
Possible Value of Faecal Immunochemical Test (FIT) When Added in Symptomatic Patients Referred for Colonoscopy: A Systematic Review

 , ,
, , 
Simple Summary
Abstract
1. Introduction
- (1)
- aged 40 and over with unexplained weight loss and abdominal pain;
- (2)
- or aged 50 and over with unexplained rectal bleeding;
- (3)
- or aged 60 and over with iron-deficiency anaemia or changes in bowel habit; or tests show occult blood in their faeces.
2. Materials and Methods
2.1. Search Strategy
2.2. Quality Assessment
2.3. Data Extraction
2.4. Statistical Analysis
3. Result
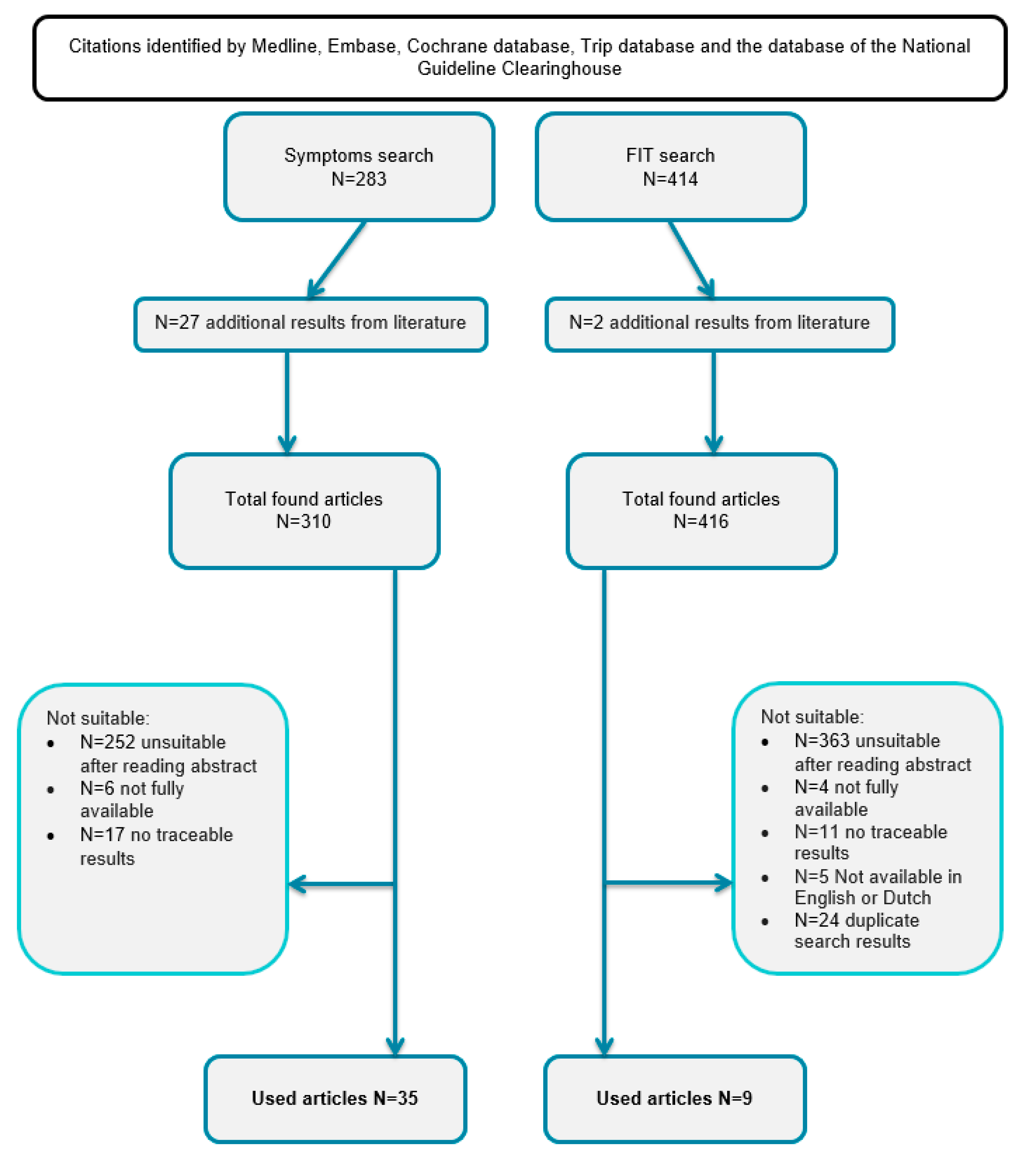
3.1. Publication Searching Results
3.2. Statistical Heterogeneity
3.3. Symptoms
3.4. Symptomatic Patients and FIT
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B
| Study | Type | N | Location | Study Period | Characteristics of Method |
| Bafandeh 2008 [21] | Prospective | 480 | Imam Hospital, Tabriz University of medical sciences, Iran. | 2 years | - long lasting lower gastrointestinal tract symptoms - every age |
| Bjerregaard 2006 [22] | Cross-sectional, prospective | 2172 | Surgical outpatient clinics of two public Danish hospitals: Randers Central Hospital (RCH) and Aarhus University Hospital (AUH) in Aarhus County, Denmark. | 16 months | - >40 years old - referred by general practitioners - symptoms consistent with CRC - Colonoscopy - Questionnaire about symptoms |
| Brewster 1994 [23] | Prospective | 462 | Leith Hospital, Edinburgh, UK | 3 years | - Referred for barium enema → also flexible sigmoidscopy. |
| Farrands 1985 [24] | Prospective | 152 | Southampton General hospital, UK | - | - Gastro-intestinal symptoms suggestive of colorectal disease. - 101: Rectal examination, proctoscopy and sigmoidscopy → FIT → colonoscopy or bariumeneme - 51: FIT → bariumeneme or colonoscopy |
| Selvachandran 2002 [25] | Prospective | 2268 | Leighton hospital, Crewe, UK | 2 years | - Distal colonic symptoms - Referred by GP for endoscopic assessment - Questionnaire |
| Tan 2002 [27] | Prospective Cross-sectional | 485 | University Hospital, Kuala Lumpur, Malaysia. | 22 months | - Referred by GP for colonoscopy - Questionnaire |
| Tate 1988 [28] | Prospective | 137 | Royal South Hampshire Hospital, Southampton, UK 52 GP’s. | 1 year | - Referral by GP suspected for colonic neoplasia |
| Thompson 2007 [29] | Prospective, observational | 8529 | Portsmouth, single surgical outpatient clinic, UK | 12 years | - All consecutive patients with lower gastrointestinal symptoms - Everyone sigmoidscopy - When doctor decided: colonoscopy/Barium enema? |
| Thompson 2008 [30] | Prospective, observational | 16,433 |
St Mary’s Hospital and two peripheral hospitals in and near Portsmouth, UK | 16 years | - newly referred patients with symptoms or signs of colorectal cancer. - Sigmoidscopy either alone or followed by bariumenema, colonoscopy or CT colonography. |
| Panzuto 2003 [32] | Prospective | 280 | Lazio, Italy; 159 GP’s. | 8 weeks | - consecutive outpatients with symptoms considered suspicious for the presence of a colon disease to rule out the presence of CRC. - Colonoscopy or barium enema - Trained GP’s - Exclusion: previous diagnoses of colorectal disorders or a recent large bowel examination |
| Curless 1994 [33] | Retrospective | 123 +125 control <70 year 150 + 148 control <70 year | Hospitals of Gateshead and Newcastle Health Districts, UK | 1 year | - histological diagnosis of colorectal adenocarcinoma - Within 2 weeks interview - Exclusions: previous diagnosis of colorectal adenoma or carcinoma, known colitis, non-whites, and those dying before interview - Controls: matched with sex and age |
| Jensen 1993 [34] | Prospective | 194 | Varberg Hospital, Sweden | - | - symptoms indicating colorectal disease, referred by GP for double-contrast barium enema (DCE) - fecal occult blood test and rectosigmoidoscopy before the DCE |
| Patel 2016 [35] | Retrospective | 197 | West Suffolk Hospital, Suffolk, UK | 6 years | - primary care referrals for suspected colorectal malignancy - <50 years |
| Cheong 2000 [36] | Prospective | 375 | Hospital University Kebangsaan Malaysia, Kuala Lumpur | 1 year | - All patients undergoing colonoscopy |
| Hippisley-Cox 2012 [37] | Cohort study using data from 375 UK QResearch® general practices for development and 189 for validation. | 4.1 million person years | All practices in England and Wales that had been using their EMIS (Egton Medical Information System) computer system for at least a year. | 10 years | - 30–84 years - free at baseline from a diagnosis of colorectal cancer and without rectal bleeding, abdominal pain, appetite loss, or weight loss in the previous 12 months. - colorectal cancer recorded in the next 2 years |
| Simpkins 2017 [38] | Prospective | 1981 | The McMaster University Medical Center, and St. Joseph’s Healthcare, Hamilton, Canada | 4 years, | - Lower GI symptoms. - Assessors were blinded to symptom status. - Reference: histopathological confirmation - Controls: patients without CRC. |
| Hamilton 2005 [41] | Population based Case-control, retrospective | 2093 | 21 GP’s, Exeter, Devon, UK | 4 years | - full medical record for 2 years before diagnosis was coded using the International Classification of Primary Care-2. |
| Koning 2015 [40] | Cross-sectional | 3855 | Julius General Practitioners’ Network (JGPN) database Utrecht area, Netherlands | 5 years | - Referred for colonoscopy by GP - Data were obtained from the Julius General Practitioners’ Network (JGPN) database. - Exclusion: history of CRC |
| Hamilton 2008 [59] | Case-control | 51,508 | Database UK | 6 years | - data from The Health Improvement Network (electronic medical records from GP practices) - >30 years with CRC |
| Hamilton 2009 [39] | Case-control | 43,791 | Database UK | 5 years | - Data were provided by The Health Improvement Network - 2 years of data - Patients >30 years with CRC |
| De Bosset 2002 [42] | Prospective, observational | 1188 | Two district hospitals; Porrentruy and Dele mont, one university hospital and its outpatient department in Zurich and two gastroenterology practices in Delemont and Yverdon in Switzerland. | 17 months | - Consecutive patients referred for diagnostic Colonoscopy Swiss criteria developed by the Rand Corporation/University of California at Los Angeles (RAND/UCLA) panel method |
| Cai 2002 [43] | Retrospective | 580 | First Affiliated Hospital of Chongqing Medical University, southwest China. | 6 years | - Colonoscopic findings from patients with chronic abdominal pain, chronic diarrhea and constipation systematically analyzed in retrospect. - 13–77 years old |
| Pepin 2002 [44] | Retrospective | 563 | Moffitt- Long Hospital (MLH), General Hospital (SFGH) and the San Francisco Veterans Administration Medical Center (SFVAMC), San Francisco, US | 3 years | - endoscopic database was searched systematically to identify all patients who underwent sigmoidoscopy (SIG) or colonoscopy (COL) for constipation. |
| Flashman 2004 [45] | Prospective | 249 | Queen Alexandra Hospital, Cosham, Portsmouth | 1 year | - All patients with bowel cancer; all patients referred on the basis of the two week standard and to a routine colorectal surgical outpatient clinic. |
| Du toit 2006 [46] | Cohort | 265 | GP practice in the UK | 10 years | - Participants: Patients aged 45 or more with new onset rectal bleeding, irrespective of other symptoms. - Main outcome: Percentage of participants in whom colorectal cancer or colonic adenoma was identified after investigation of the bowel. |
| Nakama 2000 [47] | Cross-sectional | 9625 | Japan | 4 years | - Medical check up - Colonoscopy + Fobt (for screening) - 2 groups: rectal bleeding or not - No other symptoms |
| Wauters 2000 [48] | Retrospective | 83,890 | A network of sentinel practices, Belgium, (covering 1% of the population), | 1 year | - Patients presenting with rectal bleeding - Reference standard: CRC |
| Ahmed 2005 [49] | Prospective | 563 | Scotland | 1 year | - consecutive individuals with a positive FOB test in the Scottish arm of the national colorectal cancer screening pilot - standard questionnaire to elicit gastrointestinal symptoms; |
| Brenna 1990 [50] | Prospective | 833 | Trondheim Regional and University Hospital, Trondheim, Norway | 1 year | - Referred for colonoscopy |
| Mc donald 2013 [51] | Prospective | 280 | Ninewells Hospital and Medical School, Dundee, UK | 2 years | - referred from primary care for endoscopic examination of the lower gastrointestinal tract - Symptomatic patients - single sample faecal collection for Hb concentration measurement. - >16 year |
| Elias 2016 [52] | Prospective | 810 | 266 Dutch primary care practices | 3 years | - SCD-suspected patients referred for endoscopy to develop a diagnostic model for SCD with routine clinical information, with faecal calprotectin POC (quantitatively in μg/g faeces) and/or POC FIT results (qualitatively with a 6 μg/g faeces detection limit). - SCD: colorectal cancer (CRC), inflammatory bowel disease, diverticulitis, or advanced adenoma (>1 cm). |
| Hogberg 2017 [53] | Prospective | 373 | Four health care centres in Region Jamtland Harjedalen, Sweden | 1 year | - consecutive patients that received a FIT or a FC test ordered by a primary care physician. - samples for FITs, FC tests, full blood counts and iron-deficiency tests. - Physicians were instructed to refer patients with a positive FIT or FC test (cut-off 100 lg/g) for bowel imaging. - The patients’ presenting symptoms were recorded. |
| Mowat 2016 [54] | Prospective | 1031 | Ninewells Hospital and Medical School, Dundee, UK | 5 months | - All adult patients referred for investigation of bowel symptoms - GPs: FHb and FC, full blood count, urea and electrolytes and CRP and record the presenting symptoms via the NHS Tayside electronic test requesting software. - More than one presenting symptom → attributed to one. - FHB detectable and >10. |
| Cubiela 2014 [55] | multicentre, prospective, blind study | 787 | two tertiary hospitals in northern Spain. | 7 months | - patients referred for a diagnostic colonoscopy, patients with NICE and SIGN referral criteria. - All patients one FIT determination (OCsensor™) - (CRISP) questionnaire was used to record symptoms - Exclusion: age under 18, pregnancy, asymptomatic individuals for CRC screening, patients with a history of colonic for surveillance colonoscopy, patients requiring hospital admission, patients whose symptoms had ceased within 3 months before evaluation |
| Cubiela 2016 [56] | Prospective cross-sectional study | 3053 | Complexo Hospitalario Universitario de Ourense, Spain. | 19 months | - consecutive patients with gastrointestinal symptoms referred for colonoscopy In the derivation cohort, assessed symptoms, NICE referral criteria, levels of faecal haemoglobin and calprotectin, blood haemoglobin, and serum carcinoembryonic antigen before colonoscopy. - Exclusion: age under 18, pregnancy, asymptomatic individuals for CRC screening, patients with a history of colonic for surveillance colonoscopy, patients requiring hospital admission, patients whose symptoms had ceased within 3 months before evaluation |
| Steine 1994 [26] | Prospective | 1852 | Oslo, Norway | - | - referred from primary health care for a double-contrast barium enema |
| Zarchy 1991 [31] | Prospective | 794 | large multispecialty medical group, LA | - | - Physicians completed a form before ordering a double-contrast barium enema, listing information about patient history, symptoms, and objective findings, including the results of a complete blood count, stool hemoccult, and sigmoidoscopy |
| Rodriguez 2015 [57] | Prospective | 1054 | Bellvitge UniversityHospital Spain | 25 months | - symptomatic patients referred for a colonoscopy who provided a sample for faecal immunochemical testing - >18 years - Exclusion: adenoma surveillance andpostoperative surveillance of CRC. Hospitalized patients and those with a history of previous colectomy, IBD and polyp syndrome, incomplete colonoscopies were included only if the cause was a stenosing neoplasm. |
| Law 2014 [58] | Cross-sectional, prospective | 1013 | University Malaya, Kuala Lumpur, Malaysia | 20 months | - symptomatic adults referred for an index colonoscopy. - Questionnaire - Complete examination |
References
- Ferlay, J.; Autier, P.; Boniol, M.; Heanue, M.; Colombet, M.; Boyle, P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann. Oncol. 2007, 18, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Knottnerus, J.A. Bevolkingsonderzoek naar darmkanker. Bijblijven 2009, 25, 34–44. [Google Scholar]
- O’Connell, J.B.; Maggard, M.A.; Ko, C.Y. Colon cancer survival rates with the new American Joint Committee on Cancer sixth edition staging. J. Natl. Cancer Inst. 2004, 96, 1420–1425. [Google Scholar] [CrossRef]
- Van Veldhuizen-Eshuis, H.; Carpay, M.E.M.; van Delden, J.A.; Grievink, L.; Hoebee, B.; Lock, A.J.J.; Reij, R. Uitvoeringstoets Bevolkingsonderzoek Darmkanker: Opsporing van Darmkanker in Praktijk Gebracht; National Institute for Public Health and the Environment: Bilthoven, MA, USA, 2011. [Google Scholar]
- Adelstein, B.-A.; Macaskill, P.; Chan, S.F.; Katelaris, P.H.; Irwig, L. Most bowel cancer symptoms do not indicate colorectal cancer and polyps: A systematic review. BMC Gastroenterol. 2011, 11, 65. [Google Scholar] [CrossRef]
- Astin, M.; Griffin, T.; Neal, R.D.; Rose, P.; Hamilton, W. The diagnostic value of symptoms for colorectal cancer in primary care: A systematic review. Br. J. Gen. Pract. 2011, 61, e231–e243. [Google Scholar] [CrossRef] [PubMed]
- Ford, A.C.; Zanten, S.J.O.V.V.; Rodgers, C.C.; Talley, N.J.; Vakil, N.B.; Moayyedi, P. Diagnostic utility of alarm features for colorectal cancer: Systematic review and meta-analysis. Gut 2008, 57, 1545–1553. [Google Scholar] [CrossRef]
- Jellema, P.; Windt, D.A.W.M.V.D.; Bruinvels, D.; Mallen, C.; Van Weyenberg, S.J.B.; Mulder, C.J.; De Vet, H.C.W. Value of symptoms and additional diagnostic tests for colorectal cancer in primary care: Systematic review and meta-analysis. BMJ 2010, 340, c1269. [Google Scholar] [CrossRef]
- Olde Bekkink, M.; McCowan, C.; Falk, G.A.; Teljeur, C.; Van de Laar, F.A.; Fahey, T. Diagnostic accuracy systematic review of rectal bleeding in combination with other symptoms, signs and tests in relation to colorectal cancer. Br. J. Cancer 2010, 102, 48–58. [Google Scholar] [CrossRef]
- Morini, S.; Hassan, C.; Meucci, G.; Toldi, A.; Zullo, A.; Minoli, G. Diagnostic yield of open access colonoscopy according to appropriateness. Gastrointest. Endosc. 2001, 54, 175–179. [Google Scholar] [CrossRef]
- Gonvers, J.J.; Harris, J.K.; Wietlisbach, V.; Burnand, B.; Vader, J.P.; Froehlich, F.; EPAGE study group. A European view of diag-nostic yield and appropriateness of colonoscopy. Hepatogastroenterology 2007, 54, 729–735. [Google Scholar]
- Muris, J.W.; Starmans, R.; Fijten, G.H.; Crebolder, H.F.; Schouten, H.J.; Knottnerus, J.A. Non-acute abdominal complaints in general practice: Diagnostic value of signs and symptoms. Br. J. Gen. Pract. 1995, 45, 313–316. [Google Scholar] [PubMed]
- Hassan, C.; Di Giulio, E.; Pickhardt, P.J.; Zullo, A.; Laghi, A.; Kim, D.H.; Lafrate, F.; Morini, S. Cost effectiveness of colonoscopy, based on the appropriateness of an indication. Clin. Gastroenterol. Hepatol. 2008, 6, 1231–1236. [Google Scholar] [CrossRef] [PubMed]
- Hewitson, P.; Glasziou, P.; Irwig, L.; Towler, B.; Watson, E. Screening for colorectal cancer using the faecal occult blood test, Hemoccult. Cochrane Database Syst. Rev. 2007, 1, CD001216. [Google Scholar] [CrossRef] [PubMed]
- Young, G.P.; Symonds, E.L.; Allison, J.E.; Cole, S.R.; Fraser, C.G.; Halloran, S.P.; Kuipers, E.J.; Seaman, H.E. Advances in Fecal Occult Blood Tests: The FIT revolution. Dig. Dis. Sci. 2015, 60, 609–622. [Google Scholar] [CrossRef]
- Young, G.P.; Fraser, C.G.; Halloran, S.P.; Cole, S. Guaiac based faecal occult blood testing for colorectal cancer screening: An obsolete strategy? Gut 2012, 61, 959–960. [Google Scholar] [CrossRef] [PubMed]
- Halloran, S.P.; Launoy, G.; Zappa, M. International Agency for Research on Cancer. European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition--Faecal occult blood testing. Endoscopy 2012, 44 (Suppl. 3), SE6–SE87. [Google Scholar]
- Rabeneck, L.; Rumble, R.B.; Thompson, F.; Mills, M.; Oleschuk, C.; Whibley, A.; Messersmith, H.; Lewis, N.; Panel, T.F.G.E. Fecal Immunochemical Tests Compared with Guaiac Fecal Occult Blood Tests for Population-Based Colorectal Cancer Screening. Can. J. Gastroenterol. 2012, 26, 131–147. [Google Scholar] [CrossRef]
- Wiersma, T.; de Wit, N.; Drenthen, T. NHG-Standpunt Bevolkingsonderzoek darmkanker. Huisarts En Wet. 2013, 56, 640–643. [Google Scholar]
- Newland, A.; Kroese, M.; Akehurst, R.; Crawfors, S. Quantitative Faecal Immunochemical Tests to Guide Referral for Colorectal Cancer in Primary Care; The National Institute for Health and Care Excellence: London, UK, 26 July 2017. [Google Scholar]
- Bafandeh, Y.; Khoshbaten, M.; Sadat, A.T.E.; Farhang, S. Clinical predictors of colorectal polyps and carcinoma in a low prevalence region: Results of a colonoscopy based study. World J. Gastroenterol. 2008, 14, 1534–1538. [Google Scholar] [CrossRef]
- Bjerregaard, N.C.; Tøttrup, A.; Sørensen, H.T.; Laurberg, S. Diagnostic value of self-reported symptoms in Danish outpatients referred with symptoms consistent with colorectal cancer. Color. Dis. 2007, 9, 443–451. [Google Scholar] [CrossRef]
- Brewster, N.T.; Grieve, D.C.; Saunders, J.H. Double-contrast barium enema and flexible sigmoidoscopy for routine colonic investigation. Br. J. Surg. 1994, 81, 445–447. [Google Scholar] [CrossRef]
- Farrands, P.A.; O’Regan, D.; Taylor, I. An assessment of occult blood testing to determine which patients with large bowel symptoms require urgent investigation. Br. J. Surg. 1985, 72, 835–837. [Google Scholar] [CrossRef] [PubMed]
- Selvachandran, S.; Hodder, R.; Ballal; Jones, P.; Cade, D. Prediction of colorectal cancer by a patient consultation questionnaire and scoring system: A prospective study. Lancet 2002, 360, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Steine, S.; Stordahl, A.; Laerum, F.; Laerum, E.; Lærum, F.; Lærum, E. Referrals for Double-Contrast Barium Examination: Factors Influencing the Probability of Finding Polyps or Cancer. Scand. J. Gastroenterol. 1994, 29, 260–264. [Google Scholar] [CrossRef]
- Tan, Y.M.; Rosmawati, M.; Ranjeev, P.; Goh, K.L. Predictive factors by multivariate analysis for colorectal cancer in Malaysian patients undergoing colonoscopy. J. Gastroenterol. Hepatol. 2002, 17, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Tate, J.J.; Royle, G.T. Open access colonoscopy for suspected colonic neoplasia. Gut 1988, 29, 1322–1325. [Google Scholar] [CrossRef]
- Thompson, M.R.; Perera, R.; Senapati, A.; Dodds, S. Predictive value of common symptom combinations in diagnosing colo-rectal cancer. Br. J. Surg. 2007, 94, 1260–1265. [Google Scholar] [CrossRef]
- Thompson, M.R.; Flashman, K.G.; Wooldrage, K.; Rogers, P.A.; Senapati, A.; O’Leary, D.P.; Atkin, W. Flexible sigmoidoscopy and whole colonic imaging in the diagnosis of cancer in patients with colorectal symptoms. Br. J. Surg. 2008, 95, 1140–1146. [Google Scholar] [CrossRef]
- Zarchy, T.M.; Ershoff, D. Which clinical variables predict an abnormal double-contrast barium enema result? Ann. Intern. Med. 1991, 114, 137–141. [Google Scholar] [CrossRef]
- Panzuto, F.; Chiriatti, A.; Bevilacqua, S.; Giovannetti, P.; Russo, G.; Impinna, S.; Pistilli, F.; Capurso, G.; Annibale, B.; Fave, G.D. Symptom-based approach to colorectal cancer: Survey of primary care physicians in Italy. Dig. Liver Dis. 2003, 35, 869–875. [Google Scholar] [CrossRef]
- Curless, R.; French, J.; Williams, G.V.; James, O.F. Comparison of gastrointestinal symptoms in colorectal carcinoma patients and community controls with respect to age. Gut 1994, 35, 1267–1270. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.; Kewenter, J.; Swedenborg, J. The Correlation of Symptoms, Occult Blood Tests, and Neoplasms in Patients Referred for Double-Contrast Barium Enema. Scand. J. Gastroenterol. 1993, 28, 911–914. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.; Doulias, T.; Hoad, T.; Lee, C.; Alberts, J.C. Primary-to-secondary care referral experience of suspected colorectal ma-lignancy in young adults. Ann. R. Coll. Surg. Engl. 2016, 98, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Cheong, K.L.; Roohi, S.A.; Jarmin, R.; Sagap, I.; Tong, S.H.; Qureshi, A. The yield for colorectal cancer and adenoma by indication at colonoscopy. Med. J. Malays. 2000, 55, 464–466. [Google Scholar]
- Hippisley-Cox, J.; Coupland, C. Identifying patients with suspected colorectal cancer in primary care: Derivation and val-idation of an algorithm. Br. J. Gen. Pract. 2012, 62, e29–e37. [Google Scholar] [CrossRef] [PubMed]
- Simpkins, S.J.; Pinto-Sanchez, M.I.; Moayyedi, P.; Bercik, P.; Morgan, D.G.; Bolino, C.; Ford, A.C. Poor predictive value of lower gastrointestinal alarm features in the diagnosis of colorectal cancer in 1981 patients in secondary care. Aliment. Pharmacol. Ther. 2017, 45, 91–99. [Google Scholar] [CrossRef]
- Hamilton, W.; Lancashire, R.; Sharp, D.; Peters, T.J.; Cheng, K.; Marshall, T. The risk of colorectal cancer with symptoms at different ages and between the sexes: A case-control study. BMC Med. 2009, 7, 17. [Google Scholar] [CrossRef]
- Koning, N.R.; Moons, L.M.; Buchner, F.L.; Helsper, C.W.; Ten Teije, A.; Numans, M.E. Identification of patients at risk for colorectal cancer in primary care: An explorative study with routine healthcare data. Eur. J. Gastroenterol. Hepatol. 2015, 27, 1443–1448. [Google Scholar] [CrossRef]
- Hamilton, W.; Round, A.; Sharp, D.; Peters, T. Clinical features of colorectal cancer before diagnosis: A population-based case–control study. Br. J. Cancer 2005, 93, 399–405. [Google Scholar] [CrossRef]
- de Bosset, V.; Froehlich, F.; Rey, J.P.; Thorens, J.; Schneider, C.; Wietlisbach, V.; Vader, J.P.; Burnand, B.; Muhlhaupt, B.; Fried, M.; et al. Do explicit appropriateness criteria enhance the diagnostic yield of colonoscopy? Endoscopy 2002, 34, 360–368. [Google Scholar] [CrossRef]
- Cai, J.; Yuan, Z.; Zhang, S. Abdominal pain, diarrhea, constipation--which symptom is more indispensable to have a colon-oscopy? Int. J. Clin. Exp. Pathol. 2015, 8, 938–942. [Google Scholar] [PubMed]
- Pepin, C.; Ladabaum, U. The yield of lower endoscopy in patients with constipation: Survey of a university hospital, a public county hospital, and a Veterans Administration medical center. Gastrointest. Endosc. 2002, 56, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Flashman, K.; O’Leary, D.P.; Senapati, A.; Thompson, M.R. The Department of Health’s “two week standard” for bowel cancer: Is it working? Gut 2004, 53, 387–391. [Google Scholar] [CrossRef] [PubMed]
- du Toit, J.; Hamilton, W.; Barraclough, K. Risk in primary care of colorectal cancer from new onset rectal bleeding: 10 year prospective study. BMJ 2006, 333, 69–70. [Google Scholar] [CrossRef]
- Nakama, H.; Zhang, B.; Fattah, A.A.; Kamijo, N.; Fukazawa, K. Relationships between a sign of rectal bleeding and the results of an immunochemical occult blood test, and colorectal cancer. Eur. J. Cancer Prev. 2000, 9, 325–328. [Google Scholar] [CrossRef]
- Wauters, H.; Van Casteren, V.; Buntinx, F. Rectal bleeding and colorectal cancer in general practice: Diagnostic study. BMJ 2000, 321, 998–999. [Google Scholar] [CrossRef]
- Ahmed, S.; Leslie, A.; Thaha, M.A.; Carey, F.A.; Steele, R.J.C. Lower gastrointestinal symptoms are not predictive of colorectal neoplasia in a faecal occult blood screen-positive population. Br. J. Surg. 2005, 92, 478–481. [Google Scholar] [CrossRef]
- Brenna, E.; Skreden, K.; Waldum, H.L.; Marvik, R.; Dybdahl, J.H.; Kleveland, P.M.; Sandvik, A.K.; Halvorsen, T.; Myrvold, H.E.; Petersen, H. The benefit of colonoscopy. Scand. J. Gastroenterol. 1990, 25, 81–88. [Google Scholar] [CrossRef]
- McDonald, P.J.; Digby, J.; Innes, C.; Strachan, J.A.; Carey, F.A.; Steele, R.J.; Fraser, C.G. Low faecal haemoglobin concentration potentially rules out significant colorectal disease. Color. Dis. 2013, 15, e151–e159. [Google Scholar] [CrossRef]
- Elias, S.G.; Kok, L.; de Wit, N.J.; Witteman, B.J.M.; Goedhard, J.G.; Romberg-Camps, M.J.L.; Muris, J.W.M.; Moons, K.G.M. Is there an added value of faecal calprotectin and haemoglobin in the diagnostic work-up for primary care patients suspected of significant colorectal disease? A cross-sectional diagnostic study. BMC Med. 2016, 14, 141. [Google Scholar] [CrossRef]
- Högberg, C.; Karling, P.; Rutegård, J.; Lilja, M. Diagnosing colorectal cancer and inflammatory bowel disease in primary care: The usefulness of tests for faecal haemoglobin, faecal calprotectin, anaemia and iron deficiency. A prospective study. Scand. J. Gastroenterol. 2017, 52, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Mowat, C.; Digby, J.; Strachan, J.A.; Wilson, R.; Carey, F.A.; Fraser, C.G.; Steele, R.J.C. Faecal haemoglobin and faecal calprotectin as indicators of bowel disease in patients presenting to primary care with bowel symptoms. Gut 2016, 65, 1463–1469. [Google Scholar] [CrossRef]
- Cubiella, J.; Salve, M.; Díaz-Ondina, M.; Vega, P.; Alves, M.T.; Iglesias, F.; Sánchez, E.; Macía, P.; Blanco, I.; Bujanda, L.; et al. Diagnostic accuracy of the faecal immunochemical test for colorectal cancer in symptomatic patients: Comparison with NICE and SIGN referral criteria. Color. Dis. 2014, 16, O273–O282. [Google Scholar] [CrossRef] [PubMed]
- Cubiella, J.; Vega, P.; Salve, M.; Díaz-Ondina, M.; Alves, M.T.; Quintero, E.; Álvarez-Sánchez, V.; Fernández-Bañares, F.; Boadas, J.; Campo, R.; et al. Development and external validation of a faecal immunochemical test-based prediction model for colorectal cancer detection in symptomatic patients. BMC Med. 2016, 14, 128. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Alonso, L.; Rodríguez-Moranta, F.; Ruiz-Cerulla, A.; Lobatón, T.; Arajol, C.; Binefa, G.; Moreno, V.; Guardiola, J. An urgent referral strategy for symptomatic patients with suspected colorectal cancer based on a quantitative immunochemical faecal occult blood test. Dig Liver Dis. 2015, 47, 797–804. [Google Scholar] [CrossRef]
- Law, C.-W.; Rampal, S.; Roslani, A.C.; Mahadeva, S. Development of a risk score to stratify symptomatic adults referred for colonoscopy. J. Gastroenterol. Hepatol. 2014, 29, 1890–1896. [Google Scholar] [CrossRef]
- Hamilton, W.; Lancashire, R.; Sharp, D.; Peters, T.; Cheng, K.; Marshall, T. The importance of anaemia in diagnosing colorectal cancer: A case–control study using electronic primary care records. Br. J. Cancer 2008, 98, 323–327. [Google Scholar] [CrossRef]


{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bafandeh 2008 [21] | + | +/− | + | + | + | + | ? | + | + | − | − | + | + | + |
| Bjerregaard 2006 [22] | + | + | + | + | + | + | + | + | + | +/− | +/− | + | ? | + |
| Brewster 1994 [23] | + | +/− | − | + | + | − | + | − | + | + | +/− | + | − | − |
| Farrands 1985 [24] | + | +/− | +/− | + | + | +/− | + | +/− | + | + | +/− | + | ? | − |
| Selvachandran 2002 [25] | + | +/− | + | + | + | +/− | + | + | + | + | +/− | + | ? | + |
| Steine 1994 [26] | NB | |||||||||||||
| Tan 2002 [27] | + | +/− | + | + | + | + | + | +/− | + | +/− | +/− | + | ? | − |
| Tate 1988 [28] | + | +/− | + | + | + | +/− | + | +/− | + | − | +/− | + | ? | + |
| Thompson 2007 [29] | + | + | +/− | + | + | + | + | + | + | + | − | + | ? | − |
| Thompson 2008 [30] | + | + | +/− | + | + | +/− | + | +/− | + | + | +/− | + | ? | − |
| Zarchy 1991 [31] | NB | |||||||||||||
| Panzuto 2003 [32] | + | + | + | + | + | +/− | + | + | + | + | +/− | + | ? | + |
| Curless 1994 [33] | + | + | + | + | + | − | + | +/− | + | − | + | − | ? | + |
| Jensen 1993 [34] | + | +/− | +/− | + | + | +/− | + | +/− | + | +/− | − | + | ? | ? |
| Patel 2016 [35] | + | +/− | + | + | + | +/− | + | +/− | + | − | +/− | + | ? | ? |
| Cheong 2000 [36] | + | +/− | + | + | + | +/− | + | +/− | + | +/− | +/− | + | ? | ? |
| Hipsley-Cox 2012 [37] | + | + | + | ? | + | +/− | + | + | +/− | − | ? | + | − | + |
| Simpkins 2017 [38] | + | + | + | + | + | +/− | + | + | + | + | + | + | ? | + |
| Hamilton 2009 [39] | + | + | + | + | + | + | + | + | + | + | +/− | + | ? | ? |
| Koning 2015 [40] | + | + | + | + | + | +/− | + | + | + | + | − | + | ? | ? |
| Hamilton 2005 [41] | + | + | ? | ? | ? | ?+ | + | +/− | ? | − | ? | + | − | + |
| De Bosset 2002 [42] | + | + | + | + | + | + | + | + | + | + | − | + | ? | ? |
| Cai 2015 [43] | +/− | +/− | + | + | + | +/− | + | +/− | + | + | − | + | ? | ? |
| Pepin 2002 [44] | + | + | + | + | + | + | + | +/− | + | +/− | +/− | + | ? | ? |
| Flashman 2004 [45] | +/− | + | + | + | + | +/− | + | + | + | + | + | + | ? | + |
| Du toit 2006 [46] | + | − | + | + | + | − | + | +/− | + | + | − | + | ? | ? |
| Nakama 2000 [47] | + | + | + | + | + | + | + | + | + | + | − | − | ? | ? |
| Wauters 2000 [48] | + | +/− | + | + | +/− | +/− | + | +/− | +/− | +/− | +/− | ? | ? | − |
| Ahmet 2005 [49] | +/− | + | + | + | + | − | + | + | + | +/− | +/− | + | − | + |
| Brenna 1990 [50] | + | +/− | + | + | + | −/+ | + | − | + | + | − | + | − | + |
| Mc donald 2013 [51] | + | + | + | + | + | + | + | + | + | ? | ? | + | ? | − |
| Elias 2016 [52] | + | + | + | + | + | +/− | + | + | + | + | + | + | ? | + |
| Hogberg 2017 [53] | + | + | + | + | − | − | + | + | + | + | − | + | ? | + |
| Mowat 2016 [54] | + | +/− | + | + | + | + | + | + | + | + | + | + | ? | + |
| Cubiela 2014 [55] | + | + | + | + | + | + | + | +/− | + | + | + | + | ? | + |
| Cubiela 2016 [56] | + | + | + | + | + | + | + | + | + | + | + | + | ? | + |
| Rodriguez 2015 [57] | + | + | + | + | + | + | + | + | + | + | + | + | ? | + |
| Law 2014 [58] | + | +/− | + | + | + | + | + | +/− | + | + | ? | + | ? | + |
|
Pooled Sensitivity |
Pooled Specificity |
Pooled Likelihood + |
Pooled Likelihood − | Pooled DOR | |
|---|---|---|---|---|---|
| Changed bowel habit |
0.235 (0.226–0.244) |
0.974 (0.974–0.973) |
1.603 (1.194–2.151) |
0.841 (0.773–0.914) |
1.979 (1.158–3.382) |
| Diarrhea |
0.192 (0.182–0.202) |
0.635 (0.625–0.644) |
0.747 (0.278–2.008) |
1.119 (0.684–1.834) |
0.650 (0.139–3.050) |
| Obstipation |
0.266 (0.254–0.277) |
0.888 (0.885–0.891) |
1.168 (0.754–1.809) |
1.022 (0.900–1.161) |
1.177 (0.698–1.986) |
| Anemia |
0.285 (0.274–0.297) |
0.985 (0.985–0.984) |
2.661 (1.911–3.704) |
0.818 (0.707–0.947) |
3.490 (2.523–4.826) |
| Abdominal pain |
0.329 (0.319–0.340) |
0.741 (0.743–0.738) |
1.176 (0.825- 1.676) |
1.006 (0.894–1.133) |
1.161 (0.703–1.918) |
| Weight loss |
0.116 (0.110–0.123) |
0.986 (0.987–0.986) |
2.358 (1.684–3.300) |
0.902 (0.863–0.943) |
2.741 (1.835–4.094) |
| Rectal blood loss |
0.313 (0.305–0.322) |
0.963 (0.963–0.963) |
2.037 (1.286–3.227) |
0.837 (0.767–0.913) |
2.501 (1.337–4.677) |
| Abdominal mass |
0.055 (0.030–0.090) |
0.969 (0.963–0.974) |
1.780 (0.798–3.969) |
0.991 (0.950–1.033) |
1.018 (0.364–2.843) |
| Cumulative symptoms | 0.248 (0.244–0.251) | 0.972 (0.971–0.972) | 1.620 (1.356–1.936) | 0.923 (0.896–0.951) | 1.792 (1.389–2.311) |
| Pooled Sensitivity | Pooled Specificity | Pooled Likelihood + | Pooled Likelihood − | Pooled DOR | |
|---|---|---|---|---|---|
| FIT |
0.830 (0.792–0.863) |
0.765 (0.755–0.775) |
3.886 (2.640–5.721) |
0.155 (0.086–0.278) |
27,025 (18,509–39,459) |
| Effect Size | Chi Square | I2% | p |
|---|---|---|---|
| Sensitivity | 63.19 | 82.6 | 0.000 |
| Specificity | 725.01 | 98.5 | 0.000 |
| Positive likelihood ratio | 589.80 | 98.1 | 0.000 |
| Negative likelihood ratio | 39.82 | 72.4 | 0.000 |
| Diagnostic odds ratio | 12.80 | 14 | 0.307 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brands, H.J.; Van Dijk, B.; Brohet, R.M.; van Westreenen, H.L.; de Groot, J.W.B.; Moons, L.M.G.; de Vos tot Nederveen Cappel, W.H. Possible Value of Faecal Immunochemical Test (FIT) When Added in Symptomatic Patients Referred for Colonoscopy: A Systematic Review. Cancers 2023, 15, 2011. https://doi.org/10.3390/cancers15072011
Brands HJ, Van Dijk B, Brohet RM, van Westreenen HL, de Groot JWB, Moons LMG, de Vos tot Nederveen Cappel WH. Possible Value of Faecal Immunochemical Test (FIT) When Added in Symptomatic Patients Referred for Colonoscopy: A Systematic Review. Cancers. 2023; 15(7):2011. https://doi.org/10.3390/cancers15072011
Chicago/Turabian StyleBrands, Henrike Jacoba, Brigit Van Dijk, Richard M. Brohet, Henderik L. van Westreenen, Jan Willem B. de Groot, Leon M. G. Moons, and Wouter H. de Vos tot Nederveen Cappel. 2023. "Possible Value of Faecal Immunochemical Test (FIT) When Added in Symptomatic Patients Referred for Colonoscopy: A Systematic Review" Cancers 15, no. 7: 2011. https://doi.org/10.3390/cancers15072011
APA StyleBrands, H. J., Van Dijk, B., Brohet, R. M., van Westreenen, H. L., de Groot, J. W. B., Moons, L. M. G., & de Vos tot Nederveen Cappel, W. H. (2023). Possible Value of Faecal Immunochemical Test (FIT) When Added in Symptomatic Patients Referred for Colonoscopy: A Systematic Review. Cancers, 15(7), 2011. https://doi.org/10.3390/cancers15072011