
Prognostic Importance of Axillary Lymph Node Response to Neoadjuvant Systemic Therapy on Axillary Surgery in Breast Cancer—A Single Center Experience

 , , ,
, , ,  ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Treatment
2.2. Endpoints
2.3. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Treatment
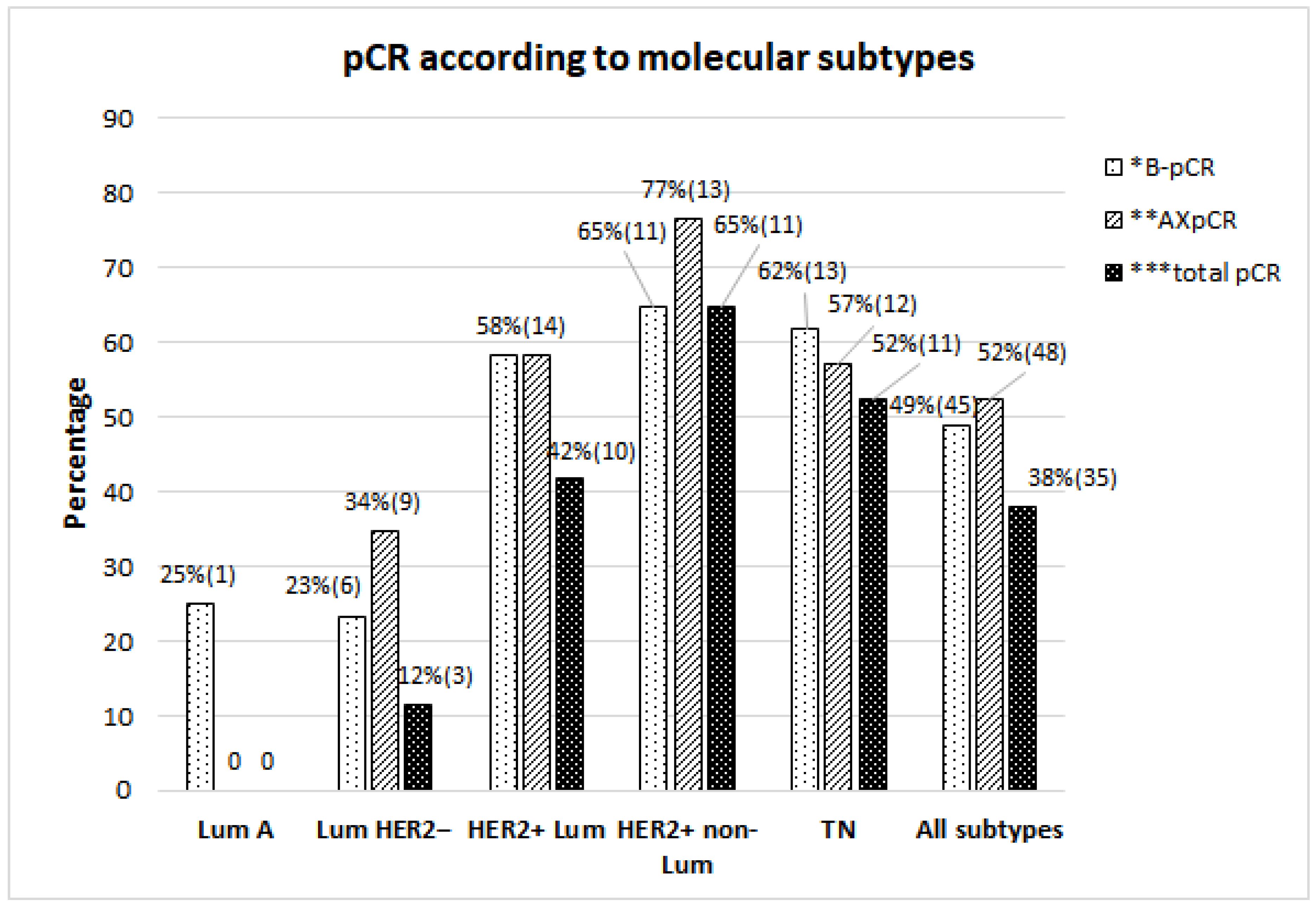
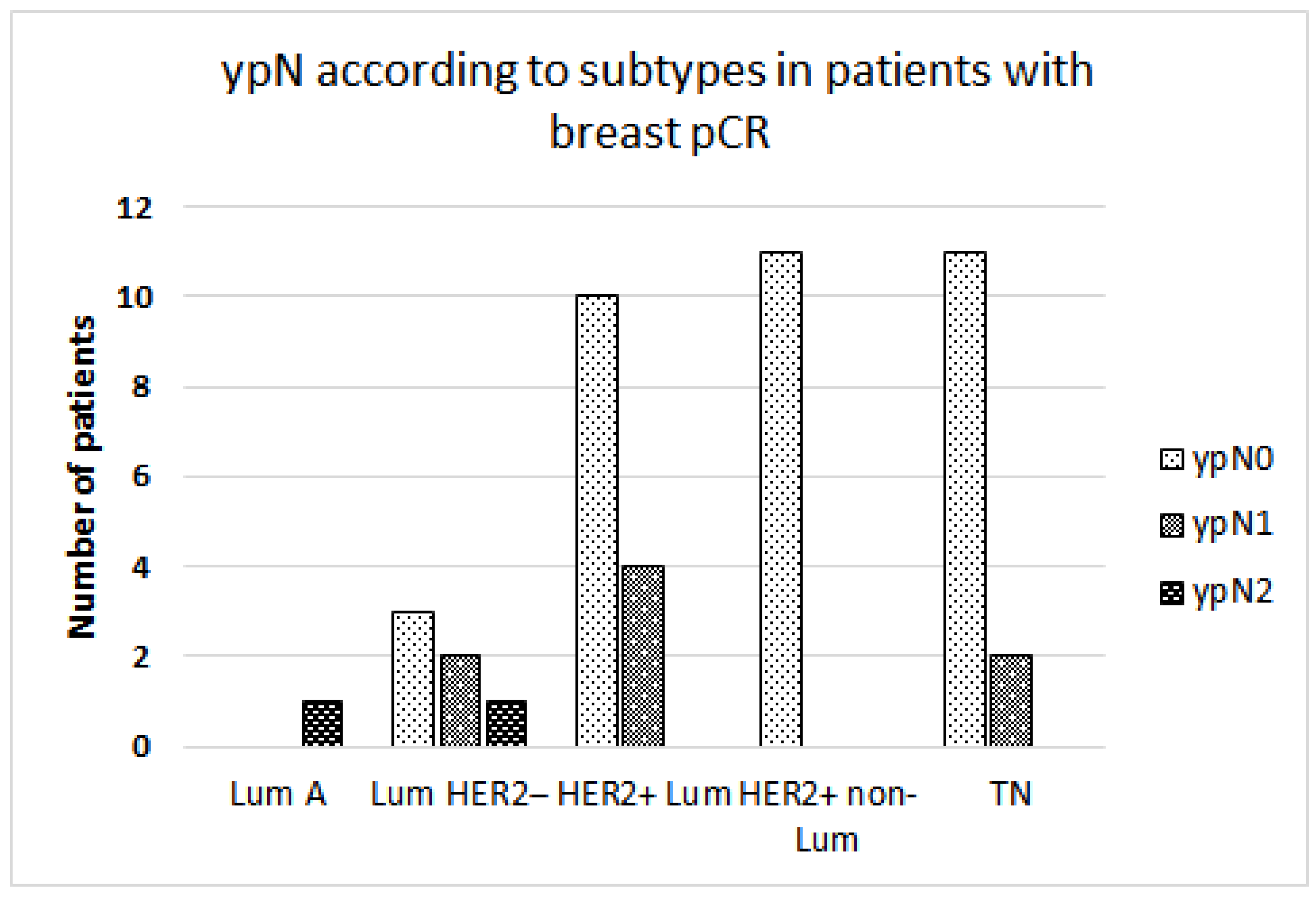
3.3. pCR According to Molecular Subtypes
3.4. Association of Clinical, Pathological, and Treatment Factors with AXpCR
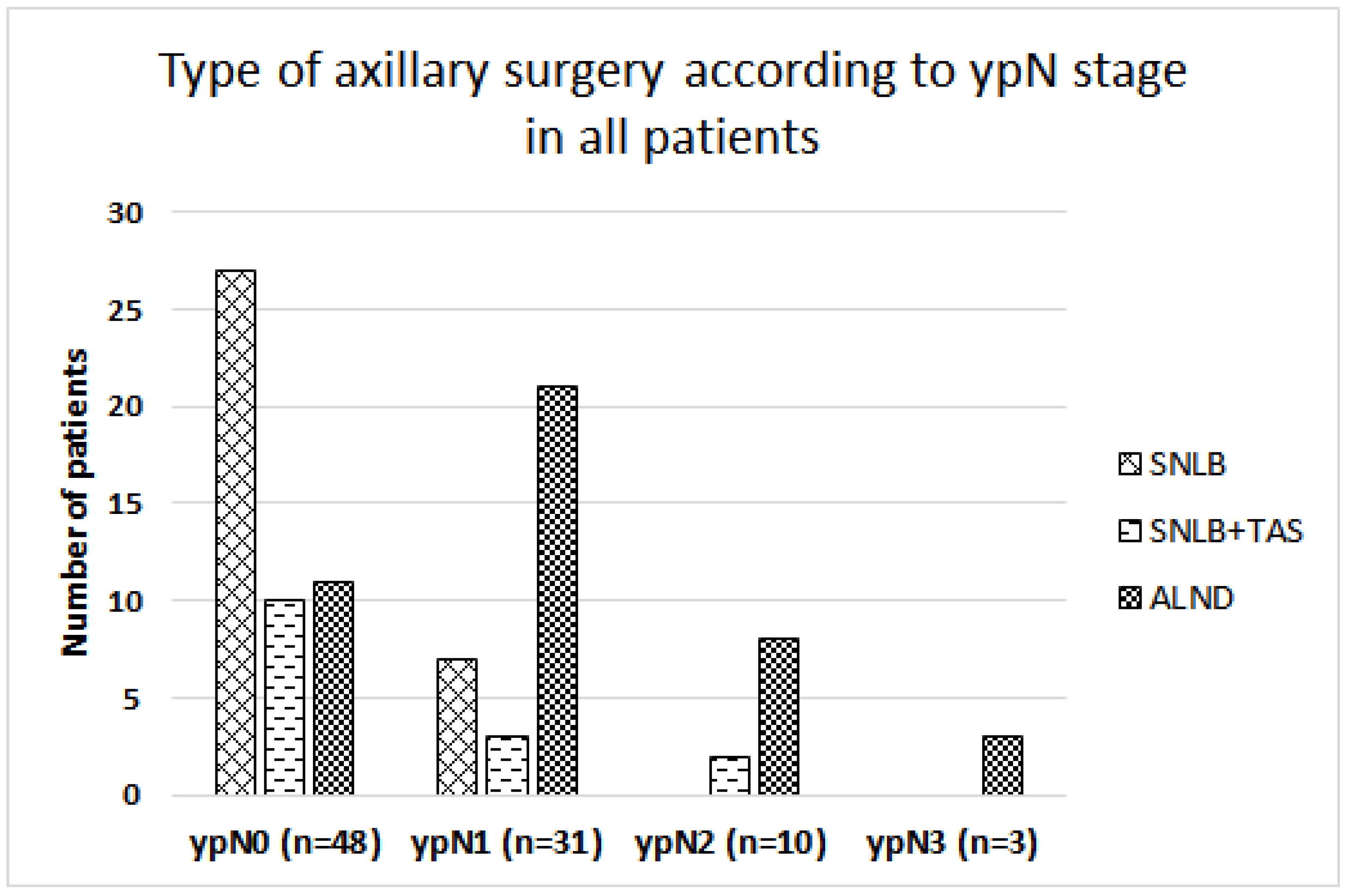
3.5. Surgical Treatment
3.6. Adjuvant Radiation Therapy
3.7. Relapse-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hennessy, B.T.; Hortobagyi, G.N.; Rouzier, R.; Kuerer, H.; Sneige, N.; Buzdar, A.U.; Kau, S.W.; Fornage, B.; Sahin, A.; Broglio, K.; et al. Outcome after pathologic complete eradication of cytologically proven breast cancer axillary node metastases following primary chemotherapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 9304–9311. [Google Scholar] [CrossRef]
- Bhargava, R.; Beriwal, S.; Dabbs, D.J.; Ozbek, U.; Soran, A.; Johnson, R.R.; Brufsky, A.M.; Lembersky, B.C.; Ahrendt, G.M. Immunohistochemical surrogate markers of breast cancer molecular classes predicts response to neoadjuvant chemotherapy: A single institutional experience with 359 cases. Cancer 2010, 116, 1431–1439. [Google Scholar] [CrossRef] [PubMed]
- Loibl, S.; Poortmans, P.; Morrow, M.; Denkert, C.; Curigliano, G. Breast cancer. Lancet 2021, 397, 1750–1769. [Google Scholar] [CrossRef]
- Boileau, J.F.; Poirier, B.; Basik, M.; Holloway, C.M.; Gaboury, L.; Sideris, L.; Meterissian, S.; Arnaout, A.; Brackstone, M.; McCready, D.R.; et al. Sentinel node biopsy after neoadjuvant chemotherapy in biopsy-proven node-positive breast cancer: The SN FNAC study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Boughey, J.C.; Suman, V.J.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Leitch, A.M.; Kuerer, H.M.; Bowling, M.; Flippo-Morton, T.S.; et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: The ACOSOG Z1071 (Alliance) clinical trial. JAMA 2013, 310, 1455–1461. [Google Scholar] [CrossRef]
- Mamounas, E.P.; Brown, A.; Anderson, S.; Smith, R.; Julian, T.; Miller, B.; Bear, H.D.; Caldwell, C.B.; Walker, A.P.; Mikkelson, W.M.; et al. Sentinel node biopsy after neoadjuvant chemotherapy in breast cancer: Results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 2694–2702. [Google Scholar] [CrossRef] [PubMed]
- Classe, J.M.; Loaec, C.; Gimbergues, P.; Alran, S.; de Lara, C.T.; Dupre, P.F.; Rouzier, R.; Faure, C.; Paillocher, N.; Chauvet, M.P.; et al. Sentinel lymph node biopsy without axillary lymphadenectomy after neoadjuvant chemotherapy is accurate and safe for selected patients: The GANEA 2 study. Breast Cancer Res. Treat. 2019, 173, 343–352. [Google Scholar] [CrossRef]
- Kuehn, T.; Bauerfeind, I.; Fehm, T.; Fleige, B.; Hausschild, M.; Helms, G.; Lebeau, A.; Liedtke, C.; von Minckwitz, G.; Nekljudova, V.; et al. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): A prospective, multicentre cohort study. Lancet Oncol. 2013, 14, 609–618. [Google Scholar] [CrossRef]
- Caudle, A.S.; Yang, W.T.; Krishnamurthy, S.; Mittendorf, E.A.; Black, D.M.; Gilcrease, M.Z.; Bedrosian, I.; Hobbs, B.P.; DeSnyder, S.M.; Hwang, R.F.; et al. Improved Axillary Evaluation Following Neoadjuvant Therapy for Patients with Node-Positive Breast Cancer Using Selective Evaluation of Clipped Nodes: Implementation of Targeted Axillary Dissection. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 1072–1078. [Google Scholar] [CrossRef]
- Morgan, C.; Stringfellow, T.D.; Rolph, R.; Kovacs, T.; Kothari, A.; Pinder, S.E.; Hamed, H.; Sever, A.R. Neoadjuvant chemotherapy in patients with breast cancer: Does response in the breast predict axillary node response? Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2020, 46 Pt A, 522–526. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef]
- Coates, A.S.; Winer, E.P.; Goldhirsch, A.; Gelber, R.D.; Gnant, M.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.J. Tailoring therapies—Improving the management of early breast cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 1533–1546. [Google Scholar] [CrossRef] [PubMed]
- Masuda, N.; Lee, S.-J.; Ohtani, S.; Im, Y.-H.; Lee, E.-S.; Yokota, I.; Kuroi, K.; Im, S.-A.; Park, B.-W.; Kim, S.-B.; et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef] [PubMed]
- von Minckwitz, G.; Huang, C.-S.; Mano, M.S.; Loibl, S.; Mamounas, E.P.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N. Engl. J. Med. 2019, 380, 617–628. [Google Scholar] [CrossRef] [PubMed]
- Barron, A.U.; Hoskin, T.L.; Day, C.N.; Hwang, E.S.; Kuerer, H.M.; Boughey, J.C. Association of Low Nodal Positivity Rate Among Patients with ERBB2-Positive or Triple-Negative Breast Cancer and Breast Pathologic Complete Response to Neoadjuvant Chemotherapy. JAMA Surg. 2018, 153, 1120–1126. [Google Scholar] [CrossRef]
- Kolberg, H.C.; Kühn, T.; Krajewska, M.; Bauerfeind, I.; Fehm, T.N.; Fleige, B.; Helms, G.; Lebeau, A.; Stäbler, A.; Schmatloch, S.; et al. Residual Axillary Burden After Neoadjuvant Chemotherapy (NACT) in Early Breast Cancer in Patients with a priori Clinically Occult Nodal Metastases—A transSENTINA Analysis. Geburtshilfe Und Frauenheilkd. 2020, 80, 1229–1236. [Google Scholar] [CrossRef]
- Weiss, A.; Campbell, J.; Ballman, K.V.; Sikov, W.M.; Carey, L.A.; Hwang, E.S.; Poppe, M.M.; Partridge, A.H.; Ollila, D.W.; Golshan, M. Factors Associated with Nodal Pathologic Complete Response Among Breast Cancer Patients Treated with Neoadjuvant Chemotherapy: Results of CALGB 40601 (HER2+) and 40603 (Triple-Negative) (Alliance). Ann. Surg. Oncol. 2021, 28, 5960–5971. [Google Scholar] [CrossRef] [PubMed]
- Al-Hilli, Z.; Hoskin, T.L.; Day, C.N.; Habermann, E.B.; Boughey, J.C. Impact of Neoadjuvant Chemotherapy on Nodal Disease and Nodal Surgery by Tumor Subtype. Ann. Surg. Oncol. 2018, 25, 482–493. [Google Scholar] [CrossRef] [PubMed]
- Iwamoto, N.; Aruga, T.; Horiguchi, S.; Saita, C.; Onishi, M.; Goto, R.; Ishiba, T.; Honda, Y.; Miyamoto, H.; Kuroi, K. Predictive factors of an axillary pathological complete response of node-positive breast cancer to neoadjuvant chemotherapy. Surg. Today 2020, 50, 178–184. [Google Scholar] [CrossRef]
- Schneeweiss, A.; Chia, S.; Hickish, T.; Harvey, V.; Eniu, A.; Hegg, R.; Tausch, C.; Seo, J.H.; Tsai, Y.F.; Ratnayake, J.; et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: A randomized phase II cardiac safety study (TRYPHAENA). Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2013, 24, 2278–2284. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Cerbelli, B.; Botticelli, A.; Pisano, A.; Campagna, D.; De Vincentiis, L.; Pernazza, A.; Frusone, F.; Scavina, P.; Monti, M.; Fortunato, L.; et al. Breast cancer subtypes affect the nodal response after neoadjuvant chemotherapy in locally advanced breast cancer: Are we ready to endorse axillary conservation? Breast J. 2019, 25, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Tong, Y.; He, J.; Chen, X.; Shen, K. Association between tumor molecular subtype, clinical stage and axillary pathological response in breast cancer patients undergoing complete pathological remission after neoadjuvant chemotherapy: Potential implications for de-escalation of axillary surgery. Ther. Adv. Med. Oncol. 2021, 13, 1758835921996673. [Google Scholar] [CrossRef]
- Chen, R.; Li, S.; Li, Y.; Zhu, Q.; Shi, X.; Xu, L.; Xu, Y.; Zhang, W.; Huang, X.; Wang, J.; et al. Can axillary surgery be omitted in patients with breast pathologic complete response after neoadjuvant systemic therapy for breast cancer? A real-world retrospective study in China. J. Cancer Res. Clin. Oncol. 2021, 147, 3495–3501. [Google Scholar] [CrossRef] [PubMed]
- Myers, S.P.; Ahrendt, G.M.; Lee, J.S.; Steiman, J.G.; Soran, A.; Johnson, R.R.; McAuliffe, P.F.; Diego, E.J. Association of Tumor Molecular Subtype and Stage with Breast and Axillary Pathologic Complete Response After Neoadjuvant Chemotherapy for Breast Cancer. Ann. Surg. Oncol. 2021, 28, 8636–8642. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.; Sabel, M.S.; Hughes, T.M.; Chang, A.E.; Dossett, L.A.; Jeruss, J.S. Impact of Breast Cancer Pretreatment Nodal Burden and Disease Subtype on Axillary Surgical Management. J. Surg. Res. 2021, 261, 67–73. [Google Scholar] [CrossRef]
- Tee, S.R.; Devane, L.A.; Evoy, D.; Rothwell, J.; Geraghty, J.; Prichard, R.S.; McDermott, E.W. Meta-analysis of sentinel lymph node biopsy after neoadjuvant chemotherapy in patients with initial biopsy-proven node-positive breast cancer. Br. J. Surg. 2018, 105, 1541–1552. [Google Scholar] [CrossRef] [PubMed]
- Simons, J.M.; van Nijnatten, T.J.A.; van der Pol, C.C.; Luiten, E.J.T.; Koppert, L.B.; Smidt, M.L. Diagnostic Accuracy of Different Surgical Procedures for Axillary Staging After Neoadjuvant Systemic Therapy in Node-positive Breast Cancer: A Systematic Review and Meta-analysis. Ann. Surg. 2019, 269, 432–442. [Google Scholar] [CrossRef]
- Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 11 February 2024).
- Barrio, A.V.; Montagna, G.; Mamtani, A.; Sevilimedu, V.; Edelweiss, M.; Capko, D.; Cody, H.S., 3rd; El-Tamer, M.; Gemignani, M.L.; Heerdt, A.; et al. Nodal Recurrence in Patients with Node-Positive Breast Cancer Treated With Sentinel Node Biopsy Alone After Neoadjuvant Chemotherapy—A Rare Event. JAMA Oncol. 2021, 7, 1851–1855. [Google Scholar] [CrossRef]
- Dubsky, P.; Pinker, K.; Cardoso, F.; Montagna, G.; Ritter, M.; Denkert, C.; Rubio, I.T.; de Azambuja, E.; Curigliano, G.; Gentilini, O.; et al. Breast conservation and axillary management after primary systemic therapy in patients with early-stage breast cancer: The Lucerne toolbox. Lancet Oncol. 2021, 22, e18–e28. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Tejedor, A.; Fernandez-Gonzalez, S.; Ortega, R.; Gil-Gil, M.; Perez-Montero, H.; Fernandez-Montolí, E.; Stradella, A.; Recalde, S.; Soler, T.; Petit, A.; et al. Can we avoid axillary lymph node dissection in N2 breast cancer patients with chemo-sensitive tumours such as HER2 and TNBC? Breast Cancer Res. Treat. 2021, 185, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Reimer, T.; Glass, A.; Botteri, E.; Loibl, S.; Gentilini, O.D. Avoiding Axillary Sentinel Lymph Node Biopsy after Neoadjuvant Systemic Therapy in Breast Cancer: Rationale for the Prospective, Multicentric EUBREAST-01 Trial. Cancers 2020, 12, 3698. [Google Scholar] [CrossRef] [PubMed]
- Pfob, A.; Sidey-Gibbons, C.; Rauch, G.; Thomas, B.; Schaefgen, B.; Kuemmel, S.; Reimer, T.; Hahn, M.; Thill, M.; Blohmer, J.U.; et al. Intelligent Vacuum-Assisted Biopsy to Identify Breast Cancer Patients with Pathologic Complete Response (ypT0 and ypN0) After Neoadjuvant Systemic Treatment for Omission of Breast and Axillary Surgery. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2022, 40, 1903–1915. [Google Scholar] [CrossRef] [PubMed]
- Heil, J.; Pfob, A.; Morrow, M. De-escalation of breast and axillary surgery in exceptional responders to neoadjuvant systemic treatment. Lancet. Oncol. 2021, 22, 435–436. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Hoskin, T.L.; Day, C.N.; Degnim, A.C.; Jakub, J.W.; Hieken, T.J.; Boughey, J.C. Decreasing Use of Axillary Dissection in Node-Positive Breast Cancer Patients Treated with Neoadjuvant Chemotherapy. Ann. Surg. Oncol. 2018, 25, 2596–2602. [Google Scholar] [CrossRef] [PubMed]
- Tinterri, C.; Sagona, A.; Barbieri, E.; Grimaldi, S.D.M.; Caraceni, G.; Ambrogi, G.; Jacobs, F.; Biondi, E.; Scardina, L.; Gentile, D. Sentinel Lymph Node Biopsy in Breast Cancer Patients Undergoing Neo-Adjuvant Chemotherapy: Clinical Experience with Node-Negative and Node-Positive Disease Prior to Systemic Therapy. Cancers 2023, 15, 1719. [Google Scholar] [CrossRef] [PubMed]
- Donker, M.; van Tienhoven, G.; Straver, M.E.; Meijnen, P.; van de Velde, C.J.; Mansel, R.E.; Cataliotti, L.; Westenberg, A.H.; Klinkenbijl, J.H.; Orzalesi, L.; et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): A randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol. 2014, 15, 1303–1310. [Google Scholar] [CrossRef]
- Almahariq, M.F.; Levitin, R.; Quinn, T.J.; Chen, P.Y.; Dekhne, N.; Kiran, S.; Desai, A.; Benitez, P.; Jawad, M.S.; Gustafson, G.S.; et al. Omission of Axillary Lymph Node Dissection is Associated with Inferior Survival in Breast Cancer Patients with Residual N1 Nodal Disease Following Neoadjuvant Chemotherapy. Ann. Surg. Oncol. 2021, 28, 930–940. [Google Scholar] [CrossRef]
- Weber, W.P.; Matrai, Z.; Hayoz, S.; Tausch, C.; Henke, G.; Zwahlen, D.R.; Gruber, G.; Zimmermann, F.; Seiler, S.; Maddox, C.; et al. Tailored axillary surgery in patients with clinically node-positive breast cancer: Pre-planned feasibility substudy of TAXIS (OPBC-03, SAKK 23/16, IBCSG 57-18, ABCSG-53, GBG 101). Breast 2021, 60, 98–110. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Untch, M.; Blohmer, J.-U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and Impact of Pathologic Complete Response on Prognosis After Neoadjuvant Chemotherapy in Various Intrinsic Breast Cancer Subtypes. J. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients N (%) 92 (100) | Luminal A N (%) 4 (4.3) | LumHER2− N (%) 26 (28.3) | LumHER2+ N (%) 24 (26.1) | HER2+ NonLum N (%) 17 (18.5) | Triple Neg. N (%) 21 (22.8) | p-Value |
|---|---|---|---|---|---|---|---|
| Age (Years) Median Range (min, max) | 50.6 (27.0–88.2) | 67.6 (35.5–75.6) | 46.6 (27.0–78.5) | 50.9 (33.0–74.6) | 55.5 (32.0–88.2) | 46.6 (38.3–87.4) | 0.428 |
| Age groups n (%) 20–35 years 36–50 years 51–65 years >65 years | 5 (5.4) 40 (43.5) 26 (28.3) 21 (22.8) | 0 (0) 1 (25) 0 (0) 3 (75) | 3 (11.5) 13 (50) 7 (26.9) 3 (11.6) | 1 (4.2) 9 (37.5) 9 (37.5) 5 (20.8) | 1 (5.9) 4 (23.5) 5 (29.4) 7 (41.2) | 0 (0) 13 (61.9) 5 (23.8) 3 (14.3) | 0.097 |
| Tumor stage n (%) Unknown (cT0/x) cT1 cT2 cT3 cT4 | 2 (2.2) 16 (17.4) 49 (53.3) 18 (19.5) 7 (7.6) | 0 (0) 1 (25) 1 (25) 1 (25) 1 (25) | 1 (3.8) 4 (15.4) 13 (50) 6 (23.1) 2 (7.7) | 1 (4.2) 1 (4.2) 16 (66.7) 4 (16.6) 2 (8.3) | 0 (0) 3 (17.7) 8 (47.1) 4 (23.5) 2 (11.7) | 0 (0) 7 (33.3) 11 (52.4) 3 (14.3) 0 (0) | 0.589 |
| Nodal stage n (%) cN1 cN2 cN3 | 69 (75) 16 (17.4) 7 (7.6) | 3 (75) 1 (25) 0 (0) | 16 (61.5) 5 (19.2) 5 (19.2) | 19 (79.2) 4 (16.7) 1 (4.2) | 13 (76.5) 3 (17.6) 1 (5.9) | 18 (85.7) 3 (14.3) 0 (0) | 0.407 |
| Grade n (%) Grade 1 Grade 2 Grade 3 Unknown | 2 (2.2) 23 (25) 48 (52.1) 19 (20.7) | 0 (0) 3 (75) 0 (0) 1 (25) | 1 (3.8) 7 (27) 15 (57.7) 3 (11.5) | 0 (0) 6 (25) 13 (54.2) 5 (20.8) | 0 (0) 3 (17.7) 9 (52.9) 5 (29.4) | 1 (4.8) 4 (19) 11 (52.4) 5 (23.8) | 0.551 |
| Characteristics | All Patients N (%) 92 (100) | Luminal A N (%) 4 (4.3) | LumHER2− N (%) 26 (28.3) | LumHER2+ N (%) 24 (26.1) | HER2+ NonLum N (%) 17 (18.5) | Triple Neg. N (%) 21 (22.8) | p-Value |
|---|---|---|---|---|---|---|---|
| Neoadj. Cht No 1 A→Tax TCb A→TCb Tax Capecitabine A 2 | 1 (1.1) 39 (42.4) 24 (26.1) 20 (21.7) 4 (4.3) 3 (3.3) 1 (1.1) | 0 (0) 2 (50) 0 (0) 1 (25) 1 (25) 0 (0) 0 (0) | 0 (0) 21 (80.9) 1 (3.8) 3 (11.5) 0 (0) 1 (3.8) 0 (0) | 0 (0) 9 (37.5) 12 (50) 1 (4.2) 0 (0) 2 (8.3) 0 (0) | 1 (5.9) 5 (29.4) 8 (47.1) 0 (0) 2 (8.3) 0 (0) 1 (5.9) | 0 (0) 2 (9.5) 3 (14.3) 15 (71.4) 1 (4.8) 0 (0) 0 (0) | <0.001 |
| Neoadjuvant antiHER2 th. No T TP | 52 (56.5) 8 (8.7) 32 (34.8) | 4 (100) 0 (0) 0 (0) | 26 (100) 0 (0) 0 (0) | 0 (0) 4 (16.7) 20 (83.3) | 1 (5.9) 2 4 (23.5) 12 (70.6) | 21 (100) 0 (0) 0 (0) | <0.001 |
| Neo/adjuvant ICI No Yes | 88 (95.7) 4 (4.3) | 4 (100) 0 (0) | 26 (100) 0 (0) | 24 (100) 0 (0) | 17 (100) 0 (0) | 17 (81) 4 (19) | 0.007 |
| Surgery of breast Mastectomy BCS | 40 (43.5) 52 (56.5) | 3 (75) 1 (25) | 9 (34.6) 17 (65.4) | 8 (33.3) 16 (66.7) | 9 (52.9) 8 (47.1) | 11 (52.4) 10 (47.6) | 0.314 |
| Surgery of axilla SLNB SLNB + TAS ALND | 33 (35.9) 16 (17.4) 43 (46.7) | 1 (25) 1 (25) 2 (25) | 7 (26.9) 5 (19.2) 14 (53.8) | 7 (29.2) 4 (16.7) 13 (54.2) | 10 (58.5) 3 (17.6) 4 (23.5) | 8 (38.1) 3 (14.3) 10 (23.5) | 0.604 |
| Adjuvant RT No Yes | 23 (23.9) 69 (75) | 0 (0) 4 (100) | 2 (7.7) 24 (92.3) | 3 (12.5) 21 (87.5) | 10 (58.8) 7 (41.2) | 8 (38.1) 13 (61.9) | 0.002 |
| Adjuvant Cht No Yes | 84 (91.3) 8 (8.7) | 3 (75) 1 (25) | 25 (96.2) 1 (3.8) | 22 (91.7) 2 (8.3) | 16 (94.1) 1 (5.9) | 18 (85.7) 3 (14.3) | 0.540 |
| Adj. antiHER2 th. No T TP T-DM1 | 51 (55.4) 20 (21.7) 15 (16.3) 6 (6.5) | 4 (100) 0 (0) 0 (0) 0 (0) | 26 (100) 0 (0) 0 (0) 0 (0) | 0 (0) 12 (50) 6 (25) 6 (25) | 0 (0) 8 (47.1) 9 (52.9) 0 (0) | 21 (0) 0 (0) 0 (0) 0 (0) | <0.001 |
| Adjuvant ET No Tamoxifen AI | 39 (42.4) 7 (7.6) 46 (50) | 0 (0) 0 (0) 4 (100) | 0 (0) 3 (11.5) 23 (88.5) | 1 (4.2) 4 (16.7) 19 (79.1) | 17 (100) 0 (0) 0 (0) | 21 (100) 0 (0) 0 (0) | <0.001 |
| Characteristics | No AXpCR N (%) | AX-pCR N (%) | p-Value |
|---|---|---|---|
| Tumor stage cT1/T2 cT3/T4 | 28 (43.1) 14 (56) | 37 (56.9) 10 (44) | 0.271 |
| Tumor grade Grade I Grade II Grade III Unknown | 2 (100) 15 (65.2) 18 (37.5) 9 (47.4) | 0 (0) 8 (34.5) 30 (62.5) 10 (52.6) | 0.056 |
| Nodal stage n cN1 cN2/3 | 35 (45.5) 9 (60) | 42 (54.5) 6 (40) | 0.302 |
| Chemotherapy Polychemotherapy Single-agent | 39 (47) 4 (50) | 44 (53) 4 (50) | 0.579 |
| Anti-HER2 th. No Yes | 30 (57.7) 14 (35) | 22 (42.3) 26 (75) | 0.031 |
| Subtype Lum A Lum HER2− Lum HER2+ HER2+ non-Lum TN | 4 (100) 17 (64.5) 10 (41.7) 4 (23.5) 9 (42.9) | 0 (0) 9 (34.6) 14 (58.3) 13 (76.5) 12 (57.1) | 0.013 |
| Breast-pCR No Yes | 13 (27.7) 35 (77.8) | 34 (72.3) 10 (22.2) | <0.0001 |
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| Clinical tumor stage cT3/T4 vs. cT1/T2 | 0.10 (0.015–0.83) | 0.033 |
| Molecular subtype HER2+ (Lum + non Lum)/TN vs. Lum A/Lum HER2− | 11.24 (1.18–107.10) | 0.036 |
| Clinical nodal stage cN2/3 and cN1 | 0.23 (0.03–1.58) | 0.146 |
| Variable | HR (95% CI) | p-Value |
|---|---|---|
| Type of breast surgery (mastectomy vs. BCS) | 0.36 (0.10–1.30) | 0.119 |
| Type of axillary surgery | ||
| ALND | 1.00 | 0.290 |
| SLNB vs. ALND | 0.31 (0.07–1.40) | 0.126 |
| SLNB + TAS vs. ALND | 0.55 (0.07–4.40) | 0.576 |
| Adjuvant radiation (yes vs. no) | 0.76 (0.23–2.46) | 0.641 |
| Adjuvant endocrine therapy (yes vs. no) | 0.56 (0.31–1.03) | 0.063 |
| Adjuvant antiHER2 therapy (yes vs. no) | 0.61 (0.44–1.97) | 0.735 |
| Molecular subtype (HER2+/TN vs. Lum A/Lum HER2−) | 1.50 (0.46–4.89) | 0.505 |
| pCR in breast (yes vs. no) | 0.24 (0.05–1.08) | 0.062 |
| pCR in axilla (yes vs. no) | 0.18 (0.04–0.80) | 0.024 |
| Total pCR (yes vs. no) | 0.19 (0.03–1.47) | 0.112 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grašič Kuhar, C.; Geiger, J.; Schwab, F.D.; Heinzelmann-Schwartz, V.; Vetter, M.; Weber, W.P.; Kurzeder, C. Prognostic Importance of Axillary Lymph Node Response to Neoadjuvant Systemic Therapy on Axillary Surgery in Breast Cancer—A Single Center Experience. Cancers 2024, 16, 1306. https://doi.org/10.3390/cancers16071306
Grašič Kuhar C, Geiger J, Schwab FD, Heinzelmann-Schwartz V, Vetter M, Weber WP, Kurzeder C. Prognostic Importance of Axillary Lymph Node Response to Neoadjuvant Systemic Therapy on Axillary Surgery in Breast Cancer—A Single Center Experience. Cancers. 2024; 16(7):1306. https://doi.org/10.3390/cancers16071306
Chicago/Turabian StyleGrašič Kuhar, Cvetka, James Geiger, Fabienne Dominique Schwab, Viola Heinzelmann-Schwartz, Marcus Vetter, Walter Paul Weber, and Christian Kurzeder. 2024. "Prognostic Importance of Axillary Lymph Node Response to Neoadjuvant Systemic Therapy on Axillary Surgery in Breast Cancer—A Single Center Experience" Cancers 16, no. 7: 1306. https://doi.org/10.3390/cancers16071306
APA StyleGrašič Kuhar, C., Geiger, J., Schwab, F. D., Heinzelmann-Schwartz, V., Vetter, M., Weber, W. P., & Kurzeder, C. (2024). Prognostic Importance of Axillary Lymph Node Response to Neoadjuvant Systemic Therapy on Axillary Surgery in Breast Cancer—A Single Center Experience. Cancers, 16(7), 1306. https://doi.org/10.3390/cancers16071306