Simple Summary
Patients with breast cancer endure psychological and physical symptoms that negatively impact their quality of life. This study underscores the importance of addressing the needs of metastatic breast cancer patients through four assessment tools that evaluate the patient from different perspectives: general quality of life, depression/anxiety/stress, fatigue, and sleep quality. To the best of our knowledge, this is the only study in Europe to utilize four distinct evaluation instruments to assess quality of life in a real-world context for patients with metastatic breast cancer undergoing treatment with CDK4/6 inhibitors. Our findings demonstrate that the quality of life for these patients is affected in various ways, particularly in their physical, social, and role functioning. Consequently, we encourage all medical oncologists to incorporate quality of life evaluation tools into their daily practice.
Abstract
Purpose: To evaluate the impact of the type of CDK4/6 inhibitor administered and comorbidities on the quality of life in patients with metastatic breast cancer, as well as the correlation between quality of life and patient outcomes. Materials and Methods: This prospective single-center study utilized four internationally validated questionnaires: the EORTC QLQ-C30 (European Organization for Research and Treatment of Cancer Core Cancer Quality of Life Questionnaire), the Depression, Anxiety, and Stress Scale-21 (DASS-21), the Multidimensional Fatigue Inventory (MFI), and the Pittsburgh Sleep Quality Index (PSQI), administered to a cohort of 76 patients undergoing treatment for metastatic breast cancer with CDK4/6 inhibitors. Results: Ribociclib is associated with fewer insomnia problems and appears to provide better sleep quality compared to other CDK4/6 inhibitors. Mental fatigue and loss of appetite negatively influence patient survival. Patients with comorbidities reported more severe insomnia and constipation. Comorbidities are associated with a lower quality of life, reflected in greater fatigue, insomnia, and constipation, as well as increased scores for depression and stress. Conclusions: Assessing global quality of life in metastatic breast cancer patients is essential, as it can predict patient progression and should be integrated into every breast cancer unit.
1. Introduction
Breast cancer is a heterogeneous disease, with treatment decisions and prognosis traditionally guided by immunohistochemistry (IHC) markers such as estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), and Ki67 (a proliferation index marker), along with tumor size, tumor grade, and nodal status [1]. Of all patients with stage IV breast cancer, approximately 75% are hormone receptor-positive (HR+) and human epidermal growth factor receptor 2-negative (HER2−) [2].
The current treatment paradigm for HR+/HER2− advanced breast cancer involves sequencing endocrine therapy, targeted therapy, and/or chemotherapy to prolong patients’ lives, delay disease progression, and minimize cancer-related symptoms [3]. Cyclin-dependent kinase 4 and 6 inhibitors (CDK4/6 inhibitors) are rapidly transforming this treatment landscape. Currently, three CDK4/6 inhibitors have been approved by the US Food and Drug Administration: palbociclib, ribociclib, and abemaciclib [4,5,6].
Over the past decade, two significant developments in cancer medicine have emerged. The first is the understanding that cancer treatment depends on the patient’s overall health. The second is evaluating their well-being using psychosocial and quality of life (QOL) surveys. QOL has been an inferred medicinal outcome [7] since the time of Hippocrates. The first attempt by physicians to objectively evaluate how cancer treatments affect patients’ quality of life, rather than merely their quantity of life, was documented by Karnofsky et al. [8] in 1948. Clinical trials currently employ QOL tools to screen for psychological morbidity, predict survival, and measure treatment response [9].
One of the main clinical and research questions has been how breast cancer treatment affects a patient’s quality of life. Research on interventions for women with breast cancer has focused on psychosocial and emotional issues for the past 25 years. Findings by Ganz and Goodwin [10] indicated that as the number of survivors has increased, patients with breast cancer have been evaluated using various quality of life (QOL) tools to compare the effects of the disease and its treatments to those of healthy women and individuals with other chronic illnesses.
However, as the diagnosis and treatment of the disease have improved significantly over time, quality of life has become an important outcome measure in breast cancer clinical investigations and survivorship studies [11]. To evaluate and summarize the existing evidence on quality of life in breast cancer patients, numerous questionnaires have been developed. Among these, we focused on the following validated instruments, which are among the most common and well-developed tools for measuring quality of life in breast cancer patients: the EORTC QLQ-C30 (European Organization for Research and Treatment of Cancer Core Cancer Quality of Life Questionnaire), the Depression, Anxiety, and Stress Scale-21 (DASS-21), the Multidimensional Fatigue Inventory (MFI), and the Pittsburgh Sleep Quality Index (PSQI). We chose to implement these questionnaires because we believe that the four most important aspects of quality of life (Figure 1)—global health status, emotional state, fatigue, and sleep quality—are very well comprised within these assessment tools.
Figure 1.
The four most important aspects of quality of life from our perspective.
Quality of life in patients with breast cancer is a crucial outcome. This paper presents an extensive overview of the topic ranging from descriptive findings in a specific population to real-world data regarding quality of life. Therefore, the aim of our study was to identify correlations between clinical and pathological characteristics and the quality of life in women with HR+/HER2− metastatic breast cancer. We outlined the patient’s real-world profile from clinical, biological, medical, and quality of life perspectives.
The four main quality of life surveys that we deemed pertinent to our study population are described in this original paper, along with the benefits, acceptability, and limitations. We have also discussed future directions and suggested solutions to address challenges related to questionnaire-type evaluations.
2. Materials and Methods
Participants
This study was conducted on a group of 95 patients diagnosed with HR+/HER2− metastatic breast cancer and treated with CDK4/6 inhibitors. Out of these, 76 patients met the inclusion criteria, and the reported outcomes are derived from this carefully selected group (Figure 2). Three patients with psychiatric problems, seven patients with less than three months of therapy with CDK4/6i, eight patients who declined to answer, and one male patient were eliminated from the study.
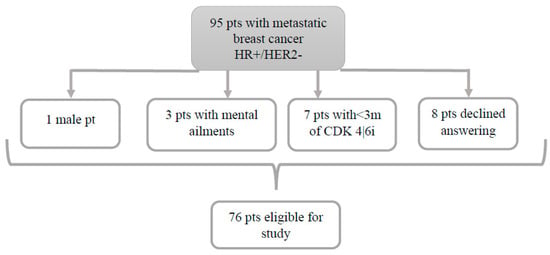
Figure 2.
Flowchart diagram of the study.
Patient demographics and clinical characteristics were retrospectively extracted from electronic medical records during clinical evaluations at Elias University Emergency Hospital, Bucharest, Romania, from January 2018 to January 2024. Quality-of-life data were prospectively collected using the four questionnaires described below.
The study protocol was approved by the Ethics Committee of the Elias University Emergency Hospital, Bucharest, Romania. The study design, data analysis, interpretation, drafting, and revisions comply with the Helsinki Declaration and the Committee on Publication Ethics guidelines. All collected data were anonymized, considering the observational nature of the study, without personal data that could lead to the formal identification of the patient.
Inclusion criteria:
- Female patients aged ≥18 years.
- Either treated or currently in treatment with CDK4/6 inhibitors, with pathologically confirmed HR+/HER2− breast cancer.
- Minimum of three presentations in our oncology department.
We note that the respondents in our study are only patients who had received at least three months of therapy with one of the three CDK4/6 inhibitors (either palbociclib, ribociclib, or abemaciclib).
Exclusion criteria:
- Male patients or females aged < 18 years.
- Patients in critical condition or with mental/psychiatric ailments.
- Patients with < 3 months of CDK4/6 inhibitor therapy.
- Patients who did not complete all four questionnaires or declined answering all questions.
Data collected included age at diagnosis, area of residence, histological grade, stage at diagnosis (locally advanced vs. metastatic), metastasis localization, type of CDK4/6 inhibitor used, duration of CDK4/6 inhibitor therapy, associated endocrine therapy, menopausal status, Ki67 percentage, CA15-3 levels at diagnosis, comorbidities, survival status, family cancer history, and prior chemotherapy (before or after CDK4/6 inhibitor therapy).
3. Questionnaires
From January 2018 to January 2024, patients completed the four questionnaires via telephone after providing prior informed consent. Patients were given four questionnaires: the EORTC QLQ-C30 (European Organization for Research and Treatment of Cancer Core Cancer Quality of Life Questionnaire), the Depression, Anxiety and Stress Scale-21 (DASS-21), the Multidimensional Fatigue Inventory (MFI), and the Pittsburgh Sleep Quality Index (PSQI). Participation in the study was voluntary. Only patients with clear consciousness and no communication impairments were included. The patients were given the Romanian versions of the questionnaires. Both Romanian and English versions of the questionnaires are presented as Supplementary Materials. In this study, the Romanian version of the questionnaires was used, having been requested from each individual organization (EORTC group, Academic Medical Centre, University of Amsterdam Department of Medical Psychology Amsterdam, and Pittsburgh University). The DASS questionnaire is in the public domain, so permission is not needed for its use. All of these prestigious organizations confirm that the translations are conceptually equivalent to the original, culturally relevant to the context of the target country, and easily understood by the individuals to whom the translated instrument is administered.
3.1. EORTC QLQ-C30
The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) is a 30-item tool designed to assess various quality-of-life aspects in cancer patients. It was the first instrument developed by the EORTC QLG and is the product of over a decade of collaborative research. Following its general release in 1993, the QLQ-C30 has been utilized in several cancer clinical trials by a large number of research groups and in various non-trial studies [12]. Version 3.0 is currently the standard version of the QLQ-C30, and the one used in this study.
The QLQ-C30 comprises both multi-item scales and single-item measures covering the following:
- Five functional scales.
- Three symptom scales.
- A global health status/quality-of-life scale.
- Six single items.
Each multi-item scale includes a different set of items, with no item occurring in more than one scale. All scales and single-item measures range in score from 0 to 100. Scores range from 0 to 100, with higher functional and global health scores indicating better quality of life, while higher symptom scores denote greater symptom severity [13].
3.2. Depression, Anxiety, and Stress Scale-21 Items (DASS-21)
The DASS-21 is a set of three self-report scales designed to measure the emotional states of depression, anxiety, and stress.
Each of the three DASS-21 scales contains seven items, divided into subscales with similar content.
- Depression: Assesses dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest/involvement, anhedonia, and inertia.
- Anxiety: Measures autonomic arousal, skeletal muscle effects, situational anxiety, and subjective experiences of anxious affect.
- Stress: Evaluates chronic nonspecific arousal, difficulty relaxing, nervous arousal, irritability, and impatience.
Scores for depression, anxiety, and stress are calculated by summing the scores for the relevant items.
The DASS-21 is based on a dimensional rather than a categorical concept of psychological disorder. The assumption underlying the DASS-21 development (which has been confirmed by research data) is that the differences between depression, anxiety, and stress experienced by normal subjects and clinical populations are essentially differences in degrees [14].
The questionnaire’s 21 items consist of three self-reported measures intended to evaluate DASS. The four possible scores for the seven items on the scales are as follows:
- “Did not apply to me at all”.
- “Applied to me to some degree or some of the time”.
- “Applied to me to a considerable degree or a good part of the time”.
- “Applied to me very much or most of the time”.
Each item is rated on a Likert scale from 0 to 3. Scores of related items are summed to determine the depression, anxiety, and stress scores. According to the manual, the resulting ratings are classified as: “normal, mild, moderate, severe, or extremely severe” [14].
3.3. Multidimensional Fatigue Inventory (MFI)
The MFI is a 20-item scale designed to evaluate five dimensions of fatigue: general fatigue, physical fatigue, reduced motivation, reduced activity, and mental fatigue. It has been utilized in various participant populations, including cancer patients, with an average age of 61 years.
Respondents use a scale ranging from 1 to 5 to indicate how well certain statements regarding fatigue represent their experiences. Several positively phrased items are reverse-scored. Higher total scores correspond to more acute levels of fatigue [15].
The questionnaire has 20 questions rated on a 5-point scale (1 = “yes, that is true” to 5 = “no, that is not true”).
Items are scored 1–5, with ten positively phrased items reverse-scored (items 2, 5, 9, 10, 13, 14, 16, 17, 18, and 19). In the final score, high scores represent more fatigue. The final score is divided into the following subscales:
- General fatigue: Items 1, 5, 12, and 16.
- Physical fatigue: Items 2, 8, 14, and 20.
- Reduced activity: Items 3, 6, 10, and 17.
- Reduced motivation: Items 4, 9, 15, and 18.
- Mental fatigue: Items 7, 11, 13, and 19.
3.4. Pittsburgh Sleep Quality Index (PSQI)
The PSQI is a 19-item self-reported questionnaire designed to assess sleep quality over the past month. The items are grouped into seven components:
- Subjective sleep quality.
- Sleep latency.
- Sleep duration.
- Habitual sleep efficiency.
- Sleep disturbances.
- Use of sleeping medication.
- Daytime dysfunction.
Five additional questions rated by the respondent’s roommate or bed partner are included for clinical purposes and are not scored. The questionnaire has been validated with various clinical populations, including patients with major depressive disorder, disorders of initiating and maintaining sleep, disorders of excessive somnolence, cancer, and fibromyalgia [16].
Each component score of the PSQI ranges from 0 to 3, with 3 indicating the greatest dysfunction or disturbance. The seven component scores are summed to obtain a global PSQI score, which ranges from 0 to 21. Higher scores indicate poorer sleep quality, with a score greater than 5 suggesting significant sleep difficulties.
4. Statistical Analysis
All questionnaire data were collected on paper and entered into Microsoft Excel by an independent researcher. Statistical processing was conducted using IBM SPSS Statistics for Windows, Version 29.0 (30-day trial version, Armonk, NY, USA: IBM Corp.).
- Nominal data: Presented as absolute frequency and percentage.
- Continuous variables: Expressed as mean, standard deviation, minimum, and maximum.
Analysis of the association between categorical variables was conducted using cross-tabulation and the χ2 (chi-square) test. If the results of the chi-square test were altered enough to be considered, Fisher’s exact test was used. The Mann–Whitney U test was used to compare means for dichotomous variables. The Kruskal–Wallis H test compared means between groups, as the variables had a non-Gaussian distribution. A p-value of < 0.05 was considered statistically significant.
In this study, we used bootstrapped 95% confidence intervals (CIs) to assess the variability and reliability of clinical outcome measures among oncology patients with and without comorbidities. The bootstrap method was employed with 1000 resamples, allowing us to generate robust estimates of the mean and confidence intervals without assuming normality. The interquartile range (IQR) was used as a measure of dispersion for skewed distributions, in line with best practices in biostatistics. A horizontal bar plot with confidence intervals was constructed to visually compare the two groups, with blue representing patients without comorbidities and red representing those with comorbidities. The mean values were plotted as discrete points, while the 95% CIs were illustrated as horizontal lines, providing a clear depiction of the uncertainty around the estimates. The overlap or separation of confidence intervals was used to qualitatively assess the presence of statistically meaningful differences between the groups.
To account for the potential inflation of Type I error due to multiple comparisons, we applied false discovery rate (FDR) correction using the Benjamini–Hochberg procedure. This method controls the expected proportion of false positives while maintaining statistical power. Adjusted p-values were calculated for all analyses involving multiple testing, ensuring a more rigorous interpretation of statistical significance. p-values below 0.05 after FDR correction were considered statistically significant.
5. Results
Patients’ demographics and clinical characteristics are shown in Table 1.

Table 1.
The patients’ demographics and clinical characteristics.
The most frequent comorbidities that we encountered were as follows:
- Hypertension (30 patients).
- Type II diabetes (16 patients).
- Cardiovascular comorbidities (16 patients).
- Dyslipidemia (15 patients).
- Obesity (13 patients).
- Osteoporosis (9 patients).
- Hypothyroidism (6 patients).
- Depressive syndrome (6 patients).
- Chronic kidney disease (5 patients).
- Hepatic steatosis (4 patients).
Other comorbidities that we encountered in the case of patients in this study were the following: cataract, tuberculosis in history, respiratory failure, Parkinson’s disease, hiatal hernia, polynodular goiter, chronic obstructive pulmonary disease, pulmonary fibrosis, dementia, fractures on pathological bone, polyneuropathy, autoimmune thyroiditis, stroke, hearing loss, right calf amputation, diabetic nephropathy, gallbladder stones. These comorbidities were encountered with a frequency of one or two cases in our study population.
We need to mention that breast cancer was the cause of all deaths, despite the fact that these patients also had many major comorbidities.
The analysis of quality of life, as derived from the four questionnaires, was correlated with the type of CDK4/6 inhibitor received, patient’s evolution (death vs. survival), and associated comorbidities. Three multivariate analyses were conducted to identify statistically significant differences among patient groups. The findings of each analysis are evaluated separately in the following subchapters.
5.1. Overall Analysis of Quality of Life (QoL)
The following statistics (Table 2) summarize overall health status, functioning, physical and emotional symptoms, sleep quality, and stress/anxiety levels. For improved accuracy, data from the four questionnaires were consolidated into the SPSS database, allowing for comprehensive statistical analysis. The findings were divided into subgroups as follows:
Table 2.
Analysis of overall health status, functioning, physical and emotional symptoms, sleep quality, and stress/anxiety levels.
The final two single items on the EORTC-QLC-C30 tool assessment are “How would you rate your overall health during the past week?” and “How would you rate your overall quality of life during the past week?”, ranging from 1 (poor) to 7 (excellent) in response. These two questions rank among the most important when evaluating quality of life, and the answers from our patients are displayed in the following figures (Figure 3 and Figure 4).
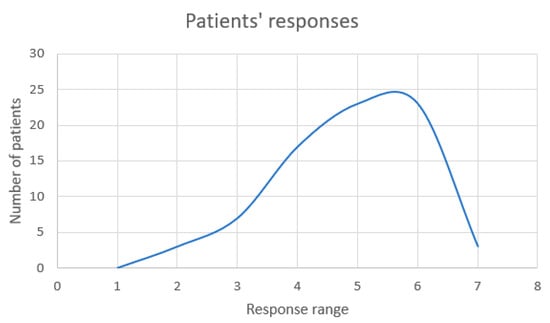
Figure 3.
Analysis of patients’ responses to the question “How would you rate your overall health during the past week?”.
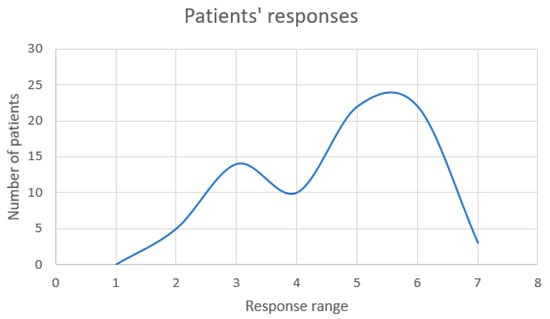
Figure 4.
Analysis of patients’ responses to the question “How would you rate your overall quality of life during the past week?”.
With an answer of 5 (n = 23) or 6 (n = 23) out of 7, which is the highest health quality, the majority of patients (n = 46) believed that their general health had been good over the last several weeks.
In terms of subjective perception and quality of life, the majority of our patients (n = 44) believed they had a good quality of life, with responses ranging from 5 (n = 22) to 6 (n = 22) out of 7, which is regarded as an exceptional quality of life.
The three emotional states—stress, anxiety, and depression—are also graphically analyzed (Figure 5). There are patients who may have mild, moderate, severe, or extremely severe emotions, with a wide range and variability across patients. However, the majority of respondents appear to have no issues related to depression (n = 35), anxiety (n = 31), or stress (n = 42).
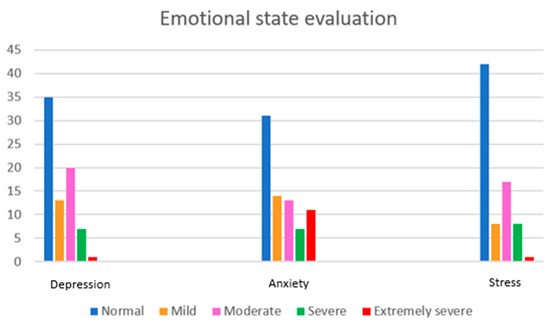
Figure 5.
Analysis of the three emotional states: depression, anxiety, and stress.
5.2. Quality of Life Analysis Correlated with CDK4/6 Inhibitor Type
The following analysis (Table 3; Table S1: the Kruskal–Wallis H test statistics which compares means between groups for the quality of life analysis correlated with CDK4/6i test statistics can be found in the Supplementary Material) examines how each item of the four questionnaires correlates with the type of CDK4/6 inhibitor (palbociclib, ribociclib, and abemaciclib).
Table 3.
Quality of life analysis correlated with CDK4/6i.
Differences between groups regarding insomnia, diarrhea, and sleep quality were the only significant ones. All other correlations and differences between groups were not statistically significant.
5.3. Analysis of Quality of Life Correlated with Patient Evolution
The following statistics (Table 4; Table S2: the Kruskal–Wallis H test statistics which compares means between groups for the quality of life analysis correlated with patient evolution test statistics can be found in the Supplementary Material) analyze how each item of the four questionnaires correlates with patient evolution (survival vs. death):
Table 4.
Quality of life analysis correlated with patient evolution.
Below is a summary table (Table 5) showing the point-biserial correlation coefficient (rpb) for each variable comparing survival (coded as 1) versus death (coded as 0). For each variable, the coefficient was computed using the following formula:
where M1 and M0 are the group “means” (using the provided medians as surrogates), sp is the pooled standard deviation, and p and q are the proportions in the survival and death groups, respectively.
rpb = (M1 − M0)⁄sp × √(p · q)
Table 5.
Correlation coefficients for survival.
The next figure (Figure 6) is the graphical representation of the correlation coefficients for survival vs. death.
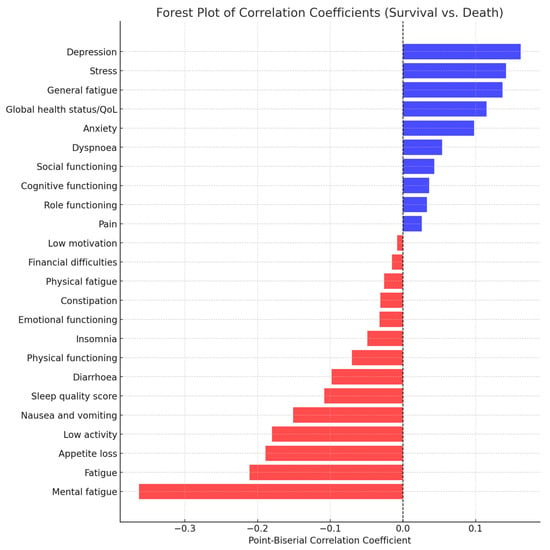
Figure 6.
Forest plot of correlation coefficients for survival vs. death. Positive correlations (blue bars) indicate that higher scores on that variable are associated with survival. Negative correlations (red bars) indicate that higher scores on that variable are associated with death. The dashed vertical line at zero represents no association.
5.4. Analysis of Quality of Life Correlated with Comorbidities
The following statistics (Table 6; Table S3: the Kruskal–Wallis H test statistics which compares means between groups for the quality of life analysis correlated with comorbidities test statistics can be found in the Supplementary Material) analyze how each item of the four questionnaires correlates with the comorbidities present in the patients:
Table 6.
Quality of life analysis correlated with comorbidities.
In the figure below (Figure 7), we analyzed bootstrapped 95% confidence intervals for clinical outcomes in oncology patients with and without comorbidities.
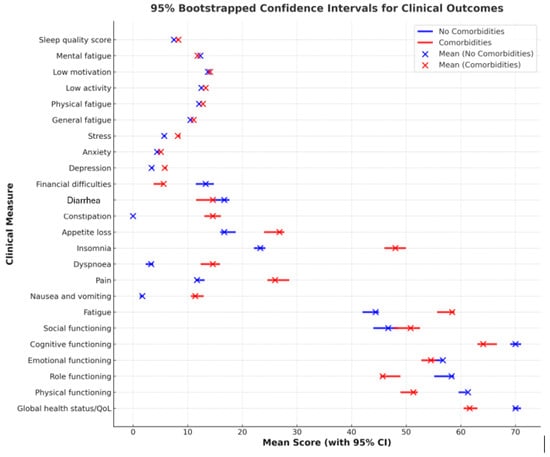
Figure 7.
Bootstrapped 95% confidence intervals for clinical outcomes in oncology patients with and without comorbidities. Blue (No Comorbidities): represents the mean scores and 95% confidence intervals (CIs) for patients without comorbidities. Red (Comorbidities): represents the mean scores and 95% confidence intervals (CIs) for patients with comorbidities. Each horizontal line represents the range of the 95% confidence interval (CI) for a given clinical measure, while the dots indicate the mean values.
5.5. Analysis of Quality of Life During COVID Pandemic
We acknowledge that the pandemic introduced unique challenges in oncology care, including delays in diagnosis and treatment, modifications in therapeutic approaches, and disruptions in healthcare access, all of which could influence progression-free survival (PFS), overall survival (OS), and time on treatment (ToT).
To address this concern, we conducted an analysis specifically examining the impact of COVID-19 infection on PFS, OS, and ToT within our cohort. The findings from this analysis have been incorporated into Table 7 and Table 8, allowing for a more comprehensive understanding of the potential confounding effects introduced by the pandemic.
Table 7.
Impact of COVID-19 infection on time on treatment (ToT), progression-free survival (PFS), and overall survival (OS) in patients receiving CDK4/6 inhibitors.
Table 8.
Statistical comparison of time on treatment (ToT), progression-free survival (PFS), and overall survival (OS) between patients with and without COVID-19 infection.
We believe that taking the COVID pandemic period into consideration strengthens the robustness of our study by considering external factors that may have influenced treatment outcomes.
Time on treatment (ToT) is defined as the duration a patient remains on CDK4/6i therapy before discontinuation, regardless of the reason for stopping treatment. Progression-free survival (PFS) is defined as time from treatment initiation to disease progression or death. Overall survival (OS) is defined as time from diagnosis or treatment initiation to death from any cause.
6. Discussions
Quality of life is affected in multiple dimensions, particularly in physical, social, and role functioning. Fatigue is a central symptom that impacts physical functioning and motivation. Sleep problems are common and correlated with other symptoms, such as fatigue and stress. Financial difficulties and nausea are less common compared to other issues. Levels of stress and depression range from moderate to high, with significant variations between patients.
Differences between groups regarding insomnia and diarrhea are significant. Ribociclib is associated with fewer insomnia problems, while abemaciclib is linked to more frequent diarrhea. Ribociclib appears to provide better sleep quality compared to other treatments.
Indicators with statistically significant differences regarding patient evolution (death vs. survival) include loss of appetite (p = 0.036)—those who died had higher scores—and mental fatigue (p = 0.003)—those who died had higher scores. Indicators with nearly significant differences include fatigue (p = 0.094), with higher scores in those who died, and nausea and vomiting (p = 0.088), with higher scores in those who died. These results suggest that mental fatigue and loss of appetite may have a greater influence on patient survival and warrant further investigation in the context of symptom management.
Indicators with statistically significant differences in the analysis of comorbidities include insomnia (p = 0.014)—people with comorbidities reported more severe insomnia—and constipation (p = 0.046). Nearly significant indicators include fatigue (p = 0.091), with higher scores in those with comorbidities, depression (p = 0.075), and stress (p = 0.121).
Comorbidities are associated with a lower quality of life, reflected in greater fatigue, insomnia, and constipation, as well as increased scores for depression and stress. These differences indicate the need for special attention to symptom management and psychological health in patients with comorbidities.
6.1. Patient Profile from a Clinical, Biological, Treatment, and Quality-of-Life Perspective
Quality of life was moderate-to-good (62.72 ± 19.93), but physical (52.63 ± 25.96) and social (50.22 ± 37.96) functioning were significantly affected. Emotionally, patients were at a moderate level (54.82 ± 23.50), with large variations between cases. The main symptoms included fatigue (56.58 ± 26.37) and insomnia (44.74 ± 30.58), which had a significant negative impact. Pain (24.12 ± 29.61) and loss of appetite (25.44 ± 29.75) were present but moderate on average. Cognitive functioning (64.91 ± 27.83) was better preserved than in other domains, but the social score indicated isolation for some patients. Effective symptom management (e.g., fatigue, insomnia) and social support are essential for improving quality of life.
6.2. Benefits of Quality of Life Assessment in Breast Cancer Patients
One significant advantage of quality of life assessment, according to Greenhalgh and Meadows, Di Maio and Perrone, and Le et al., is that it promotes shared decision-making and facilitates communication between doctors and patients [17,18,19,20] by providing patients with feedback on their expectations, goals, and progress [21].
Additional potential benefits of quality-of-life testing include establishing a baseline evaluation when initiating treatment or therapy, identifying treatable problems that may otherwise be overlooked in routine patient care, and addressing crucial supportive measures such as illness education and dietary counseling. These aspects can play a vital role in enhancing patient well-being, treatment adherence, and overall quality of care. Measuring quality of life may also be useful in detecting additional mental and physical issues and tracking declines in functional ability.
6.3. Acceptability of Quality of Life Assessments
Quality of life assessments are deemed acceptable by both patients and healthcare providers for assisting individuals with breast cancer in addressing aspects of their quality of life that have been impacted by the disease. Numerous studies have illustrated the rationale behind doctors’ acceptance of the use of quality of life measures.
According to Stiggelbout et al. [22], patients’ emotions about quality of life, as opposed to quantity of life, can be assessed using questionnaires. In their study on patient acceptability of quality of life questionnaires, Apolone et al. [23] found that 64% of patients responded to the surveys, with very few items missing. These findings demonstrate that quality of life questionnaires, specifically the EORTC QLQ-C30 used in this study, are acceptable to patients [23].
6.4. Limitations of Quality of Life Assessments
Assessments with fewer answer alternatives and verbal questions, rather than solely numerical ones, were deemed acceptable by cancer patients. Furthermore, research by Pijls-Johannesma et al. has shown that respondents preferred questionnaires that did not include excessively sensitive, personal, or irrelevant questions [24].
This could be one of the limitations of our study, given that the majority of answers were numerical, some questions were too personal (e.g., those regarding sexual life), and some questions were irrelevant to specific subgroups of patients. For instance, since many respondents were retired, inquiries about work-related issues were irrelevant.
Another major limitation is the reluctance of doctors to use the tests due to logistical issues, such as time and budget constraints [25,26]. Moreover, physicians are often less familiar with quality of life assessments than with imaging or physiological tests and may be unsure how to interpret the results or respond to them [26].
Particularly in the elderly, compliance with questionnaires can be problematic due to cognitive disorders, comorbidities, and illiteracy. This is why one of the exclusion criteria in our study was patients in critical condition or those with mental or psychiatric ailments.
Another significant limitation of this study is that quality of life (QoL) was assessed at a single time point rather than longitudinally. As a result, we were unable to evaluate changes in QoL over time, such as before and after initiating systemic therapy with CDK4/6 inhibitors. A longitudinal assessment would provide a more comprehensive understanding of the impact of treatment on patient-reported outcomes.
Furthermore, several respondents felt embarrassed to answer certain questions in the presence of researchers. We assured them that their responses would remain confidential.
In conclusion, our review has several limitations that must be considered with caution when interpreting the results.
6.5. Future Directions and Suggested Solutions to Address Challenges in Questionnaire-Type Evaluations
Simply adding quality of life metrics to the everyday duties of oncology staff will not suffice for future implementation. Quality of life should be integrated into the care process of patient-reported outcomes by rethinking care delivery, particularly by considering the principles of effective distribution and establishing new infrastructures and technologies.
The ideal evaluation system must be clinically relevant (helpful and delivered on time), adaptable, culturally sensitive, low-burden, low-cost, integrated into standard operating processes, and meet community, consumer, and regulatory needs [27].
Patients, doctors, and office workers may be reluctant to adopt new practices due to time constraints. Rather than merely providing the doctor with a functional status score, offering interpretations and suggestions regarding the score and available resources could be more beneficial [28].
Overall, we believe breast cancer patients stand to benefit significantly from the use of quality of life evaluations in clinical practice. Physicians will be better equipped to make treatment decisions if they receive reliable information about health-related quality of life from self-reported questionnaires. Quality of life has become a more significant consideration in the holistic treatment of patients with breast cancer.
We firmly believe that all breast cancer units should implement these questionnaires, along with specialized personnel to administer them, interpret the results, and communicate findings to the medical staff.
7. Conclusions
To the best of our knowledge, this is the only study in Romania and throughout Europe to assess quality of life in a real-world setting for patients with metastatic breast cancer receiving CDK4/6 inhibitors using four different evaluation tools.
This study demonstrates that the EORTC QLQ-C30 (European Organization for Research and Treatment of Cancer Core Cancer Quality of Life Questionnaire), the Depression, Anxiety and Stress Scale-21 (DASS-21), the Multidimensional Fatigue Inventory (MFI), and the Pittsburgh Sleep Quality Index (PSQI) are practical and valid instruments for measuring quality of life in patients with advanced breast cancer. We encourage every medical oncologist to implement these questionnaires in their day-to-day practice.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/cancers17050818/s1, Table S1: The Kruskal–Wallis H test statistics which compares medians between groups for the quality of life analysis correlated with CDK4/6i. Table S2: The Kruskal–Wallis H test statistics which compares medians between groups for the quality of life analysis correlated with patient evolution. Table S3: The Kruskal–Wallis H test statistics which compares medians between groups for the quality of life analysis correlated with comorbidities. All the four questionnaires can also be found in this section, both in English and in Romanian.
Author Contributions
Conceptualization, I.-M.S.; methodology, I.-M.S.; software, I.-M.S.; validation, I.-M.S.; formal analysis, I.-M.S.; investigation, I.-M.S. and C.N.; resources, I.-M.S.; data curation, I.-M.S.; writing—original draft preparation, I.-M.S.; writing—review and editing, I.-M.S. and C.N.; visualization, I.-M.S. and C.N.; supervision, I.-M.S. and C.N.; project administration, I.-M.S. All authors have read and agreed to the published version of the manuscript.
Funding
The cost for the publication of this manuscript will be supported by the Romanian National Society of Medical Oncology.
Institutional Review Board Statement
The present study is part of the first author’s PhD thesis. The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Elias University Emergency Hospital no 1489/01.03.2024.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request from the first author, due to privacy and ethical restrictions.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Gao, J.J.; Swain, S.M. Luminal A Breast Cancer and Molecular Assays: A Review. Oncologist 2018, 23, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Altekruse, S.F.; Li, C.I.; Chen, V.W.; Clarke, C.A.; Ries, L.A.G.; Cronin, K.A. US Incidence of Breast Cancer Subtypes Defined by Joint Hormone Receptor and HER2 Status. JNCI J. Natl. Cancer Inst. 2014, 106, dju055. [Google Scholar] [CrossRef]
- Shah, M.; Nunes, M.R.; Stearns, V. CDK4/6 Inhibitors: Game Changers in the Management of Hormone Receptor–Positive Advanced Breast Cancer? Oncol. Williston Park N 2018, 32, 216–222. [Google Scholar]
- Finn, R.S.; Martin, M.; Rugo, H.S.; Jones, S.; Im, S.-A.; Gelmon, K.; Harbeck, N.; Lipatov, O.N.; Walshe, J.M.; Moulder, S.; et al. Palbociclib and Letrozole in Advanced Breast Cancer. N. Engl. J. Med. 2016, 375, 1925–1936. [Google Scholar] [CrossRef]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.S.; Sonke, G.S.; Paluch-Shimon, S.; Campone, M.; Petrakova, K.; Blackwell, K.L.; Winer, E.P.; et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann. Oncol. 2018, 29, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- Goetz, M.P.; Toi, M.; Campone, M.; Sohn, J.; Paluch-Shimon, S.; Huober, J.; Park, I.H.; Trédan, O.; Chen, S.-C.; Manso, L.; et al. MONARCH 3: Abemaciclib As Initial Therapy for Advanced Breast Cancer. J. Clin. Oncol. 2017, 35, 3638–3646. [Google Scholar] [CrossRef] [PubMed]
- Ganz, P.A. Quality of Life Measures in Cancer Chemotherapy: Methodology and Implications. PharmacoEconomics 1994, 5, 376–388. [Google Scholar] [CrossRef] [PubMed]
- Karnofsky, D.A.; Abelmann, W.H.; Craver, L.F.; Burchenal, J.H. The use of the nitrogen mustards in the palliative treatment of carcinoma: With particular reference to bronchogenic carcinoma. Cancer 1948, 1, 634–656. [Google Scholar] [CrossRef]
- Velikova, G.; Wright, E.P.; Smith, A.B.; Cull, A.; Gould, A.; Forman, D.; Perren, T.; Stead, M.; Brown, J.; Selby, P.J. Automated Collection of Quality-of-Life Data: A Comparison of Paper and Computer Touch-Screen Questionnaires. J. Clin. Oncol. 1999, 17, 998–1007. [Google Scholar] [CrossRef] [PubMed]
- Ganz, P.A.; Goodwin, P.J. Quality of life in breast cancer: What have we learned and where do we go from here? In Outcomes Assessment in Cancer: Measures, Methods and Applications; Gotay, C.C., Snyder, C., Lipscomb, J., Eds.; Cambridge University Press: Cambridge, UK, 2004; pp. 93–125. ISBN 978-0-521-83890-0. [Google Scholar]
- Mokhtari-Hessari, P.; Montazeri, A. Health-related quality of life in breast cancer patients: Review of reviews from 2008 to 2018. Health Qual. Life Outcomes 2020, 18, 338. [Google Scholar] [CrossRef] [PubMed]
- CSI EORTC QLQ-C30. Available online: https://qol.eortc.org/questionnaires/core/eortc-qlq-c30/ (accessed on 24 January 2025).
- Fayers, P.M.; Aaronson, N.K.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomley, A.; on behalf of the EORTC Quality of Life Group. The EORTC QLQ-C30 Scoring Manual, 3rd ed.; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2001. [Google Scholar]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety & Stress Scales, 2nd ed.; Psychology Foundation: Sydney, Australia, 1995. [Google Scholar]
- Smets, E.M.A.; Garssen, B.; Bonke, B.; De Haes, J.C.J.M. The multidimensional fatigue inventory (MFI) psychometric qualities of an instrument to assess fatigue. J. Psychosom. Res. 1995, 39, 315–325. [Google Scholar] [CrossRef]
- Shahid, A.; Wilkinson, K.; Marcu, S.; Shapiro, C.M. (Eds.) STOP, THAT and One Hundred Other Sleep Scales; Springer Science + Business Media, LLC.: Berlin/Heidelberg, Germany, 2012. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index (PSQI): A new instrument for psychiatric research and practice. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, J.; Meadows, K. The effectiveness of the use of patient-based measures of health in routine practice in improving the process and outcomes of patient care: A literature review. J. Eval. Clin. Pract. 1999, 5, 401–416. [Google Scholar] [CrossRef]
- Di Maio, M.; Perrone, F. Quality of Life in Elderly Patients with Cancer. Health Qual. Life Outcomes 2003, 1, 44. [Google Scholar] [CrossRef] [PubMed]
- Le, P.P.; Kohane, I.S.; Weeks, J.C. Using a pen-based computer to collect health-related quality of life and utilities information. Proc. Annu. Symp. Comput. Appl. Med. Care 1995, 839–843. [Google Scholar] [PubMed]
- Donaldson, M.S. Taking Stock of Health-Related Quality-of-Life Measurement in Oncology Practice in the United States. J. Natl. Cancer Inst. Monogr. 2004, 2004, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Anne, M.; De Haes Stiggelbout, J.C.J.M.; Gwendoline, M.K.; Kievit, J.; Jan-Willem, H.L. Tradeoffs Between Quality and Quantity of Life: Development of the QQ Questionnaire for Cancer Patient Attitudes. Med. Decis. Mak. 1996, 16, 184–192. [Google Scholar] [CrossRef]
- Apolone, G.; Filiberti, A.; Cifani, S.; Ruggiata, R.; Mosconi, P. Evaluation of the EORTC QLQ-C30 Questionnaire: A Comparison with SF-36 Health Survey in a Cohort of Italian long-Survival Cancer Patients—ScienceDirect. Ann. Oncol. 1998, 9, 549–557. [Google Scholar] [CrossRef]
- Pijls-Johannesma, M.C.G.; Pijpe, A.; Kempen, G.I.J.M.; Lambin, P.; Dagnelie, P.C. Health related quality of life assessment instruments: A prospective study on preference and acceptability among cancer patients referred for radiotherapy. Eur. J. Cancer 2005, 41, 2250–2256. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.; Perez, D.; McNoe, B. The use of quality of life data in clinical practice. Qual. Life Res. 1997, 7, 85–91. [Google Scholar] [CrossRef]
- Perry, S.; Kowalski, T.L.; Chang, C.-H. Quality of life assessment in women with breast cancer: Benefits, acceptability and utilization. Health Qual. Life Outcomes 2007, 5, 24. [Google Scholar] [CrossRef] [PubMed]
- Sederer, L.I.; Dickey, B.; Eisen, S.V. Assessing Outcomes in Clinical Practice. Psychiatr. Q. 1997, 68, 311–325. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Carter, W.B. Strategies for Improving and Expanding the Application of Health Status Measures in Clinical Settings A Researcher–Developer Viewpoint. Med. Care 1992, 30, MS176–MS186. Available online: https://journals.lww.com/lww-medicalcare/abstract/1992/05001/Strategies_for_Improving_and_Expanding_the.15.aspx (accessed on 24 January 2025). [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).