

Systematic Review of Single-Agent vs. Multi-Agent Chemotherapy for Advanced Pancreatic Adenocarcinoma in Elderly vs. Younger Patients

Abstract
Simple Summary
Abstract
1. Introduction
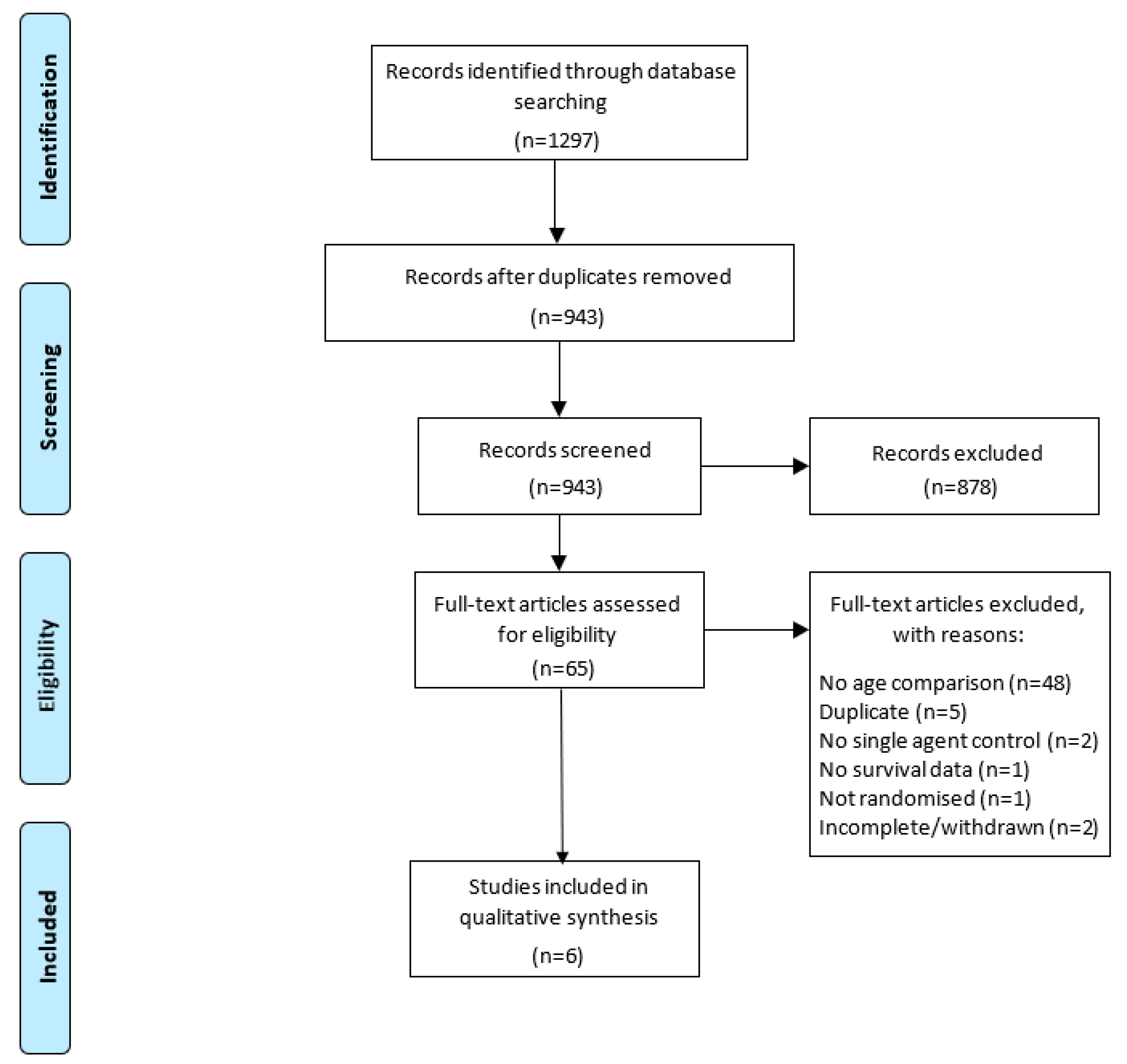
2. Materials and Methods
3. Results
3.1. Characteristics of Included Trials
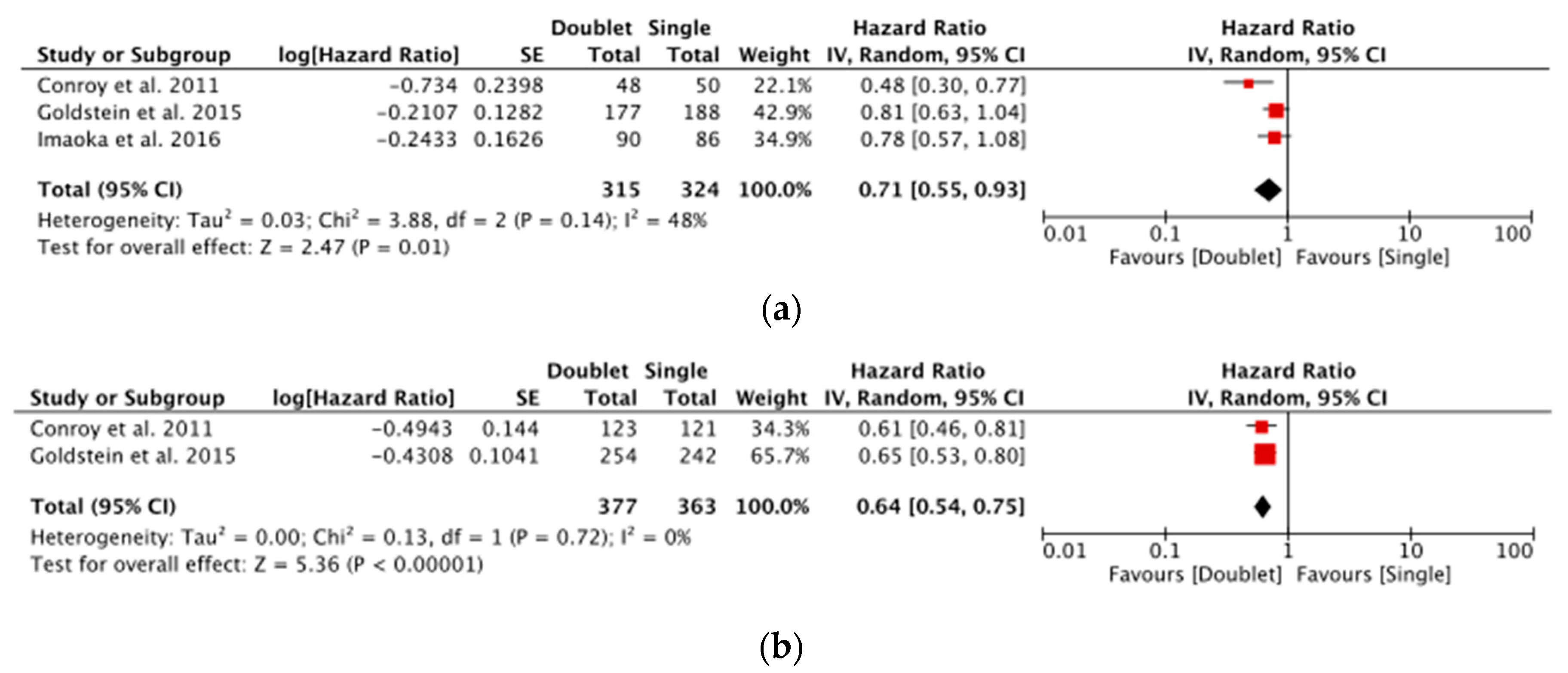
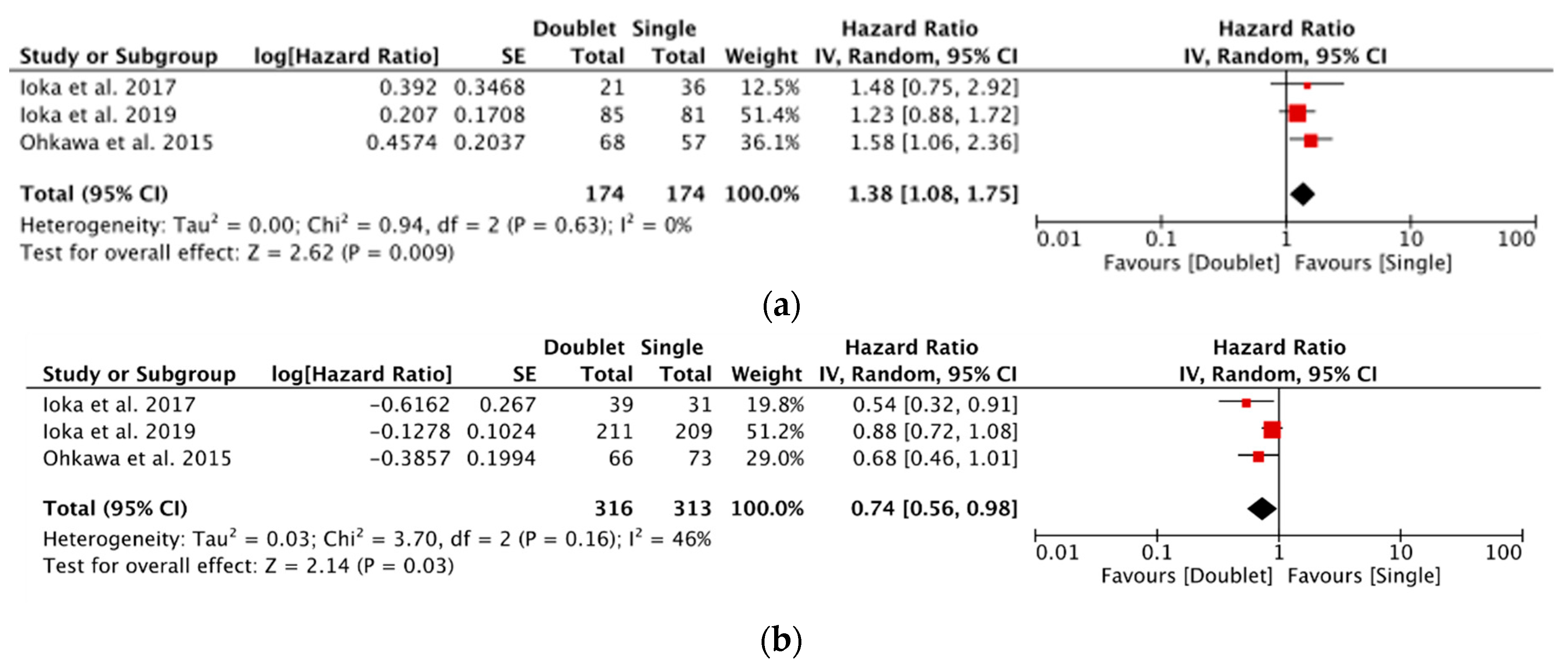
3.2. Subgroup Analysis
3.3. Toxicity
3.4. Assessment of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy Used in Medline, Embase and Cochrane Central
Appendix B. Risk of Bias for Each of the Included Studies
| Study | Selection Bias | Performance Bias | Blinding of Outcome Assessment Bias |
| Conroy et al., 2011 [15] | Low | High | Low |
| Goldstein et al., 2015 [16] | Low | High | Low |
| Imaoka et al., 2016 [17] | Low | High | Low |
| Ioka et al., 2017 [18] | Low | High | High |
| Ioka et al., 2019 [19] | Low | High | Low |
| Ohkawa et al., 2015 [4] | Low | High | High |
Appendix C. Summary of Treatment Regimens
| Study | Country | n | Treatment Regimen |
| Conroy et al., 2011 [15] | France | 171 | Gemcitabine: 1000 mg/m2 over 30 min weekly for 7 consecutive weeks, followed by 1 week of rest (cycle 1). Afterwards, continued days 1, 8, and 15 every 28 days. |
| 171 | FOLFIRINOX: oxaliplatin 85 mg/m2 over 2 h, immediately followed by leucovorin 400 mg/m2 over 2 h, with the addition, after 30 min, of irinotecan 180 mg/m2 over 90 min through a Y connector. Followed immediately by fluorouracil 400 mg/m2. | ||
| Goldstein et al., 2015 [16] | Global | 430 | Gemcitabine: 1000 mg/m2 weekly for 7 consecutive weeks, followed by 1 week of rest (cycle 1). Afterwards, continued days 1, 8, and 15 every 4 weeks in subsequent cycles. |
| 431 | Nab-Paclitaxel: 125 mg/m2, followed by an infusion of; Gemcitabine: 1000 mg/m2 on days 1, 8, 15, 29, 36, and 43. Patients received treatment on days 1, 8, and 15 every 4 weeks in subsequent cycles. | ||
| Imaoka et al., 2016 [17] | Japan/ Taiwan | 277 | Gemcitabine: 1000 mg/m2 over 30 min on days 1, 8, and 15 of a 28 day cycle. |
| 280 | S-1: orally twice daily at a dose according to BSA (<1.25 m2, 80 mg/d; ≥1.25 to <1.5 m2, 100 mg/d; ≥1.5 m2, 120 mg/d) on days 1 through 28 of a 42-day cycle. | ||
| 275 | Gemcitabine: 1000 mg/m2 on days 1 and 8. S-1: orally twice daily at a dose according to the BSA (<1.25 m2, 80 mg/d; ≥1.25 to <1.5 m2, 100 mg/d; ≥1.5 m2, 120 mg/d) on days 1 through 14 of a 21 day cycle. | ||
| Ioka et al., 2017 [18] | Japan | 67 | S-1: orally twice daily at a dose according to BSA (<1.25 m2, 40 mg; ≥1.25 to <1.5 m2, 50 mg; ≥1.5 m2, 60 mg) for 28 days, repeating every 6 weeks. |
| 60 | S-1: orally twice daily at a dose according to BSA (<1.25 m2, 40 mg; ≥1.25 to <1.5 m2, 50 mg; ≥1.5 m2, 60 mg) for 14 days, repeating every 4 weeks. Irinotecan: 100 mg/ m2 on day 1 and 15. | ||
| Ioka et al., 2019 [19] | Japan/ Korea | 290 | S-1: orally twice daily at a dose according to BSA (<1.25 m2, 40 mg; ≥1.25 to <1.5 m2, 50 mg; ≥1.5 m2, 60 mg) for 28 days, repeating every 6 weeks. |
| 296 | S-1 (30, 40, 50, or 60 mg) and; Leucovorin (25 mg), administered orally twice daily for 1 week in a 2 week cycle. Doses determined according to BSA (<1.25 m2, 40 mg; ≥1.25 to <1.5 m2, 50 mg; ≥1.5 m2, 60 mg). | ||
| Ohkawa et al., 2015 [4] | Japan | 135 | S-1: orally twice daily at a dose according to BSA (<1.25 m2, 80 mg; ≥1.25 to <1.5 m2, 100 mg; ≥1.5 m2, 120 mg) for 28 days, repeating every 6 weeks. |
| 136 | S-1: orally twice daily at a dose according to BSA (<1.25 m2, 80 mg; ≥1.25 to <1.5 m2, 100 mg; ≥1.5 m2, 120 mg) on days 1–14 of every 3 week period. Oxaliplatin: 100 mg/ m2 over 2 h on day 1. |
References
- Chin, V.; Nagrial, A.; Sjoquist, K.; O’Connor, C.A.; Chantrill, L.; Biankin, A.V.; Scholten, R.J.; Yip, D. Chemotherapy and radiotherapy for advanced pancreatic cancer. Cochrane Database Syst. Rev. 2018, 3, CD011044. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Xie, W.; Zou, Y.; Xie, S.; Zhang, J.; Yuan, W.; Ma, J.; Zhao, J.; Zheng, C.; Chen, Y. First-line chemotherapy regimens for locally advanced and metastatic pancreatic adenocarcinoma: A Bayesian analysis. Cancer Manag. Res. 2018, 10, 5965. [Google Scholar] [CrossRef]
- Ryan, D.P.; Hong, T.S.; Bardeesy, N. Pancreatic adenocarcinoma. N. Engl. J. Med. 2014, 1, 1039–1049. [Google Scholar] [CrossRef] [PubMed]
- Ohkawa, S.; Okusaka, T.; Isayama, H.; Fukutomi, A.; Yamaguchi, K.; Ikeda, M.; Funakoshi, A.; Nagase, M.; Hamamoto, Y.; Nakamori, S.; et al. Randomised phase II trial of S-1 plus oxaliplatin vs. S-1 in patients with gemcitabine-refractory pancreatic cancer. Br. J. Cancer 2015, 112, 1428–1434. [Google Scholar] [CrossRef]
- Rahma, O.; Duffy, A.; Liewehr, D.; Steinberg, S.; Greten, T. Second-line treatment in advanced pancreatic cancer: A comprehensive analysis of published clinical trials. Ann. Oncol. 2013, 24, 1972–1979. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.K.; Abel, U.; Komander, C.; Harig, S.; Jager, D.; Springfeld, C. Chemotherapy for advanced pancreatic adenocarcinoma in elderly patients (≥70 years of age): A retrospective cohort study at the National Center for Tumor Diseases Heidelberg. Pancreatology 2014, 14, 211–215. [Google Scholar] [CrossRef]
- Guion-Dusserre, J.F.; Bertaut, A.; Ghiringhelli, F.; Vincent, J.; Quipourt, V.; Marilier, S.; Tharin, Z.; Bengrine-Lefevre, L. Folfirinox in elderly patients with pancreatic or colorectal cancer-tolerance and efficacy. World J. Gastroenterol. 2016, 22, 9378–9386. [Google Scholar] [CrossRef] [PubMed]
- Ellenrieder, V.; Konig, A.; Seufferlein, T. Current Standard and Future Perspectives in First- and Second-Line Treatment of Metastatic Pancreatic Adenocarcinoma. Digestion 2016, 94, 44–49. [Google Scholar] [CrossRef]
- Park, S.J.; Kim, H.; Shin, K.; Lee, M.A.; Hong, T.H. Oral chemotherapy for second-line treatment in patients with gemcitabine-refractory advanced pancreatic cancer. World J. Gastrointest. Oncol. 2019, 11, 1021–1030. [Google Scholar] [CrossRef]
- Schiavo, J.H. Prospero: An international register of systematic review protocols. Med. Ref. Serv. Q. 2019, 38, 171–180. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, 14898. [Google Scholar] [CrossRef] [PubMed]
- Cochrane. Cochrane Revman: Cochrane. 2020. Available online: https://training.cochrane.org/online-learning/core-software/revman (accessed on 1 January 2022).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Becouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardiere, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.; El-Maraghi, R.H.; Hammel, P.; Heinemann, V.; Kunzmann, V.; Sastre, J.; Scheithauer, W.; Siena, S.; Tabernero, J.; Teixeira, L.; et al. Nab-Paclitaxel plus gemcitabine for metastatic pancreatic cancer: Long-term survival from a phase III trial. J. Natl. Cancer Inst. 2015, 107, dju413. [Google Scholar] [CrossRef]
- Imaoka, H.; Kou, T.; Tanaka, M.; Egawa, S.; Mizuno, N.; Hijioka, S.; Hara, K.; Yazumi, S.; Shimizu, Y.; Yamao, K. Clinical outcome of elderly patients with unresectable pancreatic cancer treated with gemcitabine plus S-1, S-1 alone, or gemcitabine alone: Subgroup analysis of a randomised phase III trial, GEST study. Eur. J. Cancer 2016, 54, 96–103. [Google Scholar] [CrossRef]
- Ioka, T.; Komatsu, Y.; Mizuno, N.; Tsuji, A.; Ohkawa, S.; Tanaka, M.; Iguchi, H.; Ishiguro, A.; Kitano, M.; Satoh, T. Randomised phase II trial of irinotecan plus S-1 in patients with gemcitabine-refractory pancreatic cancer. Br. J. Cancer 2017, 116, 464–471. [Google Scholar] [CrossRef]
- Ioka, T. Second line chemotherapy for advanced pancreatic cancer patients in Japan. Ann. Oncol. 2019, 30 (Suppl. S6), vi30. [Google Scholar] [CrossRef]
- Berlin, J.D.; Catalano, P.; Thomas, J.P.; Kugler, J.W.; Haller, D.G.; Benson, A.B., 3rd. Phase III study of gemcitabine in combination with fluorouracil versus gemcitabine alone in patients with advanced pancreatic carcinoma: Eastern Cooperative Oncology Group Trial E2297. J. Clin. Oncol. 2002, 20, 3270–3275. [Google Scholar] [CrossRef]
- Pusceddu, S.; Ghidini, M.; Torchio, M.; Corti, F.; Tomasello, G.; Niger, M.; Prinzi, N.; Nichetti, F.; Coinu, A.; Di Bartolomeo, M. Comparative effectiveness of gemcitabine plus nab-paclitaxel and FOLFIRINOX in the first-line setting of metastatic pancreatic cancer: A systematic review and meta-analysis. Cancers 2019, 11, 484. [Google Scholar] [CrossRef]
- Dragovich, T.; Laheru, D.; Dayyani, F.; Bolejack, V.; Smith, L.; Seng, J.; Burris, H.; Rosen, P.; Hidalgo, M.; Ritch, P.; et al. Phase II trial of vatalanib in patients with advanced or metastatic pancreatic adenocarcinoma after first-line gemcitabine therapy (PCRT O4-001). Cancer Chemother. Pharmacol. 2014, 74, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Ueno, M.; Ikeda, M.; Ozaka, M.; Sano, Y.; Hirotani, A.; Tozuka, Y.; Fukushima, T.; Tezuka, S.; Moriya, S.; et al. A Multicenter Retrospective Study of Gemcitabine Plus Nab-Paclitaxel for Elderly Patients with Advanced Pancreatic Cancer. Pancreas 2020, 49, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Nagrial, A.M.; Chin, V.T.; Sjoquist, K.M.; Pajic, M.; Horvath, L.G.; Biankin, A.V.; Yip, D. Second-line treatment in inoperable pancreatic adenocarcinoma: A systematic review and synthesis of all clinical trials. Crit. Rev. Oncol. Hematol. 2015, 96, 483–497. [Google Scholar] [CrossRef] [PubMed]
- Schultheis, B.; Strumberg, D.; Bergmann, L.; Graeven, U.; Hanauske, A.-R.; Lipp, R.; Schuette, J.; Saito, K.; Scigalla, P.; Scheulen, M.E. Results of a phase II trial of S-1 as first-line treatment of metastatic pancreatic cancer (CESAR-study group). Investig. New Drugs 2012, 30, 1184–1192. [Google Scholar] [CrossRef]
- Garcia, G.; Odaimi, M. Systemic combination chemotherapy in elderly pancreatic cancer: A review. J. Gastrointest. Cancer 2017, 48, 121–128. [Google Scholar] [CrossRef]
- Baldini, C.; Escande, A.; Bouché, O.; El Hajbi, F.; Volet, J.; Bourgeois, V.; Vantroys, T.R.; Ploquin, A.; Desauw, C.; Hebbar, M. Safety and efficacy of FOLFIRINOX in elderly patients with metastatic or locally advanced pancreatic adenocarcinoma: A retrospective analysis. Pancreatology 2017, 17, 146–149. [Google Scholar] [CrossRef]
- Macchini, M.; Chiaravalli, M.; Zanon, S.; Peretti, U.; Mazza, E.; Gianni, L.; Reni, M. Chemotherapy in elderly patients with pancreatic cancer: Efficacy, feasibility and future perspectives. Cancer Treat. Rev. 2019, 72, 1–6. [Google Scholar] [CrossRef]
- Webb, P.; Bain, C.; Page, A. Essential Epidemiology: An Introduction for Students and Health Professionals; Cambridge University Press: Cambridge, UK, 2017. [Google Scholar]
- Cao, C.; Kuang, M.; Xu, W.; Zhang, X.; Chen, J.; Tang, C. Gemcitabine plus S-1: A hopeful frontline treatment for Asian patients with unresectable advanced pancreatic cancer. Jpn. J. Clin. Oncol. 2015, 45, 1122–1130. [Google Scholar] [CrossRef]
- Easterbrook, P.J.; Gopalan, R.; Berlin, J.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study | Country | n | Treatment Regimen | Patients with PDAC (n) | Mean Age (Years) | Age Range (Years) | M:F Ratio (% Male) | Locally Advanced (%) | Metastatic (%) | Elderly Subgroup (n) | Young Subgroup (n) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Conroy et al., 2011 [15] | France | 171 | Gemcitabine | 171 | 61 | 34–75 | 61.4 | 0 | 100 | 50 | 121 |
| 171 | FOLFIRINOX | 171 | 61 | 25–76 | 62 | 0 | 100 | 48 | 123 | ||
| Goldstein et al., 2015 [16] | Global | 430 | Gemcitabine | 430 | |||||||
| 431 | Nab-Paclitaxel + Gemcitabine | 63 | 32–88 | 60 | 0 | 100 | 189 | 241 | |||
| Imaoka et al., 2016 [17] | Japan/ Taiwan | 277 | Gemcitabine | 430 | 62 | 27–86 | 57 | 0 | 100 | 176 | 254 |
| 280 | S-1 | 277 | |||||||||
| 275 | Gemcitabine | - | - | 61.4 | 23.8 | 76.2 | 86 | 191 | |||
| Ioka et al., 2017 [18] | Japan | 67 | S-1 | 280 | - | - | 60.7 | 24.3 | 75.7 | 85 | 195 |
| 60 | S-1 + Irinotecan | 275 | - | - | 57.5 | 24.7 | 75.3 | 90 | 185 | ||
| Ioka et al., 2019 [19] | Japan/ Korea | 290 | S-1 | 70 | 65 | 42–76 | 67.2 | 0 | 100 | 36 | 31 |
| 296 | S-1 + Leucovorin | 67 | 62 | 33–83 | 58.3 | 0 | 100 | 21 | 39 | ||
| Ohkawa et al., 2015 [4] | Japan | 135 | S-1 | 302 | 64 | 32–79 | 57.6 | 0 | 100 | 81 | 209 |
| 136 | S-1 + Oxaliplatin | 301 | 65 | 30–79 | 58.4 | 0 | 100 | 85 | 211 |
| Study | Country | n | Treatment Regimen | Median OS (Months) | HR | p | Median PFS (Months) | HR | p | ORR (%) | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Conroy et al., 2011 [15] | France | 171 | Control: gemcitabine | 6.8 [5.5–7.6] | 3.3 [2.2–3.6] | 9.4 [5.4–14.7] | |||||
| 171 | Arm 1: FOLFIRINOX | 11.1 [9.0–13.1] | 0.57 [0.45–0.73] | <0.001 | 6.4 [5.5–7.2] | 0.47 [0.37–0.59] | <0.001 | 31.6 [24.7–39.1] | <0.001 | ||
| Goldstein et al., 2015 [16] | Global | 430 | Control: gemcitabine | 6.6 [6.01–7.20] | 3.7 | 7 [5.0–10.0] | |||||
| 431 | Arm 1: gemcitabine + nab-Paclitaxel | 8.7 [7.89–9.69] | 0.72 [0.62–0.83] | <0.001 | 5.5 | 0.69 [0.58–0.82] | <0.001 | 23 [19.0–27.0] | <0.001 | ||
| Imaoka et al., 2016 [17] | Japan/ Taiwan | 277 | Control: gemcitabine | 8.8 [8.0–9.7] | 4.1 [3.0–4.4] | 13.3 [9.3–18.2] | NA | ||||
| 280 | Arm 1: S-1 | 9.7 [7.6–10.8] | 0.96 | <0.001 | 3.8 [2.9–4.2] | 1.09 | 0.02 | 21.0 [16.1–26.6] | 0.02 | ||
| 275 | Arm 2: S-1 + gemcitabine | 10.1 [9.0–11.2] | 0.88 | 0.15 | 5.7 [5.4–6.7] | 0.66 | <0.001 | 29.3 [23.7–35.5] | <0.001 | ||
| Ioka et al., 2017 [18] | Japan | 67 | Control: S-1 | 5.8 [5.1–8.0] | 1.9 [1.8–2.1] | 6.0 [1.7–14.6] | |||||
| 60 | Arm 1: S-1 + irinotecan | 6.8 [5.8–9.3] | 0.75 [0.51–1.09] | 0.13 | 3.5 [2.1–4.6] | 0.77 [0.53–1.11] | 0.18 | 18.3 [9.5–30.4] | 0.03 | ||
| Ioka et al., 2019 [19] | Japan/ Korea | 290 | Control: S-1 | 7.9 [7.0–8.4] | 2.8 [2.7–2.9] | 15.1 | |||||
| 296 | Arm 1: S-1 + leucovorin | 7.6 [7.0–8.2] | 0.98 [0.82–1.16] | 0.756 | 3.9 [2.8–4.2] | 0.80 [0.67–0.95] | 0.009 | 20.6 | 0.127 | ||
| Ohkawa et al., 2015 [4] | Japan | 135 | Control: S-1 | 6.9 [5.8–9.0] | 2.8 [1.9–3.5] | 11.5 [6.6–18.3] | |||||
| 136 | Arm 1: S-1 + oxaliplatin | 7.4 [6.2–8.6] | NA | NA | 3.0 [2.8–3.7] | NA | NA | 20.9 [14.4–28.8] | 0.04 |
| Study | Treatment Arm | OS (Months) | HR | p | PFS (Months) | HR | p | ORR (%) | p |
|---|---|---|---|---|---|---|---|---|---|
| Conroy et al., 2011 [15] | Control: gemcitabine | NA | NA | NA | NA | ||||
| Arm 1: FOLFIRINOX | NA | 0.48 [0.30–0.77] | NA | NA | NA | NA | NA | NA | |
| Goldstein et al., 2015 [16] | Control: gemcitabine | 6.5 | NA | NA | NA | ||||
| Arm 1: gemcitabine + nab-Paclitaxel | 7.7 | 0.80 | 0.048 | NA | NA | NA | NA | NA | |
| Imaoka et al., 2016 [17] | Control: gemcitabine | 8.5 [7.4–9.4] | 4.5 [3.0–5.6] | 14.3 [7.1–24.7] | 0.835 | ||||
| Arm 1: S-1 | 8.0 [6.6–10.8] | 0.940 [0.69–1.29] | 0.715 | 4.2 [2.9–4.7] | 1.153 | 0.424 | 25.3 [16.0–36.7] | 0.309 | |
| Arm 2: S-1 + gemcitabine | 10.2 [8.8–12.4] | 0.784 [0.57–1.08] | 0.120 | 6.9 [5.6–8.3] | 0.662 | 0.007 | 27.6 [18.0–39.1] | 0.762 | |
| Ioka et al., 2017 [18] | Control: S-1 | NA | NA | NA | NA | ||||
| Arm 1: S-1 + irinotecan | NA | 1.48 [0.75–2.93] | 0.07 | NA | 1.35 [0.70–2.60] | 0.07 | NA | NA | |
| Ioka et al., 2019 [19] | Control: S-1 | NA | NA | NA | NA | ||||
| Arm 1: S-1 + leucovorin | NA | 1.23 [0.88–1.71] | 0.093 | NA | 1.00 [0.72–1.38] | 0.091 | NA | NA | |
| Ohkawa et al., 2015 [4] | Control: S-1 | NA | NA | NA | NA | ||||
| Arm 1: S-1 plus oxaliplatin | NA | 1.58 [1.06–2.36] | 0.024 | NA | 1.07 [0.46–1.00] | 0.724 | NA | NA |
| Study | Treatment Arm | OS (Months) | HR | p | PFS (Months) | HR | p | ORR (%) | p |
|---|---|---|---|---|---|---|---|---|---|
| Conroy et al., 2011 [15] | Control: gemcitabine | NA | NA | NA | NA | ||||
| Arm 1: FOLFIRINOX | NA | 0.61 [0.46–0.82] | NA | NA | NA | NA | NA | NA | |
| Goldstein et al., 2015 [16] | Control: gemcitabine | 6.8 | NA | NA | NA | ||||
| Arm 1: gemcitabine + nab-Paclitaxel | 9.6 | 0.65 | <0.001 | NA | NA | NA | NA | NA | |
| Imaoka et al., 2016 [17] | Control: gemcitabine | 8.9 [8.1–10.0] | 0.275 | 3.5 [2.8–4.3] | 0.338 | 12.9 [8.2–18.8] | 0.835 | ||
| Arm 1: S-1 | 10 [7.4–11.4] | NA | 0.325 | 3.7 [2.9–4.2] | NA | 0.691 | 19.1 [13.5–25.7] | 0.309 | |
| Arm 2: S-1 + gemcitabine | 10.2 [8.8–12.4] | NA | 0.835 | 5.4 [4.3–6.5] | NA | 0.319 | 30.1 [23.3–37.7] | 0.762 | |
| Ioka et al., 2017 [18] | Control: S-1 | NA | NA | NA | NA | ||||
| Arm 1: S-1 + irinotecan | NA | 0.54 [0.32–0.92] | 0.07 | NA | 0.58 [0.34–0.99] | 0.07 | NA | NA | |
| Ioka et al., 2019 [19] | Control: S-1 | NA | NA | NA | NA | ||||
| Arm 1: S-1 + leucovorin | NA | 0.88 [0.72–1.08] | 0.093 | NA | 0.72 [0.59–0.89] | 0.091 | NA | NA | |
| Ohkawa et al., 2015 [4] | Control: S-1 | NA | NA | NA | NA | ||||
| Arm 1: S-1 plus oxaliplatin | NA | 0.68 [0.46–1.00] | 0.0498 | NA | 0.68 [0.47–0.98] | 0.041 | NA | NA |
| Study | Neutropenia (%) | Nausea (%) | Vomiting (%) | Fatigue (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Single-Agent | Doublet | p | Single-Agent | Doublet | p | Single-Agent | Doublet | p | Single-Agent | Doublet | p | |
| Conroy et al., 2011 [15] | 21 | 45.7 | <0.001 | NA | NA | NA | 8.3 | 14.5 | NS | 17.8 | 23.6 | NS |
| Goldstein et al., 2015 [16] | 26 | 37 | NA | NA | NA | NA | NA | NA | NA | 6 | 17 | NA |
| Ioka et al., 2017 [18] | 4.3 | 15.6 | 0.03 | 2.9 | 6.3 | 0.35 | 1.4 | 3.1 | 0.52 | NA | NA | NA |
| Ioka et al., 2019 [19] | 3.3 | 1.7 | NA | 0.7 | 1.7 | NA | 0.7 | 2.0 | NA | 0.7 | 1.0 | NA |
| Ohkawa et al., 2015 [4] | 11.4 | 8.1 | NA | 3.0 | 6.6 | NA | 0.8 | 2.9 | NA | 3.8 | 2.9 | NA |
| Study | Neutropenia (%) | Nausea (%) | Vomiting (%) | Fatigue (%) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| GEM | S-1 | GEM + S-1 | p | GEM | S-1 | GEM + S-1 | p | GEM | S-1 | GEM + S-1 | p | GEM | S-1 | GEM + S-1 | p | |
| <70 | 37.2 | 7.7 | 58.9 | NA | 9.4 | 15.9 | 20.5 | NA | 5.8 | 7.7 | 16.2 | NA | 14.1 | 19.5 | 25.9 | NA |
| ≥70 | 47.7 | 10.6 | 63.3 | NA | 12.8 | 16.5 | 10.0 | NA | 9.3 | 10.6 | 7.8 | NA | 18.6 | 24.7 | 21.1 | NA |
| p | 0.113 | 0.487 | 0.513 | NA | 0.402 | 1.00 | 0.039 | NA | 0.308 | 0.487 | 0.061 | NA | 0.372 | 0.342 | 0.455 | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lewis, A.; Nagrial, A. Systematic Review of Single-Agent vs. Multi-Agent Chemotherapy for Advanced Pancreatic Adenocarcinoma in Elderly vs. Younger Patients. Cancers 2023, 15, 2289. https://doi.org/10.3390/cancers15082289
Lewis A, Nagrial A. Systematic Review of Single-Agent vs. Multi-Agent Chemotherapy for Advanced Pancreatic Adenocarcinoma in Elderly vs. Younger Patients. Cancers. 2023; 15(8):2289. https://doi.org/10.3390/cancers15082289
Chicago/Turabian StyleLewis, Alison, and Adnan Nagrial. 2023. "Systematic Review of Single-Agent vs. Multi-Agent Chemotherapy for Advanced Pancreatic Adenocarcinoma in Elderly vs. Younger Patients" Cancers 15, no. 8: 2289. https://doi.org/10.3390/cancers15082289
APA StyleLewis, A., & Nagrial, A. (2023). Systematic Review of Single-Agent vs. Multi-Agent Chemotherapy for Advanced Pancreatic Adenocarcinoma in Elderly vs. Younger Patients. Cancers, 15(8), 2289. https://doi.org/10.3390/cancers15082289