, R. Allergen immunotherapy: A practice parameter second update. J. Allergy Clin. Immunol. 2007, 120, S25–S85. [Google Scholar] [CrossRef]
- Marcoval, J.; Moreno, A.; Mañá, J. Subcutaneous sarcoidosis localised to sites of previous desensitizing injections. Clin. Exp. Dermatol. 2007, 33, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.; Durham, S.R.; Till, S.; Roberts, G.; Corrigan, C.; Leech, S.C.; Krishna, M.T.; Rajakulasingham, R.K.; Williams, A.; Chantrell, J.; et al. Immunotherapy for allergic rhinitis. Clin. Exp. Allergy 2011, 41, 1177–1200. [Google Scholar] [CrossRef] [PubMed]
- Miehlke, S.; Alpan, O.; Schröder, S.; Straumann, A. Induction of Eosinophilic Esophagitis by Sublingual Pollen Immunotherapy. Case Rep. Gastroenterol. 2013, 7, 363–368. [Google Scholar] [CrossRef]
- Iragorri, N.; Spackman, E. Assessing the value of screening tools: Reviewing the challenges and opportunities of cost-effectiveness analysis. Public Heal. Rev. 2018, 39, 17. [Google Scholar] [CrossRef] [Green Version]
- Lin, E.C. Radiation Risk From Medical Imaging. Mayo Clin. Proc. 2010, 85, 1142–1146. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Cancer | Action | |
|---|---|---|
| Breast cancer | Concerning family history | Refer for genetic counseling/testing |
| Hereditary breast and ovarian syndrome | Screen per recommendations | |
| Women > 40 | Individual decision; if screening desired, screen with mammography every two years | |
| Cervical cancer | Women 21 to 29 years | Pap smear every three years |
| Women ≥ 30 years | Pap smear every three years, or Pap smear + HPV testing every five years | |
| Colorectal cancer | Patients with risk factors | Screen per recommendations |
| Patients ≥ 50 years without risk factors | Screening (decide among colonoscopy, flexible sigmoidoscopy, fecal occult blood test) | |
| Lung cancer | Patients 55 to 74 years, ≥30 pack-year smoking history and either currently smoking or quit in the past 15 years | Consider screening with low-dose helical CT scan |
| Prostate cancer | High-risk men 40 to 45 years | Discuss screening, individual decision |
| Men ≥ 50 years without risk factors | Discuss screening, individual decision | |
| Melanoma | High-risk patients | Periodic skin exam |
| Average-risk patients | Remain vigilant for suspicious lesions |
| Workup | Suggestions |
|---|---|
| sIgE and total IgE | Optional |
| Molecular sIgE (CRD) | Optional (polysensitized patients) |
| Tryptase | VIT; mandatory in moderate-severe sting-induced anaphylaxis |
| BAT | VIT; optional (exceptional cases of negative IgE-tests) |
| Complete cell count | Mandatory |
| Glucose, BUN, creatinine, AST, ALT, albumin, electrolytes | Optional |
| ESR, CRP | Optional |
| HIV detection | Highly suggested |
| Hepatitis B/C serology | Optional |
| ANA | Highly suggested, only when physical examination reveals characteristic signs and symptoms posing probability of ARD |
| Pregnancy test | Highly suggested in atypical last menstrual period and/or irregular menses |
| Urinalysis | Optional |
| Stool analysis | Optional |
| Chest X-ray | Highly suggested |
| Cardiology consultation | AIT; optional, when cardiologic problems preexist. VIT; highly suggested in history of sting-induced anaphylactic shock. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pitsios, C.; Petalas, K.; Dimitriou, A.; Parperis, K.; Gerasimidou, K.; Chliva, C. Workup and Clinical Assessment for Allergen Immunotherapy Candidates. Cells 2022, 11, 653. https://doi.org/10.3390/cells11040653
Pitsios C, Petalas K, Dimitriou A, Parperis K, Gerasimidou K, Chliva C. Workup and Clinical Assessment for Allergen Immunotherapy Candidates. Cells. 2022; 11(4):653. https://doi.org/10.3390/cells11040653
Chicago/Turabian StylePitsios, Constantinos, Konstantinos Petalas, Anastasia Dimitriou, Konstantinos Parperis, Kyriaki Gerasimidou, and Caterina Chliva. 2022. "Workup and Clinical Assessment for Allergen Immunotherapy Candidates" Cells 11, no. 4: 653. https://doi.org/10.3390/cells11040653
APA StylePitsios, C., Petalas, K., Dimitriou, A., Parperis, K., Gerasimidou, K., & Chliva, C. (2022). Workup and Clinical Assessment for Allergen Immunotherapy Candidates. Cells, 11(4), 653. https://doi.org/10.3390/cells11040653