
Prevalence and Risk Factors of Oropharyngeal Dysphagia in Newly Diagnosed Head-and-Neck Cancer Patients


 , ,
, ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Demographic and Oncological Data Collection
2.3. Screening for Oropharyngeal Dysphagia and Malnutrition
2.4. Statistical Analysis
3. Results
3.1. Study Design and Participants
3.2. Patient Demographic and Oncological Characteristics
3.3. Prevalence of Being at Risk of Oropharyngeal Dysphagia and Malnutrition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pezzuto, F.; Buonaguro, L.; Caponigro, F.; Ionna, F.; Starita, N.; Annunziata, C.; Buonaguro, F.M.; Tornesello, M.L. Update on Head and Neck Cancer: Current Knowledge on Epidemiology, Risk Factors, Molecular Features and Novel Therapies. Oncology 2015, 89, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Barsouk, A.; Aluru, J.S.; Rawla, P.; Saginala, K.; Barsouk, A. Epidemiology, Risk Factors, and Prevention of Head and Neck Squamous Cell Carcinoma. Med. Sci. 2023, 11, 42. [Google Scholar] [CrossRef] [PubMed]
- IKNL. Hoofd-Halskanker. Available online: https://iknl.nl/ (accessed on 13 December 2024).
- Okuni, I.; Otsubo, Y.; Ebihara, S. Molecular and Neural Mechanism of Dysphagia Due to Cancer. Int. J. Mol. Sci. 2021, 22, 7033. [Google Scholar] [CrossRef]
- Wall, L.R.; Ward, E.C.; Cartmill, B.; Hill, A.J. Physiological changes to the swallowing mechanism following (chemo)radiotherapy for head and neck cancer: A systematic review. Dysphagia 2013, 28, 481–493. [Google Scholar] [CrossRef]
- Baijens, L.W.J.; Walshe, M.; Aaltonen, L.M.; Arens, C.; Cordier, R.; Cras, P.; Crevier-Buchman, L.; Curtis, C.; Golusinski, W.; Govender, R.; et al. European white paper: Oropharyngeal dysphagia in head and neck cancer. Eur. Arch. Otorhinolaryngol. 2021, 278, 577–616. [Google Scholar] [CrossRef]
- Rommel, N.; Hamdy, S. Oropharyngeal dysphagia: Manifestations and diagnosis. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 49–59. [Google Scholar] [CrossRef]
- Alshadwi, A.; Nadershah, M.; Carlson, E.R.; Young, L.S.; Burke, P.A.; Daley, B.J. Nutritional considerations for head and neck cancer patients: A review of the literature. J. Oral. Maxillofac. Surg. 2013, 71, 1853–1860. [Google Scholar] [CrossRef]
- Chen, K.C.; Jeng, Y.; Wu, W.T.; Wang, T.G.; Han, D.S.; Ozcakar, L.; Chang, K.V. Sarcopenic Dysphagia: A Narrative Review from Diagnosis to Intervention. Nutrients 2021, 13, 4043. [Google Scholar] [CrossRef]
- Silva, P.B.; Ramos, G.H.A.; Petterle, R.R.; Borba, V.Z.C. Sarcopenia as an early complication of patients with head and neck cancer with dysphagia. Eur. J. Cancer Care 2021, 30, e13343. [Google Scholar] [CrossRef]
- Jones, E.; Speyer, R.; Kertscher, B.; Denman, D.; Swan, K.; Cordier, R. Health-Related Quality of Life and Oropharyngeal Dysphagia: A Systematic Review. Dysphagia 2018, 33, 141–172. [Google Scholar] [CrossRef]
- Kulbersh, B.D.; Rosenthal, E.L.; McGrew, B.M.; Duncan, R.D.; McColloch, N.L.; Carroll, W.R.; Magnuson, J.S. Pretreatment, preoperative swallowing exercises may improve dysphagia quality of life. Laryngoscope 2006, 116, 883–886. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.M.; Lawton, M. Dysphagia Advances in Head and Neck Cancer. Curr. Otorhinolaryngol. Rep. 2023, 11, 166–173. [Google Scholar] [CrossRef] [PubMed]
- Cates, D.J.; Evangelista, L.M.; Belafsky, P.C. Effect of Pretreatment Dysphagia on Postchemoradiation Swallowing Function in Head and Neck Cancer. Otolaryngol. Head. Neck Surg. 2022, 166, 506–510. [Google Scholar] [CrossRef]
- Wieland, M.W.M.; Pilz, W.; Winkens, B.; Hoeben, A.; Willemsen, A.C.H.; Kremer, B.; Baijens, L.W.J. Multi-Domain Screening: Identification of Patient’s Risk Profile Prior to Head-and-Neck Cancer Treatment. Cancers 2023, 15, 5254. [Google Scholar] [CrossRef]
- Belafsky, P.C.; Mouadeb, D.A.; Rees, C.J.; Pryor, J.C.; Postma, G.N.; Allen, J.; Leonard, R.J. Validity and reliability of the Eating Assessment Tool (EAT-10). Ann. Otol. Rhinol. Laryngol. 2008, 117, 919–924. [Google Scholar] [CrossRef]
- O’Sullivan, B.; Brierley, J.; Byrd, D.; Bosman, F.; Kehoe, S.; Kossary, C.; Pineros, M.; Van Eycken, E.; Weir, H.K.; Gospodarowicz, M. The TNM classification of malignant tumours-towards common understanding and reasonable expectations. Lancet Oncol. 2017, 18, 849–851. [Google Scholar] [CrossRef]
- van Overveld, L.F.; Braspenning, J.C.; Hermens, R.P. Quality indicators of integrated care for patients with head and neck cancer. Clin. Otolaryngol. 2017, 42, 322–329. [Google Scholar] [CrossRef]
- Singh, B.; Bhaya, M.; Stern, J.; Roland, J.T.; Zimbler, M.; Rosenfeld, R.M.; Har-El, G.; Lucente, F.E. Validation of the Charlson comorbidity index in patients with head and neck cancer: A multi-institutional study. Laryngoscope 1997, 107, 1469–1475. [Google Scholar] [CrossRef]
- The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [CrossRef]
- SONCOS. Normeringsrapport van SONCOS. 2024. Available online: https://www.soncos.org/#:~:text=HET%20NORMERINGSRAPPORT%20VAN%20SONCOS%20%2D%20VERSIE,het%20voorgaande%20jaar%20te%20vinden (accessed on 13 December 2024).
- Heijnen, B.J.; Speyer, R.; Kertscher, B.; Cordier, R.; Koetsenruijter, K.W.; Swan, K.; Bogaardt, H. Dysphagia, Speech, Voice, and Trismus following Radiotherapy and/or Chemotherapy in Patients with Head and Neck Carcinoma: Review of the Literature. Biomed. Res. Int. 2016, 2016, 6086894. [Google Scholar] [CrossRef]
- Kruizenga, H.B.S.; Huisman-de Waal, J.-S.C.; Klos, M.; Rmeijnse-Meester, W.; Thijs, A.; Tieland, M.; Vasse, E.; Witteman, B. Richtlijn Ondervoeding Herkenning, Diagnosestelling en Behandeling van Ondervoeding bij Volwassenen; Stuurgroep Ondervoeding: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Kruizenga, H.M.; Seidell, J.C.; de Vet, H.C.; Wierdsma, N.J.; van Bokhorst-de van der Schueren, M.A. Development and validation of a hospital screening tool for malnutrition: The short nutritional assessment questionnaire (SNAQ). Clin. Nutr. 2005, 24, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.H.; Yeh, K.Y.; Huang, J.S.; Lai, C.H.; Wu, T.H.; Lan, Y.J.; Tsai, J.C.; Chen, E.Y.; Yang, S.W.; Wang, C.H. Pretreatment performance status and nutrition are associated with early mortality of locally advanced head and neck cancer patients undergoing concurrent chemoradiation. Eur. Arch. Otorhinolaryngol. 2013, 270, 1909–1915. [Google Scholar] [CrossRef] [PubMed]
- Chalker, C.; Voutsinas, J.M.; Wu, Q.V.; Santana-Davila, R.; Hwang, V.; Baik, C.S.; Lee, S.; Barber, B.; Futran, N.D.; Houlton, J.J.; et al. Performance status (PS) as a predictor of poor response to immune checkpoint inhibitors (ICI) in recurrent/metastatic head and neck cancer (RMHNSCC) patients. Cancer Med. 2022, 11, 4104–4111. [Google Scholar] [CrossRef] [PubMed]
- Husmeela, H.; Kartini, A.; Zakinah, Y.; Sharifa Ezat, W.P.; Hasherah, M.I. The prevalence of Dysphagia among head and neck cancer patients in tertiary public hospitals in Malaysia. Med. J. Malays. 2021, 76, 837–844. [Google Scholar]
- Porto de Toledo, I.; Pantoja, L.L.Q.; Luchesi, K.F.; Assad, D.X.; De Luca Canto, G.; Guerra, E.N.S. Deglutition disorders as a consequence of head and neck cancer therapies: A systematic review and meta-analysis. Support. Care Cancer 2019, 27, 3681–3700. [Google Scholar] [CrossRef]
- Simon, S.R.; Pilz, W.; Hoebers, F.J.P.; Leeters, I.P.M.; Schols, A.; Willemsen, A.C.H.; Winkens, B.; Baijens, L.W.J. Malnutrition screening in head and neck cancer patients with oropharyngeal dysphagia. Clin. Nutr. ESPEN 2021, 44, 348–355. [Google Scholar] [CrossRef]
- Simon, S.R.; Florie, M.; Pilz, W.; Winkens, B.; Winter, N.; Kremer, B.; Baijens, L.W.J. Association Between Pharyngeal Pooling and Aspiration Using Fiberoptic Endoscopic Evaluation of Swallowing in Head and Neck Cancer Patients with Dysphagia. Dysphagia 2019, 35, 42–51. [Google Scholar] [CrossRef]
- Espitalier, F.; Fanous, A.; Aviv, J.; Bassiouny, S.; Desuter, G.; Nerurkar, N.; Postma, G.; Crevier-Buchman, L. International consensus (ICON) on assessment of oropharyngeal dysphagia. Eur. Ann. Otorhinolaryngol. Head. Neck Dis. 2018, 135, S17–S21. [Google Scholar] [CrossRef]
- Treanor, C.; Kyaw, T.; Donnelly, M. An international review and meta-analysis of prehabilitation compared to usual care for cancer patients. J. Cancer Surviv. 2018, 12, 64–73. [Google Scholar] [CrossRef]
- Orlandi, E.; Alfieri, S.; Simon, C.; Trama, A.; Licitra, L.; Group, R.A.W. Treatment challenges in and outside a network setting: Head and neck cancers. Eur. J. Surg. Oncol. 2019, 45, 40–45. [Google Scholar] [CrossRef]
- Miller, J.L.; Evers, J. Barriers to Adherence to Cancer Treatments Among Head and Neck Cancer Patients. J. Adv. Pract. Oncol. 2022, 13, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.J.; Benowitz, N.L. Current advances in research in treatment and recovery: Nicotine addiction. Sci. Adv. 2019, 5, eaay9763. [Google Scholar] [CrossRef] [PubMed]
- Denaro, N.; Merlano, M.C.; Russi, E.G. Dysphagia in Head and Neck Cancer Patients: Pretreatment Evaluation, Predictive Factors, and Assessment during Radio-Chemotherapy, Recommendations. Clin. Exp. Otorhinolaryngol. 2013, 6, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef]
- Frowen, J.; Hughes, R.; Skeat, J. The prevalence of patient-reported dysphagia and oral complications in cancer patients. Support. Care Cancer 2020, 28, 1141–1150. [Google Scholar] [CrossRef]
- Kenny, C.; Regan, J.; Balding, L.; Higgins, S.; O’Leary, N.; Kelleher, F.; McDermott, R.; Armstrong, J.; Mihai, A.; Tiernan, E.; et al. Dysphagia Prevalence and Predictors in Cancers Outside the Head, Neck, and Upper Gastrointestinal Tract. J. Pain. Symptom Manag. 2019, 58, 949–958.e2. [Google Scholar] [CrossRef]
- Cristofaro, M.G.; Barca, I.; Ferragina, F.; Novembre, D.; Ferro, Y.; Pujia, R.; Montalcini, T. The health risks of dysphagia for patients with head and neck cancer: A multicentre prospective observational study. J. Transl. Med. 2021, 19, 472. [Google Scholar] [CrossRef]
- Tagliaferri, S.; Lauretani, F.; Pela, G.; Meschi, T.; Maggio, M. The risk of dysphagia is associated with malnutrition and poor functional outcomes in a large population of outpatient older individuals. Clin. Nutr. 2019, 38, 2684–2689. [Google Scholar] [CrossRef]
- Ueshima, J.; Momosaki, R.; Shimizu, A.; Motokawa, K.; Sonoi, M.; Shirai, Y.; Uno, C.; Kokura, Y.; Shimizu, M.; Nishiyama, A.; et al. Nutritional Assessment in Adult Patients with Dysphagia: A Scoping Review. Nutrients 2021, 13, 778. [Google Scholar] [CrossRef]
- Linda Yarrow, J.M.G. Malnutrition: Risks & Concerns in Dysphagia Management. Perspect. Swallowing Swallowing Disord. (Dysphagia) 2010, 19, 115–120. [Google Scholar] [CrossRef]
- Seron-Arbeloa, C.; Labarta-Monzon, L.; Puzo-Foncillas, J.; Mallor-Bonet, T.; Lafita-Lopez, A.; Bueno-Vidales, N.; Montoro-Huguet, M. Malnutrition Screening and Assessment. Nutrients 2022, 14, 2392. [Google Scholar] [CrossRef] [PubMed]
- Florie, M.; Pilz, W.; Kremer, B.; Verhees, F.; Waltman, G.; Winkens, B.; Winter, N.; Baijens, L. EAT-10 Scores and Fiberoptic Endoscopic Evaluation of Swallowing in Head and Neck Cancer Patients. Laryngoscope 2021, 131, E45–E51. [Google Scholar] [CrossRef] [PubMed]
- Narasimhan, S.V.; Panarath, A. An Evaluation of Psychometric Properties of EAT-10: A Malayalam Version. Dysphagia 2024, 39, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Schindler, A.; de Fatima Lago Alvite, M.; Robles-Rodriguez, W.G.; Barcons, N.; Clave, P. History and Science behind the Eating Assessment Tool-10 (Eat-10): Lessons Learned. J. Nutr. Health Aging 2023, 27, 597–606. [Google Scholar] [CrossRef]
- Cordier, R.; Joosten, A.; Clave, P.; Schindler, A.; Bulow, M.; Demir, N.; Arslan, S.S.; Speyer, R. Evaluating the Psychometric Properties of the Eating Assessment Tool (EAT-10) Using Rasch Analysis. Dysphagia 2017, 32, 250–260. [Google Scholar] [CrossRef]
- Wilmskoetter, J.; Bonilha, H.; Hong, I.; Hazelwood, R.J.; Martin-Harris, B.; Velozo, C. Construct validity of the Eating Assessment Tool (EAT-10). Disabil. Rehabil. 2019, 41, 549–559. [Google Scholar] [CrossRef]
- Printza, A.; Kyrgidis, A.; Pavlidou, E.; Triaridis, S.; Constantinidis, J. Reliability and validity of the Eating Assessment Tool-10 (Greek adaptation) in neurogenic and head and neck cancer-related oropharyngeal dysphagia. Eur. Arch. Otorhinolaryngol. 2018, 275, 1861–1868. [Google Scholar] [CrossRef]
- Zhang, P.P.; Yuan, Y.; Lu, D.Z.; Li, T.T.; Zhang, H.; Wang, H.Y.; Wang, X.W. Diagnostic Accuracy of the Eating Assessment Tool-10 (EAT-10) in Screening Dysphagia: A Systematic Review and Meta-Analysis. Dysphagia 2023, 38, 145–158. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Diagnosis of HNC between December 2021 and May 2023 | Illiteracy or blindness |
| ≥18 years of age | Incomplete EAT-10 questionnaire |
| Informed consent | Diagnosis of incurable HNC |
| Diagnosis other than HNC (e.g., sarcoma, thyroid gland carcinoma, skin cancer, hematological malignancies, etc.) | |
| Refusal of oncological diagnostics/staging | |
| Cancer treatment or follow-up at other hospital |
| Variable | Completed EAT-10 | Not Completed EAT-10 | p-Value | |
|---|---|---|---|---|
| Age, N | N = 225 | N = 41 | ||
| Age < 70 years, N (%) | 136 (60.4%) | 26 (63.4%) | 0.244 d | |
| Age ≥ 70 years, N (%) | 89 (39.6%) | 15 (36.6%) | 0.774 a | |
| Mean (SD) | 66.8 (10.7) | 67.3 (9.9) | ||
| Sex, N | N = 225 | N = 41 | ||
| Male | 144 (64.0%) | 24 (58.5%) | 0.598 c | |
| Female | 81 (36.0%) | 17 (41.5%) | ||
| Tobacco consumption, N | N = 225 | N = 41 | ||
| Never | 37 (16.4%) | 6 (14.6%) | 0.956 d | |
| Former | 106 (47.1%) | 20 (48.8%) | 0.039 b | |
| Current | 82 (36.4%) | 15 (36.6%) | ||
| Number of pack years of smoking, median (IQR) | 25.5 (5.3–43.0) | 36.0 (21.5–55.0) | ||
| Alcohol consumption, N | N = 224 | N = 40 | ||
| Never | 59 (26.3%) | 8 (20.0%) | 0.276 d | |
| Former | 34 (15.2%) | 10 (25.0%) | 0.805 b | |
| Current | 131 (58.5%) | 22 (55.0%) | ||
| Number of alcoholic drinks per day, median (IQR) | 1.0 (0.3–3.0) | 0.7 (0.1–3.0) | ||
| Marital status, N | N = 220 | N = 38 | ||
| Single | 34 (15.5%) | 13 (34.2%) | 0.068 d | |
| Married | 136 (61.8%) | 20 (52.6%) | ||
| Divorced | 6 (2.7%) | 2 (5.3%) | ||
| Widower | 23 (10.5%) | 2 (5.3%) | ||
| Partner but not married | 21 (9.6%) | 1 (2.6%) | ||
| Occupation, N | N = 165 | N = 30 | ||
| Employed | 66 (40.0%) | 13 (43.3%) | 0.875 d | |
| Unemployed | 22 (13.3%) | 5 (16.7%) | ||
| Retired | 73 (44.2%) | 11 (36.7%) | ||
| Voluntary work | 4 (2.4%) | 1 (3.3%) | ||
| CCI grade, N | N = 224 | N = 40 | ||
| 0 No comorbidity | 108 (48.2%) | 18 (45.0%) | 0.301 d | |
| 1 Mild comorbidity | 73 (32.6%) | 10 (25.0%) | ||
| 2 Moderate comorbidity | 34 (15.2%) | 8 (20.0%) | ||
| 3 Severe comorbidity | 9 (4.0%) | 4 (10.0%) | ||
| PS, N | N = 224 | N = 40 | ||
| 0 Asymptomatic | 152 (67.9%) | 24 (60.0%) | 0.114 d | |
| 1 Symptomatic, fully ambulatory | 37 (16.5%) | 7 (17.5%) | ||
| 2 Symptomatic, in bed <50% of the day | 27 (12.1%) | 4 (10.0%) | ||
| 3 Symptomatic, in bed >50% of the day | 8 (3.6%) | 5 (12.5%) | ||
| 4 Completely disabled, bedridden | 0 (0%) | 0 (0%) | ||
| SNAQ, N | N = 220 | N = 4 | ||
| <2, N (%) | 181 (82.3%) | 2 (50.0%) | 0.154 c | |
| ≥2, N (%) | 39 (17.7%) | 2 (50.0%) | 0.086 e | |
| Median (IQR) | 0 (0–1.0) | 1.5 (0.3–3.5) | ||
| BMI, N | N = 224 | N = 39 | ||
| Not at risk of malnutrition: ≥20 kg/m2 if age < 70 y or ≥22 kg/m2 if age ≥ 70 y, N (%) | 192 (85.7%) | 34 (87.2%) | 0.901 d | |
| At risk of malnutrition: <20 kg/m2 if age < 70 y or <22 kg/m2 if age ≥ 70 y, N (%) | 32 (14.3%) | 5 (12.8%) | 0.799 a | |
| Mean (SD) | 25.8 (5.0) | 25.6 (4.7) | ||
| Primary tumor location, N (%) | N = 225 (84.6%) | N = 41 (15.4%) | ||
| Oral cavity | 77 (34.2%) | 12 (9.32%) | 0.834 d | |
| (Para)nasal cavity | 16 (7.1%) | 1 (2.4%) | ||
| Pharynx | 70 (31.1%) | 15 (36.6%) | ||
| Larynx | 45 (20.0%) | 10 (24.4%) | ||
| Salivary glands | 12 (5.3%) | 2 (4.9%) | ||
| Neck lymph node metastasis of unknown primary origin | 5 (2.2%) | 1 (2.4%) | ||
| T classification, N (%) | N = 225 (84.6%) | N = 41 (15.4%) | ||
| T0–1 | 76 (33.8%) | 18 (43.9%) | 0.367 d | |
| T2 | 58 (25.8%) | 6 (14.6%) | ||
| T3 | 31 (13.8%) | 5 (12.2%) | ||
| T4 | 60 (26.7%) | 12 (29.3%) | ||
| N classification, N (%) | N = 225 (84.6%) | N = 41 (15.4%) | ||
| N0 | 145 (64.4%) | 21 (51.2%) | 0.007 d | |
| N1 | 36 (16.0%) | 7 (17.0%) | ||
| N2 | 27 (12.0%) | 10 (24.3%) | ||
| N3 | 17 (7.6%) | 3 (7.3%) | ||
| M classification, N (%) | N = 223 (84.5%) | N = 41 (15.5%) | ||
| M0 | 222 (99.6%) | 41 (100%) | 0.667 d | |
| M1 (curable oligometastatic disease) | 1 (0.4%) | 0 (0.0%) | ||
| CSG, N (%) | N = 224 (84.5%) | N = 41 (15.5%) | ||
| 0–1 | 84 (37.5%) | 17 (41.5%) | 0.324 d | |
| 2 | 47 (21.0%) | 4 (9.8%) | ||
| 3 | 30 (13.4%) | 5 (12.2%) | ||
| 4 | 63 (28.1%) | 15 (36.6%) | ||
| HPV/p16, N (%) | N = 58 (25.7% of 225) | N = 11 (15.9% of 41) | ||
| Positive | 24 (41.4%) | 6 (54.5%) | 0.514 c | |
| Negative | 34 (58.6%) | 5 (45.5%) | ||
| EBV, N (%) | N = 13 (22.4% of 225) | N = 1 (7.1% of 41) | ||
| Positive | 8 (61.5%) | 0 (0%) | 0.429 c | |
| Negative | 5 (38.5%) | 1 (100.0%) |
| Groups | EAT-10 Median (IQR) | p-Value | EAT-10 ≥ 3, N (%) | p-Value |
|---|---|---|---|---|
| Age < 70 years (N = 136) | 0 (0–2) | 0.892 a | 29 (21.3) | 0.996 b |
| Age 70 years (N = 89) | 0 (0–2) | 19 (21.3) | ||
| Male (N = 144) | 0 (0–2) | 0.312 a | 29 (20.1) | 0.560 b |
| Female (N = 81) | 0 (0–2) | 19 (23.5) | ||
| CCI grade < 2 (N = 181) | 0 (0–2) | 0.982 a | 37 (20.3) | 0.450 b |
| CCI grade 2 (N = 43) | 0 (0–4) | 11 (25.6) | ||
| PS 0–1 (N = 189) | 0 (0–2) | 0.247 a | 38 (20.1) | 0.262 b |
| PS 2–3 (N = 35) | 0 (0–5) | 10 (28.6) | ||
| CSG 0–2 (N = 131) | 0 (0–1) | 0.030 a | 17 (13.0) | <0.001 b |
| CSG 3–4 (N = 93) | 0 (0–6) | 31 (33.3) | ||
| Oral cavity (N = 77) | 0 (0–1) | 0.020 a | 14 (18.2) | 0.014 b |
| Pharynx (N = 70) | 0.5 (0–6.5) | 23 (32.9) | ||
| Larynx (N = 45) | 0 (0–2) | 9 (20.0) | ||
| Other (N = 33) | 0 (0–0) | 2 (6.1) | ||
| Normal BMI c (N = 193) | 0 (0–1.5) | 0.004 a | 37 (19.2) | 0.052 b |
| Abnormal BMI c (N = 32) | 1.5 (0–12) | 11 (34.4) | ||
| SNAQ 2 (N = 181) | 0 (0–1) | <0.001 a | 26 (14.4) | <0.001 b |
| SNAQ 2 (N = 39) | 3 (0–19) | 20 (51.3) | ||
| No malnutrition risk d (N = 161) | 0 (0–1) | <0.001 a | 22 (13.7) | <0.001 b |
| Malnutrition risk d (N = 61) | 2 (0–11) | 25 (41.0) |
| Variable | OR (95% CI) | p-Value | Post Hoc OR (95% CI) | Post Hoc p-Value |
|---|---|---|---|---|
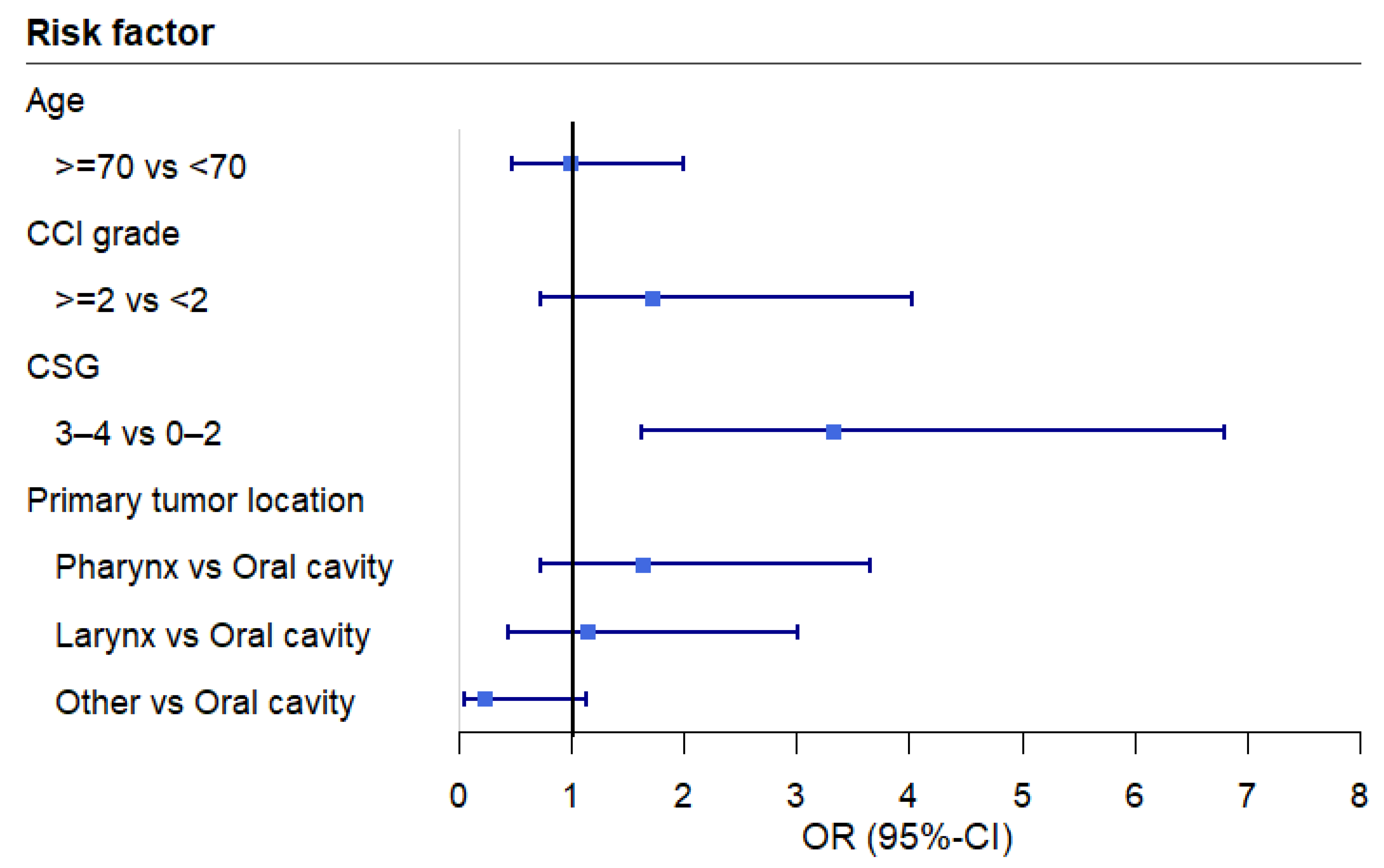
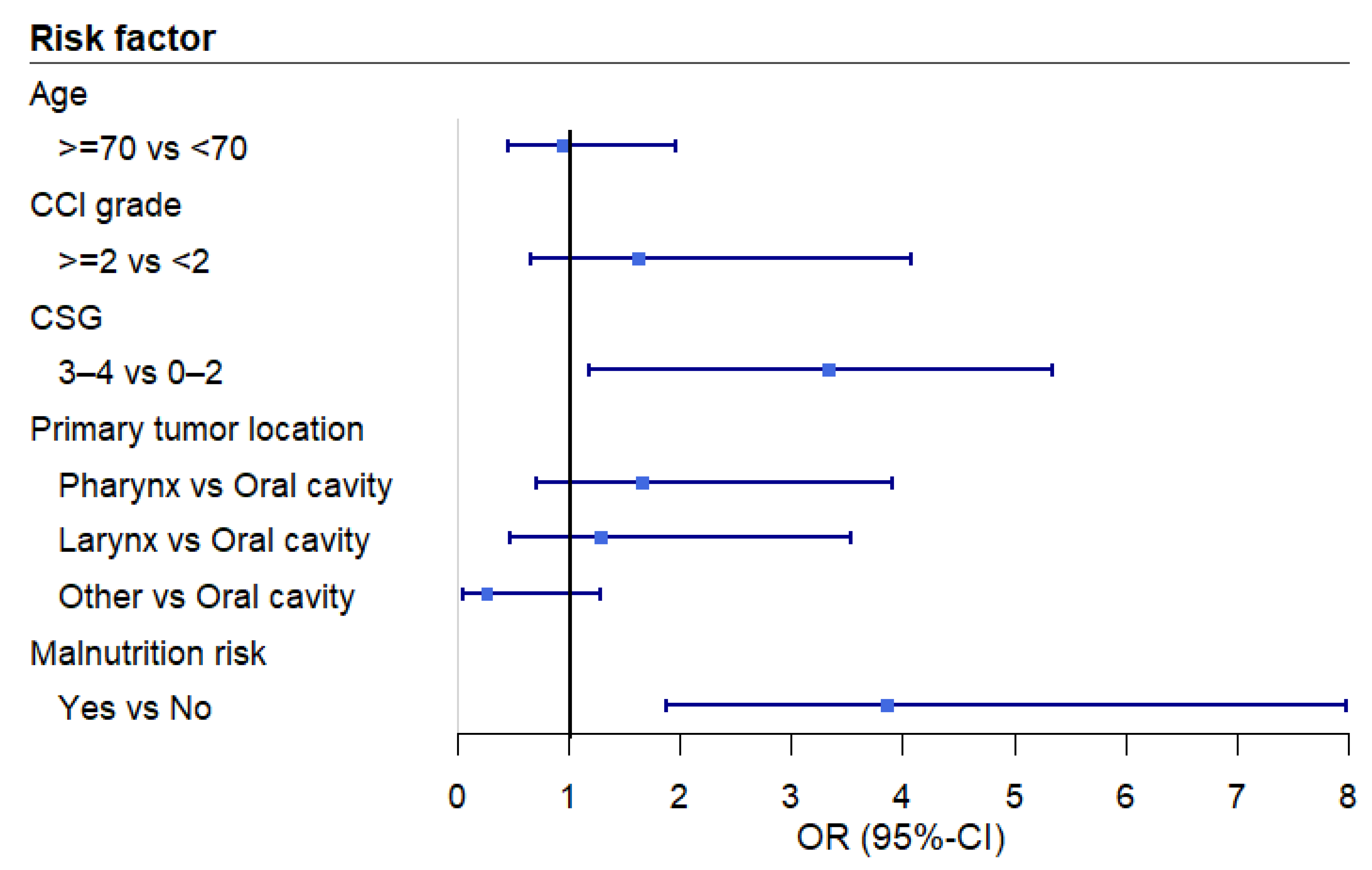
| Age | ||||
| <70 years | Reference | 0.945 | Reference | 0.861 |
| 70 years | 0.98 (0.48, 1.99) | 0.94 (0.45, 1.96) | ||
| CCI grade | ||||
| <2 | Reference | 0.224 | Reference | 0.292 |
| 2 | 1.71 (0.72–4.03) | 1.63 (0.66–4.07) | ||
| CSG | ||||
| 0–2 | Reference | <0.001 | Reference | 0.016 |
| 3–4 | 3.33 (1.63–6.80) | 3.33 (1.19–5.35) | ||
| Primary tumor location | 0.090 | 0.121 | ||
| Oral cavity | Reference | Reference | ||
| Pharynx | 1.63 (0.72–3.66) | 0.238 | 1.66 (0.71–3.90) | 0.243 |
| Larynx | 1.14 (0.43–3.01) | 0.788 | 1.29 (0.47–3.53) | 0.615 |
| Other | 0.23 (0.05–1.14) | 0.072 | 0.26 (0.05–1.28) | 0.097 |
| Malnutrition risk a | ||||
| No | Reference | <0.001 | ||
| Yes | 3.86 (1.87–7.99) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Florie, M.G.M.H.; Wieland, M.W.M.; Pilz, W.; Partoens, R.; Winkens, B.; Hoeben, A.; Rommel, N.; Baijens, L.W.J. Prevalence and Risk Factors of Oropharyngeal Dysphagia in Newly Diagnosed Head-and-Neck Cancer Patients. Cancers 2025, 17, 9. https://doi.org/10.3390/cancers17010009
Florie MGMH, Wieland MWM, Pilz W, Partoens R, Winkens B, Hoeben A, Rommel N, Baijens LWJ. Prevalence and Risk Factors of Oropharyngeal Dysphagia in Newly Diagnosed Head-and-Neck Cancer Patients. Cancers. 2025; 17(1):9. https://doi.org/10.3390/cancers17010009
Chicago/Turabian StyleFlorie, Michelle G. M. H., Monse W. M. Wieland, Walmari Pilz, Rosanne Partoens, Bjorn Winkens, Ann Hoeben, Nathalie Rommel, and Laura W. J. Baijens. 2025. "Prevalence and Risk Factors of Oropharyngeal Dysphagia in Newly Diagnosed Head-and-Neck Cancer Patients" Cancers 17, no. 1: 9. https://doi.org/10.3390/cancers17010009
APA StyleFlorie, M. G. M. H., Wieland, M. W. M., Pilz, W., Partoens, R., Winkens, B., Hoeben, A., Rommel, N., & Baijens, L. W. J. (2025). Prevalence and Risk Factors of Oropharyngeal Dysphagia in Newly Diagnosed Head-and-Neck Cancer Patients. Cancers, 17(1), 9. https://doi.org/10.3390/cancers17010009