
Immunotherapy and Advanced Vulvar Cancer: A Systematic Review and Meta-Analysis of Survival and Safety Outcomes

 ,
,  ,
,  and
and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
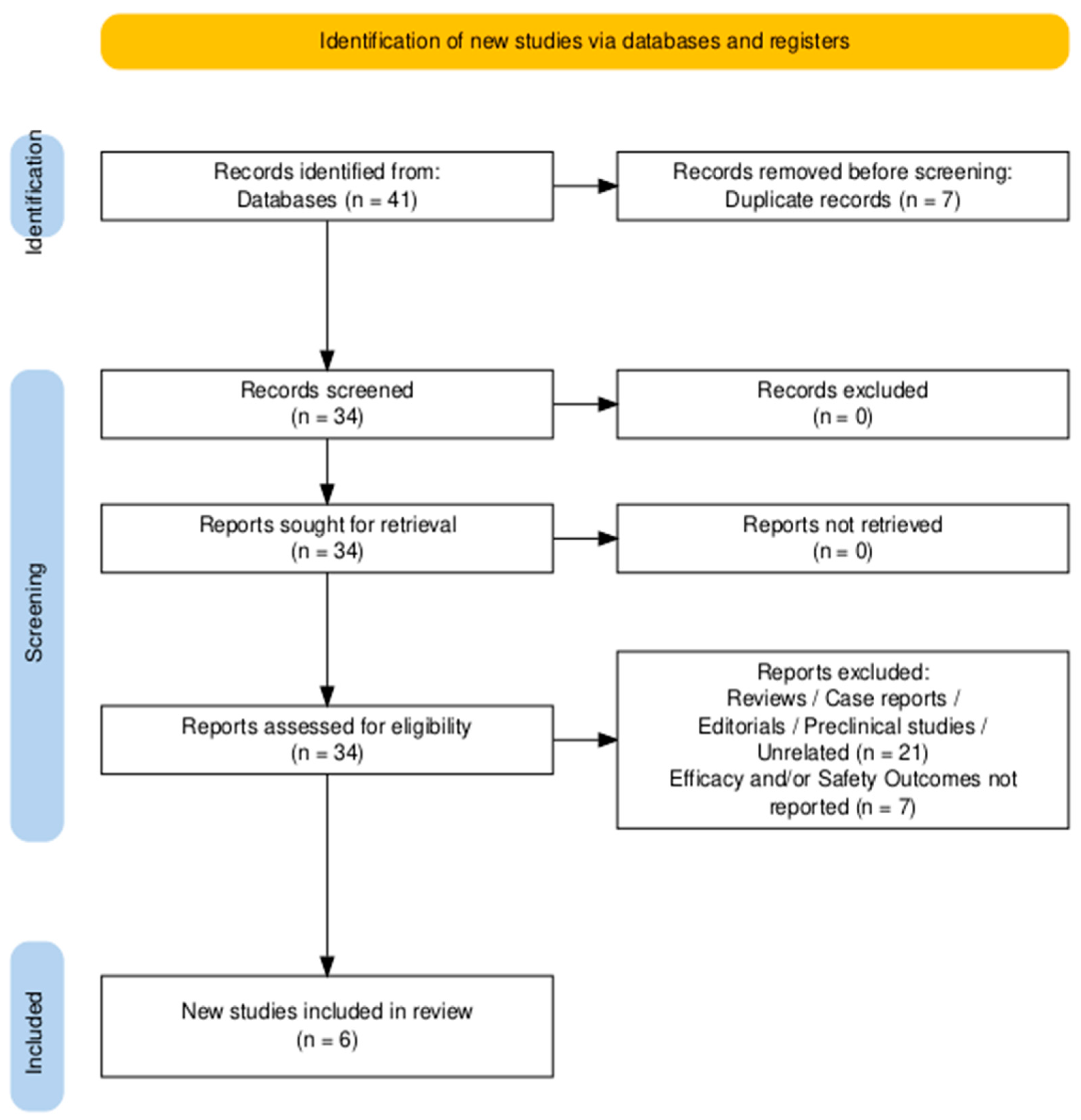
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection and Data Extraction
2.4. Data Extraction
2.5. Risk of Bias Assessment
2.6. Data Synthesis and Statistical Analysis
3. Results
3.1. Characteristics of the Included Studies and Main Overall Findings
3.2. Patient Population, Previous Therapies, and Intervention
3.3. Efficacy Outcomes
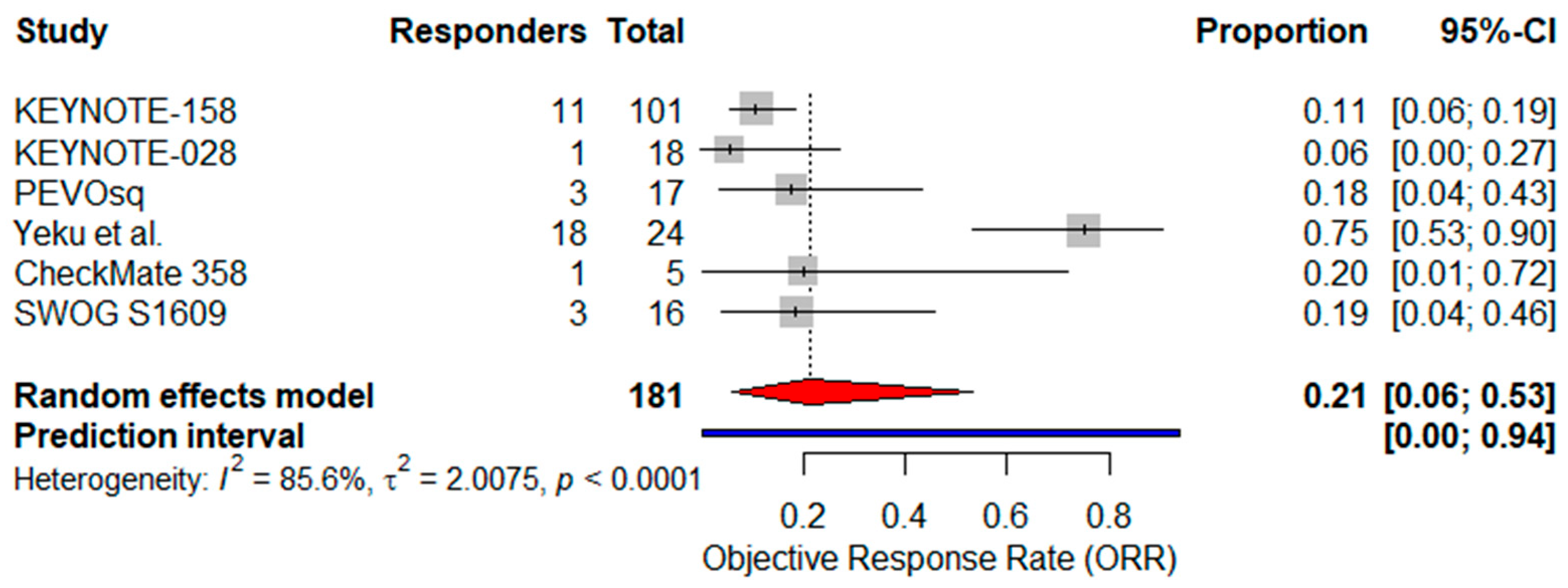
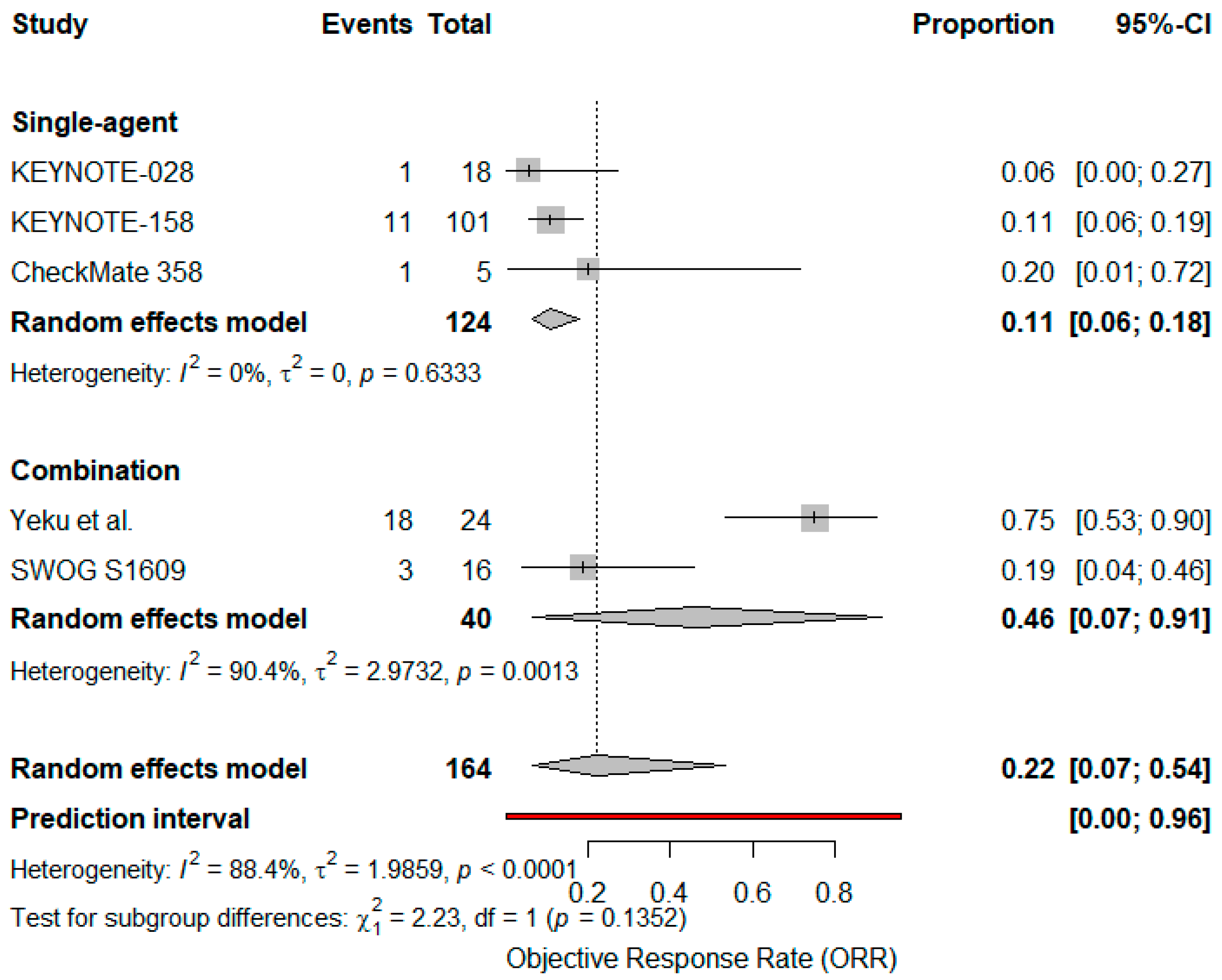
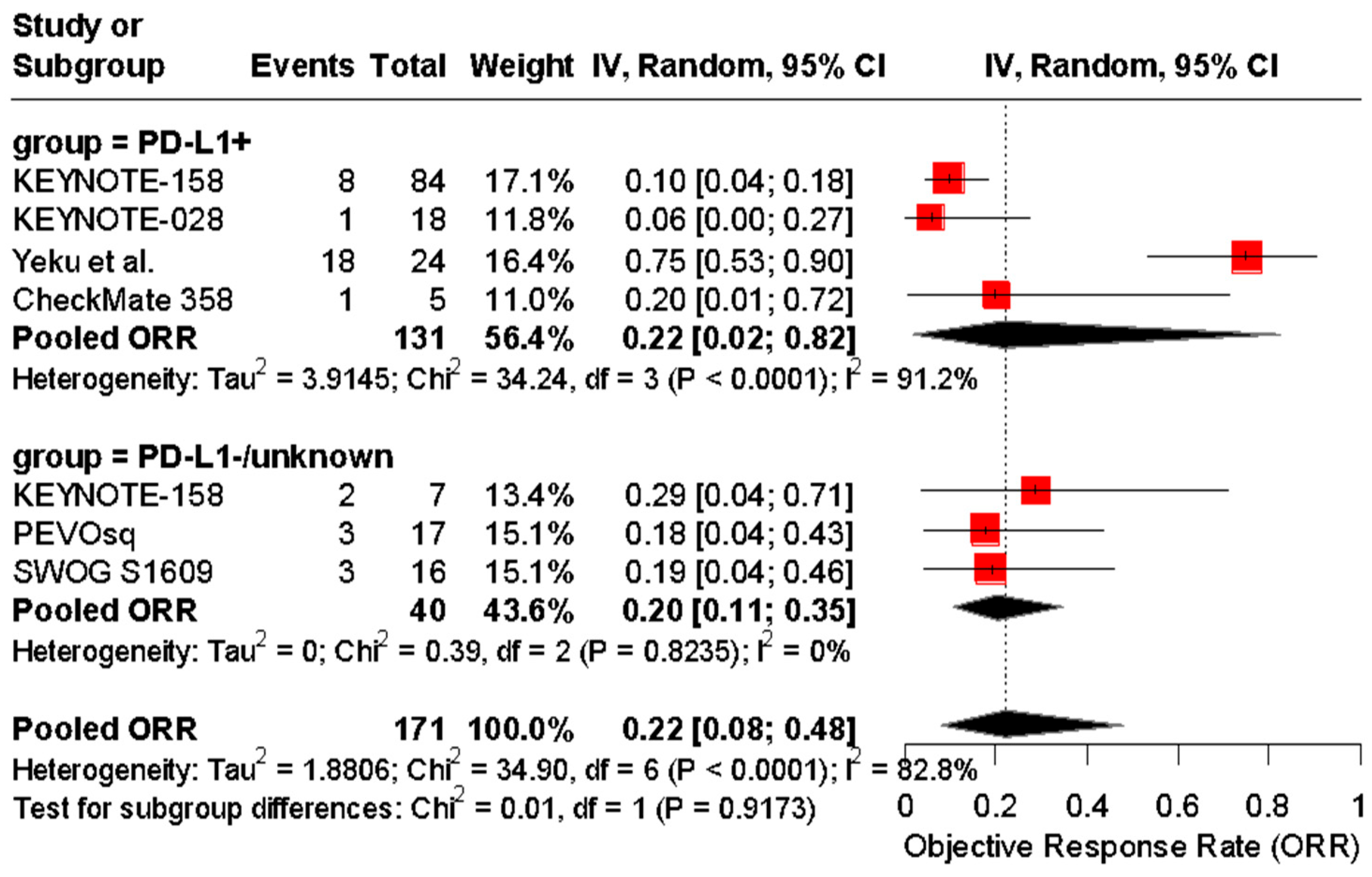
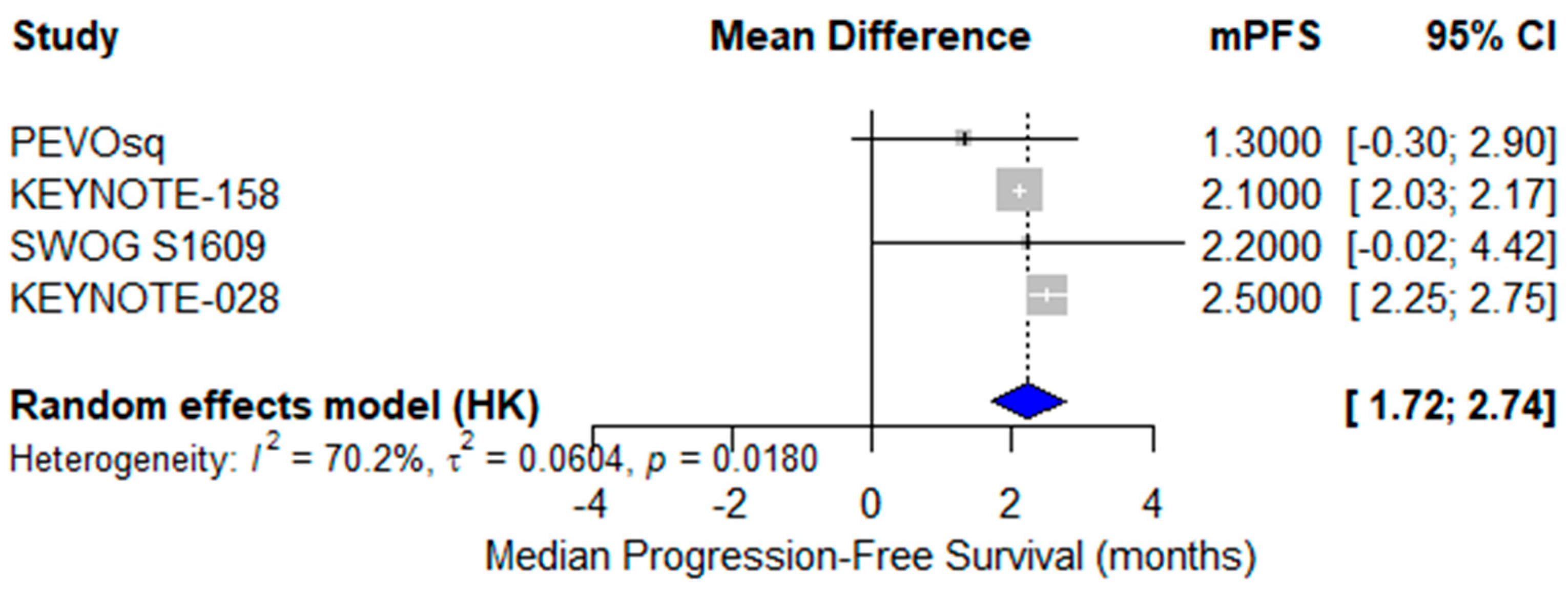
3.4. Pooled Analyses of ICIs’ Efficacy in VSCC
3.5. Safety Outcomes and Meta Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Cancer statistics for the year 2020: An overview. Int. J. Cancer 2021, 149, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Singhal, S.; Sharma, D.N.; Mathur, S.; Tomar, S.; Meena, J.; Singh, A.; Bhatla, N. Patterns of care for vulvar cancer and insights from revised FIGO staging: A retrospective study. World J. Surg. Oncol. 2024, 22, 329. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.; Li, L.; Yi, T.; Su, L.; Gao, Q.; Wu, L.; OuYang, Z. Epidemiologic characteristics and a prognostic nomogram for patients with vulvar cancer: Results from the Surveillance, Epidemiology, and End Results (SEER) program in the United States, 1975 to 2016. J. Gynecol. Oncol. 2023, 34, e81. [Google Scholar] [CrossRef] [PubMed]
- Pedrão, P.G.; Guimarães, Y.M.; Godoy, L.R.; Possati-Resende, J.C.; Bovo, A.C.; Andrade, C.E.M.C.; Longatto-Filho, A.; Dos Reis, R. Management of early-stage vulvar cancer. Cancers 2022, 14, 4184. [Google Scholar] [CrossRef] [PubMed]
- Li, J.Y.; Arkfeld, C.K.; Tymon-Rosario, J.; Webster, E.; Schwartz, P.; Damast, S.; Menderes, G. An evaluation of prognostic factors, oncologic outcomes, and management for primary and recurrent squamous cell carcinoma of the vulva. J. Gynecol. Oncol. 2022, 33, e13. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, H.; Hagerling, C.; Werb, Z. Roles of the immune system in cancer: From tumor initiation to metastatic progression. Genes Dev. 2018, 32, 1267–1284. [Google Scholar] [CrossRef] [PubMed]
- Gupta, I.; Hussein, O.; Sastry, K.S.; Bougarn, S.; Gopinath, N.; Chin-Smith, E.; Sinha, Y.; Korashy, H.M.; Maccalli, C. Deciphering the complexities of cancer cell immune evasion: Mechanisms and therapeutic implications. Adv. Cancer Biol. Metastasis 2023, 8, 100107. [Google Scholar] [CrossRef]
- Shiravand, Y.; Khodadadi, F.; Kashani, S.M.A.; Hosseini-Fard, S.R.; Hosseini, S.; Sadeghirad, H.; Ladwa, R.; O’Byrne, K.; Kulasinghe, A. Immune checkpoint inhibitors in cancer therapy. Curr. Oncol. 2022, 29, 3044–3060. [Google Scholar] [CrossRef] [PubMed]
- Manca, P.; Corti, F.; Intini, R.; Mazzoli, G.; Miceli, R.; Germani, M.M.; Bergamo, F.; Ambrosini, M.; Cristarella, E.; Cerantola, R.; et al. Tumor mutational burden as a biomarker in patients with mismatch repair-deficient/microsatellite instability-high metastatic colorectal cancer treated with immune checkpoint inhibitors. Eur. J. Cancer 2023, 187, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, H.; Watanabe, Y.; Arai, H.; Umemoto, K.; Tateishi, K.; Sunakawa, Y. Microsatellite instability: A 2024 update. Cancer Sci. 2024, 115, 1738–1748. [Google Scholar] [CrossRef] [PubMed]
- Fanale, D.; Dimino, A.; Pedone, E.; Brando, C.; Corsini, L.R.; Filorizzo, C.; Fiorino, A.; Lisanti, M.C.; Magrin, L.; Randazzo, U.; et al. Prognostic and predictive role of tumor-infiltrating lymphocytes (TILs) in ovarian cancer. Cancers 2022, 14, 4344. [Google Scholar] [CrossRef] [PubMed]
- Colombo, N.; Dubot, C.; Lorusso, D.; Caceres, M.V.; Hasegawa, K.; Shapira-Frommer, R.; Tewari, K.S.; Salman, P.; Hoyos Usta, E.; Yañez, E.; et al. Pembrolizumab for persistent, recurrent, or metastatic cervical cancer. N. Engl. J. Med. 2021, 385, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Harrington, K.J.; Burtness, B.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Brana, I.; Basté, N.; Neupane, P.; et al. Pembrolizumab with or without chemotherapy in recurrent or metastatic head and neck squamous cell carcinoma: Updated results of the Phase III KEYNOTE-048 Study. J. Clin. Oncol. 2023, 41, 790–802. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, D.; Xiang, Y.; Hasegawa, K.; Scambia, G.; Leiva, M.; Ramos-Elias, P.; Acevedo, A.; Cvek, J.; Randall, L.; de Santana Gomes, A.J.P.; et al. Pembrolizumab or placebo with chemoradiotherapy followed by pembrolizumab or placebo for newly diagnosed, high-risk, locally advanced cervical cancer (ENGOT-cx11/GOG-3047/KEYNOTE-A18): Overall survival results from a randomized, double-blind, placebo-controlled, phase 3 trial. Lancet 2024, 404, 1321–1332. [Google Scholar] [PubMed]
- Borella, F.; Preti, M.; Bertero, L.; Collemi, G.; Castellano, I.; Cassoni, P.; Cosma, S.; Carosso, A.R.; Bevilacqua, F.; Gallio, N.; et al. Is there a place for immune checkpoint inhibitors in vulvar neoplasms? A state-of-the-art review. Int. J. Mol. Sci. 2020, 22, 190. [Google Scholar] [CrossRef] [PubMed]
- Kortekaas, K.E.; Santegoets, S.J.; Abdulrahman, Z.; van Ham, V.J.; van der Tol, M.; Ehsan, I.; van Doorn, H.C.; Bosse, T.; van Poelgeest, M.I.E.; van der Burg, S.H. High numbers of activated helper T cells are associated with better clinical outcome in early stage vulvar cancer, irrespective of HPV or p53 status. J. Immunother. Cancer 2019, 7, 236. [Google Scholar] [CrossRef] [PubMed]
- Sznurkowski, J.J.; Zawrocki, A.; Emerich, J.; Sznurkowska, K.; Biernat, W. Expression of indoleamine 2,3-dioxygenase predicts shorter survival in patients with vulvar squamous cell carcinoma (vSCC) not influencing the recruitment of FOXP3-expressing regulatory T cells in cancer nests. Gynecol. Oncol. 2011, 122, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.-S.; Lee, S.-M.; Kim, M.-K.; Park, S.-G.; Choi, I.-W.; Choi, I.; Joo, Y.-D.; Park, S.-J.; Kang, S.-W.; Seo, S.-K. The tryptophan metabolite 3-hydroxyanthranilic acid suppresses T cell responses by inhibiting dendritic cell activation. Int. Immunopharmacol. 2013, 17, 721–726. [Google Scholar] [CrossRef] [PubMed]
- Chinn, Z.; Stoler, M.H.; Mills, A.M. PD-L1 and IDO expression in cervical and vulvar invasive and intraepithelial squamous neoplasias: Implications for combination immunotherapy. Histopathology 2019, 74, 256–268. [Google Scholar] [CrossRef] [PubMed]
- Boujelbene, N.; Ben Yahia, H.; Babay, W.; Gadria, S.; Zemni, I.; Azaiez, H.; Dhouioui, S.; Zidi, N.; Mchiri, R.; Mrad, K.; et al. HLA-G, HLA-E, and IDO overexpression predicts a worse survival of Tunisian patients with vulvar squamous cell carcinoma. HLA 2019, 94, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Karoń, P.; Olejek, A.; Olszak-Wąsik, K. TGF-β expression in vulvar cancer. Pol. Gynaecol. 2014, 85, 847–851. [Google Scholar] [CrossRef] [PubMed]
- Hecking, T.; Thiesler, T.; Schiller, C.; Lunkenheimer, J.-M.; Ayub, T.H.; Rohr, A.; Condic, M.; Keyver-Paik, M.-D.; Fimmers, R.; Kirfel, J.; et al. Tumoral PD-L1 expression defines a subgroup of poor-prognosis vulvar carcinomas with non-viral etiology. Oncotarget 2017, 8, 92890–92903. [Google Scholar] [CrossRef] [PubMed]
- Ott, P.A.; Bang, Y.J.; Piha-Paul, S.A.; Razak, A.R.A.; Bennouna, J.; Soria, J.C.; Rugo, H.S.; Cohen, R.B.; O’Neil, B.H.; Mehnert, J.M.; et al. T-cell-inflamed gene-expression profile, programmed death ligand 1 expression, and tumor mutational burden predict efficacy in patients treated with pembrolizumab across 20 cancers: KEYNOTE-028. J. Clin. Oncol. 2019, 37, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Naumann, R.W.; Hollebecque, A.; Meyer, T.; Devlin, M.J.; Oaknin, A.; Kerger, J.; López-Picazo, J.M.; Machiels, J.-P.; Delord, J.-P.; Evans, T.R.J.; et al. Safety and efficacy of nivolumab monotherapy in recurrent or metastatic cervical, vaginal, or vulvar carcinoma: Results from the Phase I/II CheckMate 358 Trial. J. Clin. Oncol. 2019, 37, 2825–2834. [Google Scholar] [CrossRef] [PubMed]
- Marcus, L.; Fashoyin-Aje, L.A.; Donoghue, M.; Yuan, M.; Rodriguez, L.; Gallagher, P.S.; Philip, R.; Ghosh, S.; Theoret, M.R.; Beaver, J.A.; et al. FDA approval summary: Pembrolizumab for the treatment of tumor mutational burden-high solid tumors. Clin. Cancer Res. 2021, 27, 4685–4689. [Google Scholar] [CrossRef] [PubMed]
- Abu-Rustum, N.R.; Yashar, C.M.; Arend, R.; Barber, E.; Bradley, K.; Brooks, R.; Campos, S.M.; Chino, J.; Chon, H.S.; Crispens, M.A.; et al. Vulvar cancer, version 3.2024, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2024, 22, 117–135. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Cochran, W.G. The comparison of percentages in matched samples. Biometrika 1950, 37, 256–266. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows; Version 24.0; IBM Corp: Armonk, NY, USA, 2016. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 9 March 2025).
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]
- Shapira-Frommer, R.; Mileshkin, L.; Manzyuk, L.; Penel, N.; Burge, M.; Piha-Paul, S.A.; Girda, E.; Martin, J.A.L.; Van Dongen, M.G.; Italiano, A.; et al. Efficacy and safety of pembrolizumab for patients with previously treated advanced vulvar squamous cell carcinoma: Results from the phase 2 KEYNOTE-158 study. Gynecol. Oncol. 2022, 166, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Saint-Ghislain, M.; Abdeddaim, C.; Chaltiel, R.; Cousin, S.; Gomez-Roca, C.; Borel, C.; Ghiringhelli, F.; Vansteene, D.; Bigot, F.; Jeannot, E.; et al. 758P Phase II trial evaluating the efficacy of pembrolizumab combined with vorinostat in patients with recurrent and/or metastatic vulvar and vaginal squamous cell carcinoma: Subgroup analysis of the PEVOsq basket trial. Ann. Oncol. 2023, 34, S518. [Google Scholar] [CrossRef]
- Yeku, O.; Russo, A.L.; Lee, H.; Spriggs, D. A phase 2 study of combined chemo-immunotherapy with cisplatin-pembrolizumab and radiation for unresectable vulvar squamous cell carcinoma. J. Transl. Med. 2020, 18, 350. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.J.; Othus, M.; Patel, S.P.; Ryan, C.; Sangal, A.; Powers, B.; Budd, G.T.; Victor, A.I.; Hsueh, C.T.; Chugh, R.; et al. Multicenter phase II trial (SWOG S1609, cohort 51) of ipilimumab and nivolumab in metastatic or unresectable angiosarcoma: A substudy of dual anti-CTLA-4 and anti-PD-1 blockade in rare tumors (DART). J. Immunother. Cancer 2021, 9, e002990. [Google Scholar] [CrossRef] [PubMed]
- Schwab, R.; Schiestl, L.J.; Cascant Ortolano, L.; Klecker, P.H.; Schmidt, M.W.; Almstedt, K.; Heimes, A.-S.; Brenner, W.; Stewen, K.; Schmidt, M.; et al. Efficacy of pembrolizumab in advanced cancer of the vulva: A systematic review and single-arm meta-analysis. Front. Oncol. 2024, 14, 1352975. [Google Scholar] [CrossRef] [PubMed]
- Tewari, K.S.; Monk, B.J.; Vergote, I.; Miller, A.; de Melo, A.C.; Kim, H.-S.; Kim, Y.M.; Lisyanskaya, A.; Samouëlian, V.; Lorusso, D.; et al. Investigators for GOG Protocol 3016 and ENGOT Protocol En-Cx9. Survival with cemiplimab in recurrent cervical cancer. N. Engl. J. Med. 2022, 386, 544–555. [Google Scholar] [CrossRef] [PubMed]
- Flindris, S.; Margioula-Siarkou, C.; Chalitsios, C.V.; Margioula-Siarkou, G.; Almperi, E.-A.; Almperis, A.; Styliara, E.; Flindris, K.; Paschopoulos, M.; Navrozoglou, I.; et al. Positivity Rate of PD-L1 Expression and Its Clinical Significance in Vulvar Cancer: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2025, 26, 4594. [Google Scholar] [CrossRef] [PubMed]
- Sznurkowski, J.J.; Żawrocki, A.; Sznurkowska, K.; Pęksa, R.; Biernat, W. PD-L1 expression on immune cells is a favorable prognostic factor for vulvar squamous cell carcinoma patients. Oncotarget 2017, 8, 89903–89912. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Tan, Y.; Zhu, L.X.; Zhou, L.N.; Zeng, P.; Liu, Q.; Chen, M.B.; Tian, Y. Prognostic value of HPV DNA status in cervical cancer before treatment: A systematic review and meta-analysis. Oncotarget 2017, 8, 66352–66359. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, Y.; Zhang, Z. Prevalence of human papillomavirus and its prognostic value in vulvar cancer: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0204162. [Google Scholar] [CrossRef] [PubMed]
- Marabelle, A.; Cassier, P.A.; Fakih, M.; Kao, S.; Nielsen, D.; Italiano, A.; Guren, T.K.; van Dongen, M.G.J.; Spencer, K.; Bariani, G.M.; et al. Pembrolizumab for previously treated advanced anal squamous cell carcinoma: Results from the non-randomised, multicohort, multicentre, phase 2 KEYNOTE-158 study. Lancet Gastroenterol. Hepatol. 2022, 7, 446–454. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Phase/Design | Population | PD-L1 | Intervention | Efficacy | Safety | Key Findings |
|---|---|---|---|---|---|---|---|
| KEYNOTE-158 [37] | II, single arm | 101 advanced (metastatic, unresectable) VSCC Median age 64 (31–87) 88.1% stage IV 19.8% M0 II 3% III 10% | 84 PD-L1+ 7 PD-L1− 10 unknown | Pembrolizumab (200 mg IV q3w up to 35 cycles or 2 yrs) | ORR 10.9% (1 CR 10 PR) PD-L1+: ORR 9.5% PD-L1−: ORR 28.6% mPFS 2.1 months mOS 6.2 months mDoR 20.4 months | 50.5% AEs 11.9% G3–5 (2 deaths) | Durable responses in a subset of patients regardless of PD-L1 status. |
| KEYNOTE-028 [24] | Ib, single arm | 18 advanced (metastatic, unresectable) VSCC | PD-L1+ | Pembrolizumab (10 mg/kg q2w for up to 2 yrs) | ORR 5.6% mPFS 2.5 months mOS 3.7 months mDoR 3.9 months | 66% AEs 14% ≥ G3 4% TD | Higher PD-L1 expression correlated with better ORR and PFS |
| PEVOsq basket trial [38] | II, single arm | 17 advanced VSCC Median age 63 (40–85) 14 metastatic 3 relapsed (unresectable) | NA | Pembrolizumab (200 mg q3w IV) with vorinostat (400 mg QD PO) FIRST LINE | ORR 18.8% (1 CR and 2 PR) mPFS 1.3 months mOS 17.5 months | 23.5% G3/4 AEs | Encouraging efficacy in VSCC |
| Yeku et al. [39] | II, single arm | 24 advanced VSCC 22 unresectable 2 recurrent | PD-L1+ | Pembrolizumab (200 mg q3w IV) with cisplatin and RT | ORR 75% 6-month RFS rate 70% mPFS NR | 78.6% G3/4 AEs | Combined pembrolizumab improved ORR and 6-month RFS |
| CheckMate 358 [25] | I/II, single arm | 5 advanced (locally, metastatic) VSCC Median age 59 (40–78) 1 IIB 1 IIIB/C 3 IVA/B 2 HPV+ 3 HPV− | PD-L1+ | Nivolumab (240 mg IV q2w) 1 first line 4 one or 2 prior lines (Platinum) | ORR 20% (1 PR, 3 SD) DCR 80% mDoR 5 months 6-month PFS rate 40.0% 12-month OS rate 40% 18-month OS rate 20.0% | 100% G1–2 AEs 0% G3–5 | Encouraging responses from Nivolumab monotherapy, additional investigation warranted |
| SWOG S1609 trial [40] | II, single arm | 16 advanced VSCC Median age 55.5 | NA | Nivolumab (240 mg IV q2w) with ipilimumab (1 mg/kg IV q6w) | ORR 18.8% mPFS 2.2 months mOS 7.6 months | G1/2 25% G3/4 25% G5 6.7% (1 death) | Objective responses lasting over 1 year |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maiorano, M.F.P.; Loizzi, V.; Cormio, G.; Maiorano, B.A. Immunotherapy and Advanced Vulvar Cancer: A Systematic Review and Meta-Analysis of Survival and Safety Outcomes. Cancers 2025, 17, 2392. https://doi.org/10.3390/cancers17142392
Maiorano MFP, Loizzi V, Cormio G, Maiorano BA. Immunotherapy and Advanced Vulvar Cancer: A Systematic Review and Meta-Analysis of Survival and Safety Outcomes. Cancers. 2025; 17(14):2392. https://doi.org/10.3390/cancers17142392
Chicago/Turabian StyleMaiorano, Mauro Francesco Pio, Vera Loizzi, Gennaro Cormio, and Brigida Anna Maiorano. 2025. "Immunotherapy and Advanced Vulvar Cancer: A Systematic Review and Meta-Analysis of Survival and Safety Outcomes" Cancers 17, no. 14: 2392. https://doi.org/10.3390/cancers17142392
APA StyleMaiorano, M. F. P., Loizzi, V., Cormio, G., & Maiorano, B. A. (2025). Immunotherapy and Advanced Vulvar Cancer: A Systematic Review and Meta-Analysis of Survival and Safety Outcomes. Cancers, 17(14), 2392. https://doi.org/10.3390/cancers17142392