
Exploring the Microbiome’s Impact on Glioma and Brain Metastases: Insights into Development, Progression, and Treatment Response—A Scoping Review

 , , and
, , and 
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Protocol
2.2. Eligibility Criteria
2.3. Information Sources and Search
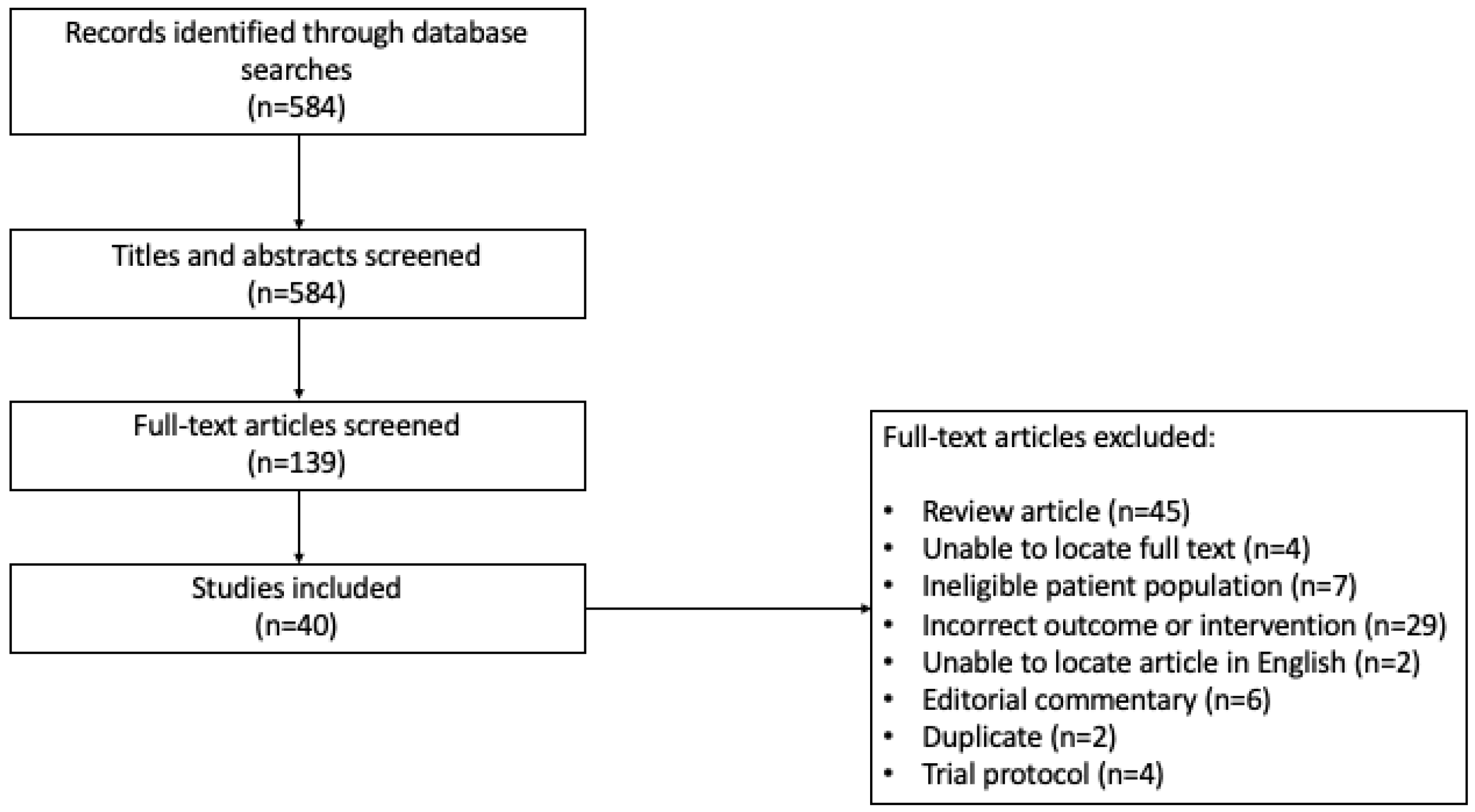
2.4. Study Selection
2.5. Extraction of Data
2.6. Outcome Measures
3. Results
3.1. Characteristics of Selected Studies
3.2. Study Characteristics: Microbiome and Brain Tumor Development Relationship
3.3. Microbiome Signatures Associated with Primary Brain Tumor Growth
3.4. Microbiome Signatures Associated with Brain Metastasis
3.5. Microbiome Signatures Associated with Treatment Response
3.6. Impact of Dietary Changes on the Microbiome and Brain Tumors
3.7. Microbiome and the Immune System
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
| Set # | Search Query | Results |
| 17 | #16 AND #9 | 135 |
| 16 | #12 OR #11 OR #13 OR #14 OR #15 | 222447 |
| 15 | (“brain-gut” or “gut-brain”) NEAR/3 (axis or axes or crosstalk* or cross-talk* or interplay* or inter-play or interact* or inter-act*) (Topic) | 6002 |
| 14 | dysbiosis or dysbioses or dysbiotic* or “dys-biosis” or “dys-bioses” or “dys-biotic” or “dys-biotics” or disbiosis or disbioses or disbiotic* or “dis-biosis” or “dis-bioses” or “dis-biotic” or “dis-biotics” or dysbacterios* or dys-bacterios* or disbacterios* or dis-bacterios* or dyssymbio* or dys-symbio* or dissymbio* or dis-symbio* (Topic) | 18291 |
| 13 | (mouth or mouths or oral or throat or throats or dental or tooth or teeth) NEAR/3 (bacteria* or bacterium or flora or florae or floral or floras or microb* or micro-b* or microflora* or “micro-flora” or “micro-floras” or “micro-floral” or “micro-floras” or microbe* or microorganism* or “micro-organism” or “micro-organisms”) (Topic) | 19081 |
| 12 | (alimentary or bowel or bowels or digesti* or enteric* or gastric* or gut or GI or intestin* or gastrointestin* or “gastro-intestine” or “gastro-intestines” or “gastro-intestinal” or caecal or cecal or cecum or colon or colon or colons or colonic or duodenum or faecal or fecal or feces or ileum or jejunum or stomach or stool or stools or anal or anally or anus or anuses or rectal or rectally or rectum or rectums) NEAR/3 (bacteria* or bacterium or flora or florae or floral or floras or microb* or micro-b* or microflora* or “micro-flora” or “micro-floras” or “micro-floral” or “micro-floras” or microbe* or microorganism* or “micro-organism” or “micro-organisms”) (Topic) | 145634 |
| 11 | microbiome* or “micro-biome” or “micro-biomes” or microbiota* or “micro-biota” or “micro-biotas” or “bacterial biome” or “bacterial biomes” or bacteriobiome* or “bacterio-biome” or “bacterio-biomes” or bacteriome* or “fungal biome” or “fungal biomes” or “fungi biome” or “fungi biomes” or “fungus biome” or “fungus biomes” or “myco-biome” or “myco-biomes” or phagome* or “viral biome” or “viral biomes” or “virus biome” or “virus biomes” or viralbiome* or virobiome* or virobiota* or virome* (Topic) | 152006 |
| 10 | #8 OR #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1 | 238544 |
| 9 | #8 OR #7 OR #6 OR #5 OR #4 OR #3 OR #2 OR #1 | 238544 |
| 8 | (brain or brains or cerebral* or cerebell* or cerebri or cerebrum or intracerebral* or intra-cerebral* or intracran* or intra-cran* or midline or subtentorial or “sub-tentorial” or supratentorial or “supra-tentorial”) NEAR/3 (metasta* or meta-sta* or micrometasta* or micro-metasta*) (Topic) | 29744 |
| 7 | oligodendroglioma* or “oligodendro-glioma” or “oligodendro-gliomas” or “oligo-dendroglioma” or “oligo-dendrogliomas” or “oligo-dendro-glioma” or “oligo-dendro-gliomas” or olegodendrocytoma* or “olegodendro-cytoma” or “olegodendro-cytomas” or “olego-dendrocytoma” or “olego-dendrocytomas” or “olego-dendro-cytoma” or “olego-dendro-cytomas” or oligodendrocytoma* or “oligodendro-cytoma” or “oligodendro-cytomas” or “oligo-dendrocytoma” or “oligodendro-cytomas” or “oligo-dendro-cytoma” or “oligo-dendro-cytomas” or “oligo-dendrocytesis” or “oligo-dendrocyteses” or “oligodendro-cytosis” or “oligodendro-cytoses” or “oligo-dendro-cytesis” or “oligo-dendro-cyteses” or “oligo-dendro-cytosis” or “oligo-dendro-cytoses” or oligodendroblastoma* or “oligodendro-blastoma” or “oligodendro-blastomas” or “oligo-dendroblastoma” or “oligo-dendroblastomas” or “oligo-dendro-blastoma” or “oligo-dendro-blastomas” (Topic) | 5443 |
| 6 | glioblastoma* or “glio-blastoma” or “glio-blastomas” or glyoblastoma* or “glyo-blastoma” or “glyo-blastomas” or gliosarcoma* or “glio-sarcoma” or “glio-sarcomas” or glyosarcoma* or “glyo-sarcoma” or “glyo-sarcomas” (Topic) | 73747 |
| 5 | astrocytoma* or “astro-cytoma” or “astro-cytomas” or astroglioma* or “astro-glioma” or “astro-gliomas” or oligoastrocytoma* or “oligo-astrocytoma” or “oligo-astrocytomas” or “oligoastro-cytoma” or “oligoastro-cytomas” or “oligo-astro-cytoma” or “oligo-astro-cytomas” (Topic) | 21979 |
| 4 | (glia or glial) NEAR/3 (malignan* or neoplasm or neoplasms or tumor or tumors or tumour or tumours) (Topic) | 3954 |
| 3 | glioma or gliomas (Topic) | 103014 |
| 2 | cerebroma* or encephalophyma* (Topic) | 29 |
| 1 | (brain or brains or cerebral* or cerebell* or cerebri or cerebrum or intracerebral* or intra-cerebral* or intracran* or intra-cran* or midline or subtentorial or “sub-tentorial” or supratentorial or “supra-tentorial”) NEAR/3 (cancer* or malignan* or neoplasm or neoplasms or tumor or tumors or tumour or tumours) (Topic) | 108162 |
References
- Gilbert, J.A.; Blaser, M.J.; Caporaso, J.G.; Jansson, J.K.; Lynch, S.V.; Knight, R. Current understanding of the human microbiome. Nat. Med. 2018, 24, 392–400. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhang, Y. Intratumor microbiome in cancer progression: Current developments, challenges and future trends. Biomark. Res. 2022, 10, 37. [Google Scholar] [CrossRef] [PubMed]
- Jain, T.; Sharma, P.; Are, A.C.; Vickers, S.M.; Dudeja, V. New Insights Into the Cancer–Microbiome–Immune Axis: Decrypting a Decade of Discoveries. Front. Immunol. 2021, 12, 622064. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, M.H.; Sheweita, S.A.; O’Connor, P.J. Relationship between schistosomiasis and bladder cancer. Clin. Microbiol. Rev. 1999, 12, 97–111. [Google Scholar] [CrossRef]
- Lamb, A.; Chen, L.F. Role of the Helicobacter pylori-Induced inflammatory response in the development of gastric cancer. J. Cell. Biochem. 2013, 114, 491–497. [Google Scholar] [CrossRef]
- Paulos, C.M.; Wrzesinski, C.; Kaiser, A.; Hinrichs, C.S.; Chieppa, M.; Cassard, L.; Palmer, D.C.; Boni, A.; Muranski, P.; Yu, Z.; et al. Microbial translocation augments the function of adoptively transferred self/tumor-specific CD8+ T cells via TLR4 signaling. J. Clin. Investig. 2007, 117, 2197–2204. [Google Scholar] [CrossRef]
- Viaud, S.; Saccheri, F.; Mignot, G.; Yamazaki, T.; Daillère, R.; Hannani, D.; Enot, D.P.; Pfirschke, C.; Engblom, C.; Pittet, M.J.; et al. The intestinal microbiota modulates the anticancer immune effects of cyclophosphamide. Science 2013, 342, 971–976. [Google Scholar] [CrossRef]
- Vétizou, M.; Pitt, J.M.; Daillère, R.; Lepage, P.; Waldschmitt, N.; Flament, C.; Rusakiewicz, S.; Routy, B.; Roberti, M.P.; Duong, C.P.M.; et al. Anticancer immunotherapy by CTLA-4 blockade relies on the gut microbiota. Science 2015, 350, 1079–1084. [Google Scholar] [CrossRef]
- Sivan, A.; Corrales, L.; Hubert, N.; Williams, J.B.; Aquino-Michaels, K.; Earley, Z.M.; Benyamin, F.W.; Lei, Y.M.; Jabri, B.; Alegre, M.L.; et al. Commensal Bifidobacterium promotes antitumor immunity and facilitates anti-PD-L1 efficacy. Science 2015, 350, 1084–1089. [Google Scholar] [CrossRef]
- Daisley, B.A.; Chanyi, R.M.; Abdur-Rashid, K.; Al, K.F.; Gibbons, S.; Chmiel, J.A.; Wilcox, H.; Reid, G.; Anderson, A.; Dewar, M.; et al. Abiraterone acetate preferentially enriches for the gut commensal Akkermansia muciniphila in castrate-resistant prostate cancer patients. Nat. Commun. 2020, 11, 4822. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO classification of tumors of the central nervous system: A summary. Neuro-oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; Van Den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus Concomitant and Adjuvant Temozolomide for Glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [PubMed]
- Pearson, J.R.D.; Cuzzubbo, S.; McArthur, S.; Durrant, L.G.; Adhikaree, J.; Tinsley, C.J.; Pockley, A.G.; McArdle, S.E.B. Immune Escape in Glioblastoma Multiforme and the Adaptation of Immunotherapies for Treatment. Front. Immunol. 2020, 11, 582106. [Google Scholar] [CrossRef]
- Patrizz, A.; Dono, A.; Zorofchian, S.; Hines, G.; Takayasu, T.; Husein, N.; Otani, Y.; Arevalo, O.; Choi, H.A.; Savarraj, J.; et al. Glioma and temozolomide induced alterations in gut microbiome. Sci. Rep. 2020, 10, 21002. [Google Scholar] [CrossRef]
- Dono, A.; Nickles, J.; Rodriguez-Armendariz, A.G.; Mcfarland, B.C.; Ajami, N.J.; Ballester, L.Y.; Wargo, J.A.; Esquenazi, Y. Glioma and the gut-brain axis: Opportunities and future perspectives. Neuro-Oncol. Adv. 2022, 4, vdac054. [Google Scholar] [CrossRef]
- Dono, A.; Patrizz, A.; McCormack, R.M.; Putluri, N.; Ganesh, B.P.; Kaur, B.; McCullough, L.D.; Ballester, L.Y.; Esquenazi, Y. Glioma induced alterations in fecal short-chain fatty acids and neurotransmitters. CNS Oncol. 2020, 9, CNS57. [Google Scholar] [CrossRef]
- Liberati, A. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339. [Google Scholar]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef]
- D’Alessandro, G.; Antonangeli, F.; Marrocco, F.; Porzia, A.; Lauro, C.; Santoni, A.; Limatola, C. Gut microbiota alterations affect glioma growth and innate immune cells involved in tumor immunosurveillance in mice. Eur. J. Immunol. 2020, 50, 705–711. [Google Scholar] [CrossRef]
- Fan, Y.; Su, Q.; Chen, J.; Wang, Y.; He, S. Gut Microbiome Alterations Affect Glioma Development and Foxp3 Expression in Tumor Microenvironment in Mice. Front. Oncol. 2022, 12, 836953. [Google Scholar] [CrossRef]
- Herbreteau, A.; Aubert, P.; Croyal, M.; Naveilhan, P.; Billon-Crossouard, S.; Neunlist, M.; Delneste, Y.; Couez, D.; Aymeric, L. Late-Stage glioma is associated with deleterious alteration of gut bacterial metabolites in mice. Metabolites 2022, 12, 290. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, R.; Van Den Broek, T.; Carvalheiro, T.; Lammers, J.; Legemaat, M.; Quaedvlieg, M.; Van Mastrigt, E.; De Zoete, M.; Top, J.; Mueller, S.; et al. IMMU-50. DIFFERENCES IN GUT MICROBIAL COMPOSITION BETWEEN PEDIATRIC BRAIN TUMOR PATIENTS AND HEALTHY CONTROLS–THE MIMIC PROGRAM. Neuro-Oncology 2023, 25, v153–v154. [Google Scholar] [CrossRef]
- Fan, H.; Wang, Y.; Han, M.; Wang, L.; Li, X.; Kuang, X.; Du, J.; Peng, F. Multi-omics-based investigation of Bifidobacterium’s inhibitory effect on glioma: Regulation of tumor and gut microbiota, and MEK/ERK cascade. Front. Microbiol. 2024, 15, 1344284. [Google Scholar] [CrossRef]
- Hou, X.; Du, H.; Deng, Y.; Wang, H.; Liu, J.; Qiao, J.; Liu, W.; Shu, X.; Sun, B.; Liu, Y. Gut microbiota mediated the individualized efficacy of Temozolomide via immunomodulation in glioma. J. Transl. Med. 2023, 21, 198. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Zeng, W.; Zhang, X.; Pei, Y.; Zhang, H.; Li, Y. The role of gut microbiota in patients with benign and malignant brain tumors: A pilot study. Bioengineered 2022, 13, 7847–7859. [Google Scholar] [CrossRef]
- Jiang, H.; Zeng, W.; Zhang, X.; Li, Y.; Wang, Y.; Peng, A.; Cao, D. Gut microbiota and its metabolites in non-small cell lung cancer and brain metastasis: From alteration to potential microbial markers and drug targets. Front. Cell. Infect. Microbiol. 2024, 13, 1211855. [Google Scholar] [CrossRef]
- Johnson, S.; Morad, G.; Ajami, N.; Wargo, J.; Wong, M.; Lastrapes, M. The role of microbiota in metastatic brain tumors. J. Immunother. Cancer 2021, 9 (Suppl. 2), A879. [Google Scholar] [CrossRef]
- Ju, C.; Chen, Y.; Yang, L.; Huang, Y.; Liu, J. Causal relationship between gut microbiota and glioblastoma: A two-sample Mendelian randomization study. J. Cancer 2024, 15, 332–342. [Google Scholar] [CrossRef]
- Kim, H.C.; Kim, H.-J.; Lee, H.K. Gut microbiota changed by tryptophan modulates anti-tumor CTL responses against brain tumor. J. Immunol. 2023, 210 (Suppl. 1), 89.01. [Google Scholar] [CrossRef]
- Li, T.; Zhao, Z.; Peng, M.; Zhang, L.; Wang, C.; Luo, F.; Zeng, M.; Sun, K.; Fang, Z.; Luo, Y.; et al. Multi-omics analysis reveals the interplay between intratumoral bacteria and glioma. mSystems 2024, 10, e00457-24. [Google Scholar] [CrossRef]
- Li, X.C.; Wu, B.S.; Jiang, Y.; Li, J.; Wang, Z.F.; Ma, C.; Li, Y.R.; Yao, J.; Jin, X.Q.; Li, Z.Q. Temozolomide-Induced Changes in Gut Microbial Composition in a Mouse Model of Brain Glioma. Drug Des. Devel. Ther. 2021, 15, 1641–1652. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Jiang, H.; Wang, X.; Liu, X.; Huang, Y.; Wang, Z.; Ma, Q.; Dong, L.; Qi, Y.; Zhang, H.; et al. Crosstalk between the gut and brain: Importance of the fecal microbiota in patient with brain tumors. Front. Cell. Infect. Microbiol. 2022, 12, 881071. [Google Scholar] [CrossRef]
- Lu, H.; Gao, N.L.; Tong, F.; Wang, J.; Li, H.; Zhang, R.; Ma, H.; Yang, N.; Zhang, Y.; Wang, Y.; et al. Alterations of the Human Lung and Gut Microbiomes in Non-Small Cell Lung Carcinomas and Distant Metastasis. Microbiol. Spectr. 2021, 9, e0080221. [Google Scholar] [CrossRef] [PubMed]
- Meléndez-Vázquez, N.M.; Nguyen, T.T.; Fan, X.; López-Rivas, A.R.; Fueyo, J.; Gomez-Manzano, C.; Godoy-Vitorino, F. Gut microbiota composition is associated with the efficacy of Delta-24-RGDOX in malignant gliomas. Mol. Ther. Oncol. 2024, 32, 200787. [Google Scholar] [CrossRef] [PubMed]
- Morad, G.; Wong, M.C.; Fukumura, K.; Huse, J.T.; Ferguson, S.D.; Ajami, N.J.; Wargo, J.A. Abstract 2906: Retrospective analyses of sequencing datasets suggest that intratumoral microbes exist in metastatic brain tumorsRetrospective analyses of sequencing datasets suggest that intratumoral microbes exist in metastatic brain tumors. Cancer Res. 2021, 81, 2906. [Google Scholar] [CrossRef]
- Rosito, M.; Maqbool, J.; Reccagni, A.; Giampaoli, O.; Sciubba, F.; Antonangeli, F.; Scavizzi, F.; Raspa, M.; Cordella, F.; Tondo, L.; et al. Antibiotics treatment promotes vasculogenesis in the brain of glioma-bearing mice. Cell Death Dis. 2024, 15, 210. [Google Scholar] [CrossRef]
- Strong, M.J.; Blanchard, E.; Lin, Z.; Morris, C.A.; Baddoo, M.; Taylor, C.M.; Ware, M.L.; Flemington, E.K. A comprehensive next generation sequencing-based virome assessment in brain tissue suggests no major virus-tumor association. Acta Neuropathol. Commun. 2016, 4, 71. [Google Scholar] [CrossRef]
- Wang, J.; Li, H.; Tong, F.; Zeng, H.; Wei, C.; Wang, Y.; Dong, X. P63.04 Dysbiosis of Sputum and Gut Microbiota Modulate Development and Distant Metastasis of Non-Small Cell Lung Carcinomas. J. Thorac. Oncol. 2021, 16 (Suppl. 3), S553. [Google Scholar] [CrossRef]
- Wang, L.; Li, S.; Fan, H.; Han, M.; Xie, J.; Du, J.; Peng, F. Bifidobacterium lactis combined with Lactobacillus plantarum inhibit glioma growth in mice through modulating PI3K/AKT pathway and gut microbiota. Front. Microbiol. 2022, 13, 986837. [Google Scholar] [CrossRef]
- Wang, S.; Yin, F.; Guo, Z.; Li, R.; Sun, W.; Wang, Y.; Geng, Y.; Sun, C.; Sun, D. Association between gut microbiota and glioblastoma: A Mendelian randomization study. Front. Genet. 2024, 14, 1308263. [Google Scholar] [CrossRef]
- Wen, Y.; Feng, L.; Wang, H.; Zhou, H.; Li, Q.; Zhang, W.; Wang, M.; Li, Y.; Luan, X.; Jiang, Z.; et al. Association Between Oral Microbiota and Human Brain Glioma Grade: A Case-Control Study. Front. Microbiol. 2021, 12, 746568. [Google Scholar] [CrossRef]
- Yang, J.; Moon, H.E.; Park, H.W.; McDowell, A.; Shin, T.S.; Jee, Y.K.; Kym, S.; Paek, S.H.; Kim, Y.K. Brain tumor diagnostic model and dietary effect based on extracellular vesicle microbiome data in serum. Exp. Mol. Med. 2020, 52, 1602–1613. [Google Scholar] [CrossRef] [PubMed]
- Zeng, C.; Zhang, C.; He, C.; Song, H. Investigating the causal impact of gut microbiota on glioblastoma: A bidirectional Mendelian randomization study. BMC Genom. 2023, 24, 784. [Google Scholar] [CrossRef]
- Zhou, M.; Song, C.; Gu, J.; Wang, T.; Shi, L.; Li, C.; Zhu, L.; Li, H.; Qi, S.; Lu, Y. Novel gut microbiota and microbiota-metabolites signatures in gliomas and its predictive/prognosis functions. bioRxiv 2023. [Google Scholar] [CrossRef]
- Li, H.; Wang, J.; Zeng, H.; Bin, Y.; Tong, F.; Dong, X. FP07.01 Dysbiosis of Gut Microbiota Suppress the Brain Metastasis of Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2021, 16 (Suppl. 3), S203. [Google Scholar] [CrossRef]
- Morad, G.; Lastrapes, M.; Wong, M.; Sahasrabhojane, P.; Ferguson, S.; Ajami, N.; Wargo, J. Distinct oral microbial signatures are associated with primary and metastatic brain tumors. Cancer Res. Conf. Am. Assoc. Cancer Res. Annu. Meet. ACCR 2020, 82, 3045. [Google Scholar] [CrossRef]
- Dees, K.J.; Koo, H.; Humphreys, J.F.; Hakim, J.A.; Crossman, D.K.; Crowley, M.R.; Nabors, L.B.; Benveniste, E.N.; Morrow, C.D.; McFarland, B.C. Human gut microbial communities dictate efficacy of anti-PD-1 therapy in a humanized microbiome mouse model of glioma. Neuro-Oncol. Adv. 2021, 3, vdab023. [Google Scholar] [CrossRef]
- De Cecco, L.; Biassoni, V.; Schiavello, E.; Carenzo, A.; Ianno, M.F.; Licata, A.; Marra, M.; Carollo, M.; Boschetti, L.; Massimino, M. The brain-gut-microbiota axis to predict outcome in pediatric diffuse intrinsic pontine glioma. Neuro-Oncology 2022, 24 (Suppl. 1), i26. [Google Scholar] [CrossRef]
- Gomez-Manzano, C.; Melendez-Vazquez, N.M.; Nguyen, T.; Ossimetha, A.; Jiang, H.; Fueyo, J.; Godoy-Vitorino, F. Abstract 927: Gut microbiome changes are associated with the efficacy of Delta-24-RGDOX viroimmunotherapy against malignant glioma. Cancer Res. 2021, 81, 927. [Google Scholar] [CrossRef]
- Ladomersky, E.; Zhai, L.; Lauing, K.; Qian, J.; Bell, A.; Otto-Meyer, S.; Savoor, R.; Wainwright, D. Modulating dietary tryptophan or gut microbiota levels does not improve the efficacy of combined treatment with radiation, anti-PD-1 mab, and an IDO1 enzyme inhibitor in a model of glioblastoma. Neuro-Oncology 2019, 21 (Suppl. 6), vi40. [Google Scholar] [CrossRef]
- Weathers, S.P.S.; Zhu, H.; Knafl, M.; Damania, A.; Kamiya-Matsuoka, C.; Harrison, R.A.; Lyons, L.; Yun, C.; Darbonne, W.C.; Loghin, M.; et al. Baseline tumor genomic and gut microbiota association with clinical outcomes in newly diagnosed glioblastoma (GBM) treated with atezolizumab in combination with temozolomide (TMZ) and radiation. JCO 2022, 40, 16. [Google Scholar] [CrossRef]
- Zhu, J.; Su, J. Alterations of the Gut Microbiome in Recurrent Malignant Gliomas Patients Received Bevacizumab and Temozolomide Combination Treatment and Temozolomide Monotherapy. Indian J. Microbiol. 2022, 62, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Sarvesh, S.; Valbak, O.; Backan, O.; Chen, D.; Morrow, C.; Benvensite, E.; Nabors, B.; Bekal, M.; Dono, A.; et al. MODL-06. THE GUT MICROBIOTA OF BRAIN TUMOR PATIENTS CAN IMPACT IMMUNOTHERAPY EFFICACY IN A PRECLINICAL MODEL OF GLIOMA. Neuro-Oncology 2023, 25, v299. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.; La, J.; Park, W.H.; Kim, H.-J.; Park, S.H.; Ku, K.B.; Kang, B.H.; Lim, J.; Kwon, M.S.; et al. Supplementation with a high-glucose drink stimulates anti-tumor immune responses to glioblastoma via gut microbiota modulation. Cell Rep. 2023, 42, 113220. [Google Scholar] [CrossRef] [PubMed]
- Dees, K.; Koo, H.; Humphreys, J.; Hakim, J.; Crossman, D.; Crowley, M.; Nabors, L.B.; Benveniste, E.; Morrow, C.; McFarland, B. Human microbiota influence the efficacy of immunotherapy in a mouse model of glioblastoma. Neuro-Oncology 2021, 23 (Suppl. 6), vi93–vi94. [Google Scholar] [CrossRef]
- McFarland, B.; Dees, K.; Melo, N.; Fehling, S.; Gibson, S.; Yan, Z.Q.; Kumar, R.; Morrow, C.; Benveniste, E. THERAPEUTIC BENEFIT OF A KETOGENIC DIET THROUGH ALTERED GUT MICROBIOTA IN A MOUSE MODEL OF GLIOMA. Neuro-Oncology 2017, 19, 78. [Google Scholar] [CrossRef]
- Wong, C.C.; Yu, J. Gut microbiota in colorectal cancer development and therapy. Nat. Rev. Clin. Oncol. 2023, 20, 429–452. [Google Scholar] [CrossRef]
- Magne, F.; Gotteland, M.; Gauthier, L.; Zazueta, A.; Pesoa, S.; Navarrete, P.; Balamurugan, R. The Firmicutes/Bacteroidetes Ratio: A Relevant Marker of Gut Dysbiosis in Obese Patients? Nutrients 2020, 12, 1474. [Google Scholar] [CrossRef]
- Ma, Q.; Xing, C.; Long, W.; Wang, H.Y.; Liu, Q.; Wang, R.-F. Impact of microbiota on central nervous system and neurological diseases: The gut-brain axis. J. Neuroinflamm. 2019, 16, 53. [Google Scholar] [CrossRef]
- Routy, B.; Le Chatelier, E.; Derosa, L.; Duong, C.P.M.; Alou, M.T.; Daillère, R.; Fluckiger, A.; Messaoudene, M.; Rauber, C.; Roberti, M.P.; et al. Gut microbiome influences efficacy of PD-1–based immunotherapy against epithelial tumors. Science 2018, 359, 91–97. [Google Scholar] [CrossRef]
- Routy, B.; Lenehan, J.G.; Miller, W.H.; Jamal, R.; Messaoudene, M.; Daisley, B.A.; Hes, C.; Al, K.F.; Martinez-Gili, L.; Punčochář, M.; et al. Fecal microbiota transplantation plus anti-PD-1 immunotherapy in advanced melanoma: A phase I trial. Nat. Med. 2023, 29, 2121–2132. [Google Scholar] [CrossRef]

{kind=link}
| Primary Author | Year | Country | Type of Study | Type of Publication | Human Involvement (Y/N) | Mouse Involvement (Y/N) | Type of Brain Tumor | Microbiome Source | Objective |
|---|---|---|---|---|---|---|---|---|---|
| D’Alessandro G | 2020 | Italy | Case–Control | Article | N | Y | Glioma | Cecum | Investigate the impact of gut microbiome alterations on glioma growth |
| Herbreteau A | 2022 | France | Case–Control | Article | N | Y | Glioma | Cecum | Investigate the impact of glioma development on GI function and microbiota |
| De Cecco L | 2022 | Italy | Cohort | Abstract | Y | N | DIPG | Feces | Determine gut microbiota in DIPG before and after radiotherapy |
| Dees K | 2021 | USA | Cohort | Article | N | Y | GBM | Feces | Determine the effect of microbial communities on glioma growth and immunotherapy response in a human mouse microbiome model |
| Dono A | 2020 | USA | Cohort | Article | Y | Y | GBM and diffuse astrocytoma | Feces | Explore the role of fecal short chain fatty acids in glioma growth |
| Fan H | 2024 | China | Cohort | Article | N | Y | Glioma | Feces | Investigate the impact of Bifidobacterium on glioma growth |
| Fan Y | 2022 | China | Cohort | Article | N | Y | Glioma | Feces | Investigate the effects of glioma growth on gut microbiome, and impact of gut dysbiosis on glioma development |
| Gomez-Manzano C | 2021 | USA | Case–Control | Abstract | N | Y | Glioma | Feces | Evaluate the changes in gut microbiome after treatment with viroimmunotherapy |
| Hermida LC | 2021 | USA | Cohort | Abstract | N | N | Low grade glioma | Tumor | Investigate whether can use a tumor’s microbial abundances to predict clinical outcomes and drug response |
| Hoogendijk R | 2023 | Netherlands | Case–Control | Abstract | Y | N | High grade glioma | Feces | Compare the gut microbiome composition in pediatric patients with high grade brain tumors compared to healthy controls |
| Hou X | 2023 | USA | Case–Control | Article | N | Y | Glioma | Feces | Reveal the potential role of gut microbiota in glioma development and individualized efficacy of TMZ using integrated microbiomics and metabolomics analysis |
| Jiang H | 2022 | China | Case–Control | Article | Y | N | Glioma and meningioma | Feces | Investigate the correlation between gut microbiota and benign and malignant brain tumors |
| Jiang H | 2023 | China | Case–Control | Article | Y | N | Brain Metastasis | Feces | Investigate the relationship between the microbiome and its metabolites in NSCLC, included subgroup of brain metastasis |
| Johnson S | 2021 | USA | Cohort | Abstract | Y | y | Brain Metastasis | Feces and oral | Explore the role of microbiota in brain metastases development |
| Ju C | 2024 | China | Mendelian randomization | Article | N | N | GBM | N/A | Analyze the causal association between gut microbiota and glioblastoma multiforme (GBM) using Mendelian randomization |
| Kim D | 2024 | USA | Case–Control | Abstract | N | Y | Brain Metastasis and GBM | Feces | Investigate whether the gut microbiome can influence immunotherapy response for GBM |
| Kim H | 2023 | South Korea | Case–Control | Abstract | N | Y | GBM | Not reported | Evaluate how the gut microbiome influences GBM |
| Kim J | 2023 | South Korea | Case–Control | Article | N | Y | GBM | Feces | Determine the effects of short-term supplementation with a high-glucose drink (HGD) on GBM growth and the anti-tumor immune response in mice |
| Ladomersky E | 2019 | USA | Cohort | Abstract | N | Y | GBM | N/A | Explore the impact of microbiome depletion on immunotherapy efficacy |
| Li H | 2021 | China | Case–Control | Abstract | Y | Y | Brain Metastasis | Feces | Explore the impact of gut microbiome on brain metastasis development in NSCLC |
| Li T | 2023 | China | Cohort | Abstract | Y | Y | Glioma | Brain Tissue | Investigate the microbial community composition in glioma tissues and elucidate its role in glioma development |
| Li X | 2021 | China | Cohort | Article | N | Y | Glioma | Feces | Explore gut microbiome alterations during glioma growth |
| Li Y | 2022 | China | Case–Control | Article | Y | N | Benign and Malignant Brain Tumors | Feces | Examine alterations in gut microbiota in patients with brain tumors |
| Lu H | 2021 | China | Case–Control | Article | Y | N | Brain Metastasis | Sputum and Feces | Explore microbiome profiles in patients with NSCLC |
| McFarland B | 2017 | USA | Case–Control | Abstract | N | Y | Glioma | Gut | Determine if ketogenic diet is an effective treatment for glioma, and correlate this with gut microbiota changes |
| Melendez-Vazquez N | 2024 | USA | Case–Control | Article | N | Y | GBM | Feces | Assess whether gut bacterial signatures are associated with oncolytic viral therapy efficacy |
| Morad G | 2022 | USA | Case–Control | Abstract | Y | N | Primary Brain Tumor and Brain Metastasis | N/A | Identify oral and gut microbiome signatures in primary brain tumors and brain metastasis |
| Morad G | 2021 | USA | Case–Control | Abstract | Y | N | Brain Metastasis | Feces, sputum and buccal | Evaluate the impact of microbiome depletion on melanoma brain metastasis growth |
| Patrizz A | 2020 | USA | Case–Control | Article | Y | Y | Glioma | Feces | Identify gut microbiota changes in glioma growth and in response to temozolomide |
| Rosito M | 2024 | Italy | Case–Control | Article | N | Y | Glioma | N/A | Investigate the role of dysbiosis induced by the administration of non-absorbable antibiotics on mouse metabolome and on tumor microenvironment |
| Strong M | 2016 | USA | Cohort | Article | N | N | GBM | Tumor | Identify the relationship between GBM and human cytomegalovirus |
| Wang J | 2021 | China | Case–Control | Abstract | Y | Y | Brain Metastasis | Feces and sputum | Investigate the role of the microbiome on metastatic NSCLC |
| Wang L | 2022 | China | Case–Control | Article | N | Y | Glioma | Feces | Investigate the impact of probiotic strains on glioma growth |
| Wang S | 2024 | China | Mendelian Randomization | Article | N | N | GBM | N/A | Analyze the causal association between gut microbiota and glioblastoma multiforme (GBM) using Mendelian randomization |
| Weathers S | 2022 | USA | Cohort | Abstract | Y | N | GBM | Feces | Identify factors that predict response to atezolizumab, temozolomide and radiation |
| Wen Y | 2021 | China | Case–Control | Article | Y | N | Glioma | Saliva | Investigate the relationship between oral microbiota and glioma grade |
| Yang J | 2020 | South Korea | Case–Control | Article | Y | Y | Primary Brain Tumor | Serum | Determine the predictive model for brain tumors based on microbiome signatures and extracellular vesicles |
| Zeng C | 2023 | China | Mendelian Randomization | Article | N | N | GBM | N/A | Uncover the causal relationship between glioblastoma and the gut microbiome using Mendelian randomization analysis |
| Zhou M | 2023 | China | Case–Control | Abstract | Y | N | Glioma | Feces | Profile the gut microbiome and metabolome in fecal samples from healthy volunteers and compare to those with gliomas |
| Zhou J | 2022 | China | Case–Control | Article | Y | N | Glioma | Feces | Investigate gut microbiota in recurrent glioma on bevacizumab and /or temozolomide |
| Author | Year | Brain Tumor Type | Population | Study Design | Impact on Glioma Growth or Development |
|---|---|---|---|---|---|
| D’Alessandro, G | 2020 | Glioma | Mice | -Glioma mouse model was treated with five weeks of antibiotics | -Tumor volume increased in mice treated with oral vancomycin and gentamicin -Interruption of antibiotic treatment decreased tumor size -In antibiotic treated mice, increased abundance of Burkholderiales families, and decreased Prevotellaceae, Rikenellacaea, and Helicobacteracae families |
| Dono, A | 2020 | Glioma | Mice and humans (n = 10 glioma, n = 6 control) | -Mice implanted with glioma cells and given TMZ or placebo -Fecal sample collected from humans prior to surgical resection and analyzed | -Glioma development alters the short chain fatty acids excreted by mice -Abundance of Bacteroides increased after tumor development. Akkermansia and Verrucomicrobia also increased -In humans, there was no difference between bacterial alpha and beta diversity and taxa abundance in glioma vs. healthy control using 16s rRNA sequencing |
| Fan H | 2024 | Glioma | Mice (n = 26) | -Mice implanted with glioma cells received intragastric gavage of a Bifidobacterium mixture. T2-weighted MRI used to evaluate tumor volume, tumor and fecal samples collected to examine microbiome | -Administration of Bifidobacterium mixture increased median survival in mice with glioma from 42 days to 52 days, p < 0.05. No significant difference in hepatic or renal toxicity -Bifidobacterium mixture resulted in significant increase in both the Shannon and Simpson indices, p < 0.01 when assessing the tumor tissue microbiome -Bifidobacterium mixture did not affect the alpha-diversity of the gut microbiota. At the phylum level, the group receiving this mixture had higher levels of gut Actinobacteriota and lower levels of Myxococcota, p < 0.05 |
| Herbreteau, A | 2022 | Glioma | Mice | -Mice injected with glioma cells and given antibiotics daily -Cecum harvested on day 16 and contents analyzed | -Concentration of bacterial metabolites (short-chain fatty acids) was reduced in the cecum of glioma mice -Antibiotic treatment did not change tumor size, but changed frequency of myeloid cells in tumor environment |
| Hoogendijk R | 2023 | High grade glioma | Humans (n = 33 pediatric high-grade glioma, n = 26 controls) | -Prospectively collected fecal samples from patients at diagnosis and analyzed the microbial composition | -Comparable alpha-diversity between the groups (Shannon-index p = 0.45), but significant beta-diversity (Permanova test p = 0.02) |
| Hou X | 2023 | Glioma | Mice | -Implanted glioma cells into mice and gave one group TMZ (50 mg/kg). Fecal and tumor tissue samples collected -Broad spectrum antibiotics were given to part of the TMZ group to confirm the role of the gut microbiome on TMZ sensitivity | -Gut bacteria composition significantly changed during both glioma development and TMZ treatment -Alpha diversity indexes did not significantly change during glioma development; however, beta-diversity was different between control and glioma mice, suggesting that dysbiosis is induced by glioma development -Bacteroides was the most dominant phylum in the glioma group, versus Bacillota in the control group |
| Fan, Y | 2022 | Glioma | Mice | -Mice were injected with glioma cells and then treated with antibiotics or not. A third group was randomized to fecal transplant or not | -Abundance of Bacteroidia and Actinobacteria decreased, and Bacillota (formerly Firmicutes) increased during glioma growth with resultant increased F/B ratio -Tumor growth significantly worsened in mice treated with antibiotics versus those not |
| Jiang, H | 2022 | Meningioma and Malignant Glioma | Humans (n = 32 meningioma, n = 27 glioma, n = 41 control) | -Collected fecal specimen of patients with newly diagnosed brain tumor within 6 h of admission -Compared to healthy controls | -In the meningioma group, most common gut microbes at phylum level: Bacteroidetes, Bacillota, Proteobacteria, Actinobacteria, Fusobacteria, and Verrucomicrobiota -In the glioma group, most common at phylum level: Bacteroidetes, Bacillota, Proteobacteria, Fusobacteria, Verrucomicrobiota, Actinobacteria -In the healthy control group, most common at phylum level included Firmictutes, Bacteroidetes, Proteobacteria, Actinobacteria, Verrucomicrobiota, Fusobacteria -Alpha diversity indices all reduced in brain tumor groups compared to control |
| Jiang H | 2023 | Brain Metastasis | Humans (n = 40 brain metastasis, n = 35 healthy controls) | -Collected fecal samples from healthy controls and treatment naïve patients with metastatic NSCLC with brain metastasis, and characterized the intestinal microbiome and fecal short-chain fatty acid (SCFA) levels, which are produced by the gut microbiota | -Alpha diversity less abundant in patients with NSCLC with brain metastasis compared to healthy controls -Significant difference in beta diversity between groups -Increase in pathogens in Fusobacteria and Proteobacteria and a decrease in SCFA-producing bacteria in Bacillota and Actinobacteria, particularly in the BM stage |
| Johnson, S | 2021 | Brain metastasis | Humans (number not reported) and Mice | -Depleted gut microbiota in mice and injected melanoma cells intracranially -Evaluated tumor growth, and gut and oral microbial signatures | -Distinct enrichment pattern of bacterial and viral taxa within gut and oral microbiota in brain metastasis patients -Gut microbiome depletion decreased tumor growth in mice |
| Ju C | 2024 | GBM | Human dataset | -Took two datasets from genome-wide association studies and utilized mendelian randomization to determine causal relationship between gut microbiota and GBM | -Family Ruminococcaceae was shown to be protective against glioblastoma -An increase in the two microbial families, Bacteroidaceae and Peptococcaceae were associated with a high risk of GBM development -An increase in four microbial genera, Eubacterium, Actinomyces, Bacteroides, and Ruminiclostridium6, were found to be associated with an increased risk of GBM |
| Kim, H | 2023 | GBM | Mice | -Examined gut microbiome composition in mice with GBM | -Observed a distinct change in gut microbial composition and metabolism during GBM progression -Found that tryptophan levels significantly reduced in GBM mice, and thus supplemented diet with tryptophan and found it improved survival in a commensal microbiota-dependent manner |
| Li, H | 2021 | Brain Metastasis | Humans (n = 60 brain metastasis, n = 25 without brain metastasis) and Mice | -Collected fecal samples from patients with NSCLC with or without brain metastasis -Utilized mouse glioma model and gave one group antibiotics | -No differences in microbial diversity between samples from patients with and without brain metastases -Blautia genus decreased in brain metastasis -Antibiotics reduced tumor burden in mice, and was associated with increased microglia cells |
| Li, T | 2023 | Glioma | Humans (n = 50) and mice | -Took tumor tissue and adjacent normal brain tissue from glioma patients and performed microbial profiling, transcriptome sequencing, and metabolomics -Then, took six genera of bacteria found to be enriched in glioma tissue and developed an animal model to validate their impact on glioma growth | -Found six genera were enriched in tumor tissue (Fusobacterium, Longibaculum, Intestinimonas, Pasteurella, Limosilactobacillus, and Arthrobacter) -In vivo and in vitro models of glioma demonstrated that Fusobacterium nucleatum promotes glioma proliferation and upregulates CCL2, CXCL1, and CXCL2 |
| Li, X | 2021 | Glioma | Mice | -Implanted mice with glioma cells and treated with TMZ for five days vs. placebo -Collected fecal samples day 0, 7, 14, 28 post-tumor implant | -Abundance of Lactobacillus decreased, and Intestinimonas and Anaerotruncus increased in mice with glioma compared to naïve before glioma cell implantation -With 7 days of TMZ treatment, at the phylum level there was increase in Verrucomicrobia compared to control; however, no change in alpha-diversity between groups -At the end of TMZ treatment, there was a significant difference in 20 genera between groups |
| Li, Y | 2022 | Benign and Malignant Primary Brain Tumors | Humans (n = 101 brain tumors, n = 57 healthy control) | -Included patients with benign and malignant brain tumors and healthy controls, collected fecal samples 2 h post hospital admission | -Gut microbial alpha diversity lower in brain tumor patients -Brain tumor cohort had higher levels of Bacteroidetes, Fusobacteria, and Proteobacteria, and lower Bacillota and Actinobacteria -Decreased F/B ratio in brain tumor group -Fusobacterium, Enterobacteriaceae and Escherichia/Shigella were all overexpressed in brain tumor patients -Parasutterella, Bifidobacterium and Lachnospira all enriched in healthy controls |
| Lu, H | 2021 | Brain Metastasis | Humans (n = 87 NSCLC, n = 34 healthy controls) | -Collected sputum and stool samples from patients with NSCLC and healthy controls | -Alpha-diversity in the gut lower in healthy control group -Different beta-diversities in sputum but not in feces in those with brain metastasis vs. NSCLC without brain metastasis -Pseudomonas was abundant in sputum and feces of brain metastasis patients, and not detectable in those without |
| Melendez-Vazquez, N | 2024 | GBM | Mice | -Created a GBM bearing mouse line and treated with either oral indoximod, Delta-24-RGDOX by intratumoral injection, or placebo. Also compared to tumor free (naïve) mouse group. -Collected fecal samples and examined bacterial composition and diversity associated with therapy | -Prominent differences in bacterial diversity between naïve and PBS treated mice, highlighting that tumor presence is associated with gut biota changes |
| Morad, G | 2022 | Primary and Metastatic Brain Tumors | Humans (n = 10 per tumor type) | -Collected stool, saliva, and buccal samples from patients with primary or metastatic brain tumors | -Distinct bacterial and viral signatures enriched in metastatic brain tumors compared to primary brain tumors |
| Patrizz, A | 2020 | Glioma | Mice and humans (n = 53) | -Implanted glioma cells into mice -Collected fecal samples prior to tumor implant, before and after TMZ or placebo -Collected stool samples from patients with glioma at diagnosis, before and after chemoradiation | -A significant decrease in the Bacillota to Bacteroides (F/B) ratio in mice suggesting dysbiosis following tumor-growth -Bacillota decreased and Verrucomicrobia phyla increased with tumor growth in mice -No difference in alpha diversity indices between controls, IDH wild-type, or IDH mutant patients at baseline -There was significant difference in F/B ratio between IDH wild-type and mutant patients compared to controls -Marked differences were observed at the phylum level in IDH-WT patients compared to controls, with increased Bacteroidetes, Proteobacteria, and Verrucomicrobia |
| Rosito M | 2024 | Glioma | Mice | -Treated one mouse group with oral vancomycin and gentamicin for two weeks and then transplanted glioma wells. The comparator glioma group was not treated with antibiotics. | -Found that there was a significant increase in tumor volume in antibiotic treated mice compare to mice not treated with antibiotics -Antibiotic treated mice had increased expression of CD34+ vessel like structures, suggestive of increased vasculogenesis |
| Strong, M | 2016 | GBM and LGG | Humans (n-170 GBM, n = 531 LGG) | -Utilized publicly available sequencing datasets from the Cancer Genome Atlas and whole genome datasets and normal matched blood samples -Obtained and analyzed three primary GBM tissue samples -Performed comprehensive virome assessment in both | -HPV and Hepatitis B detected in some LGG samples (4 and 1, respectively) -Concluded that likely no association between viruses and GBM development |
| Wang, J | 2021 | Brain metastasis | Mice and humans (n-87 NSCLC, n = 34 healthy volunteers) | -Treated mice with antibiotics for 2 weeks before injecting with lung cancer cells -Collected sputum and fecal samples from patients with NSCLC and healthy controls | -Pseudomonas aeruginosa was associated with brain metastasis |
| Wang, L | 2022 | Glioma | Mice | -Mice were treated with different probiotic cocktails and then injected with glioma cells. Fecal and tissue samples collected | -Tumor growth declined in mice treated with Bifidobacterium lactus and Lactiplantibacillus plantarum -This impact was found to be through the PI3K/AKT pathway |
| Wang S | 2024 | GBM | Human dataset | -Took a human gut microbiota dataset and utilized mendelian randomization to analyze the causal association between gut microbiota and GBM | -Found that the family Peptostreptococcaceae and genus Eubacterium brachy group were associated with increased risk of GBM -Family Ruminococcaceae, genus. Anaerostipes, genus. Faecalibacterium, genus. LachnospiraceaeUCG004, genus. Phascolartobacterium, genus. Prevotella7, and genus. Streptococcus were associated with reduced risk of GBM -Found family Ruminococcaceae to be protective against GBM (OR = 0.04, 95% CI 0.01–0.19) |
| Wen, Y | 2021 | HGG and LGG | Humans (n = 23 HGG, n = 12 LGG, n = 24 controls) | -Collected saliva samples from patients with HGG, LGG and healthy controls | -HGG was associated with a shift in oral microbiota beta-diversity -Genera Capnocythophaga and Leptotrichia were associated with glioma grade -Genera Bergeyella and Capnocytophaga were correlated with IDH1 mutation in glioma -The oral microbial features (Capnocythophaga Porphyromonas, Haemophilus Leptotrichia, and TM7x) discriminated HGG from LGG |
| Yang, J | 2020 | Glioma and Metastatic Brain Tumor | Mice and humans (n = 152 brain tumor patients, n = 198 control) | -Extracted extracellular (EV) vesicles that are produced by bacteria from serum of brain tumor patients and healthy controls, and glioma mouse model tissues -Then, created diagnostic models using the EV data | -Alpha diversity and beta diversity of the serum EV microbiome differed between brain tumor group and healthy controls -Bacillota abundance was lower in control group, and Actinobacteria and Proteobacteria were higher |
| Zeng C | 2023 | GBM | Human dataset | -Took a human gut microbiota dataset and utilized mendelian randomization to analyze the causal association between gut microbiota and GBM | -Eubacterium brachy group, Eubacterium ruminantium group, Prevotella7, and Peptostreptococcaceae were confirmed in two Mendelian Randomization methods to exhibit causality with GBM -Ruminococcaceae demonstrated causality with GBM in three distinct Mendelian Randomization methods |
| Zhou M | 2023 | Glioma | Humans (n = 78 glioma patients, n = 37 healthy controls) | -Collected fecal samples from healthy controls and patients with glioma, and profiled the gut microbiome and metabolome |
-Found 56 discriminatory operational taxonomic units and 144 metabolites in samples from patients with gliomas compared to control -Patients with higher proportion of fecal Faecalibacterium had significantly better median PFS (495 d vs. 281 d, p = 0.005) and median OS (604 d vs. 395 d, p = 0.044) |
| Author | Year | Brain Tumor Type | Population | Study Design | Treatments Included | Impact on Treatment |
|---|---|---|---|---|---|---|
| Dees K | 2021 | Glioma | Mice | -Generated five colonies of mice transplanted with different gut microbiomes transplanted from human donors; injected them with glioma cells -Mice randomized to receipt of anti-PD-1, TMZ, or placebo | Anti-PD-1 or TMZ | -Anti-PD-1 improved survival in 2/5 strains of mice -Increased CD8+/Treg ratio in responder strains -Responder mice colonies had high levels of Bacteroides cellulosilyticus and most similar gut microbiomes -TMZ improved survival in all five strains |
| De Cecco L | 2022 | DIPG | Humans (n = 18) | -Collected fecal samples in children with DIPG before and after RT | RT | -Flavobacteriaceae and Bacillales associated with increased risk of disease progression -Synergistaceae was associated with decreased risk of progression -F/B ratio changed with RT, however the direction in which is not reported |
| Dono A | 2020 | Glioma | Mice and Humans (n = 15) | -Mice implanted with glioma cells and given TMZ or placebo -Fecal sample collected from humans prior to surgical resection and analyzed | TMZ vs. placebo | -TMZ increased three fecal metabolites (acetylcholine, 3-methyl valerate, caproate) and decreased histamine -No difference in gut alpha diversity OTU or Shannon Diversity Index before and after TMZ -TMZ diminished the microbiome changes seen with glioma growth |
| Gomez-Manzano C | 2021 | Glioma | Mice | -Mice injected with Delta-24-RGDOX or saline Used immunocompetent and CD4+ depleted mouse strains | Delta-24-RGDOX vs. placebo | -Mice with intact T cells treated with therapy had increased Actinobacteria compared to control mice -Bifidobacterium and Lactobacillus associated with better response to therapy -No difference in fungal species, which was dominated by Ascomycota |
| Hou X | 2023 | Glioma | Mice | -Implanted glioma cells into mice and gave one group TMZ (50 mg/kg). Fecal and tumor tissue samples collected -Broad spectrum antibiotics were given to part of the TMZ group to confirm the role of the gut microbiome on TMZ sensitivity | TMZ | -Gut bacteria composition significantly changed during both glioma development and TMZ treatment -Alpha diversity indexes did not significantly change during glioma development; however, beta-diversity was different between control and glioma mice, suggesting that dysbiosis is induced by glioma development. -Bacteroides was the most dominant phylum in the glioma group, versus Bacillota in the control group -Treatment with TMZ reversed the gut microbiome dysbiosis that was induced by glioma. It let to significantly increased alpha diversity indexes (Shannon and Simpson), suggesting elevated microbial community richness and diversity. -At the phylum level, TMZ treated mice were dominated by Firmictutes, versus Bacteroides for the non-TMZ group |
| Kim D | 2024 | Brain Metastasis and GBM | Mice | -Obtained fecal samples from GBM and melanoma brain metastases (MBM) patients prior to any treatment and transplanted these microbiome samples into mice. These mice were then injected with glioma cells | Anti-PD-1 | -Two strains of mice (one MBM and one GBM strain) were resistant to anti-PD-1 whereas the other two strains responded and showed prolonged survival compared to control -Ongoing microbiome sequencing underway to identify microbiome profiles of each strain |
| Kim J | 2023 | GBM | Mice | -Developed a GBM mouse model and provided them with a high glucose drink (HGD) versus a control of normal drinking water. Treated with anti-PD-1, and then tried to augment response with administration of probiotics | Anti-PD-1 | -Found no effect of anti-PD1 on their mouse model. Tried to augment this with probiotic administration and found none had a significant impact on survival |
| Ladomersky E | 2019 | GBM | Mice | -Engrafted mice with glioma cells -Fed mice tryptophan and gave one set antibiotics to deplete microbiome | RT and/or anti-PD-1 | -Depletion of gut microbiome had no effect on therapeutic efficacy |
| Li X | 2021 | Glioma | Mice | -Implanted mice with glioma cells and treated with TMZ for five days -Collected fecal samples day 0, 7,14,28 post tumor implant | TMZ vs. placebo | -Abundance of Lactobacillus decreased, and Intestinimonas and Anaerotruncus increased in mice with glioma compared to naïve -TMZ increased abundance of Verrucomicrobia at the phyla level, and of Akkermansia, Bifidobacterium, Coprobacillus and Clostridium_XVIII at the genus level in the first 7 days -At 21 days, TMZ increased abundance of Anaerotruncus genus as well as overall community diversity |
| Melendez-Vazquez, N | 2024 | GBM | Mice | -Created a GBM bearing mouse line and treated with either oral indoximod, Delta-24-RGDOX by intratumoral injection, or placebo. Also compared to tumor free (naïve) mouse group -Collected fecal samples and examined bacterial composition and diversity associated with therapy | Delta-24-RGDOX (a novel oncolytic adenovirus) | -Increased survival in those treated with Delta-24-RGDOX compared to indoximod or PBS (168 d vs. 53.4 d vs. 51.3 d, respectively) -Distinct gut microbiome composition in those treated with Delta-24-RGDOX versus placebo (p = 0.007) -Similar alpha-diversity levels between indoximod, Delta-24-RDGOX, and naïve group, suggesting that both immunomodulators modify diversity to be similar to the healthy naïve group -Indoximod and Delta-24-RGDOX treated mice had reduced F/B ratio, similar to naïve mice. Placebo treated mice with brain tumor had higher F/B ratio. This suggests that the immunomodulators contribute to reversal of tumor associated dysbiosis |
| Patrizz A | 2020 | Glioma | Mice and humans (n = 53) | -Implanted glioma cells into mice -Collected fecal samples prior to tumor implant, before and after TMZ or placebo -Collected stool samples from patients with glioma at diagnosis, before and after chemoradiation | TMZ | -TMZ prevented the decrease in F/B ratio therefore preventing glioma induced dysbiosis -F/B ratio differed between IDH-WT AND IDH-Mut patients. WT had increased Bacteroidetes, Proteobacteria, and Verrucomicrobia -No difference in F/B ratio in humans post treatment with TMZ compared to before treatment with TMZ |
| Weathers S | 2022 | GBM | Humans (n = 60) | -Collected baseline fecal samples in patients newly diagnosed with GBM -Assessed OS and PFS | Concurrent radiation, atezolizumab and TMZ, followed by atezolizumab and TMZ | -One distinct taxa (Ruminococcus species) were associated with OS -One distinct taxa (Eubacterium species) were associated with response to treatment |
| Zhou J | 2022 | WHO grade III/IV glioma | Humans (n = 29, 15 TMZ + Bev, 14 TMZ) | -Randomized patients to Bevacizumab + TMZ vs. TMZ alone, and collected fecal samples post treatment | Bevacizumab + TMZ (Group 1) versus TMZ alone (Group 2) | -Significant difference in beta-diversity of microbiome between groups -Group 1 had higher levels of Actinobacteria, Bacillota and Bacteroidetes |
| Author | Year | Brain Tumor Type | Population | Study Design | Impact on Glioma Growth or Development |
|---|---|---|---|---|---|
| Kim H | 2023 | GBM | Mice | -Developed a GBM mouse model and looked at gut microbial composition and metabolism. Then, supplemented tryptophan to diet of these mice | -Found that dietary supplementation of tryptophan to GBM mice improved survival in a commensal microbiota-dependent manner |
| Kim J | 2023 | GBM | Mice | -Developed a GBM mouse model and provided them with a high glucose drink (HGD) versus a control of normal drinking water | -Found that starting HGD supplementation 5 weeks before tumor cell inoculation improved survival, versus starting after inoculation did not change outcomes. When they tried this in a germ-free mouse model, there was no difference in survival |
| McFarland B | 2017 | Glioma | Mice | -Utilized a glioma mouse model and fed them a ketogenic versus normal diet, and then compared gut microbiome between the two as well as glioma related outcomes | -Mice fed ketogenic diet had slightly increased survival compared to mice fed a normal diet -Some long-term survivors on the ketogenic diet had significant increase in gut Faecalibaculum rodentium |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leigh, J.; Skidmore, B.; Wong, A.; Maleki Vareki, S.; Ng, T.L. Exploring the Microbiome’s Impact on Glioma and Brain Metastases: Insights into Development, Progression, and Treatment Response—A Scoping Review. Cancers 2025, 17, 1228. https://doi.org/10.3390/cancers17071228
Leigh J, Skidmore B, Wong A, Maleki Vareki S, Ng TL. Exploring the Microbiome’s Impact on Glioma and Brain Metastases: Insights into Development, Progression, and Treatment Response—A Scoping Review. Cancers. 2025; 17(7):1228. https://doi.org/10.3390/cancers17071228
Chicago/Turabian StyleLeigh, Jennifer, Becky Skidmore, Adrian Wong, Saman Maleki Vareki, and Terry L. Ng. 2025. "Exploring the Microbiome’s Impact on Glioma and Brain Metastases: Insights into Development, Progression, and Treatment Response—A Scoping Review" Cancers 17, no. 7: 1228. https://doi.org/10.3390/cancers17071228
APA StyleLeigh, J., Skidmore, B., Wong, A., Maleki Vareki, S., & Ng, T. L. (2025). Exploring the Microbiome’s Impact on Glioma and Brain Metastases: Insights into Development, Progression, and Treatment Response—A Scoping Review. Cancers, 17(7), 1228. https://doi.org/10.3390/cancers17071228