

Feasibility and Acceptability of Integrating Acupuncture for Management of Multiple Symptoms in Medically Underserved Breast Cancer Survivors

 ,
,  , , , , and
, , , , and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Procedure
2.2.1. Recruitment
2.2.2. Screening
2.2.3. Data Collection
2.2.4. Randomization
2.3. Intervention
2.4. Usual Care Group
2.5. Measures
2.5.1. Demographic and Clinical Characteristics
2.5.2. Symptoms
2.5.3. Feasibility and Acceptability
- (a)
- Recruitment rate: calculated as the number of randomized women out of those we screened and contacted.
- (b)
- Retention rate: calculated as the number of women who completed baseline and follow-up assessments at week 6 and week 12 out of the total number of participants.
- (c)
- Engagement/adherence rate: calculated as the number of women who completed all 10 acupuncture sessions out of those randomized to the acupuncture group.
- (d)
- Fidelity: calculated as the number of times acupuncturists followed the treatment protocol and adhered to the standardized point selection guidelines.
2.6. Data Analysis
3. Results
3.1. Demographic and Clinical Characteristics
3.2. Feasibility
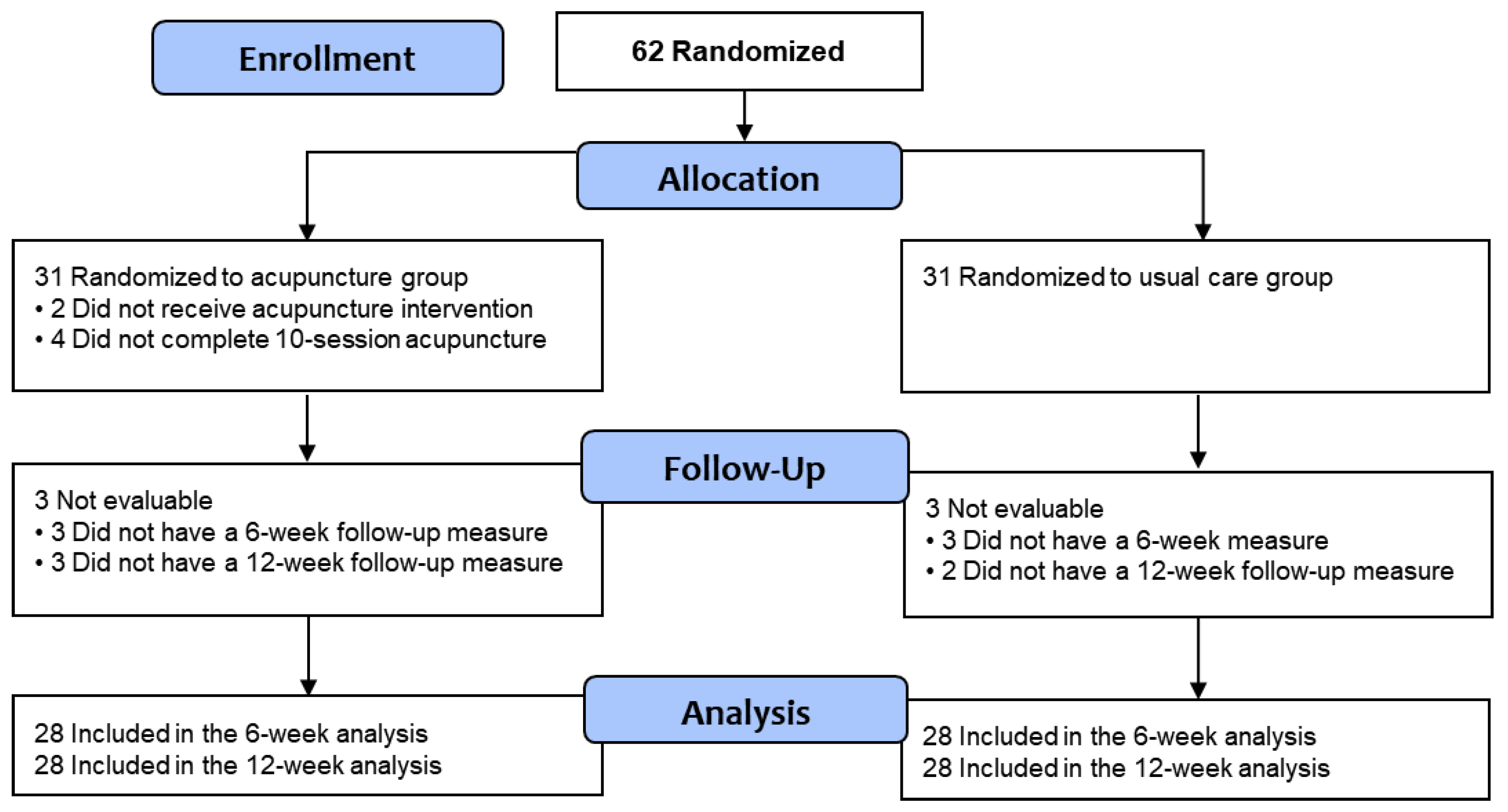
3.2.1. Recruitment and Retention
3.2.2. Engagement
3.2.3. Fidelity
3.3. Acceptability and Survivor Treatment Satisfaction
3.4. Symptom Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tonorezos, E.; Devasia, T.; Mariotto, A.B.; Mollica, M.A.; Gallicchio, L.; Green, P.; Doose, M.; Brick, R.; Streck, B.; Reed, C.; et al. Prevalence of cancer survivors in the United States. JNCI J. Natl. Cancer Inst. 2024, 116, 1784–1790. [Google Scholar] [CrossRef]
- Mandelblatt, J.S.; Zhai, W.; Ahn, J.; Small, B.J.; Ahles, T.A.; Carroll, J.E.; Denduluri, N.; Dilawari, A.; Extermann, M.; Graham, D.; et al. Symptom burden among older breast cancer survivors: The Thinking and Living With Cancer (TLC) study. Cancer 2020, 126, 1183–1192. [Google Scholar] [CrossRef]
- Whisenant, M.S.; Williams, L.A.; Mendoza, T.; Cleeland, C.; Chen, T.H.; Fisch, M.J.; Shi, Q. Identification of Breast Cancer Survivors With High Symptom Burden. Cancer Nurs. 2022, 45, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Lu, Z.; Qiu, J.; Luo, H.; Tang, L.; Li, Y.; Li, P. Symptom experience in endocrine therapy for breast cancer patients: A qualitative systematic review and meta-synthesis. Asia-Pac. J. Oncol. Nurs. 2023, 11, 100364. [Google Scholar] [CrossRef]
- Eliassen, F.M.; Blåfjelldal, V.; Helland, T.; Hjorth, C.F.; Hølland, K.; Lode, L.; Bertelsen, B.-E.; Janssen, E.A.M.; Mellgren, G.; Kvaløy, J.T.; et al. Importance of endocrine treatment adherence and persistence in breast cancer survivorship: A systematic review. BMC Cancer 2023, 23, 625. [Google Scholar] [CrossRef] [PubMed]
- Elshafie, S.; Trivedi, R.; Villa-Zapata, L.A.; Tackett, R.L.; Zaghloul, I.Y.; Young, H.N. Adherence, clinical benefits, and adverse effects of endocrine therapies among women with nonmetastatic breast cancer in developing countries: A systematic review and meta-analysis. Cancer 2024, 131, e35550. [Google Scholar] [CrossRef] [PubMed]
- Carmen, A.; Anne, O.; Monika, S.; Daniel, E.; Johannes, G.; Verena, M.; Michael, H.; Christine, B. Does the toxicity of endocrine therapy persist into long-term survivorship?: Patient-reported outcome results from a follow-up study beyond a 10-year-survival. Breast Cancer Res. Treat. 2023, 198, 475–485. [Google Scholar] [CrossRef]
- Alnaim, L. Health-Related Quality of Life in Women With Breast Cancer Undergoing Treatment With Hormonal Therapy–A Review Study. Eur. J. Breast Health 2022, 18, 292. [Google Scholar] [CrossRef] [PubMed]
- Bjerkeset, E.; Röhrl, K.; Schou-Bredal, I. Symptom cluster of pain, fatigue, and psychological distress in breast cancer survivors: Prevalence and characteristics. Breast Cancer Res. Treat. 2020, 180, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.J.; Ismaila, N.; Bao, T.; Barton, D.; Ben-Arye, E.; Garland, E.L.; Greenlee, H.; Leblanc, T.; Lee, R.T.; Lopez, A.M. Integrative medicine for pain management in oncology: Society for integrative oncology–ASCO guideline. J. Clin. Oncol. 2022, 40, 3998–4024. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Schlaeger, J.M.; Jang, M.K.; Lin, Y.; Park, C.; Liu, T.; Sun, M.; Doorenbos, A.Z. Acupuncture improves multiple treatment-related symptoms in breast cancer survivors: A systematic review and meta-analysis. J. Altern. Complement. Med. 2021, 27, 1084–1097. [Google Scholar] [CrossRef]
- Vallerand, A.H.; Hasenau, S.; Templin, T.; Collins-Bohler, D. Disparities between black and white patients with cancer pain: The effect of perception of control over pain. Pain Med. 2005, 6, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Alcalá, H.E. Differential mental health impact of cancer across racial/ethnic groups: Findings from a population-based study in California. BMC Public Health 2014, 14, 930. [Google Scholar] [CrossRef] [PubMed]
- Tarver, W.L.; Justice, Z.; Jonnalagadda, P.; Rahurkar, S.; Obeng-Gyasi, S.; Krok-Schoen, J.L.; Petrecca, A.; Paskett, E.D. A scoping review of the evidence on survivorship care plans among minority, rural, and low-income populations. J. Cancer Surviv. 2024, 14, 930. [Google Scholar] [CrossRef] [PubMed]
- Caraballo, C.; Ndumele, C.D.; Roy, B.; Lu, Y.; Riley, C.; Herrin, J.; Krumholz, H.M. Trends in racial and ethnic disparities in barriers to timely medical care among adults in the US, 1999 to 2018. JAMA Health Forum 2022, 3, e223856. [Google Scholar] [CrossRef] [PubMed]
- Tangkiatkumjai, M.; Boardman, H.; Walker, D.-M. Potential factors that influence usage of complementary and alternative medicine worldwide: A systematic review. BMC Complement. Med. Ther. 2020, 20, 363. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.W.; Roseen, E.J.; Stone, J.A.M.; Gardiner, P.; Olson, J.; Rosen, S.; Wayne, P.; Davis, R.; Coeytaux, R. Incorporating Acupuncture Into American Healthcare: Initiating a Discussion on Implementation Science, the Status of the Field, and Stakeholder Considerations. Glob. Adv. Health Med. 2021, 10, 21649561211042574. [Google Scholar] [CrossRef] [PubMed]
- Teets, R.; Nielsen, A.; Moonaz, S.; Anderson, B.J.; Mah, D.M.; Walter, E.; Milanes, M.; Jyung, H.; Soto Cossio, L.E.; Meissner, P. Group acupuncture therapy with yoga therapy for chronic neck, low back, and osteoarthritis pain in safety net settings for an underserved population: A feasibility pilot study. Glob. Adv. Integr. Med. Health 2023, 12, 27536130231202515. [Google Scholar] [CrossRef]
- Li, H.; Schlaeger, J.M.; Patil, C.L.; Danciu, O.; Chen, Z.; Lif, N.; Gao, S.; Doorenbos, A.Z. Feasibility of implementing acupuncture in medically underserved breast cancer survivors (FAB): A protocol. Contemp. Clin. Trials 2024, 136, 107387. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c332. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Ramsey, K.; Buckley, D.I.; Michaels, L.; Kobus, A.; Eckstrom, E.; Forro, V.; Morris, C. Performance of a Patient Reported Outcomes Measurement Information System (PROMIS) Short Form in Older Adults with Chronic Musculoskeletal Pain. Pain Med. 2015, 17, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.; Kim, Y.; Lim, J.; Yoon, J.; Kim, S.; Kang, E.; Nam, H.; Shim, S.; Lee, M.; Bok, H.; et al. Validation of the Korean Version of the Patient-Reported Outcomes Measurement Information System 29 Profile V2.1 among Cancer Survivors. Cancer Res. Treat. 2022, 54, 10–19. [Google Scholar] [CrossRef]
- Cella, D.; Choi, S.W.; Condon, D.M.; Schalet, B.; Hays, R.D.; Rothrock, N.E.; Yount, S.; Cook, K.F.; Gershon, R.C.; Amtmann, D.; et al. PROMIS(®) Adult Health Profiles: Efficient Short-Form Measures of Seven Health Domains. Value Health 2019, 22, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Sloan, J.A.; Loprinzi, C.L.; Novotny, P.J.; Barton, D.L.; Lavasseur, B.I.; Windschitl, H. Methodologic Lessons Learned From Hot Flash Studies. J. Clin. Oncol. 2001, 19, 4280–4290. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.J.; Bowman, M.A.; Xie, S.X.; Bruner, D.; DeMichele, A.; Farrar, J.T. Electroacupuncture versus gabapentin for hot flashes among breast cancer survivors: A randomized placebo-controlled trial. J. Clin. Oncol. 2015, 33, 3615. [Google Scholar] [CrossRef] [PubMed]
- Wilkie, D.J.; Huang, H.-Y.; Berry, D.L.; Schwartz, A.; Lin, Y.-C.; Ko, N.-Y.; Chen, A.; Gralow, J.; Lindsley, S.K.; Fitzgibbon, D. Cancer symptom control: Feasibility of a tailored, interactive computerized program for patients. Fam. Community Health 2001, 24, 48–62. [Google Scholar] [CrossRef] [PubMed]
- Wilkie, D.J.; Judge, M.K.M.; Berry, D.L.; Dell, J.; Zong, S.; Gilespie, R. Usability of a computerized PAINReportIt in the general public with pain and people with cancer pain. J. Pain Symptom Manag. 2003, 25, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Laird, N.M.; Ware, J.H. Random-effects models for longitudinal data. Biometrics 1982, 38, 963–974. [Google Scholar] [CrossRef] [PubMed]
- SAS Institute. SAS Certified Professional Prep Guide: Advanced Programming Using SAS 9.4; SAS institute: Cary, NC, USA, 2019. [Google Scholar]
- Illinois Department of Healthcare and Family Services. Provider Notice: Fee-for-Service Claims—October 2023 Pricer Updates. Available online: https://hfs.illinois.gov/medicalproviders/notices/notice.prn231018a.html (accessed on 18 October 2023).
- Terwee, C.B.; Peipert, J.D.; Chapman, R.; Lai, J.S.; Terluin, B.; Cella, D.; Griffiths, P.; Mokkink, L.B. Minimal important change (MIC): A conceptual clarification and systematic review of MIC estimates of PROMIS measures. Qual. Life Res. 2021, 30, 2729–2754. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Sun, Y.; Li, D.; Liu, X.; Fang, C.; Yang, C.; Luo, T.; Lu, H.; Li, H.; Zhang, H. Acupuncture for breast cancer: A systematic review and meta-analysis of patient-reported outcomes. Front. Oncol. 2021, 11, 646315. [Google Scholar] [CrossRef] [PubMed]
- Choi, T.Y.; Ang, L.; Jun, J.H.; Alraek, T.; Birch, S.; Lu, W.; Lee, M.S. Acupuncture for Managing Cancer-Related Fatigue in Breast Cancer Patients: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 4419. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | Total (N = 62) | Acupuncture (n = 31) | Usual Care (n = 31) | p-Value |
|---|---|---|---|---|
| Age (years) | 55.2 (9.3) | 55.4 (9.1) | 55.1 (9.5) | 0.921 |
| Ethnicity | 0.534 | |||
| Hispanic/Latino | 13 (21.0%) | 8 (25.8%) | 5 (16.1%) | |
| Non-Hispanic | 48 (77.4%) | 23 (74.2%) | 25 (80.7%) | |
| Unknown | 1 (1.6%) | 0 (0.0%) | 1 (3.2%) | |
| Race | 0.620 | |||
| Black/African American | 34 (54.9%) | 15 (48.4%) | 19 (61.3%) | |
| White/Caucasian | 18 (29.0%) | 11 (35.5%) | 7 (22.5%) | |
| Asian | 3 (4.8%) | 1 (3.2%) | 2 (6.5%) | |
| American Indian/Alaska Native | 1 (1.6%) | 1 (3.2%) | 0 (0.0%) | |
| Unknown/other | 6 (9.7%) | 3 (9.7%) | 3 (9.7%) | |
| Education level | 0.942 | |||
| <High school | 4 (6.5%) | 2 (6.5%) | 2 (6.5%) | |
| High school graduate | 9 (14.5%) | 4 (12.9%) | 5 (16.1%) | |
| Some college | 17 (27.4%) | 7 (22.5%) | 10 (32.3%) | |
| Bachelor’s degree | 19 (30.6%) | 11 (35.5%) | 8 (25.8%) | |
| Some graduate school | 2 (3.2%) | 1 (3.2%) | 1 (3.2%) | |
| Graduate degree | 11 (17.7%) | 6 (19.4%) | 5 (16.1%) | |
| Marital status | 0.723 | |||
| Never married | 19 (30.6%) | 8 (25.8%) | 11 (35.5%) | |
| Married/living w/partner | 21 (33.9%) | 10 (32.3%) | 11 (35.5%) | |
| Divorced/separated | 17 (27.4%) | 10 (32.3%) | 7 (22.5%) | |
| Widowed | 5 (8.1%) | 3 (9.7%) | 2 (6.5%) | |
| Annual household income | 0.936 | |||
| <$35,000 | 23 (37.1%) | 12 (38.7%) | 11 (35.5%) | |
| $35,000–$54,999 | 16 (25.8%) | 8 (25.8%) | 8 (25.8%) | |
| $55,000–$100,000 | 15 (24.2%) | 8 (25.8%) | 7 (22.5%) | |
| >$100,000 | 8 (12.9%) | 3 (9.7%) | 5 (16.1%) | |
| Cancer stage | 0.674 | |||
| 0 | 2 (3.2%) | 1 (3.2%) | 1 (3.2%) | |
| I | 29 (46.8%) | 14 (45.2%) | 15 (48.4%) | |
| II | 22 (35.5%) | 13 (41.9%) | 9 (29.0%) | |
| III | 9 (14.5%) | 3 (9.7%) | 6 (19.4%) | |
| Treatment history a | ||||
| Chemotherapy | 40 (64.5%) | 20 (64.5%) | 20 (64.5%) | 1.000 |
| Radiation therapy | 50 (82.0%) | 24 (77.4%) | 26 (83.9%) | 0.749 |
| Endocrine therapy drug type | 0.321 | |||
| Anastrozole | 22 (35.5%) | 14 (45.2%) | 8 (25.8%) | |
| Exemestane | 9 (14.5%) | 5 (16.1%) | 4 (12.9%) | |
| Letrozole | 19 (30.6%) | 8 (25.8%) | 11 (35.5%) | |
| Tamoxifen | 12 (19.4%) | 4 (12.9%) | 8 (25.8%) | |
| Pain site a | ||||
| Joints, hands | 39 (62.9%) | 21 (67.7%) | 18 (58.1%) | 0.600 |
| Joints, knees | 38 (61.3%) | 20 (64.5%) | 18 (58.1%) | 0.795 |
| Joints, feet/ankles | 27 (43.5%) | 13 (41.9%) | 14 (45.2%) | 1.000 |
| Lower back | 32 (51.6%) | 16 (51.6%) | 16 (51.6%) | 1.000 |
| Legs | 24 (38.7%) | 15 (48.4%) | 9 (29.0%) | 0.192 |
| Arms | 28 (45.2%) | 15 (48.4%) | 13 (41.9%) | 0.799 |
| Breast/chest | 30 (48.4%) | 16 (51.6%) | 14 (45.2%) | 0.800 |
| Antidepressant use, yes | 20 (32.3%) | 12 (38.7%) | 8 (25.8%) | 0.416 |
| Comorbidity a | ||||
| Heart disease | 4 (6.5%) | 2 (6.5%) | 2 (6.5%) | 1.000 |
| Diabetes | 12 (19.4%) | 6 (19.4%) | 6 (19.4%) | 1.000 |
| High blood pressure | 31 (50.0%) | 15 (48.4%) | 16 (51.6%) | 1.000 |
| Liver disease | 1 (1.6%) | 0 (0.0%) | 1 (3.2%) | 1.000 |
| Kidney disease | 1 (1.6%) | 1 (3.2%) | 0 (0.0%) | 1.000 |
| BMI (kg/m2) | 32.0 (6.4) | 32.4 (6.2) | 31.6 (6.7) | 0.647 |
| Domain | Items | Mean (SD) |
|---|---|---|
| Feasibility | Recruitment rate | 20.7% |
| Retention rate | 90.3% | |
| Engagement/adherence rate | 93.1% | |
| Fidelity | 100% | |
| Acceptability | 1. Was participating in this study too hard? | 1.9 (0.4) |
| 2. Were the study instructions easy to understand? | 1.9 (0.3) | |
| 3. Did you feel rushed to complete this study? | 2.0 (0.0) | |
| 4. Did you enjoy being in this study? | 1.9 (0.3) | |
| 5. What do you think of getting acupuncture? | 1.8 (0.6) | |
| 6. Did you think acupuncture was painful? | 1.8 (0.4) | |
| 7. Would you get acupuncture again? | 2.0 (0.0) | |
| 8. Do you think this study will be well received by other breast cancer survivors? | 1.7 (0.4) | |
| 9. Do you think the length of the study period was | 1.6 (0.6) | |
| Total acceptability score | 16.6 (1.4) | |
| Acceptability rate | 92.8% |
| Symptom | Total (N = 62) | Acupuncture (n = 31) | Usual Care (n = 31) | p-Value a |
|---|---|---|---|---|
| Pain interference b | 58.9 (8.5) | 59.6 (8.5) | 58.2 (8.5) | 0.5014 |
| Fatigue b | 57.1 (8.2) | 57.7 (8.0) | 56.5 (8.5) | 0.5766 |
| Anxiety b | 55.7 (8.3) | 55.6 (8.1) | 55.7 (8.6) | 0.9410 |
| Depression b | 52.2 (8.6) | 53.7 (8.4) | 50.8 (8.6) | 0.1811 |
| Sleep disturbance b | 57.9 (8.6) | 58.4 (6.1) | 57.4 (10.6) | 0.6681 |
| Hot flash composite score | 50.0 (6.9) | 49.1 (2.2) | 50.9 (9.5) | 0.3199 |
| Symptom cluster composite score c | 55.3 (5.3) | 55.7 (4.3) | 54.9 (6.2) | 0.5781 |
| Mean Change from Baseline (95% CI) | Between-Group Difference (95% CI) | |||
|---|---|---|---|---|
| Acupuncture (N = 28) | Usual Care (N = 28) | Acupuncture vs. Usual Care | p-Value a | |
| Pain interference b | ||||
| Week 6 | −5.1 (−7.3 to −2.8) | −0.1 (−2.2 to 2.0) | −4.9 (−8.0 to −1.9) | 0.0018 |
| Week 12 | −6.3 (−8.5 to −4.1) | −0.9 (−3.1 to 1.3) | −5.4 (−8.5 to −2.3) | 0.0008 |
| Fatigue b | ||||
| Week 6 | −9.3 (−11.8 to −6.8) | −0.8 (−3.2 to 1.6) | −8.5 (−12.0 to −5.0) | <0.0001 |
| Week 12 | −5.7 (−8.2 to −3.2) | 0.9 (−1.6 to 3.3) | −6.6 (−10.1 to −3.1) | 0.0003 |
| Anxiety b | ||||
| Week 6 | −4.8 (−7.4 to −2.2) | 2.5 (0.02 to 4.9) | −7.3 (−10.8 to −3.7) | <0.0001 |
| Week 12 | −1.5 (−4.0 to 1.0) | −0.3 (−2.8 to 2.2) | −1.2 (−4.8 to 2.3) | 0.4988 |
| Depression b | ||||
| Week 6 | −5.2 (−7.7 to −2.7) | −0.6 (−3.0 to 1.8) | −4.6 (−8.1 to −1.1) | 0.01 |
| Week 12 | −2.7 (−5.2 to −0.2) | 2.5 (−0.004 to 4.9) | −5.1 (−8.6 to −1.6) | 0.0043 |
| Sleep disturbance b | ||||
| Week 6 | −7.1 (−10.1 to −4.2) | −0.9 (−3.7 to 1.9) | −6.2 (−10.2 to −2.2) | 0.003 |
| Week 12 | −5.5 (−8.4 to −2.7) | −0.8 (−3.6 to 2.1) | −4.8 (−8.8 to −0.7) | 0.022 |
| Hot flash composite score | ||||
| Week 6 | −1.1 (−2.4 to 0.2) | −0.5 (−1.8 to 0.7) | −0.6 (−2.4 to 1.2) | 0.5096 |
| Week 12 | −1.0 (−2.3 to 0.2) | −0.1 (−1.4 to 1.2) | −0.9 (−2.7 to 0.9) | 0.3138 |
| Symptom cluster composite score c | ||||
| Week 6 | −5.4 (−6.8 to −4.1) | −0.1 (−1.5 to 1.2) | −5.3 (−7.3 to −3.4) | <0.0001 |
| Week 12 | −3.8 (−5.2 to −2.4) | 0.2 (−1.2 to 1.5) | −4.0 (−5.9 to −2.0) | 0.0001 |
| Pain/fatigue/sleep disturbance symptom cluster d | ||||
| Week 6 | −7.2 (−9.1 to −5.3) | −0.6 (−2.4 to 1.2) | −6.6 (−9.2 to −4.0) | <0.0001 |
| Week 12 | −5.9 (−7.7 to −4.0) | −0.3 (−2.1 to 1.5) | −5.6 (−8.2 to −3.0) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, H.; Doorenbos, A.Z.; Chen, Z.; Choi, H.; Ma, W.; Danciu, O.; Patil, C.L.; Gao, S.; Lif, N.; Schlaeger, J.M. Feasibility and Acceptability of Integrating Acupuncture for Management of Multiple Symptoms in Medically Underserved Breast Cancer Survivors. Cancers 2025, 17, 304. https://doi.org/10.3390/cancers17020304
Li H, Doorenbos AZ, Chen Z, Choi H, Ma W, Danciu O, Patil CL, Gao S, Lif N, Schlaeger JM. Feasibility and Acceptability of Integrating Acupuncture for Management of Multiple Symptoms in Medically Underserved Breast Cancer Survivors. Cancers. 2025; 17(2):304. https://doi.org/10.3390/cancers17020304
Chicago/Turabian StyleLi, Hongjin, Ardith Z. Doorenbos, Zhengjia Chen, Hannah Choi, Weiwei Ma, Oana Danciu, Crystal L. Patil, Shuang Gao, Natalie Lif, and Judith M. Schlaeger. 2025. "Feasibility and Acceptability of Integrating Acupuncture for Management of Multiple Symptoms in Medically Underserved Breast Cancer Survivors" Cancers 17, no. 2: 304. https://doi.org/10.3390/cancers17020304
APA StyleLi, H., Doorenbos, A. Z., Chen, Z., Choi, H., Ma, W., Danciu, O., Patil, C. L., Gao, S., Lif, N., & Schlaeger, J. M. (2025). Feasibility and Acceptability of Integrating Acupuncture for Management of Multiple Symptoms in Medically Underserved Breast Cancer Survivors. Cancers, 17(2), 304. https://doi.org/10.3390/cancers17020304