Simple Summary
Dyspnea is frequently associated with advanced and terminal cancer, and its relief becomes a key component of symptom management in palliative care. Opioids seem to be the obvious choice for cancer patients as they also address moderate to severe pain usually also present in such patients. Evidence-based conclusions on the effectiveness and safety of opioids in dyspnea management are scarce, and the results are still controversial. We aim to address this knowledge gap by conducting a systematic review of the existing literature and a pooled meta-analysis of the results.
Abstract
Background/Objectives: Dyspnea accompanies end-of-life in many cancer patients, with around 50% experiencing moderate/severe dyspnea, and is an independent factor for poor prognosis and declining quality of life. Managing dyspnea becomes a key component of palliative treatment and end-of-life support for cancer patients. Opioids seem to be the obvious choice in cancer patients as they also address the pain component (often important in such patients). Evidence-based conclusions on the effectiveness/safety of opioids in dyspnea management are scarce, and the results are still controversial. We aim to address this knowledge gap. Methods: In order to achieve the objective of this paper, we conducted a comprehensive search of international databases (PubMed, Medline, Embase, and Cochrane Library) for randomized controlled trials on the use of opioids to treat refractory dyspnea in adult cancer patients, and we performed a pooled meta-analysis of the results. Results: The effect of opioids on the relief of dyspnea was significant (SMD −0.44, 95% CI [−0.75,−0.12], p = 0.007). The significance of the opioid effect is maintained only for morphine administration (SMD −078, 95% CI [−1.45,−0.10], p = 0.02) and only for exertional dyspnea (SMD −1.00, 95% CI [−1.98, −0.03], p = 0.04). No correlation was noted between fentanyl/hydromorphone and dyspnea relief or opioids administered for dyspnea at rest. The subcutaneous route seems to be significantly correlated with dyspnea relief (SMD −0.73, 95% CI [−1.27, −0.19], p = 0.008), while the other administration modalities lack such an effect. No significant correlation was present between the usage of morphine/fentanyl and increased odds of severe adverse effects (OR 1.48, 95% CI [0.57,3.86], p = 0.42); however, fentanyl seems to be associated with increased somnolence. Although we aimed to evaluate how opioids impact the quality of life of cancer patients with dyspnea, we were unable to obtain such results due to the absolute lack of the literature available discussing QoL. Conclusions: Although we managed to provide some insights into the efficiency and safety of opioids usage for dyspnea management in cancer patients, the evidence based on the available literature is low grade. There is a marked need to address this knowledge gap with future high-quality studies with large sample sizes and standardized protocols.
Keywords:
opioid; opioids; morphine; fentanyl; oxycodone; hydromorphone; dyspnea; cancer patients; systematic review; meta-analysis 1. Introduction
Dyspnea usually accompanies the end of life in many cancer patients [1], and more than half will experience moderate to severe dyspnea [2]. This symptom is associated with worsening prognosis as an independent factor [3], and the intensity of dyspnea and the frequency of breathlessness are associated with the decline in quality of life and general condition [4,5]. Cancer patients often experience severe exertional dyspnea and sometimes even rest dyspnea, which often restricts daily life activities and social functioning of patients, leading to psychological effects (such as anger, frustration, or depression), diminished independence, and an increased need for assistance. As such, managing dyspnea becomes a key component of palliative treatment and end-of-life support for cancer patients.
Dyspnea management in cancer patients has as a prerequisite the assessment of underlying pathology and adequate treatment of all reversible causes (such as pulmonary oedema or hyperventilation due to psychologic conditions). Adjustments in daily living and activity may also contribute to dyspnea management and should be considered and implemented as a part of holistic therapeutic approaches. Environmental factors (such as allergens) also need to be considered and removed from the patient’s environment if possible. However, dyspnea in cancer patients has a non-reversible component that needs to be addressed through pharmacologic and non-pharmacologic means.
Among the existing pharmacologic means for treating the non-reversible component of cancer-related dyspnea, opioids take a center position together with benzodiazepines and are often recommended as a first-line pharmacologic intervention by several guidelines [6,7,8]. Opioids seem to be the obvious choice in cancer patients as they also address the pain component (often important in such patients). Nevertheless, evidence-based conclusions on the effectiveness and safety of opioids in dyspnea management are scarce, and the results are still controversial [9,10,11,12,13], with conclusions varying from significant improvements after opioid therapy to no effect. The available literature is also lacking when comparing opioids to other pharmacological options (for example benzodiazepines) or when comparing the effects and safety of various opioids. To the best of our ability, we could only locate three meta-analytic studies discussing opioids as therapeutic options for dyspnea management in cancer patients, but all were forced to admit inconsistent conclusions due to the low number of eligible studies and small sample size [11,12,13]. With this study, we aim to address this knowledge gap by incorporating more recently published studies. We aim at analyzing the overall effectiveness of opioids in dyspnea management in cancer patients (defined as the clinical relief of dyspnea), the effect of opioids in modifying measurable parameters (such as respiratory rate, peripheral oxygen saturation), and the security profile of opioids (adverse effects). A secondary aim of this paper is to evaluate the changes in the quality of life in cancer patients with dyspnea after opioids were administered, if sufficient data are available in the current literature. The analysis will try to compare different types of opioids and different administration routes and to compare opioids to other agents used for dyspnea management.
2. Materials and Methods
2.1. Search Strategy
In order to achieve the objective of this paper, we conducted a comprehensive review of four international databases (PubMed, Medline, Embase, and Cochrane Library) of the literature available on opioid-treated refractory dyspnea in adult cancer patients. The search was guided by the PRISMA principles for systematic reviews [14]. No limitations were imposed for publication year, and the databases were searched from inception until January 2025. All databases were searched using a combination of Boolean coordinators and relevant keywords describing the following: 1. opioids (including but not limited to: “Analgesics, Opioid” [Mesh], opioid*, opiate*, buprenorphine, codeine, fentanyl, heroin, hydrocodone, hydromorphone, laudanon, laudanum, meperidine, methadone, morphine, oxycodone, oxycontin, pentazocine, percocet, pethidine, tramadol, vicodin); 2. dyspnea (dyspnea*, dyspnoea*, dyspneic, short* of breath, breathless*); and 3. cancer patients (“Neoplasms” [Mesh], cancer*, tumor*, tumour*, neoplas*, carcinoma*, adenocarcinoma*, malignan*, oncolog*, sarcoma*). All types of opioids used for dyspnea management were considered eligible regardless of method of administration. No limitations were imposed based on cancer type. We aimed to include only high-quality research. As such, we considered optimal for inclusion only randomized controlled trials (RCT) that compared the effects of opioid usage to placebo or other pharmacologic alternatives (benzodiazepines, other opioids). All studies needed to include some form of dyspnea severity measure—either VAS (visual analog scale for dyspnea), NRS (numeric rating scale), Borg score, CPOT (clinical pain observational tool), or other such scale—as a mean of evaluating the efficacy of intervention.
Exclusion criteria included the following: 1. pediatric populations; 2. patients with other causes for dyspnea than cancer (chronic obstructive pulmonary disease—COPD, congestive heart failure); 3. non-randomized controlled trials (observational studies, single-arm studies, case reports or case series, systematic reviews, and meta-analyses); and 4. language other than English or Spanish. We considered this language limitation adequate since all databases searched provide results in English, at least as abstracts, thus making omission of potentially relevant results highly improbable. Spanish was also chosen as a possible language due to the authors’ familiarity and high number of speakers worldwide.
The primary outcome was the relief of dyspnea as a measure of efficacy of the opioid therapy. Secondary outcomes were the change in quality of life, respiratory rate, and peripheral oxygen saturation (as efficacy outcomes) as well as serious opioids adverse effects (Grade 3 or higher as per Common Terminology Criteria for Adverse Events—CTCAE) [15] and somnolence (as safety outcomes). In Table 1, we present the PICOS criteria (Population, Intervention, Comparison, Outcomes and Study framework for systematic reviews) [16] used for this research.

Table 1.
PICOS criteria for inclusion of trials.
2.2. Data Extraction
The resulting papers were then processed using an automatic tool (Mendeley Reference Manager 2.94.0), and duplicate records were excluded. The remaining articles were then screened for eligibility by title and abstract by two independent authors. Only articles considered eligible by both reviewers were included in the ulterior processing. Reasons for exclusion at this phase included wrong study type or irrelevant focus. Remaining studies were then sought for full-text retrieval, and a full-text screening was performed by two independent authors assessing relevant outcomes, adequate methodology, and overall eligibility. Discrepancies were settled by a third author. Reasons for exclusions were the absence of outcomes of interest, previously published results, type of study (observational), or lack of an available English/Spanish version of the full text.
For each study, we extracted data about the authors, year of publication, sample size and types of cancers included, inclusion and exclusion criteria, study design, intervention, doses and modalities of administration, data on outcomes of interest, and summary of findings.
2.3. Evaluation of the Risk of Bias for Individual Studies
In order to evaluate the inherent risk of bias for each individual included study, we used the seven fields of the modified Cochrane Risk of Bias Assessment Tool [17]—two reviewers evaluated the risk of bias according to random sequence generation, allocation concealment, blinding of participants/personnel, outcome blinding and assessment, incomplete results data, selective reporting of results, and other biases. Discrepancies were then settled by consultation with one of the supervisors.
2.4. Statistical Analysis
All statistical analyses performed during this meta-analysis were conducted using the Review Manager 5.4 software freely available online [18]. Differences between groups and subgroups were compared using chi-square tests. Continuous variables were analyzed as standardized mean differences (SMDs) and 95% confidence intervals (95% CIs). Categorical variables were analyzed using odds ratios (ORs). An effect was considered significant if the OR value did not intersect 1 or if the SMD value did not cross zero. The threshold for statistical significance was considered p-value ≤ 0.05. We conducted a meta-analytic study of the effects of opioids when used as therapeutic options for dyspnea management in cancer patients. I2 type statistics (which represents the proportion of total variation due to heterogeneity rather than sampling error) were used to evaluate heterogeneity between included studies, and an I2 value >50% was considered indicative of high heterogeneity. When such highly heterogenic patterns were observed, we used random effects models in our pooled analysis. In all other cases, fixed effects models were used. Sensitivity analysis was deemed necessary only if we encountered a statistically significant result associated with an I2 > 50%. However, no such situation occurred, so sensitivity analysis was waived. Pooled results analyzing the effectiveness of opioids in the management of dyspnea compared to placebo, additional efficacity outcomes (such as respiratory rate and peripheral oxygen saturation), and adverse effects of opioid therapy were performed and then presented as forest plots. Further subgroup analysis (by type of dyspnea, by opioid type, and by administration modality) were performed in order to discern if any discrepancies in the effectiveness of opioid appear under the influence of these factors. We also performed a multivariate analysis of the dyspnea management effect of opioids and their adverse effects taking into account the type of opioid and the type of controlled used in specific randomized controlled trials (placebo or active).
3. Results
3.1. Study Selection
During our databases search, we identified an initial 1993 records that seemed to meet the criteria for inclusion. An additional 20 records were identified through registers searching and manual evaluation of references. The records were processed using an open-source automated tool (Mendeley Reference Manager [19]), and 759 duplicates were removed. The remaining 1254 records were evaluated based on title and abstract, and 1181 were excluded for irrelevant focus and 22 for not being the correct study type (non-RCT). Out of the 51 studies sought for full-text retrieval, nine were unavailable. The final 42 records were furthered screened, and 29 were excluded (duplicate research, no outcomes of interest, wrong study type, and not available in English/Spanish). The final 13 RCTs were included in this analytic study. There were a few promising RCTs that seemed to meet the inclusion criteria but finally were rejected due to including mixed populations with a high number of benign disease patients that may interfere with the analysis [20], comparing the effects of opioids to non-pharmacologic methods such as acupuncture [21], or not available in English or Spanish [22]. The PRISMA search flow diagram is presented in Figure 1.
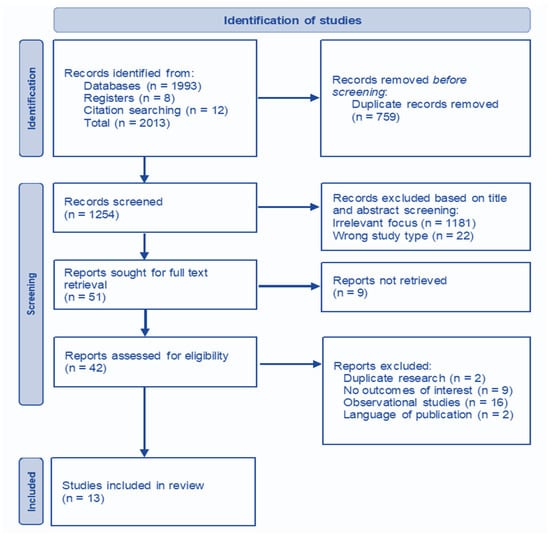
Figure 1.
PRISMA search flow diagram.
3.2. Risk of Bias
The inherent risk of bias for each individual included study was evaluated using the modified Cochrane Risk of Bias Assessment Tool. The author’s judgement is presented in Figure 2 both as results for each study and as an overall risk across studies. Three studies were evaluated as low risk [23,24,25], four as high risk [26,27,28,29], and six as intermediate (unclear) risk [30,31,32,33,34,35].
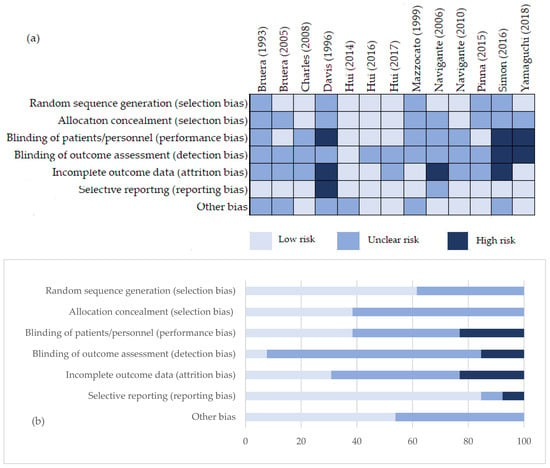
Figure 2.
Risk of bias assessment. (a) Authors’ judgement about each risk of bias item for each included study [23,24,25,26,27,28,29,30,31,32,33,34,35]; (b) authors’ judgements about each risk of bias item presented as percentages across all included studies.
3.3. Characteristics of Included Studies
A total of 397 patients were enrolled in the 13 randomized controlled trials included. Sample sized had a median of 30.5 enrolled patients (varying from 9 to 101). All studies included cancer patients with rest/exertional dyspnea. Most patients had primary lung cancer or lung metastases, but the study cohort also included other forms of cancers such as gastro-intestinal, genito-urinary, sarcomas, or hematologic cancers. Placebo control was used in eight studies [23,24,25,28,30,32,33,35], while active control was used in five [26,27,29,31,34]. In three studies, opioids were compared to other opioids [26,27,31] and with benzodiazepines in two studies [29,34]. Opioids were administered through subcutaneous injections, transmucosal path, per oral, and in nebulized form. To the best of our ability, we could not identify any studies describing the effect of intravenous opioids. The main characteristics of the included studies are presented in Table 2.
Table 2.
Characteristics of included RCT.
3.4. Primary Outcome—Dyspnea Relief
The primary outcome was evaluated in seven studies with morphine, five with fentanyl, one with oxycodone (this study is also counted as a Fentanyl study since it compares the effects of the two opioids), and one with hydromorphone. From these studies only those that expressed the intensity of dyspnea as a continuous variable or for which a clearance interval could be estimated and did not compare various forms of opioids were introduced in the pooled analysis. Finally, seven RCTs—two with morphine, four with fentanyl, and one with hydromorphone—were used for the integrated analysis, all of which were placebo controlled. The effect of opioids was significant (SMD −0.44 95% CI [−0.75,−0.12], p = 0.007) (Figure 3). No sensitivity analysis was performed for this outcome due to the absence of heterogeneity between studies (I2 = 0%). No significant publication bias was observed for this outcome when examining the corresponding funnel plot.
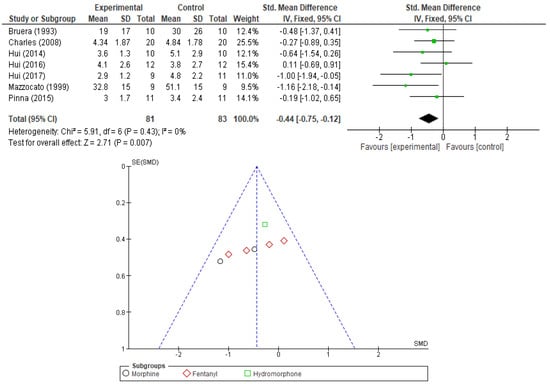
Figure 3.
Forest plot comparing the effect of opioids vs. PL in relief of dyspnea and corresponding funnel plot (showing lack of publication bias) [23,24,25,30,32,33,35].
To better discern the intricacies of the opioid effect on the primary outcome (dyspnea relief) we performed additional subgroup analysis evaluating the results by opioid type, administration modality, and type of dyspnea. In Table 3, we summarize these findings highlighting in bold the results that maintain statistical significance and a low level of heterogeneity. The significance of the opioid effect is maintained only for morphine administration (SMD −078, 95% CI [−1.45,−0.10], p-value = 0.02) and only for exertional dyspnea (SMD −1.00, 95% CI [−1.98, −0.03], p-value = 0.04). No correlation was noted between fentanyl or hydromorphone and dyspnea relief. Opioids seem to play a role in the relief of exertional dyspnea but not dyspnea at rest. Also, the subcutaneous administration seems to be significantly correlated with dyspnea relief (SMD −0.73, 95% CI [−1.27, −0.19], p-value = 0.008), while the other administration modalities lack such effect.
Table 3.
Subgroup analysis for primary outcome (dyspnea relief).
Additionally, we wanted to find out if the type of control used in the RCTs has any influence on the perceive effect of opioids in dyspnea relief. We compared the results of trials using placebo as control and those using active controls. The results are presented as forest plots in Figure 4 and Figure 5 (for morphine and fentanyl). Only when compared to placebo controls, the morphine effect maintained its significance—SMD −0.78, 95% CI [−1.45, −0.10], p-value = 0.02, I2 = 0%. When compared to active controls the significance was lost—SMD 0.48, 95% CI [−0.23, 1.19], p-value = 0.18, I2 = 0%. The difference in effect between the two subgroups was significant (p-value = 0.01). For fentanyl, we could not establish any significant correlation with dyspnea relief despite the type of control used (placebo—SMD −0.37, 95% CI [−0.81, 0.06], p-value = 0.09; active control—SMD −0.41, 95% CI [−1.44, 0.62], p-value = 0.43), and this result is in concordance with the previous subgroup analysis.
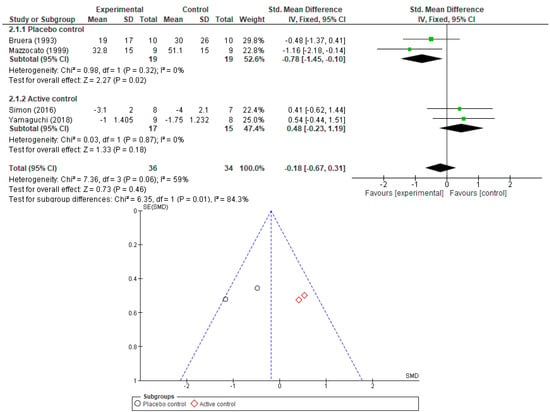
Figure 4.
Forest plot comparing the effect of morphine on dyspnea relief: subgroup analysis by type of control used in RCT (placebo or active control studies) and corresponding funnel plot (showing lack publication bias) [26,27,30,33].
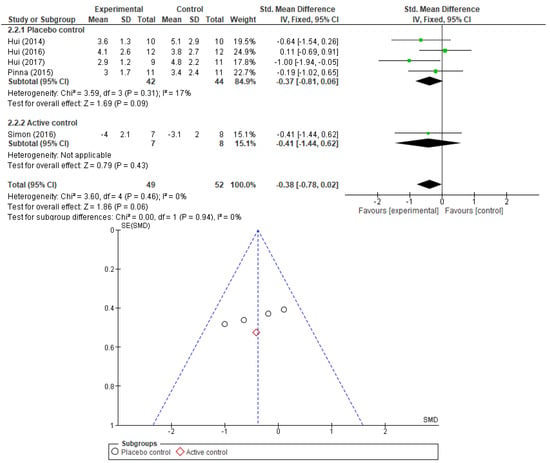
Figure 5.
Forest plot comparing the effect of fentanyl in relief of dyspnea: subgroup analysis by type of control used in RCT (placebo or active control studies) and corresponding funnel plot (showing lack of publication bias) [23,24,25,26,35].
3.5. Secondary Outcomes
Secondary outcomes included three efficacy indicators (quality of life, respiratory rate, and peripheral oxygen saturation) and two safety indicators (reported severe adverse reactions and somnolence).
No RCT discussing the quality of life (QoL) in cancer patients receiving opioids for dyspnea management met the inclusion criteria in the current meta-analysis. We could only identify one study [21] that approached the subject of QoL after opioid therapy; however, this study compared the effects of morphine to a non-pharmacologic alternative (acupuncture). Therefore, it was considered unsuitable for analysis.
Information on respiratory rate (RR) and peripheral oxygen saturation (SaO2) was included in six and seven RCTs, respectively. No correlation could be established between opioid therapy and a detrimental effect on respiratory rate or a corresponding improvement in peripheral oxygen saturation, neither as changes from baseline levels nor as post-intervention results. Results are presented in Figure 6 and Figure 7. No sensitivity analysis was performed due to low heterogeneity. No significant publication bias was found when investigating the corresponding funnel plots.
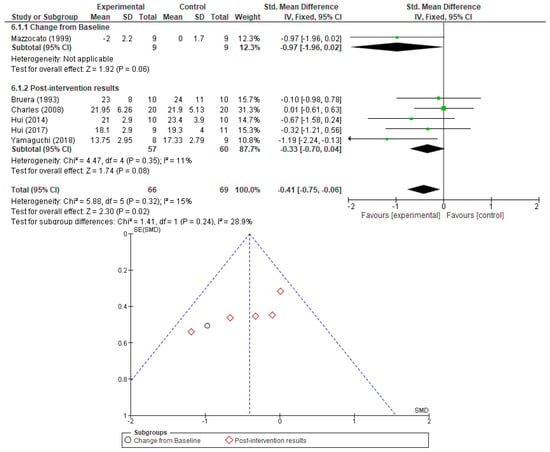
Figure 6.
Respiratory rate analysis as a measure of opioid effect and the corresponding funnel plot [23,24,27,30,32,33].
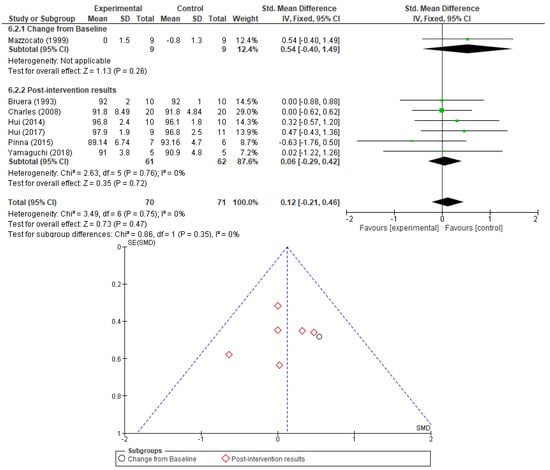
Figure 7.
Peripheral oxygen saturation analysis as a measure of opioid effect and the corresponding funnel plot [23,24,27,30,31,33,35].
The safety secondary outcomes we analyzed were the severe adverse reactions related to opioid usage in general and somnolence in particular (as the most frequent complication of therapy). Three studies [29,34,35] presented information on severe adverse reactions and 6 [23,25,27,29,33,34] offered details on somnolence. No significant correlation was present between the usage of morphine/fentanyl for dyspnea relief in cancer patients and increased odds of treatment-related severe adverse effects or somnolence (OR 1.48, 95% CI [0.57, 3.86], p-value = 0.42 and OR 1.00, 95% CI [0.55, 1.82], p-value = 1.00, respectively). Although there was no high heterogeneity observed between studies (I2 = 41%) for the somnolence outcome, we could perform a subgroup analysis to see if the type of opioid used and the type of study control may influence the overall effect. When analyzing somnolence by opioid type, we encountered a significant subgroup difference (I2 = 78.8%, p-value = 0.03). Fentanyl usage was associated with increased somnolence odds (OR 0.15, 95% CI [0.02–1.00]), and this was significant (p-value = 0.05, I2 = 0%). No such association occurred when analyzing morphine usage (OR 1.39, 95% CI [0.71, 2.70], p-value = 0.34). The odds of somnolence occurring was not influenced in any way by the type of control used in the RCTs (placebo or active). These results are presented in Figure 8 and Figure 9.
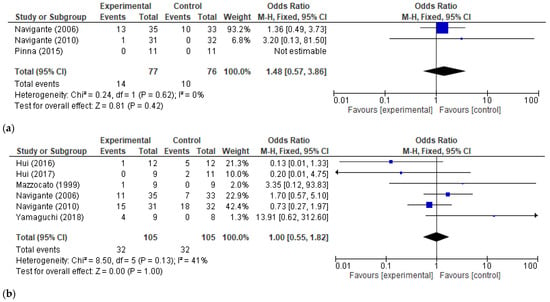
Figure 8.
Opioid treatment-related adverse reactions. (a) Forest plot for severe adverse effects (SAEs) caused by opioids vs. control—overall effect; (b) Forest plots for somnolence caused by opioids vs. control—overall effect [23,25,27,29,33,34,35].
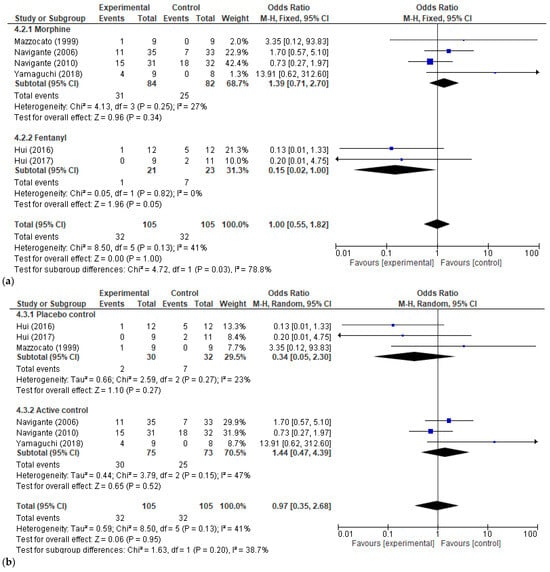
Figure 9.
Subgroup analysis of opioid treatment-related somnolence. (a) By type of opioid; (b) by type of control—placebo vs. active control [23,25,27,29,33,34].
4. Discussion
In our study, we included 13 RCTs with a total of 397 patients. The majority of studies offered information on Morphine and fentanyl; however, for all other opioids, there is a scarcity of literature (oxycodone and hydromorphone effects were described in one study each, and no additional studies on other type of opioids could be located, thus making it impossible to assess the effects and safety of these opioids). Unfortunately, the quality of the included studies is not optimal due to small sample sizes (some of them with less than 10 patients per arm) and unclear/high risk of bias. Additionally, methodological shortcomings may have influenced the results. The patients enrolled belong to an especially frail category (as exemplified by an average time until death of 5 days reported by some studies [36]), thus making it, by definition, unethical to deny crossover from placebo to active treatment. Crossover, although understandable in these situations, gives rise to increased risk of cofounding and difficult analysis of results. Concerns about patients’ safety and comfort may also justify the shorter washout periods observed in some studies [12,30,33] when patients crossover. The fact that cancer patients with symptomatic dyspnea may deteriorate suddenly and irreversible is a reality that makes it extremely difficult to conduct large randomized double-blind controlled trials with rigorous protocols, thus making it acceptable to include such a study in a pooled meta-analysis study with the current level of evidence. Another barrier in conducting high-quality studies analyzing the effects of opioids in cancer-related dyspnea is the “opiophobia”—the concern that these drugs may cause respiratory depression and hasten death [37]—which may limit enrolment. In addition to previously discussed limitations, we have to remark that there is a high variability between how the results are reported—in some studies, we could not extrapolate usable data for the integrated studies although the studies discussed the outcomes of interest. Although standardized, the forms used to evaluate dyspnea relief across studies vary widely (VAS, NRS, Borg score, 6MWT), thus limiting the possibilities of analysis.
Even so, we were able to draw some usable conclusions that add to the existing knowledge. The primary outcome analysis (dyspnea relief) showed the overall superiority of opioids when compared to placebo. However, the superiority was not maintained when comparing the opioids to active controls. This leaves room for the possible inferiority of results to other pharmacologic options (such as benzodiazepines); however, such conclusions cannot be drawn at this time due to the lack of relevant studies and small sample sizes. The subgroup analysis also seemed to indicate that the observed superiority maintains significance only when administering morphine (no correlation was noted between fentanyl or hydromorphone and dyspnea relief) and only when the opioids are used for exertional dyspnea relief (no significant correlation was found between opioid usage and rest dyspnea relief). Several potential reasons contribute to the limited effectiveness of opioids other than morphine in the management of dyspnea in cancer patients. One factor is the pharmacokinetic variability among opioids. Morphine has a relatively predictable onset and duration of action, which facilitates titration and monitoring. Other opioids, such as fentanyl and oxycodone, have variable absorption rates depending on the route of administration and patient-specific factors, such as hepatic or renal function, which may lead to inconsistent symptom control. The route of administration also plays a role. Morphine is often given orally or subcutaneously, both effective for managing dyspnea in palliative settings. Other opioids, particularly fentanyl, are commonly administered via transdermal or intranasal routes, which may not provide the rapid relief required for acute dyspnea episodes. This may limit their utility in urgent symptom management. We have to mention that no real possibility of evaluating opioids such as oxycodone or methadone was available (no relevant studies). Also, most of the studies on fentanyl focused on exertional dyspnea, and this choice can influence the results of the current analysis. Subcutaneous administration seems to be significantly correlated with dyspnea relief, while the other administration modalities lack such effect.
QoL is the most important measurement of the efficacity of therapeutic and lifestyle interventions and provides prognostic information on patient survival and subsequent evolution [38]. No RCT discussing the QoL of cancer patients receiving opioids for dyspnea management met the inclusion criteria in the current meta-analysis. We could only identify one study [21] that approached the subject of QoL after opioid therapy. However, this study compared the effects of morphine to a non-pharmacologic alternative (acupuncture); therefore, it was considered unsuitable for analysis.
No correlation could be established between opioid therapy and a detrimental effect on respiratory rate or a corresponding improvement in peripheral oxygen saturation, neither as changes from baseline levels nor as post-intervention results. This is partially contrary to previous studies that showed that opioids may induce a decline in respiratory rate [39]. As such, the evidence on the safety of opioid usage in cancer-related dyspnea remains controversial.
The safety secondary outcomes we analyzed were the severe adverse reactions related to opioid usage in general and somnolence in particular (as the most frequent complication of therapy). No significant correlation was present between the usage of morphine/fentanyl for dyspnea relief in cancer patients and increased overall odds of treatment-related severe adverse effects or somnolence. However, only fentanyl seemed to increase somnolence.
Study Limitations
Conducting proper randomized controlled studies in palliative care, especially when such involving cancer patients (who are very vulnerable, prone to rapid irreversible decline, and present unique challenges in obtaining consent and psychological issues) is more difficult than in other medical fields [40,41]. Unfortunately, the number of studies included in this meta-analysis is small, and most sample sizes were very limited. A high percentage of the included studies were considered high risk of bias (30%) providing results with a low level of evidence. In addition, many studies allowed for crossover but had a very short period of washout, which may lead to potential biases in outcome assessment. We found it difficult to analyze the safety of the opioid intervention due to the limited number of studies reporting comprehensively on adverse effects. In addition, there is little to no literature available evaluating QoL outcomes in cancer patients receiving opioid therapy for dyspnea management or evaluating the effect of some opioids like oxycodone or hydromorphone. Similar to problems noted for cancer survivorship or choosing a tailored therapeutic approach for each patient [42,43,44,45], palliative care also faces its challenges, and thus far, adequate studies for clarifying the effect and safety of the intervention are lacking. Another potential source of bias is the exclusion of studies published in other languages than English and Spanish, and this may result in potentially omitting relevant results of the database search.
5. Conclusions
Although we managed to provide some insights into the efficiency and safety of opioid usage for dyspnea management in cancer patients (1. Morphine seems to be the only type of opioid significantly associated with dyspnea relief; 2. Opioids seem to be effective only in the relief of exertional dyspnea and to a lesser degree for rest dyspnea; 3. The subcutaneous route of administration seems to be more effective in delivering optimal opioid dyspnea management; and 4. Opioids seem not to increase the frequency of severe adverse reactions, but fentanyl is associated with increased somnolence), the evidence based on the available literature is low grade. There is a marked need to address this knowledge gap using future high-quality studies with large sample sizes and standardized protocols and scales for measuring the effects of the intervention. Such studies should address both the efficiency and safety of opioids (including less used opioids such as oxycodone or hydromorphone). QoL in post-intervention settings should also be clarified through more rigorous research.
Author Contributions
Conceptualization, E.C.; methodology, E.C. and D.V.M.; validation, V.R., E.C. and L.S.; formal analysis, E.C.; software, E.C.; writing—original draft preparation, E.C.; writing—review and editing, V.R., G.G. and E.C.; supervision, L.S. and D.V.M. All authors have read and agreed to the published version of the manuscript.
Funding
Publication of this paper was supported by the University of Medicine and Pharmacy “Carol Davila” through the institutional program “Publish not Perish”.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All studies included in this review are available online.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| COPD | Chronic obstructive pulmonary disease |
| CTCAE | Common Terminology Criteria for Adverse Events |
| PICOS | Population, Intervention, Comparison, Outcomes and Study framework for systematic reviews |
| SMD | Standardized mean differences |
| OR | Odds ratio |
| 95% CI | 95 percent confidence interval |
| RCTs | Randomized controlled trials |
| Mo | Morphine |
| Fent | Fentanyl |
| HyMo | Hydromorphone |
| Oxy | Oxycodone |
| po | Per oral |
| sc | Subcutaneous administration |
| tm | Transmucosal administration |
| Inhal | Inhalation |
| SAEs | Severe adverse reactions |
| NS | Not specified |
| HTA | Arterial hypertension |
| RR | Respiratory rate |
| SaO2 | Peripheral oxygen saturation |
| VAS | Visual analog scale for dyspnea |
| CPOT | Clinical pain observational tool |
| ECOG | Eastern Cooperative Oncology Group |
| NRS | Numeric rating scale |
| QoL | Quality of life |
| KPS | Karnofsky performance status |
| MEDD | Morphine equivalent daily dose |
| DOME | Daily oral morphine equivalent dose. Effective dose: Dose that reduced the intensity of dyspnea by at least 50%. |
| 6MWT | 6-min walk test |
| OTFC | Oral transmucosal fentanyl citrate |
| FBT | Fentanyl buccal tablet |
| FPNS | Fentanyl pectin nasal spray |
References
- Booth, S.; Silvester, S.; Todd, C. Breathlessness in Cancer and Chronic Obstructive Pulmonary Disease: Using a Qualitative Approach to Describe the Experience of Patients and Carers. Palliat. Support. Care 2003, 1, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.-S.; Tse, D.M.W.; Sham, M.M.K. Dyspnoea and Other Respiratory Symptoms in Palliative Care. In Oxford Textbook of Palliative Medicine; Oxford Academic: Oxford, UK, 2015; pp. 421–434. [Google Scholar] [CrossRef]
- Cuervo Pinna, M.Á.; Vargas, R.M.; Moralo, M.J.R.; Correas, M.Á.S.; Pera Blanco, G. Dyspnea—a Bad Prognosis Symptom at the End of Life. Am. J. Hosp. Palliat. Care 2009, 26, 89–97. [Google Scholar] [CrossRef]
- Currow, D.C.; Smith, J.; Davidson, P.M.; Newton, P.J.; Agar, M.R.; Abernethy, A.P. Do the Trajectories of Dyspnea Differ in Prevalence and Intensity by Diagnosis at the End of Life? A Consecutive Cohort Study. J. Pain Symptom Manag. 2010, 39, 680–690. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, S.; Casuccio, A.; Fulfaro, F. The Course of Symptom Frequency and Intensity in Advanced Cancer Patients Followed at Home. J. Pain Symptom Manag. 2000, 20, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Maddocks, M.; Johnson, M.J.; Ekström, M.; Simon, S.T.; Ogliari, A.C.; Booth, S.; Ripamonti, C.I. Management of Breathlessness in Patients with Cancer: ESMO Clinical Practice Guidelines. ESMO Open 2020, 5, e001038. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Goya, S.; Kohara, H.; Watanabe, H.; Mori, M.; Matsuda, Y.; Nakamura, Y.; Sakashita, A.; Nishi, T.; Tanaka, K. Treatment Recommendations for Respiratory Symptoms in Cancer Patients: Clinical Guidelines from the Japanese Society for Palliative Medicine. J. Palliat. Med. 2016, 19, 925–935. [Google Scholar] [CrossRef]
- Hui, D.; Bohlke, K.; Bao, T.; Campbell, T.C.; Coyne, P.J.; Currow, D.C.; Gupta, A.; Leiser, A.L.; Mori, M.; Nava, S.; et al. Management of Dyspnea in Advanced Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1389–1411. [Google Scholar] [CrossRef] [PubMed]
- Ekström, M.; Bajwah, S.; Bland, J.M.; Currow, D.C.; Hussain, J.; Johnson, M.J. One Evidence Base; Three Stories: Do Opioids Relieve Chronic Breathlessness? Thorax 2018, 73, 88–90. [Google Scholar] [CrossRef]
- Johnson, M.J.; Abernethy, A.P.; Currow, D.C. Gaps in the Evidence Base of Opioids for Refractory Breathlessness. A Future Work Plan? J. Pain Symptom Manag. 2012, 43, 614–624. [Google Scholar] [CrossRef]
- Barnes, H.; Mcdonald, J.; Smallwood, N.; Manser, R. Opioids for the Palliation of Refractory Breathlessness in Adults with Advanced Disease and Terminal Illness. Cochrane Database Syst. Rev. 2016, 2016, CD011008. [Google Scholar] [CrossRef]
- Simon, S.T.; Köskeroglu, P.; Gaertner, J.; Voltz, R. Fentanyl for the Relief of Refractory Breathlessness: A Systematic Review. J. Pain Symptom Manag. 2013, 46, 874–886. [Google Scholar] [CrossRef] [PubMed]
- Ben-Aharon, I.; Gafter-Gvili, A.; Leibovici, L.; Stemmer, S.M. Interventions for Alleviating Cancer-Related Dyspnea: A Systematic Review and Meta-Analysis. Acta Oncol. 2012, 51, 996–1008. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) Common Terminology Criteria for Adverse Events (CTCAE) v5.0. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 6 March 2024).
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) Design as a Framework to Formulate Eligibility Criteria in Systematic Reviews. Emerg. Med. J. 2020, 37, 387. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- RevMan|Cochrane Training. Available online: https://training.cochrane.org/online-learning/core-software/revman (accessed on 24 January 2023).
- Mendeley Reference Manager|Mendeley. Available online: https://www.mendeley.com/reference-management/reference-manager (accessed on 28 January 2023).
- Date, K.; Williams, B.; Cohen, J.; Chaudhuri, N.; Bajwah, S.; Pearson, M.; Higginson, I.; Norrie, J.; Keerie, C.; Tuck, S.; et al. Modified-Release Morphine or Placebo for Chronic Breathlessness: The MABEL Trial Protocol. ERJ Open Res. 2023, 9, 00167-2023. [Google Scholar] [CrossRef] [PubMed]
- Minchom, A.; Punwani, R.; Filshie, J.; Bhosle, J.; Nimako, K.; Myerson, J.; Gunapala, R.; Popat, S.; O’brien, M.E.R. A Randomised Study Comparing the Effectiveness of Acupuncture or Morphine versus the Combination for the Relief of Dyspnoea in Patients with Advanced Non-Small Cell Lung Cancer and Mesothelioma. Eur. J. Cancer 2016, 61, 102–110. [Google Scholar] [CrossRef]
- Grimbert, D.; Lubin, O.; De Monte, M.; Vecellio None, L.; Perrier, M.; Carré, P.; Lemarié, E.; Boissinot, E.; Diot, P. Dyspnée et Aérosols de Morphine Dans Les Soins Palliatifs Du Cancer Broncho-Pulmonaire. Rev. Des Mal. Respir. 2004, 21, 1091–1097. [Google Scholar] [CrossRef]
- Hui, D.; Kilgore, K.; Park, M.; Williams, J.; Liu, D.; Bruera, E. Impact of Prophylactic Fentanyl Pectin Nasal Spray on Exercise-Induced Episodic Dyspnea in Cancer Patients: A Double-Blind, Randomized Controlled Trial. J. Pain Symptom Manag. 2016, 52, 459–468.e1. [Google Scholar] [CrossRef]
- Hui, D.; Xu, A.; Frisbee-Hume, S.; Chisholm, G.; Morgado, M.; Reddy, S.; Bruera, E. Effects of Prophylactic Subcutaneous Fentanyl on Exercise-Induced Breakthrough Dyspnea in Cancer Patients: A Preliminary Double-Blind, Randomized, Controlled Trial. J. Pain Symptom Manag. 2014, 47, 209–217. [Google Scholar] [CrossRef]
- Hui, D.; Kilgore, K.; Frisbee-Hume, S.; Park, M.; Liu, D.; Balachandran, D.D.; Bruera, E. Effect of Prophylactic Fentanyl Buccal Tablet on Episodic Exertional Dyspnea: A Pilot Double-Blind Randomized Controlled Trial. J. Pain Symptom Manag. 2017, 54, 798–805. [Google Scholar] [CrossRef] [PubMed]
- Simon, S.T.; Kloke, M.; Alt-Epping, B.; Gärtner, J.; Hellmich, M.; Hein, R.; Piel, M.; Cornely, O.A.; Nauck, F.; Voltz, R. EffenDys-Fentanyl Buccal Tablet for the Relief of Episodic Breathlessness in Patients With Advanced Cancer: A Multicenter, Open-Label, Randomized, Morphine-Controlled, Crossover, Phase II Trial. J. Pain Symptom Manag. 2016, 52, 617–625. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Matsuda, Y.; Matsuoka, H.; Hisanaga, T.; Osaka, I.; Watanabe, H.; Maeda, I.; Imai, K.; Tsuneto, S.; Wagatsuma, Y.; et al. Efficacy of Immediate-Release Oxycodone for Dyspnoea in Cancer Patient: Cancer Dyspnoea Relief (CDR) Trial. Jpn. J. Clin. Oncol. 2018, 48, 1070–1075. [Google Scholar] [CrossRef]
- Davis, C.; Penn, K.; A’Hern, R.; Daniels, J.; Slevin, M. Single Dose Randomised Controlled Trial of Nebulised Morphine in Patients with Cancer Related Breathlessness. Palliat. Med. 1996, 10, 64–65. [Google Scholar]
- Navigante, A.H.; Cerchietti, L.C.A.; Castro, M.A.; Lutteral, M.A.; Cabalar, M.E. Midazolam as Adjunct Therapy to Morphine in the Alleviation of Severe Dyspnea Perception in Patients with Advanced Cancer. J. Pain Symptom Manag. 2006, 31, 38–47. [Google Scholar] [CrossRef]
- Bruera, E.; MacEachern, T.; Ripamonti, C.; Hanson, J. Subcutaneous Morphine for Dyspnea in Cancer Patients. Ann. Intern. Med. 1993, 119, 906–907. [Google Scholar] [CrossRef] [PubMed]
- Bruera, E.; Sala, R.; Spruyt, O.; Palmer, J.L.; Zhang, T.; Willey, J. Nebulized versus Subcutaneous Morphine for Patients with Cancer Dyspnea: A Preliminary Study. J. Pain Symptom Manag. 2005, 29, 613–618. [Google Scholar] [CrossRef]
- Charles, M.A.; Reymond, L.; Israel, F. Relief of Incident Dyspnea in Palliative Cancer Patients: A Pilot, Randomized, Controlled Trial Comparing Nebulized Hydromorphone, Systemic Hydromorphone, and Nebulized Saline. J. Pain Symptom Manag. 2008, 36, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Mazzocato, C.; Buclin, T.; Rapin, C.H. The Effects of Morphine on Dyspnea and Ventilatory Function in Elderly Patients with Advanced Cancer: A Randomized Double-Blind Controlled Trial. Ann. Oncol. 1999, 10, 1511–1514. [Google Scholar] [CrossRef]
- Navigante, A.H.; Castro, M.A.; Cerchietti, L.C.C. Morphine versus Midazolam as Upfront Therapy to Control Dyspnea Perception in Cancer Patients While Its Underlying Cause Is Sought or Treated. J. Pain Symptom Manag. 2010, 39, 820–830. [Google Scholar] [CrossRef]
- Pinna, M.Á.C.; Bruera, E.; Moralo, M.J.R.; Correas, M.Á.S.; Vargas, R.M. A Randomized Crossover Clinical Trial to Evaluate the Efficacy of Oral Transmucosal Fentanyl Citrate in the Treatment of Dyspnea on Exertion in Patients with Advanced Cancer. Am. J. Hosp. Palliat. Care 2015, 32, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Mori, M.; Kawaguchi, T.; Imai, K.; Yokomichi, N.; Yamaguchi, T.; Suzuki, K.; Matsunuma, R.; Watanabe, H.; Maeda, I.; Matsumoto, Y.; et al. Visualizing How to Use Parenteral Opioids for Terminal Cancer Dyspnea: A Pilot, Multicenter, Prospective, Observational Study. J. Pain Symptom Manag. 2021, 62, 936–948. [Google Scholar] [CrossRef]
- Morgan, J.P. American Opiophobia. Adv. Alcohol Subst. Abus. 1985, 5, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Gotay, C.C.; Kawamoto, C.T.; Bottomley, A.; Efficace, F. The Prognostic Significance of Patient-Reported Outcomes in Cancer Clinical Trials. J. Clin. Oncol. 2008, 26, 1355–1363. [Google Scholar] [CrossRef]
- Luo, N.; Tan, S.; Li, X.; Singh, S.; Liu, S.; Chen, C.; Huang, Z.; Feng, S.; Lin, Y.; Lin, Y.; et al. Efficacy and Safety of Opioids in Treating Cancer-Related Dyspnea: A Systematic Review and Meta-Analysis Based on Randomized Controlled Trials. J. Pain Symptom Manag. 2021, 61, 198–210.e1. [Google Scholar] [CrossRef]
- Abernethy, A.P.; Capell, W.H.; Aziz, N.M.; Ritchie, C.; Prince-Paul, M.; Bennett, R.E.; Kutner, J.S. Ethical Conduct of Palliative Care Research: Enhancing Communication Between Investigators and Institutional Review Boards. J. Pain Symptom Manag. 2014, 48, 1211. [Google Scholar] [CrossRef]
- Addington-Hall, J.M.; Bruera, E.; Higginson, I.J.; Payne, S. Research Methods in Palliative Care; Oxford Academic: Oxford, UK, 2011; pp. 1–336. [Google Scholar] [CrossRef]
- Rotaru, V.; Chitoran, E.; Cirimbei, C.; Cirimbei, S.; Simion, L. Preservation of Sensory Nerves During Axillary Lymphadenectomy. In Proceedings of the 35th Balkan Medical Week, Athens, Greece, 25–27 September 2018; Available online: https://www.webofscience.com/wos/woscc/full-record/WOS:000471903700045 (accessed on 20 July 2023).
- Manea, E.; Chitoran, E.; Rotaru, V.; Ionescu, S.; Luca, D.; Cirimbei, C.; Alecu, M.; Capsa, C.; Gafton, B.; Prutianu, I.; et al. Integration of Ultrasound in Image-Guided Adaptive Brachytherapy in Cancer of the Uterine Cervix. Bioengineering 2024, 11, 506. [Google Scholar] [CrossRef] [PubMed]
- Simion, L.; Rotaru, V.; Cirimbei, C.; Stefan, D.-C.; Gherghe, M.; Ionescu, S.; Tanase, B.C.; Luca, D.C.; Gales, L.N.; Chitoran, E. Analysis of Efficacy-To-Safety Ratio of Angiogenesis-Inhibitors Based Therapies in Ovarian Cancer: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13, 1040. [Google Scholar] [CrossRef]
- Chitoran, E.; Rotaru, V.; Mitroiu, M.-N.; Durdu, C.-E.; Bohiltea, R.-E.; Ionescu, S.-O.; Gelal, A.; Cirimbei, C.; Alecu, M.; Simion, L. Navigating Fertility Preservation Options in Gynecological Cancers: A Comprehensive Review. Cancers 2024, 16, 2214. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).