
Peripheral T-Cell Lymphomas: Therapeutic Approaches


Abstract
:Simple Summary
Abstract
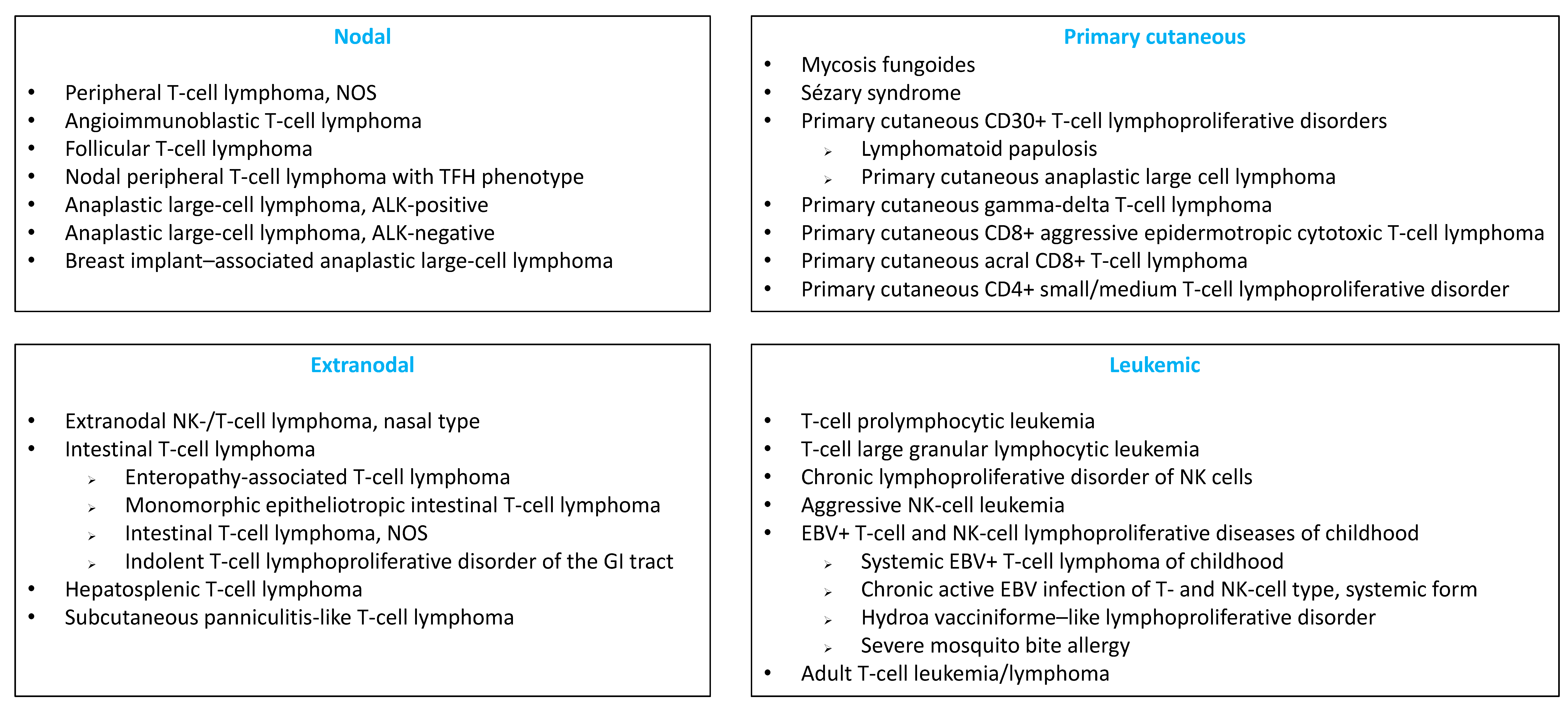
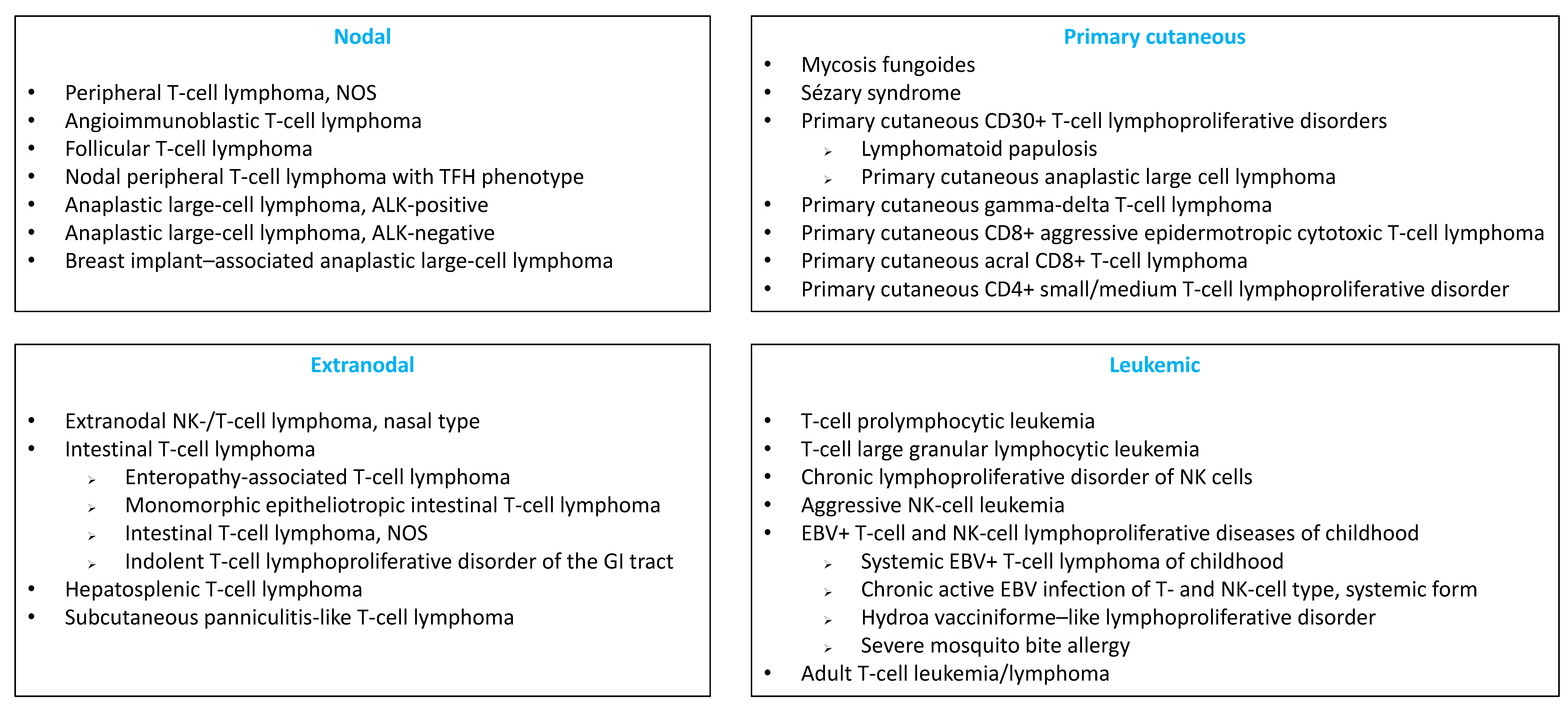
1. Introduction
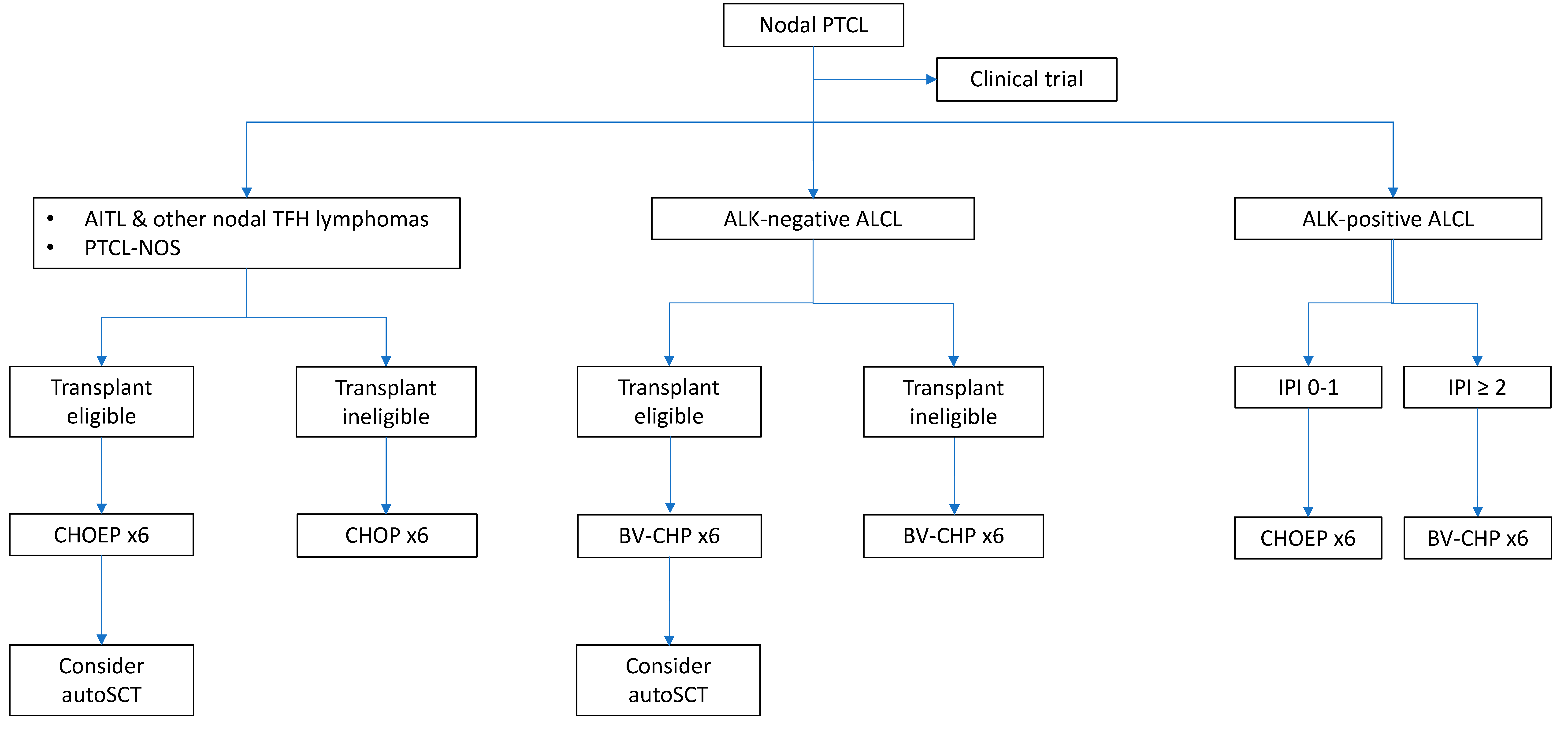
2. Frontline Treatment of PTCLs
2.1. How to Improve CHOP?
2.1.1. CHOEP and Other Intensive Chemotherapy Regimens
2.1.2. Combination of CHOP with Novel Agents
2.1.3. Randomized Studies Challenging CHOP
2.2. The role of Consolidative Hematopoietic Stem-Cell Transplantation
2.2.1. Autologous Stem-Cell Transplantation
Prospective Studies
Retrospective Studies
2.2.2. Allogeneic Stem-Cell Transplantation
Prospective Studies
Retrospective Studies
2.3. What Can Be Learned from Studies Dedicated to A Single Nodal PTCL Entity?
3. Treatment of Relapsed/Refractory PTCLs
3.1. How Many Patients Relapse or Progress?
3.2. What Is the Outcome after the First Event of Progression/Relapse?
3.3. Second-Line Chemotherapy Regimen for PTCL-NOS and AITL
3.4. Treatment of R-R ALCL
3.5. What Is the Role of Hematopoietic Stem-Cell Transplantation in R-R PTCLs?
3.5.1. Autologous Stem-Cell Transplantation
3.5.2. Allogeneic Stem-Cell Transplantation
3.5.3. Autologous or Allogeneic Stem-Cell Transplantation?
3.6. Novel Agents
4. Conclusions
Funding
Conflicts of Interest
References
- Swerdlow, S.H.; Campo, E.; Harris, N.L.; Jaffe, E.S.; Pileri, S.; Stein, H.; Thiele, J. WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues, Revised 4th ed.; IARC: Lyon, France, 2017. [Google Scholar]
- International T-Cell Lymphoma Project. International Peripheral T-Cell and Natural Killer/T-Cell Lymphoma Study: Pathology Findings and Clinical Outcomes. J. Clin. Oncol. 2008, 26, 4124–4130. [Google Scholar] [CrossRef] [PubMed]
- Laurent, C.; Baron, M.; Amara, N.; Haioun, C.; Dandoit, M.; Maynadié, M.; Parrens, M.; Vergier, B.; Copie-Bergman, C.; Fabiani, B.; et al. Impact of Expert Pathologic Review of Lymphoma Diagnosis: Study of Patients From the French Lymphopath Network. J. Clin. Oncol. 2017, 35, 2008–2017. [Google Scholar] [CrossRef] [PubMed]
- Hsi, E.D.; Horwitz, S.M.; Carson, K.R.; Pinter-Brown, L.C.; Rosen, S.T.; Pro, B.; Federico, M.; Gisselbrecht, C.; Schwartz, M.; Bellm, L.; et al. Analysis of Peripheral T-cell Lymphoma Diagnostic Workup in the United States. Clin. Lymphoma Myeloma Leuk. 2017, 17, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Fiore, D.; Cappelli, L.V.; Broccoli, A.; Zinzani, P.L.; Chan, W.C.; Inghirami, G. Peripheral T cell lymphomas: From the bench to the clinic. Nat. Cancer 2020, 20, 323–342. [Google Scholar] [CrossRef]
- Savage, K.J.; Harris, N.L.; Vose, J.M.; Ullrich, F.; Jaffe, E.S.; Connors, J.M.; Rimsza, L.; Pileri, S.A.; Chhanabhai, M.; Gascoyne, R.D.; et al. ALK− anaplastic large-cell lymphoma is clinically and immunophenotypically different from both ALK+ ALCL and peripheral T-cell lymphoma, not otherwise specified: Report from the International Peripheral T-Cell Lymphoma Project. Blood 2008, 111, 5496–5504. [Google Scholar] [CrossRef]
- Schmitz, N.; Trümper, L.; Ziepert, M.; Nickelsen, M.; Ho, A.D.; Metzner, B.; Peter, N.; Loeffler, M.; Rosenwald, A.; Pfreundschuh, M. Treatment and prognosis of mature T-cell and NK-cell lymphoma: An analysis of patients with T-cell lymphoma treated in studies of the German High-Grade Non-Hodgkin Lymphoma Study Group. Blood 2010, 116, 3418–3425. [Google Scholar] [CrossRef] [Green Version]
- Sibon, D.; Fournier, M.; Brière, J.; Lamant, L.; Haioun, C.; Coiffier, B.; Bologna, S.; Morel, P.; Gabarre, J.; Hermine, O.; et al. Long-Term Outcome of Adults With Systemic Anaplastic Large-Cell Lymphoma Treated Within the Groupe d’Étude des Lymphomes de l’Adulte Trials. J. Clin. Oncol. 2012, 30, 3939–3946. [Google Scholar] [CrossRef]
- Ellin, F.; Landström, J.; Jerkeman, M.; Relander, T. Real-world data on prognostic factors and treatment in peripheral T-cell lymphomas: A study from the Swedish Lymphoma Registry. Blood 2014, 124, 1570–1577. [Google Scholar] [CrossRef] [Green Version]
- Maurer, M.J.; Ellin, F.; Srour, L.; Jerkeman, M.; Bennani, N.N.; Connors, J.M.; Slack, G.W.; Smedby, K.E.; Ansell, S.M.; Link, B.K.; et al. International Assessment of Event-Free Survival at 24 Months and Subsequent Survival in Peripheral T-Cell Lymphoma. J. Clin. Oncol. 2017, 35, 4019–4026. [Google Scholar] [CrossRef]
- Gleeson, M.; Peckitt, C.; To, Y.M.; Edwards, L.; Oates, J.; Wotherspoon, A.; Attygalle, A.D.; Zerizer, I.; Sharma, B.; Chua, S.; et al. CHOP versus GEM-P in previously untreated patients with peripheral T-cell lymphoma (CHEMO-T): A phase 2, multicentre, randomised, open-label trial. Lancet Haematol. 2018, 5, e190–e200. [Google Scholar] [CrossRef] [Green Version]
- Sibon, D.; Nguyen, D.-P.; Schmitz, N.; Suzuki, R.; Feldman, A.L.; Gressin, R.; Lamant, L.; Weisenburger, D.D.; Rosenwald, A.; Nakamura, S.; et al. ALK−positive anaplastic large-cell lymphoma in adults: An individual patient data pooled analysis of 263 patients. Haematologica 2019, 104, e562–e565. [Google Scholar] [CrossRef] [PubMed]
- Bachy, E.; Camus, V.; Thieblemont, C.; Sibon, D.; Casasnovas, R.-O.; Ysebaert, L.; Damaj, G.; Guidez, S.; Pica, G.M.; Kim, W.S.; et al. Romidepsin Plus CHOP Versus CHOP in Patients With Previously Untreated Peripheral T-Cell Lymphoma: Results of the Ro-CHOP Phase III Study (Conducted by LYSA). J. Clin. Oncol. 2022, 40, 242–251. [Google Scholar] [CrossRef] [PubMed]
- d’Amore, F.; Relander, T.; Lauritzsen, G.F.; Jantunen, E.; Hagberg, H.; Anderson, H.; Holte, H.; Österborg, A.; Merup, M.; Brown, P.; et al. Up-Front Autologous Stem-Cell Transplantation in Peripheral T-Cell Lymphoma: NLG-T-01. J. Clin. Oncol. 2012, 30, 3093–3099. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.A.; Byun, J.M.; Park, K.; Ae, K.Y.; Lee, D.; Kim, D.S.; Yoon, S.-S.; Koh, Y. Redefining the role of etoposide in first-line treatment of peripheral T-cell lymphoma. Blood Adv. 2017, 1, 2138–2146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janikova, A.; Chloupkova, R.; Campr, V.; Klener, P.; Hamouzova, J.; Belada, D.; Prochazka, V.; Pytlik, R.; Pirnos, J.; Duras, J.; et al. First-line therapy for T cell lymphomas: A retrospective population-based analysis of 906 T cell lymphoma patients. Ann. Hematol 2019, 98, 1961–1972. [Google Scholar] [CrossRef]
- Schmitz, N.; Truemper, L.; Bouabdallah, K.; Ziepert, M.; Leclerc, M.; Cartron, G.; Jaccard, A.; Reimer, P.; Wagner, E.; Wilhelm, M.; et al. A randomized phase 3 trial of autologous vs. allogeneic transplantation as part of first-line therapy in poor-risk peripheral T-NHL. Blood 2021, 137, 2646–2656. [Google Scholar] [CrossRef]
- Shustov, A.; Cabrera, M.E.; Civallero, M.; Bellei, M.; Ko, Y.H.; Manni, M.; Skrypets, T.; Horwitz, S.M.; De Souza, C.A.; Radford, J.A.; et al. ALK−negative anaplastic large cell lymphoma: Features and outcomes of 235 patients from the International T-Cell Project. Blood Adv. 2021, 5, 640–648. [Google Scholar] [CrossRef]
- Cederleuf, H.; Bjerregård Pedersen, M.; Jerkeman, M.; Relander, T.; d’Amore, F.; Ellin, F. The addition of etoposide to CHOP is associated with improved outcome in ALK+ adult anaplastic large cell lymphoma: A Nordic Lymphoma Group study. Br. J. Haematol. 2017, 178, 739–746. [Google Scholar] [CrossRef] [Green Version]
- Dunleavy, K.; Pittaluga, S.; Shovlin, M.; Roschewski, M.; Lai, C.; Steinberg, S.M.; Jaffe, E.S.; Wilson, W.H. Phase II trial of dose-adjusted EPOCH in untreated systemic anaplastic large cell lymphoma. Haematologica 2015, 101, e27–e29. [Google Scholar] [CrossRef] [Green Version]
- Maeda, Y.; Nishimori, H.; Yoshida, I.; Hiramatsu, Y.; Uno, M.; Masaki, Y.; Sunami, K.; Masunari, T.; Nawa, Y.; Yamane, H.; et al. Dose-adjusted EPOCH chemotherapy for untreated peripheral T-cell lymphomas: A multicenter phase II trial of West-JHOG PTCL0707. Haematologica 2017, 102, 2097–2103. [Google Scholar] [CrossRef] [Green Version]
- Nickelsen, M.; Ziepert, M.; Zeynalova, S.; Glass, B.; Metzner, B.; Leithaeuser, M.; Mueller-Hermelink, H.K.; Pfreundschuh, M.; Schmitz, N. High-dose CHOP plus etoposide (MegaCHOEP) in T-cell lymphoma: A comparative analysis of patients treated within trials of the German High-Grade Non-Hodgkin Lymphoma Study Group (DSHNHL). Ann. Oncol. 2009, 20, 1977–1984. [Google Scholar] [CrossRef] [PubMed]
- Hapgood, G.; Stone, J.M.; Zannino, D.; George, A.; Marlton, P.; Prince, H.M.; Hui, C.-H.; Prosser, I.; Lewis, I.D.; Bradstock, K.; et al. A phase II study of a modified hyper-CVAD frontline therapy for patients with adverse risk diffuse large B-cell and peripheral T-cell non-Hodgkin lymphoma. Leuk. Lymphoma 2018, 60, 904–911. [Google Scholar] [CrossRef] [PubMed]
- Escalón, M.P.; Liu, N.S.; Yang, Y.; Hess, M.; Walker, P.L.; Smith, T.L.; Nam, H.; Dang, M.D. Prognostic factors and treatment of patients with T-cell non-Hodgkin lymphoma: The, M.D. Anderson Cancer Center experience. Cancer 2005, 103, 2091–2098. [Google Scholar] [CrossRef] [PubMed]
- Gallamini, A.; Zaja, F.; Patti, C.; Billio, A.; Specchia, M.R.; Tucci, A.; Levis, A.; Manna, A.; Secondo, V.; Rigacci, L.; et al. Alemtuzumab (Campath-1H) and CHOP chemotherapy as first-line treatment of peripheral T-cell lymphoma: Results of a GITIL (Gruppo Italiano Terapie Innovative nei Linfomi) prospective multicenter trial. Blood 2007, 110, 2316–2323. [Google Scholar] [CrossRef] [Green Version]
- Roswarski, J.; Roschewski, M.; Melani, C.; Pittaluga, S.; Lucas, A.; Steinberg, S.M.; Waldmann, T.A.; Wilson, W.H. Phase 1/2 study of alemtuzumab with dose-adjusted EPOCH in untreated aggressive T and NK cell lymphomas. Leuk. Lymphoma. 2019, 60, 2062–2066. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Yoon, D.H.; Kang, H.J.; Kim, J.S.; Park, S.K.; Kim, H.J.; Lee, J.; Ryoo, B.-Y.; Ko, Y.H.; Huh, J.; et al. Bortezomib in combination with CHOP as first-line treatment for patients with stage III/IV peripheral T-cell lymphomas: A multicentre, single-arm, phase 2 trial. Eur. J. Cancer 2012, 48, 3223–3231. [Google Scholar] [CrossRef]
- Foss, F.M.; Sjak-Shie, N.; Goy, A.; Jacobsen, E.; Advani, R.; Smith, M.; Komrokji, R.; Pendergrass, K.; Bolejack, V. A multicenter phase II trial to determine the safety and efficacy of combination therapy with denileukin diftitox and cyclophosphamide, doxorubicin, vincristine and prednisone in untreated peripheral T-cell lymphoma: The CONCEPT study. Leuk. Lymphoma 2013, 54, 1373–1379. [Google Scholar] [CrossRef]
- Oki, Y.; Younes, A.; Copeland, A.; Hagemeister, F.; Fayad, L.E.; McLaughlin, P.; Shah, J.; Fowler, N.; Romaguera, J.; Kwak, L.; et al. Phase I study of vorinostat in combination with standard CHOP in patients with newly diagnosed peripheral T-cell lymphoma. Br. J. Haematol. 2013, 162, 138–141. [Google Scholar] [CrossRef]
- Dupuis, J.; Morschhauser, F.; Ghesquières, H.; Tilly, H.; Casasnovas, O.; Thieblemont, C.; Ribrag, V.; Bossard, C.; LeBras, F.; Bachy, E.; et al. Combination of romidepsin with cyclophosphamide, doxorubicin, vincristine, and prednisone in previously untreated patients with peripheral T-cell lymphoma: A non-randomised, phase 1b/2 study. Lancet Haematol. 2015, 2, e160–e165. [Google Scholar] [CrossRef]
- Kim, S.J.; Shin, D.-Y.; Kim, J.S.; Yoon, D.H.; Lee, W.S.; Lee, H.; Do, Y.R.; Kang, H.J.; Eom, H.S.; Ko, Y.H.; et al. A phase II study of everolimus (RAD001), an mTOR inhibitor plus CHOP for newly diagnosed peripheral T-cell lymphomas. Ann. Oncol. 2016, 27, 712–718. [Google Scholar] [CrossRef]
- Advani, R.H.; Ansell, S.M.; Lechowicz, M.J.; Beaven, A.W.; Loberiza, F.; Carson, K.R.; Evens, A.; Foss, F.; Horwitz, S.; Pro, B.; et al. A phase II study of cyclophosphamide, etoposide, vincristine and prednisone (CEOP) Alternating with Pralatrexate (P) as front line therapy for patients with peripheral T-cell lymphoma (PTCL): Final results from the T- cell consortium trial. Br. J. Haematol. 2015, 172, 535–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanale, M.A.; Horwitz, S.M.; Forero-Torres, A.; Bartlett, N.L.; Advani, R.; Pro, B.; Chen, R.W.; Davies, A.; Illidge, T.; Uttarwar, M.; et al. Five-year outcomes for frontline brentuximab vedotin with CHP for CD30-expressing peripheral T-cell lymphomas. Blood 2018, 131, 2120–2124. [Google Scholar] [CrossRef] [PubMed]
- Johnston, P.B.; Cashen, A.F.; Nikolinakos, P.G.; Beaven, A.W.; Barta, S.K.; Bhat, G.; Hasal, S.J.; De Vos, S.; Oki, Y.; Deng, C.; et al. Belinostat in combination with standard cyclophosphamide, doxorubicin, vincristine and prednisone as first-line treatment for patients with newly diagnosed peripheral T-cell lymphoma. Exp. Hematol. Oncol. 2021, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- Herrera, A.F.; Zain, J.; Savage, K.J.; Feldman, T.A.; Brammer, J.E.; Chen, L.; Popplewell, L.L.; Budde, L.E.; Mei, M.; Leslie, L.A.; et al. Brentuximab Vedotin Plus Cyclophosphamide, Doxorubicin, Etoposide, and Prednisone (CHEP-BV) Followed By BV Consolidation in Patients with CD30-Expressing Peripheral T-Cell Lymphomas. Blood 2021, 128, 133. [Google Scholar] [CrossRef]
- Simon, A.; Peoch, M.; Casassus, P.; Deconinck, E.; Colombat, P.; Desablens, B.; Tournilhac, O.; Eghbali, H.; Foussard, C.; Jaubert, J.; et al. Upfront VIP-reinforced-ABVD (VIP-rABVD) is not superior to CHOP/21 in newly diagnosed peripheral T cell lymphoma. Results of the randomized phase III trial GOELAMS-LTP95. Br. J. Haematol. 2010, 151, 159–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horwitz, S.; O’Connor, O.A.; Pro, B.; Illidge, T.; Fanale, M.; Advani, R.; Bartlett, N.; Christensen, J.H.; Morschhauser, F.; Domenech, E.D.; et al. Brentuximab vedotin with chemotherapy for CD30-positive peripheral T-cell lymphoma (ECHELON-2): A global, double-blind, randomised, phase 3 trial. Lancet 2018, 393, 229–240. [Google Scholar] [CrossRef] [Green Version]
- Horwitz, S.; O’Connor, O.A.; Pro, B.; Trümper, L.; Iyer, S.; Advani, R.; Bartlett, N.L.; Christensen, J.H.; Morschhauser, F.; Domingo-Domenech, E.; et al. The ECHELON-2 Trial: 5-year results of a randomized, phase III study of brentuximab vedotin with chemotherapy for CD30-positive peripheral T-cell lymphoma. Ann. Oncol. 2022, 33, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Wulf, G.G.; Altmann, B.; Ziepert, M.; D’Amore, F.; Held, G.; Greil, R.; Tournilhac, O.; Relander, T.; Viardot, A.; Wilhelm, M.; et al. Alemtuzumab plus CHOP versus CHOP in elderly patients with peripheral T-cell lymphoma: The DSHNHL2006-1B/ACT-2 trial. Leukemia 2021, 35, 143–155. [Google Scholar] [CrossRef]
- Parrilla Castellar, E.R.; Jaffe, E.S.; Said, J.W.; Swerdlow, S.H.; Ketterling, R.P.; Knudson, R.A.; Sidhu, J.S.; Hsi, E.D.; Karikehalli, S.; Jiang, L.; et al. ALK−negative anaplastic large cell lymphoma is a genetically heterogeneous disease with widely disparate clinical outcomes. Blood 2014, 124, 1473–1480. [Google Scholar] [CrossRef] [Green Version]
- Hapgood, G.; Ben-Neriah, S.; Mottok, A.; Lee, D.G.; Villa, D.; Sehn, L.H.; Connors, J.M.; Gascoyne, R.D.; Feldman, A.L.; Farinha, P.; et al. Identification of high-risk DUSP22-rearranged ALK−negative anaplastic large cell lymphoma. Br. J. Haematol. 2019, 186, e28–e31. [Google Scholar] [CrossRef] [Green Version]
- Sibon, D.; Bisig, B.; Bonnet, C.; Bachy, E.; Cavalieri, D.; Fataccioli, V.; Drieux, F.; Bruneau, J.; Lemonnier, F.; Bossard, C.; et al. Impact of dusp22 rearrangement on the prognosis of systemic alk-negative anaplastic large cell lymphoma: A lysa and tenomic study. Hematol. Oncol. 2021, 39. [Google Scholar] [CrossRef]
- Illidge, T.; Horwitz, S.; Iyer, S.; Bartlett, N.L. Response to brentuximab vedotin plus CHP according to CD30 expression in the ECHELON-2 trial. Br. J. Haematol. 2020, 189, 111–112. [Google Scholar]
- Corradini, P.; Tarella, C.; Zallio, F.; Dodero, A.; Zanni, M.; Valagussa, P.; Gianni, A.M.; Rambaldi, A.; Barbui, T.; Cortelazzo, S. Long-term follow-up of patients with peripheral T-cell lymphomas treated up-front with high-dose chemotherapy followed by autologous stem cell transplantation. Leukemia 2006, 20, 1533–1538. [Google Scholar] [CrossRef]
- Rodríguez, J.; Conde, E.; Gutiérrez, A.; Arranz, R.; León, Á.; Marín, J.; Bendandi, M.; Albo, C.; Caballero, M.D.; Grupo Español de Linfomas/Trasplante Autólogo de Médula Ósea. Frontline autologous stem cell transplantation in high-risk peripheral T-cell lymphoma: A prospective study from The Gel-Tamo Study Group. Eur. J. Haematol. 2007, 79, 32–38. [Google Scholar] [CrossRef]
- Mercadal, S.; Briones, J.; Xicoy, B.; Pedro, C.; Escoda, L.; Estany, C.; Camos, M.; Colomo, L.; Espinosa, Í.; Martinez, S.; et al. Intensive chemotherapy (high-dose CHOP/ESHAP regimen) followed by autologous stem-cell transplantation in previously untreated patients with peripheral T-cell lymphoma. Ann. Oncol. 2008, 19, 958–963. [Google Scholar] [CrossRef] [PubMed]
- Reimer, P.; Rüdiger, T.; Geissinger, E.; Weissinger, F.; Nerl, C.; Schmitz, N.; Engert, A.; Einsele, H.; Müller-Hermelink, H.K.; Wilhelm, M. Autologous Stem-Cell Transplantation As First-Line Therapy in Peripheral T-Cell Lymphomas: Results of a Prospective Multicenter Study. J. Clin. Oncol. 2009, 27, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Wilhelm, M.; Smetak, M.; Reimer, P.; Geissinger, E.; Ruediger, T.; Metzner, B.; Schmitz, N.; Engert, A.; Schaefer-Eckart, K.; Birkmann, J. First-line therapy of peripheral T-cell lymphoma: Extension and long-term follow-up of a study investigating the role of autologous stem cell transplantation. Blood Cancer J. 2016, 6, e452. [Google Scholar] [CrossRef]
- d’Amore, F.; Gaulard, P.; Trümper, L.; Corradini, P.; Kim, W.-S.; Specht, L.; Pedersen, M.B.; Ladetto, M. Peripheral T-cell lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, v108–v115. [Google Scholar] [CrossRef] [Green Version]
- Park, S.I.; Horwitz, S.M.; Foss, F.M.; Pinter-Brown, L.C.; Carson, K.R.; Rosen, S.T.; Pro, B.; Hsi, E.D.; Federico, M.; Gisselbrecht, C.; et al. The role of autologous stem cell transplantation in patients with nodal peripheral T-cell lymphomas in first complete remission: Report from COMPLETE, a prospective, multicenter cohort study. Cancer 2019, 125, 1507–1517. [Google Scholar] [CrossRef]
- Fossard, G.; Broussais, F.; Coelho, I.; Bailly, S.; Nicolas-Virelizier, E.; Toussaint, E.; Lancesseur, C.; Le Bras, F.; Willems, E.; Tchernonog, E.; et al. Role of up-front autologous stem-cell transplantation in peripheral T-cell lymphoma for patients in response after induction: An analysis of patients from LYSA centers. Ann. Oncol. 2018, 29, 715–723. [Google Scholar] [CrossRef]
- Corradini, P.; Vitolo, U.; Rambaldi, A.; Miceli, R.; Patriarca, F.; Gallamini, A.; Olivieri, A.; Benedetti, F.; Todeschini, G.; Rossi, G.; et al. Intensified chemo-immunotherapy with or without stem cell transplantation in newly diagnosed patients with peripheral T-cell lymphoma. Leukemia 2014, 28, 1885–1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamez, A.-C.; Dupont, A.; Blaise, D.; Chevallier, P.; Forcade, E.; Ceballos, P.; Mohty, M.; Suarez, F.; Beguin, Y.; De Latour, R.P.; et al. Allogeneic stem cell transplantation for peripheral T cell lymphomas: A retrospective study in 285 patients from the Société Francophone de Greffe de Moelle et de Thérapie Cellulaire (SFGM-TC). J. Hematol. Oncol. 2020, 13, 56. [Google Scholar] [CrossRef] [PubMed]
- Mourad, N.; Mounier, N.; Brière, J.; Raffoux, E.; Delmer, A.; Feller, A.; Meijer, C.J.L.M.; Emile, J.-F.; Bouabdallah, R.; Bosly, A.; et al. Clinical, biologic, and pathologic features in 157 patients with angioimmunoblastic T-cell lymphoma treated within the Groupe d’Etude des Lymphomes de l’Adulte (GELA) trials. Blood 2008, 111, 4463–4470. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, T.; Shimada, K.; Yamamoto, K.; Chihara, D.; Ichihashi, T.; Oshima, R.; Tanimoto, M.; Iwasaki, T.; Isoda, A.; Sakai, A.; et al. Retrospective analysis of prognostic factors for angioimmunoblastic T-cell lymphoma: A multicenter cooperative study in Japan. Blood 2012, 119, 2837–2843. [Google Scholar] [CrossRef] [PubMed]
- Delfau-Larue, M.-H.; De Leval, L.; Joly, B.; Plonquet, A.; Challine, D.; Parrens, M.; Delmer, A.; Salles, G.; Morschhauser, F.; Delarue, R.; et al. Targeting intratumoral B cells with rituximab in addition to CHOP in angioimmunoblastic T-cell lymphoma. A clinicobiological study of the GELA. Haematologica 2012, 97, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Federico, M.; Rudiger, T.; Bellei, M.; Nathwani, B.N.; Luminari, S.; Coiffier, B.; Harris, N.L.; Jaffe, E.; Pileri, S.A.; Savage, K.J.; et al. Clinicopathologic Characteristics of Angioimmunoblastic T-Cell Lymphoma: Analysis of the International Peripheral T-Cell Lymphoma Project. J. Clin. Oncol. 2013, 31, 240–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemonnier, F.; Safar, V.; Beldi-Ferchiou, A.; Cottereau, A.-S.; Bachy, E.; Cartron, G.; Fataccioli, V.; Pelletier, L.; Robe, C.; Letourneau, A.; et al. Integrative analysis of a phase 2 trial combining lenalidomide with CHOP in angioimmunoblastic T-cell lymphoma. Blood Adv. 2021, 5, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Advani, R.; Skrypets, T.; Civallero, M.; Spinner, M.A.; Manni, M.; Kim, W.; Shustov, A.; Horwitz, S.M.; Hitz, F.; Cabrera, M.E.; et al. Outcomes and Prognostic Factors in Angioimmunoblastic T cell Lymphoma: Final Report from the International TCell Project. Blood 2021, 138, 213–220. [Google Scholar] [CrossRef]
- Gallamini, A.; Stelitano, C.; Calvi, R.; Bellei, M.; Mattei, D.; Vitolo, U.; Morabito, F.; Martelli, M.; Brusamolino, E.; Iannitto, E.; et al. Peripheral T-cell lymphoma unspecified (PTCL-U): A new prognostic model from a retrospective multicentric clinical study. Blood 2004, 103, 2474–2479. [Google Scholar] [CrossRef] [Green Version]
- Weisenburger, D.D.; Savage, K.J.; Harris, N.L.; Gascoyne, R.D.; Jaffe, E.; MacLennan, K.A.; Rüdiger, T.; Pileri, S.; Nakamura, S.; Nathwani, B.; et al. Peripheral T-cell lymphoma, not otherwise specified: A report of 340 cases from the International Peripheral T-cell Lymphoma Project. Blood 2011, 117, 3402–3408. [Google Scholar] [CrossRef] [Green Version]
- Federico, M.; Bellei, M.; Marcheselli, L.; Schwartz, M.; Manni, M.; Tarantino, V.; Pileri, S.; Ko, Y.-H.; Cabrera, M.E.; Horwitz, S.; et al. Peripheral T cell lymphoma, not otherwise specified (PTCL-NOS). A new prognostic model developed by the International T cell Project Network. Br. J. Haematol. 2018, 181, 760–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellei, M.; Foss, F.M.; Shustov, A.R.; Horwitz, S.M.; Marcheselli, L.; Kim, W.S.; Cabrera, M.E.; Dlouhy, I.; Nagler, A.; Advani, R.H.; et al. The outcome of peripheral T-cell lymphoma patients failing first-line therapy: A report from the prospective, International T-Cell Project. Haematologica 2018, 103, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Mak, V.; Hamm, J.; Chhanabhai, M.; Shenkier, T.; Klasa, R.; Sehn, L.H.; Villa, D.; Gascoyne, R.D.; Connors, J.M.; Savage, K.J. Survival of Patients With Peripheral T-Cell Lymphoma After First Relapse or Progression: Spectrum of Disease and Rare Long-Term Survivors. J. Clin. Oncol. 2013, 31, 1970–1976. [Google Scholar] [CrossRef] [PubMed]
- Ellin, F.; Landström, J.; Jerkeman, M.; Relander, T. Central nervous system relapse in peripheral T-cell lymphomas: A Swedish Lymphoma Registry study. Blood 2015, 126, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horwitz, S.M.; Ansell, S.; Ai, W.Z.; Barnes, J.; Barta, S.K.; Clemens, M.W.; Dogan, A.; Goodman, A.M.; Goyal, G.; Guitart, J.; et al. NCCN Guidelines Insights: T-Cell Lymphomas, Version 1.2021: Featured Updates to the NCCN Guidelines. J. Natl. Compr. Canc. Netw. 2020, 18, 1460–1467. [Google Scholar] [CrossRef] [PubMed]
- Damaj, G.; Gressin, R.; Bouabdallah, K.; Cartron, G.; Choufi, B.; Gyan, E.; Banos, A.; Jaccard, A.; Park, S.; Tournilhac, O.; et al. Results From a Prospective, Open-Label, Phase II Trial of Bendamustine in Refractory or Relapsed T-Cell Lymphomas: The BENTLY Trial. J. Clin. Oncol. 2013, 31, 104–110. [Google Scholar] [CrossRef]
- Reboursiere, E.; Le Bras, F.; Herbaux, C.; Gyan, E.; Clavert, A.; Morschhauser, F.; Malak, S.; Sibon, D.; Broussais, F.; Braun, T.; et al. Bendamustine for the treatment of relapsed or refractory peripheral T cell lymphomas: A French retrospective multicenter study. Oncotarget 2016, 7, 85573–85583. [Google Scholar] [CrossRef] [Green Version]
- Zinzani, P.L.; Venturini, F.; Stefoni, V.; Fina, M.; Pellegrini, C.; Derenzini, E.; Gandolfi, L.; Broccoli, A.; Argnani, L.; Quirini, F.; et al. Gemcitabine as single agent in pretreated T-cell lymphoma patients: Evaluation of the long-term outcome. Ann. Oncol. 2009, 21, 860–863. [Google Scholar] [CrossRef]
- Morel, A.; Brière, J.; Lamant, L.; Loschi, M.; Haioun, C.; Delarue, R.; Tournilhac, O.; Bachy, E.; Sonet, A.; Amorim, S.; et al. Long-term outcomes of adults with first-relapsed/refractory systemic anaplastic large-cell lymphoma in the pre-brentuximab vedotin era: A LYSA/SFGM-TC study. Eur. J. Cancer 2017, 83, 146–153. [Google Scholar] [CrossRef]
- Pro, B.; Advani, R.; Brice, P.; Bartlett, N.L.; Rosenblatt, J.D.; Illidge, T.; Matous, J.; Ramchandren, R.; Fanale, M.; Connors, J.M.; et al. Five-year results of brentuximab vedotin in patients with relapsed or refractory systemic anaplastic large cell lymphoma. Blood 2017, 130, 2709–2717. [Google Scholar] [CrossRef] [Green Version]
- Halligan, S.J.; Grainge, M.J.; Martinez-Calle, N.; Fox, C.P.; Bishton, M.J. Population-based cohort study of the efficacy of brentuximab vedotin in relapsed systemic anaplastic large-cell lymphoma using Public Health England data. Br. J. Haematol. 2021, 196, 932–938. [Google Scholar] [CrossRef] [PubMed]
- Brugières, L.; Houot, R.; Cozic, N.; De La Fouchardière, C.; Morschhauser, F.; Brice, P.; Arakelyan Laboure, N.; Auvrignon, A.; Aladjidi, N.; Kolb, B.; et al. Crizotinib in Advanced ALK+ Anaplastic Large Cell Lymphoma in Children and Adults: Results of the Acs© Phase II Trial. Blood 2017, 130, 2831. [Google Scholar] [CrossRef]
- Mossé, Y.P.; Voss, S.D.; Lim, M.; Rolland, D.; Minard, C.G.; Fox, E.; Adamson, P.; Wilner, K.; Blaney, S.M.; Weigel, B.J. Targeting ALK With Crizotinib in Pediatric Anaplastic Large Cell Lymphoma and Inflammatory Myofibroblastic Tumor: A Children’s Oncology Group Study. J. Clin. Oncol. 2017, 35, 3215–3221. [Google Scholar] [CrossRef] [PubMed]
- Gambacorti-Passerini, C.; Orlov, S.; Zhang, L.; Braiteh, F.; Huang, H.; Esaki, T.; Horibe, K.; Ahn, J.-S.; Beck, J.T.; Edenfield, W.J.; et al. Long-term effects of crizotinib in ALK−positive tumors (excluding NSCLC): A phase 1b open-label study. Am. J. Hematol. 2018, 93, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Bossi, E.; Aroldi, A.; Brioschi, F.A.; Steidl, C.; Baretta, S.; Renso, R.; Verga, L.; Fontana, D.; Sharma, G.G.; Mologni, L.; et al. Phase two study of crizotinib in patients with anaplastic lymphoma kinase ( ALK )-positive anaplastic large cell lymphoma relapsed/refractory to chemotherapy. Am. J. Hematol. 2020, 95, E319–E321. [Google Scholar] [CrossRef] [PubMed]
- Fukano, R.; Mori, T.; Sekimizu, M.; Choi, I.; Kada, A.; Saito, A.M.; Asada, R.; Takeuchi, K.; Terauchi, T.; Tateishi, U.; et al. Alectinib for relapsed or refractory anaplastic lymphoma kinase-positive anaplastic large cell lymphoma: An open-label phase II trial. Cancer Sci. 2020, 111, 4540–4547. [Google Scholar] [CrossRef]
- Fischer, M.; Moreno, L.; Ziegler, D.S.; Marshall, L.V.; Zwaan, C.M.; Irwin, M.S.; Casanova, M.; Sabado, C.; Wulff, B.; Stegert, M.; et al. Ceritinib in paediatric patients with anaplastic lymphoma kinase-positive malignancies: An open-label, multicentre, phase 1, dose-escalation and dose-expansion study. Lancet Oncol. 2021, 22, 1764–1776. [Google Scholar] [CrossRef]
- Knörr, F.; Brugières, L.; Pillon, M.; Zimmermann, M.; Ruf, S.; Attarbaschi, A.; Mellgren, K.; Burke, G.A.A.; Uyttebroeck, A.; Wróbel, G.; et al. Stem Cell Transplantation and Vinblastine Monotherapy for Relapsed Pediatric Anaplastic Large Cell Lymphoma: Results of the International, Prospective ALCL-Relapse Trial. J. Clin. Oncol. 2020, 38, 3999–4009. [Google Scholar] [CrossRef]
- Rodríguez, J.; Caballero, M.D.; Gutiérrez, A.; Marín, J.; Lahuerta, J.J.; Sureda, A.; Carreras, E.; León, A.; Arranz, R.; de Sevilla, A.F.; et al. High-dose chemotherapy and autologous stem cell transplantation in peripheral T-cell lymphoma: The GEL-TAMO experience. Ann. Oncol. 2003, 14, 1768–1775. [Google Scholar] [CrossRef]
- Nademanee, A.; Palmer, J.M.; Popplewell, L.; Tsai, N.-C.; Delioukina, M.; Gaal, K.; Cai, J.-L.; Kogut, N.; Forman, S.J. High-Dose Therapy and Autologous Hematopoietic Cell Transplantation in Peripheral T Cell Lymphoma (PTCL): Analysis of Prognostic Factors. Biol. Blood Marrow Transplant. 2011, 17, 1481–1489. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Burns, L.J.; Van Besien, K.; LeRademacher, J.; He, W.; Fenske, T.S.; Suzuki, R.; Hsu, J.W.; Schouten, H.C.; Hale, G.A.; et al. Hematopoietic Cell Transplantation for Systemic Mature T-Cell Non-Hodgkin Lymphoma. J. Clin. Oncol. 2013, 31, 3100–3109. [Google Scholar] [CrossRef] [PubMed]
- El-Asmar, J.; Reljic, T.; Ayala, E.; Hamadani, M.; Nishihori, T.; Kumar, A.; Kharfan-Dabaja, M.A. Efficacy of High-Dose Therapy and Autologous Hematopoietic Cell Transplantation in Peripheral T Cell Lymphomas as Front-Line Consolidation or in the Relapsed/Refractory Setting: A Systematic Review/Meta-Analysis. Biol. Blood Marrow Transplant. 2015, 22, 802–814. [Google Scholar] [CrossRef] [PubMed]
- Corradini, P.; Dodero, A.; Zallio, F.; Caracciolo, D.; Casini, M.; Bregni, M.; Narni, F.; Patriarca, F.; Boccadoro, M.; Benedetti, F.; et al. Graft-Versus-Lymphoma Effect in Relapsed Peripheral T-Cell Non-Hodgkin’s Lymphomas After Reduced-Intensity Conditioning Followed by Allogeneic Transplantation of Hematopoietic Cells. J. Clin. Oncol. 2004, 22, 2172–2176. [Google Scholar] [CrossRef] [PubMed]
- Le Gouill, S.; Milpied, N.; Buzyn, A.; Peffault De Latour, R.; Vernant, J.-P.; Mohty, M.; Moles, M.-P.; Bouabdallah, K.; Bulabois, C.-E.; Dupuis, J.; et al. Graft-Versus-Lymphoma Effect for Aggressive T-Cell Lymphomas in Adults: A Study by the Société Française de Greffe de Moëlle et de Thérapie Cellulaire. J. Clin. Oncol. 2008, 26, 2264–2271. [Google Scholar] [CrossRef] [PubMed]
- Dodero, A.; Spina, F.; Narni, F.; Patriarca, F.; Cavattoni, I.; Benedetti, F.; Ciceri, F.; Baronciani, D.; Scimè, R.; Pogliani, E.; et al. Allogeneic transplantation following a reduced-intensity conditioning regimen in relapsed/refractory peripheral T-cell lymphomas: Long-term remissions and response to donor lymphocyte infusions support the role of a graft-versus-lymphoma effect. Leukemia 2011, 26, 520–526. [Google Scholar] [CrossRef] [Green Version]
- Epperla, N.; Ahn, K.W.; Litovich, C.; Ahmed, S.; Battiwalla, M.; Cohen, J.B.; Dahi, P.; Farhadfar, N.; Farooq, U.; Freytes, C.O.; et al. Allogeneic hematopoietic cell transplantation provides effective salvage despite refractory disease or failed prior autologous transplant in angioimmunoblastic T-cell lymphoma: A CIBMTR analysis. J. Hematol. Oncol. 2019, 12, 6. [Google Scholar] [CrossRef]
- Du, J.; Yu, D.; Han, X.; Zhu, L.; Huang, Z. Comparison of Allogeneic Stem Cell Transplant and Autologous Stem Cell Transplant in Refractory or Relapsed Peripheral T-Cell Lymphoma: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e219807. [Google Scholar] [CrossRef]
- Coiffier, B.; Pro, B.; Prince, H.M.; Foss, F.; Sokol, L.; Greenwood, M.; Caballero, D.; Borchmann, P.; Morschhauser, F.; Wilhelm, M.; et al. Results From a Pivotal, Open-Label, Phase II Study of Romidepsin in Relapsed or Refractory Peripheral T-Cell Lymphoma After Prior Systemic Therapy. J. Clin. Oncol. 2012, 30, 631–636. [Google Scholar] [CrossRef]
- O’Connor, O.A.; Horwitz, S.; Masszi, T.; Van Hoof, A.; Brown, P.D.N.; Doorduijn, J.; Hess, G.; Jurczak, W.; Knoblauch, P.; Chawla, S.; et al. Belinostat in Patients With Relapsed or Refractory Peripheral T-Cell Lymphoma: Results of the Pivotal Phase II BELIEF (CLN-19) Study. J. Clin. Oncol. 2015, 33, 2492–2499. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Dong, M.; Hong, X.; Zhang, W.; Feng, J.; Zhu, J.; Yu, L.; Ke, X.; Huang, H.; Shen, Z.; et al. Results from a multicenter, open-label, pivotal phase II study of chidamide in relapsed or refractory peripheral T-cell lymphoma. Ann. Oncol. 2015, 26, 1766–1771. [Google Scholar] [CrossRef]
- Barr, P.M.; Li, H.; Spier, C.; Mahadevan, D.; Leblanc, M.; Haq, M.U.; Huber, B.D.; Flowers, C.R.; Wagner-Johnston, N.D.; Horwitz, S.M.; et al. Phase II Intergroup Trial of Alisertib in Relapsed and Refractory Peripheral T-Cell Lymphoma and Transformed Mycosis Fungoides: SWOG 1108. J. Clin. Oncol. 2015, 33, 2399–2404. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, O.A.; Özcan, M.; Jacobsen, E.D.; Roncero, J.M.; Trotman, J.; Demeter, J.; Masszi, T.; Pereira, J.; Ramchandren, R.; Beaven, A.; et al. Randomized Phase III Study of Alisertib or Investigator’s Choice (Selected Single Agent) in Patients With Relapsed or Refractory Peripheral T-Cell Lymphoma. J. Clin. Oncol. 2019, 37, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Dreyling, M.; Morschhauser, F.; Bouabdallah, K.; Bron, D.; Cunningham, D.; Assouline, S.E.; Verhoef, G.; Linton, K.; Thieblemont, C.; Vitolo, U.; et al. Phase II study of copanlisib, a PI3K inhibitor, in relapsed or refractory, indolent or aggressive lymphoma. Ann. Oncol. 2017, 28, 2169–2178. [Google Scholar] [CrossRef] [PubMed]
- Horwitz, S.M.; Koch, R.; Porcu, P.; Oki, Y.; Moskowitz, A.; Perez, M.; Myskowski, P.; Officer, A.; Jaffe, J.D.; Morrow, S.N.; et al. Activity of the PI3K-δ,γ inhibitor duvelisib in a phase 1 trial and preclinical models of T-cell lymphoma. Blood 2018, 131, 888–898. [Google Scholar] [CrossRef] [PubMed]
- Huen, A.; Haverkos, B.M.; Zain, J.; Radhakrishnan, R.; Lechowicz, M.J.; Devata, S.; Korman, N.J.; Pinter-Brown, L.; Oki, Y.; Barde, P.J.; et al. Phase I/Ib Study of Tenalisib (RP6530), a Dual PI3K δ/γ Inhibitor in Patients with Relapsed/Refractory T-Cell Lymphoma. Cancers 2020, 12, 2293. [Google Scholar] [CrossRef]
- Kumar, A.; Vardhana, S.; Moskowitz, A.J.; Porcu, P.; Dogan, A.; Dubovsky, J.A.; Matasar, M.J.; Zhang, Z.; Younes, A.; Horwitz, S.M. Pilot trial of ibrutinib in patients with relapsed or refractory T-cell lymphoma. Blood Adv. 2018, 2, 871–876. [Google Scholar] [CrossRef]
- Moskowitz, A.J.; Ghione, P.; Jacobsen, E.; Ruan, J.; Schatz, J.H.; Noor, S.; Myskowski, P.; Vardhana, S.; Ganesan, N.; Hancock, H.; et al. A phase 2 biomarker-driven study of ruxolitinib demonstrates effectiveness of JAK/STAT targeting in T-cell lymphomas. Blood 2021, 138, 2828–2837. [Google Scholar] [CrossRef]
- Umakanthan, J.M.; Iqbal, J.; Batlevi, C.L.; Bouska, A.; Smith, L.M.; Shostrom, V.; Nutsch, H.; William, B.M.; Bociek, R.G.; Lunning, M.; et al. Phase I/II study of dasatinib and exploratory genomic analysis in relapsed or refractory non-Hodgkin lymphoma. Br. J. Haematol. 2018, 184, 744–752. [Google Scholar] [CrossRef]
- Morschhauser, F.; Fitoussi, O.; Haioun, C.; Thieblemont, C.; Quach, H.; Delarue, R.; Glaisner, S.; Gabarre, J.; Bosly, A.; Lister, J.; et al. A phase 2, multicentre, single-arm, open-label study to evaluate the safety and efficacy of single-agent lenalidomide (Revlimid®) in subjects with relapsed or refractory peripheral T-cell non-Hodgkin lymphoma: The EXPECT trial. Eur. J. Cancer 2013, 49, 2869–2876. [Google Scholar] [CrossRef]
- Toumishey, E.; Prasad, A.; Dueck, G.; Chua, N.; Finch, D.; Johnston, J.; Van Der Jagt, R.; Stewart, D.; White, D.; Belch, A.; et al. Final report of a phase 2 clinical trial of lenalidomide monotherapy for patients with T-cell lymphoma. Cancer 2014, 121, 716–723. [Google Scholar] [CrossRef]
- Barta, S.K.; Zain, J.; MacFarlane, A.W.; Smith, S.M.; Ruan, J.; Fung, H.C.; Tan, C.R.; Yang, Y.; Alpaugh, R.K.; Dulaimi, E.; et al. Phase II Study of the PD-1 Inhibitor Pembrolizumab for the Treatment of Relapsed or Refractory Mature T-cell Lymphoma. Clin. Lymphoma Myeloma Leuk. 2019, 19, 356–364.e3. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Wu, J.; Wang, Z.; Zhang, L.; Wang, Z.; Zhang, M.; Cen, H.; Peng, Z.; Li, Y.; Fan, L.; et al. Efficacy and safety of geptanolimab (GB226) for relapsed or refractory peripheral T cell lymphoma: An open-label phase 2 study (Gxplore-002). J. Hematol. Oncol. 2021, 14, 12. [Google Scholar] [CrossRef] [PubMed]
- Ribrag, V.; Caballero, L.; Fermé, C.; Zucca, E.; Arranz, R.; Briones, J.; Gisselbrecht, C.; Salles, G.; Gianni, A.M.; Gomez, H.; et al. Multicenter phase II study of plitidepsin in patients with relapsed/refractory non-Hodgkin’s lymphoma. Haematologica 2012, 98, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Losada, A.; Muñoz-Alonso, M.J.; García, C.; Sánchez-Murcia, P.A.; Martínez-Leal, J.F.; Dominguez, J.M.; Lillo, M.P.; Gago, F.; Galmarini, C.M. Translation Elongation Factor eEF1A2 is a Novel Anticancer Target for the Marine Natural Product Plitidepsin. Sci. Rep. 2016, 6, 35100. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, O.A.; Pro, B.; Pinter-Brown, L.; Bartlett, N.; Popplewell, L.; Coiffier, B.; Lechowicz, M.J.; Savage, K.J.; Shustov, A.R.; Gisselbrecht, C.; et al. Pralatrexate in Patients With Relapsed or Refractory Peripheral T-Cell Lymphoma: Results From the Pivotal PROPEL Study. J. Clin. Oncol. 2011, 29, 1182–1189. [Google Scholar] [CrossRef]
- Boonstra, P.S.; Polk, A.; Brown, N.; Hristov, A.C.; Bailey, N.; Kaminski, M.S.; Phillips, T.; Devata, S.; Mayer, T.; Wilcox, R.A. A single center phase II study of ixazomib in patients with relapsed or refractory cutaneous or peripheral T-cell lymphomas. Am. J. Hematol. 2017, 92, 1287–1294. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, M.; Bociek, R.G.; Fanale, M.; Iyer, S.P.; Lechowicz, M.J.; Bierman, P.J.; Armitage, J.O.; Lunning, M.; Kallam, A.; Vose, J.M. Phase 1 trial of carfilzomib in relapsed/refractory peripheral T-cell lymphoma. Ann. Hematol. 2021, 101, 335–340. [Google Scholar] [CrossRef]
- Hopfinger, G.; Nösslinger, T.; Lang, A.H.; Linkesch, W.; Melchardt, T.; Weiss, L.; Egle, A.; Greil, R. Lenalidomide in combination with vorinostat and dexamethasone for the treatment of relapsed/refractory peripheral T cell lymphoma (PTCL): Report of a phase I/II trial. Ann. Hematol. 2014, 93, 459–462. [Google Scholar] [CrossRef]
- Tan, D.; Phipps, C.; Hwang, W.Y.K.; Tan, S.-Y.; Yeap, C.H.; Chan, Y.H.; Tay, K.; Lim, S.T.; Lee, Y.S.; Kumar, S.G.; et al. Panobinostat in combination with bortezomib in patients with relapsed or refractory peripheral T-cell lymphoma: An open-label, multicentre phase 2 trial. Lancet Haematol. 2015, 2, e326–e333. [Google Scholar] [CrossRef]
- Pellegrini, C.; Dodero, A.; Chiappella, A.; Monaco, F.; Degl’Innocenti, D.; Salvi, F.; Vitolo, U.; Argnani, L.; Corradini, P.; Zinzani, P.L.; et al. A phase II study on the role of gemcitabine plus romidepsin (GEMRO regimen) in the treatment of relapsed/refractory peripheral T-cell lymphoma patients. J. Hematol. Oncol. 2016, 9, 38. [Google Scholar] [CrossRef] [Green Version]
- Holkova, B.; Yazbeck, V.; Kmieciak, M.; Bose, P.; Ma, S.; Kimball, A.; Tombes, M.B.; Shrader, E.; Wan, W.; Weir-Wiggins, C.; et al. A phase 1 study of bortezomib and romidepsin in patients with chronic lymphocytic leukemia/small lymphocytic lymphoma, indolent B-cell lymphoma, peripheral T-cell lymphoma, or cutaneous T-cell lymphoma. Leuk. Lymphoma 2017, 58, 1349–1357. [Google Scholar] [CrossRef] [PubMed]
- Amengual, J.E.; Lichtenstein, R.; Lue, J.; Sawas, A.; Deng, C.; Lichtenstein, E.; Khan, K.; Atkins, L.; Rada, A.; Kim, H.A.; et al. A phase 1 study of romidepsin and pralatrexate reveals marked activity in relapsed and refractory T-cell lymphoma. Blood 2018, 131, 397–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strati, P.; Chihara, D.; Oki, Y.; Fayad, L.E.; Fowler, N.; Nastoupil, L.; Romaguera, J.E.; Samaniego, F.; Garg, N.; Feng, L.; et al. A phase I study of romidepsin and ifosfamide, carboplatin, etoposide for the treatment of patients with relapsed or refractory peripheral T-cell lymphoma. Haematologica 2018, 103, e416–e418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, O.A.; Falchi, L.; Lue, J.K.; Marchi, E.; Kinahan, C.; Sawas, A.; Deng, C.; Montanari, F.; Amengual, J.E.; Kim, H.A.; et al. Oral 5-azacytidine and romidepsin exhibit marked activity in patients with PTCL: A multicenter phase 1 study. Blood 2019, 134, 1395–1405. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.; Martin, P.; Somasundaram, N.; Lim, C.; Tao, M.; Poon, E.; Yunon, M.J.; Toh, S.Q.; Yan, S.X.; Farid, M.; et al. Phase I study of selinexor in combination with dexamethasone, ifosfamide, carboplatin, etoposide chemotherapy in patients with relapsed or refractory peripheral T-cell or naturalkiller/T-cell lymphoma. Haematologica 2020, 106. [Google Scholar] [CrossRef]
- Yhim, H.-Y.; Kim, T.; Kim, S.; Shin, H.-J.; Koh, Y.; Kim, J.; Park, J.; Park, G.; Kim, W.; Moon, J.; et al. Combination treatment of copanlisib and gemcitabine in relapsed/refractory PTCL (COSMOS): An open-label phase I/II trial. Ann. Oncol. 2020, 32, 552–559. [Google Scholar] [CrossRef]
- Stuver, R.N.; Khan, N.; Schwartz, M.; Acosta, M.; Federico, M.; Gisselbrecht, C.; Horwitz, S.M.; Lansigan, F.; Pinter-Brown, L.C.; Pro, B.; et al. Single agents vs combination chemotherapy in relapsed and refractory peripheral T-cell lymphoma: Results from the comprehensive oncology measures for peripheral T-cell lymphoma treatment (COMPLETE) registry. Am. J. Hematol. 2019, 94, 641–649. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Study Type | PTCL Subtype | N | Main Results | Reference |
|---|---|---|---|---|
| Retrospective (Patients treated within trials of the DSHNHL) | Nodal and extranodal | 320 (subgroup analysis) |
| Schmitz N, 2010 [7] |
| Phase 2 (NLG-T-01) | Nodal and extranodal (ALK+ ALCL excluded) | 160 | CHOEP-14 x6 (etoposide omitted in pts > 60 years) followed by BEAM-autoSCT: 5-y PFS = 44%, 5-y OS = 51%. | d’Amore F, 2012 [14] |
| Retrospective (Swedish Lymphoma Registry) | Nodal and extranodal | 755 (subgroup analysis) | In pts ≤ 60 years with ALK− ALCL, AITL, PTCL NOS, EATL, and TCL-U, CHOEP improved PFS over CHOP (HR 0.49; p = 0.008) in multivariate analysis; OS not affected. | Ellin F, 2014 [9] |
| Retrospective (Korean National Health Insurance Service and National Cancer Registry) | Nodal and extranodal (ENKTCL excluded) | 1933 (subgroup analysis) | CHOEP did not improve PFS and OS over CHOP. | Kim YA, 2017 [15] |
| Retrospective (Czech Lymphoma Study Group database) | Nodal and extranodal PTCL, CTCL, T-ALL/LBL | 906 (subgroup analysis) | ALK+ ALCL excluded for the comparison of CHOEP and CHOP. CHOEP (n = 68) improved 5-y PFS (59% vs. 33%, p = 0.001) and OS (66% vs. 48%, p = 0.008) over CHOP (n = 113), in multivariate analysis. | Janikova A, 2019 [16] |
| Randomized, phase 3 (AATT; autoSCT vs. alloSCT) | Nodal and extranodal (ALK+ ALCL excluded) | 104 | CHOEP-14 x4 followed by DHAP x1 followed by autoSCT or alloSCT. No significant difference between autoSCT and alloSCT arms: 3-y EFS 38% vs. 43% and 3-y OS 70% vs. 57%, respectively. | Schmitz N, 2021 [17] |
| Prospective (International T-cell Project) | ALK− ALCL | 235 (subgroup analysis) | Treatment with etoposide (n = 31) improved 5-y OS (69% vs. 44%, p = 0.05) over treatment without etoposide (n = 168); PFS not affected. | Shustov A, 2021 [18] |
| Retrospective (Nordic Lymphoma Group) | ALK+ ALCL | 122 (subgroup analysis) | In pts 41–65 years CHOEP (n = 27) improved 5-y OS over CHOP (n = 17): 78% vs. 47% (HR = 0.38, p= 0.047). | Cederleuf H, 2017 [19] |
| Retrospective (pooled analysis of individual patient data from 6 studies) | ALK+ ALCL | 263 (subgroup analysis) | CHOEP (n = 38) improved 5-y PFS (89% vs. 57%, p = 0.002) and OS (97% vs. 69%, p = 0.001) over CHOP (n = 98). | Sibon D, 2019 [12] |
| Regimen | Phase | n | ORR/CR | Survival | Reference |
|---|---|---|---|---|---|
| Alemtuzumab-CHOP | 2 | 24 | 75%/71% | 3-y FFS: 48% 3-y OS: 53% | Gallamini A, 2007 [25] |
| Alemtuzumab-DA-EPOCH | 1–2 | 30 | 83%/57% | 2-y PFS: 32% 2-y OS: 49% | Roswarski J, 2019 [26] |
| Bortezomib-CHOP | 2 | 46 | 76%/65% | 3-y PFS: 35% 3-y OS: 47% | Kim SJ, 2012 [27] |
| Denileukin diftitox-CHOP | 2 | 49 | 65%/55% | 2-y PFS: 43% 2-y OS: 65% | Foss FM, 2013 [28] |
| Vorinostat-CHOP | 1 | 14 | 86%/86% | 2-y PFS: 79% 2-y OS: 81% | Oki Y, 2013 [29] |
| Romidepsin-CHOP | 1b-2 | 37 | 68%/51% | 2.5-y PFS: 41% 2.5-y OS: 71% | Dupuis J, 2015 [30] |
| Everolimus-CHOP | 2 | 30 | 90%/57% | 2-y PFS: 33% 2-y OS: 70% | Kim SJ, 2016 [31] |
| Pralatrexate-CEOP | 2 | 33 | 70%/52% | 2-y PFS: 39% 2-y OS: 60% | Advani RH, 2016 [32] |
| BV-CHP | 1 | 26 including 19 ALCL (3 ALK+; 16 ALK−) | 100%/92% | 5-y PFS: 52% (ALK− 38%) 5-y OS: 80% (ALK− 75%) | Fanale MA, 2018 [33] |
| Belinostat-CHOP | 1 | 23 | 86%/71% | - | Johnston PB, 2021 [34] |
| Study | Regimen Compared with CHOP | Primary Endpoint | n | ORR/CR | Survival | Reference |
|---|---|---|---|---|---|---|
| LTP-95 | VIP-rABVD | EFS | VIP-rABVD (43) CHOP (45) | 58%/44% 67%/33% | 2-y EFS: 45% (VIP-rABVD) vs. 41% (CHOP) 2-y OS: 55% (VIP-rABVD) vs. 55% (CHOP) | Simon A, 2010 [36] |
| CHEMO-T | GEM-P | CR/CRu | GEM-P (44) CHOP (43) | 68%/46% 76%/62% | 2-y PFS: 38% (GEM-P) vs. 37% (CHOP) 2-y OS: 64% (GEM-P) vs. 51% (CHOP) | Gleeson M, 2018 [11] |
| ECHELON-2 | BV-CHP | Modified PFS by independent central review | BV-CHP (226) CHOP (226) | 83%/68% 72%/56% | 3-year PFS 57% (BV-CHP) vs. 44% (CHOP) 3-year OS 77% (BV-CHP) vs. 69% (CHOP) | Horwitz S, 2019 [37] |
| ECHELON-2 (updated) | BV-CHP | Modified PFS by independent central review | BV-CHP (226) CHOP (226) | - | 5-year PFS 51% (BV-CHP) vs. 43% (CHOP) 5-year OS 70% (BV-CHP) vs. 61% (CHOP) | Horwitz S, 2022 [38] |
| ACT-2 | Alemtuzumab-CHOP | EFS | A-CHOP (58) CHOP (58) | 72%/60% 66%/43% | 3-y EFS: 27% (A-CHOP) vs. 24% (CHOP) 3-y OS: 37% (A-CHOP) vs. 56% (CHOP) | Wulf GG, 2020 [39] |
| Ro-CHOP | Romidepsin-CHOP | PFS | Ro-CHOP (211) CHOP (210) | 63%/41% 60%/37% | 2-y PFS: 43% (Ro-CHOP) vs. 36% (CHOP) 2-y OS: 64% (Ro-CHOP) vs. 63% (CHOP) | Bachy E, 2022 [13] |
| Reference | PTCL Subtype | n | Induction Regimen | ORR/CR Prior to autoSCT | Transplantation Rate | Survival | TRM |
|---|---|---|---|---|---|---|---|
| Corradini P, 2006 [44] | All subtypes including 30% ALK+ ALCL | 62 | Intensified regimen or MACOP-B | 72%/56% | 74% | 12-y EFS: 30% 12-y OS: 34% | 4.8% |
| Rodriguez J, 2007 [45] | Nodal PTCL excluding ALK+ ALCL | 26 | MegaCHOP | 73%/46% | 73% | 3-y PFS 53% 3-y OS 73% | 0% |
| Mercadal S, 2008 [46] | All subtypes including 1 ALK+ ALCL | 41 | High-dose CHOP/ESHAP | 59%/49% | 41% | 4-y PFS: 30% 4-y OS: 39% | 0% |
| Reimer P, 2009 [47] | All subtypes excluding ALK+ ALCL | 83 | CHOP | 79%/39% | 66% | 3-y PFS: 36% 3-y OS: 48% | 3.6% |
| D’Amore F, 2012 [14] | All subtypes excluding ALK+ ALCL | 160 | CHOEP | 82%/51% | 72% | 5-y PFS: 44% 5-y OS: 51% | 4% |
| Wilhelm M, 2016 (extension and update of Reimer P, 2009) [47,48] | All subtypes excluding ALK+ ALCL | 111 | CHOP | 82%/62% | 68% | 5-y PFS: 39% 5-y OS: 44% | 3.6% |
| Reference | Type of Study | PTCL Subtype | Main Results |
|---|---|---|---|
| Ellin F, 2014 [9] | Swedish Lymphoma Registry | Nodal PTCL and EATL excluding ALK+ ALCL | In an intention-to-treat analysis in 252 nodal PTCLs and EATL patients excluding ALK+ ALCL, planned upfront autoSCT (n = 128) was associated with a superior PFS (HR, 0.56; p = 0.002) and OS (HR, 0.58; p = 0.004) compared with patients treated without autoSCT (n = 124). |
| Fossard G, 2018 [51] | LYSA study | Nodal PTCL excluding ALK+ ALCL | In an intention-to-treat analysis in 269 nodal PTCL patients excluding ALK+ ALCL, there was no significant difference in PFS and OS between planned upfront autoSCT group (n = 134) and patients treated without autoSCT (n = 135). |
| Sibon D, 2019 [12] | International pooled analysis | ALK+ ALCL | Among 263 pts, 34 underwent upfront autoSCT (all were <60 years). For patients <60 years in CR or PR, in stratified Cox models including etoposide-based induction, IPI and upfront autoSCT, only the etoposide-based induction and the IPI remained independently prognostic for PFS and OS, without impact of autoSCT |
| PTCL Subtype | Study Type | Treatment | n | CR Rate | Survival | Reference |
|---|---|---|---|---|---|---|
| AITL | Retrospective (LYSA) | Mainly CHOP and ACVBP | 157 | 46% | 2-y EFS: 38% 2-y OS: 51% | Mourad N, 2008 [54] |
| AITL | Retrospective (Japan) | Mainly CHOP and THP-COP | 207 | 66% | 3-y PFS: 38% 3-y OS: 54% | Tokunaga T, 2012 [55] |
| AITL | Phase 2 (LYSA) | Rituximab-CHOP | 25 | 44% | 2-y PFS: 42% 2-y OS: 62% | Delfay-Larue MH, 2012 [56] |
| AITL | Retrospective (IPTCL) | Mainly CHOP | 243 | 61% | 5-y FFS: 18% 5-y OS: 32% | Federico M, 2013 [57] |
| AITL | Phase 2 (LYSA) | Lenalidomide-CHOP | 78 | 41% | 2-y PFS: 42% 2-y OS: 59% | Lemonnier F, 2021 [58] |
| AITL | Prospective observational (ITCP) | Mainly CHOP | 282 | 51% | 3-y PFS: 38% 3-y OS: 50% | Advani RH, 2021 [59] |
| PTCL-NOS | Retrospective (IIL Lymphoma Registry) | Mainly CHOP | 385 | 53% | 5-y OS: 43% | Gallamini A, 2004 [60] |
| PTCL-NOS | Retrospective (IPTCL) | Mainly CHOP | 340 | 56% | 5-y FFS: 20% 5-y OS: 32% | Weisenburger DD, 2011 [61] |
| PTCL-NOS | Prospective observational (ITCP) | Mainly CHOP | 311 | ND | 5-y PFS: 23% 5-y OS: 32% | Federico M, 2018 [62] |
| ALK− ALCL | Prospective observational (ITCP) | Mainly CHOP | 235 | 63% | 5-y PFS: 43% 5-y OS: 49% | Shustov A, 2021 [19] |
| ALK+ ALCL | Retrospective (Nordic Lymphoma Group) | CHOEP and CHOP | CHOEP n = 27 CHOP n = 17 (pts 41–65 years) | ND | 5-y OS CHOEP: 78% CHOP: 47% | Cederleuf H, 2017 [18] |
| ALK+ ALCL | Retrospective (international pooled analysis) | Mainly CHOEP and CHOP | CHOEP n = 38 CHOP n = 98 (pts ≥ 18 years) | ND | 5-y OS CHOEP: 97% CHOP: 69% | Sibon D, 2019 [12] |
| Reference | ALK Inhibitor | Phase | n and Dosage | Median Age | ORR/CR | PFS |
|---|---|---|---|---|---|---|
| Brugières L, 2017 [73] | Crizotinib | 2 | n = 18 250 mg ×2/d (adults) 165 mg/m2 ×2/d (children) | 20 (1–60) | 67%/40% | 1-y PFS 48% |
| Mossé Y, 2017 [74] | Crizotinib | 1–2 | n = 6 (165 mg/m2 ×2/d) n = 20 (280 mg/m2 ×2/d) | 5.9 (3–13) 12.2 (6–20) | 83%/83% 90%/80% | - |
| Gambacorti-Passerini C, 2018 [75] | Crizotinib | 1b | n = 18 (250 mg ×2/d) | 25 (15–37) | 53%/47% | 2-y PFS 63% |
| Bossi E, 2020 [76] | Crizotinib | 2 | n = 12 (250 mg ×2/d) | 31 (18–83) | 83%/58% | 2-y PFS 65% |
| Fukano R, 2020 [77] | Alectinib | 2 | n = 10 300 mg ×2/d (≥35 kg) 150 mg ×2/d (<35 kg) | 19.5 (6–70) | 80%/60% | 1-y PFS 58% |
| Fischer M, 2021 [78] | Ceritinib | 1 | n = 8 (500 mg/m2) | Children | 75%/25% | 1-y PFS 67% |
| Study | PTCL Subtype | n | Survival | TRM |
|---|---|---|---|---|
| Rodriguez J, 2003 [80] | All subtypes | 78 | 5-y OS: 45% | 8% |
| Nademanee A, 2011 [81] | All subtypes | 55 | 5-y OS: 45% | 0% |
| Smith S, 2013 [82] | All subtypes | 94 | 3-y OS: 53% | 6% |
| El-Asmar J, 2016 (Meta-analysis) [83] | All subtypes | 581 | OS 47% | 10% |
| Bellei M, 2018 [63] | All subtypes | 99 (compared to 124 eligible CR-PR patients, not transplanted) | Transplanted: 3-y OS: 48% Not transplanted: 3-y OS: 27% | - |
| Knörr F, 2020 (prospective) [79] | ALK+ ALCL (≤21 years) | 22 | 5-y EFS: 41% 5-y OS: 82% | 2 deaths |
| Study | PTCL Subtype | N | Survival | NRM |
|---|---|---|---|---|
| Corradini P, 2004 (prospective) [84] | Nodal PTCL excluding ALK+ ALCL | 17 | 3-y PFS: 64% 3-y OS: 81% | 6% at 2 years |
| Knörr F, 2020 (prospective) [79] | ALK+ ALCL (≤21 years) | 36 | 5-y EFS: 81% 5-y OS: 83% | 2 deaths |
| Le Gouill S, 2008 [85] | All subtypes | 77 | 5-y EFS: 53% 5-y OS: 57% | 33% at 5 years |
| Dodero A, 2012 [86] | All subtypes | 52 | 5-y PFS: 40% 5-y OS: 50% | 12% at 5 years |
| Smith S, 2013 [82] | All subtypes | 93 | Myeloablative: 3-y PFS: 29% 3-y OS: 31% Non-myeloablative: 3-y PFS: 32% 3-y OS: 50% | Myeloablative: 34% at 3 years Non myeloablative: 27% at 3 years |
| Epperla N, 2019 [87] | AITL | 249 | 4-y PFS: 49% 4-y OS: 56% | 30% at 4 years |
| Mamez AC, 2020 [53] | All subtypes | 147 | CR ≥ 2 or PR ≥ 2: 4-y OS: 61% Progressive disease: 4-y OS: 37% | CR ≥ 2 or PR ≥ 2: 30% at 4 years Progressive disease: 40% at 4 years |
| Agent | Target | Phase | No. of Evaluable Patients (Excluding CTCL) | ORR/CR | Survival | Reference |
|---|---|---|---|---|---|---|
| Romidepsin | HDAC | 2 | 130 | 25%/15% | Median PFS 4 mo | Coiffier B, 2012 [89] |
| Belinostat | HDAC | 2 | 120 | 26%/11% | Median PFS 1.6 mo Median OS 7.9 mo | O’Connor OA, 2015 [90] |
| Chidamide | HDAC | 2 | 79 | 28%/14% | Median PFS 2.1 mo Median OS 21.4 mo | Shi Y, 2015 [91] |
| Alisertib | Aurora A kinase | 2 | 30 | 30%/7% | 1-y PFS: 8%; Median 3 mo 1-y OS: 30%; Median 8 mo | Barr PM, 2015 [92] |
| Alisertib | Aurora A kinase | 3 | 271 | 33%/18% | Median PFS 115 versus 104 days for the comparator arm | O’Connor OA, 2019 [93] |
| Copanlisib | PI3K-α/δ | 2 | 14 | 21%/14% | - | Dreyling M, 2017 [94] |
| Duvelisib | PI3K-δ/γ | 1 | 16 | 50%/19% | Median PFS 8.3 mo Median OS 8.4 mo | Horwitz SM, 2018 [95] |
| Tenalisib | PI3K-δ/γ | 1 | 15 | 47%/20% | - | Huen A, 2020 [96] |
| Ibrutinib | BTK | 1 | 7 | 0%/0% | - | Kumar A, 2018 [97] |
| Ruxolitinib | JAK1/2 | 2 | 45 | 27%/7% | Median PFS * 2.8 mo Median OS * 26.2 mo | Moskowitz AJ, 2021 [98] |
| Dasatinib | Multiple kinases | 1 | 9 | 29%/22% | Median PFS 2.5 mo Median OS 4.5 mo | Umakanthan JM, 2019 [99] |
| Lenalidomide | Immunomodulation Angiogenesis | 2 | 54 | 22%/11% | Median PFS 2.5 mo | Morschhauser F, 2013 [100] |
| Lenalidomide | Immunomodulation Angiogenesis | 2 | 39 (8 in first-line) | 26%/8% | Median PFS 4 mo Median OS 12 mo | Toumishey E, 2015 [101] |
| Pembrolizumab | PD1 | 2 | 15 | 33%/27% | Median PFS 3.2 mo Median OS 10.6 mo | Barta SK, 2019 [102] |
| Geptanolimab | PD1 | 2 | 89 | 40%/15% | Median PFS 2.7 mo Median OS 14.6 mo | Shi Y, 2021 [103] |
| Plitidepsin | eEF1A2 | 2 | 29 | 21%/7% | Median PFS 1.6 mo Median OS 10.2 mo | Ribrag V, 2013 [104]; Losada A [105] |
| Pralatrexate | Folates | 2 | 111 | 29%/11% | Median PFS 3.5 mo Median OS 14.5 mo | O’Connor OA, 2011 [106] |
| Ixazomib | Proteasome | 2 | 7 | 14%/14% | - | Boonstra PS, 2017 [107] |
| Carfilzomib | Proteasome | 1 | 12 | 25%/17% | Median PFS 2.8 mo Median OS 23 mo | Krishnan M, 2022 [108] |
| Agent | Phase | No. of Evaluable Patients (Excluding CTCL) | ORR/CR | Survival | Reference |
|---|---|---|---|---|---|
| Lenalidomide-Vorinostat—Dexamethasone | 1–2 | 8 | 25%/12.5% | Median PFS 2.2 mo Median OS 6.7 mo | Hopfinger G, 2014 [109] |
| Panobinostat—Bortezomib | 2 | 23 | 43%/22% | Median PFS 2.6 mo Median OS 9.9 mo | Tan D, 2015 [110] |
| Gemcitabine—Romidepsin | 2 | 20 | 30%/15% | Median PFS 2.5 mo Median OS 22 mo | Pellegrini C, 2016 [111] |
| Bortezomib—Romidepsin | 1 | 2 | 0%/0% | - | Holkova B, 2017 [112] |
| Romidepsin—Pralatrexate | 1 | 14 | 71%/29% | Median PFS 4.4 mo Median OS 12.4 mo | Amengual J, 2018 [113] |
| Romidepsin—ICE | 1 | 15 | 93%/80% | Median PFS 10 mo Median OS 15 mo | Strati P, 2018 [114] |
| Oral 5-Azacytidine—Romidepsin | 1 | 6 | 71%/71% | Median PFS not reached after a median follow-up of 15.3 mo | O’Connor OA, 2019 [115] |
| Selinexor—DICE | 1 | 10 | 91%/82% | Median OS not reached after a median follow-up of 32.3 mo | Tang T, 2020 [116] |
| Gemcitabine—Copanlisib | 1–2 | 25 (phase 2) | 72%/32% | Median PFS 6.9 mo Median OS not reached | Yhim H-Y, 2021 [117] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sibon, D. Peripheral T-Cell Lymphomas: Therapeutic Approaches. Cancers 2022, 14, 2332. https://doi.org/10.3390/cancers14092332
Sibon D. Peripheral T-Cell Lymphomas: Therapeutic Approaches. Cancers. 2022; 14(9):2332. https://doi.org/10.3390/cancers14092332
Chicago/Turabian StyleSibon, David. 2022. "Peripheral T-Cell Lymphomas: Therapeutic Approaches" Cancers 14, no. 9: 2332. https://doi.org/10.3390/cancers14092332
APA StyleSibon, D. (2022). Peripheral T-Cell Lymphomas: Therapeutic Approaches. Cancers, 14(9), 2332. https://doi.org/10.3390/cancers14092332