
Minimally Invasive Endoscopic and Surgical Management of Rectal Neoplasia



Abstract
:Simple Summary
Abstract
1. Introduction
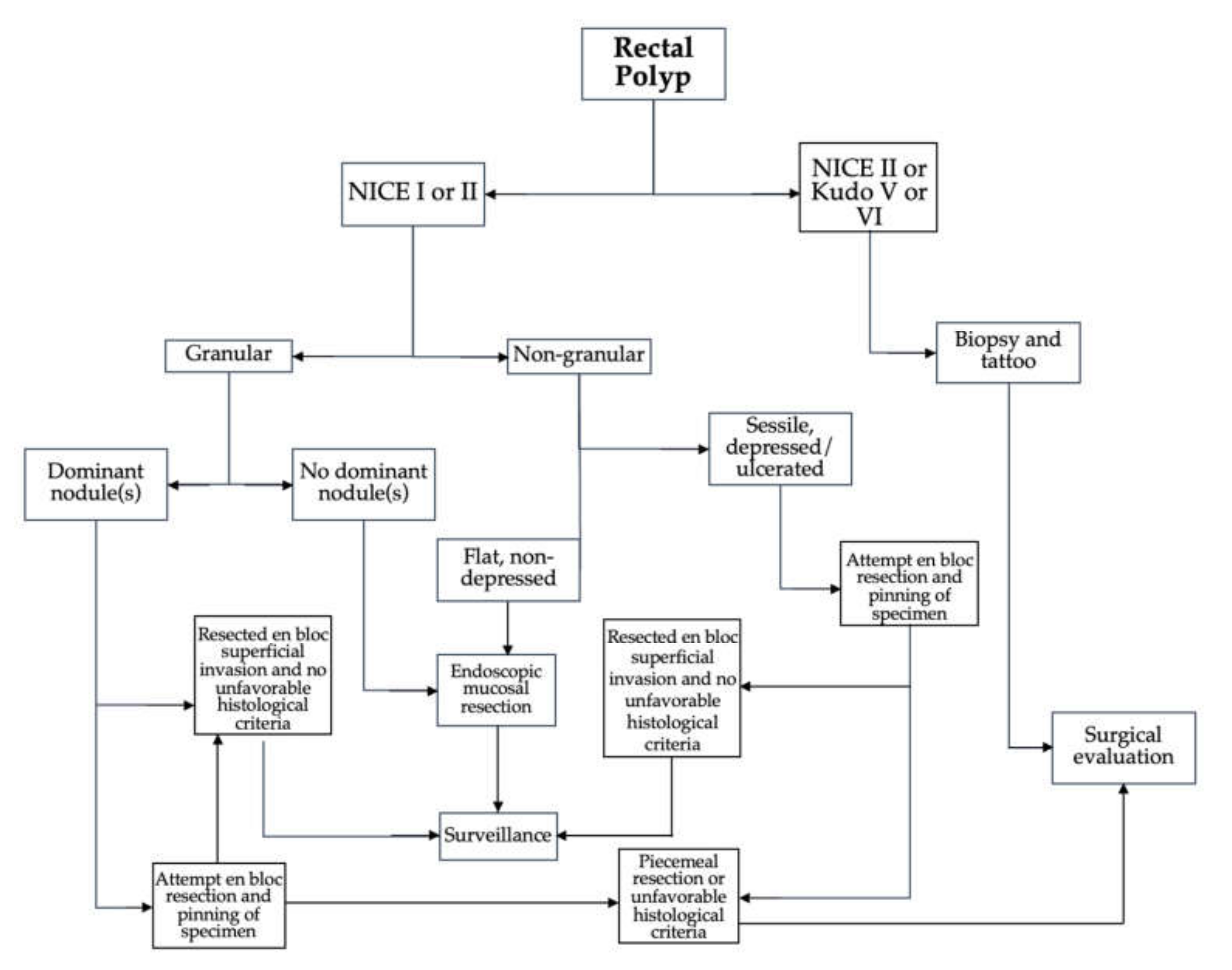
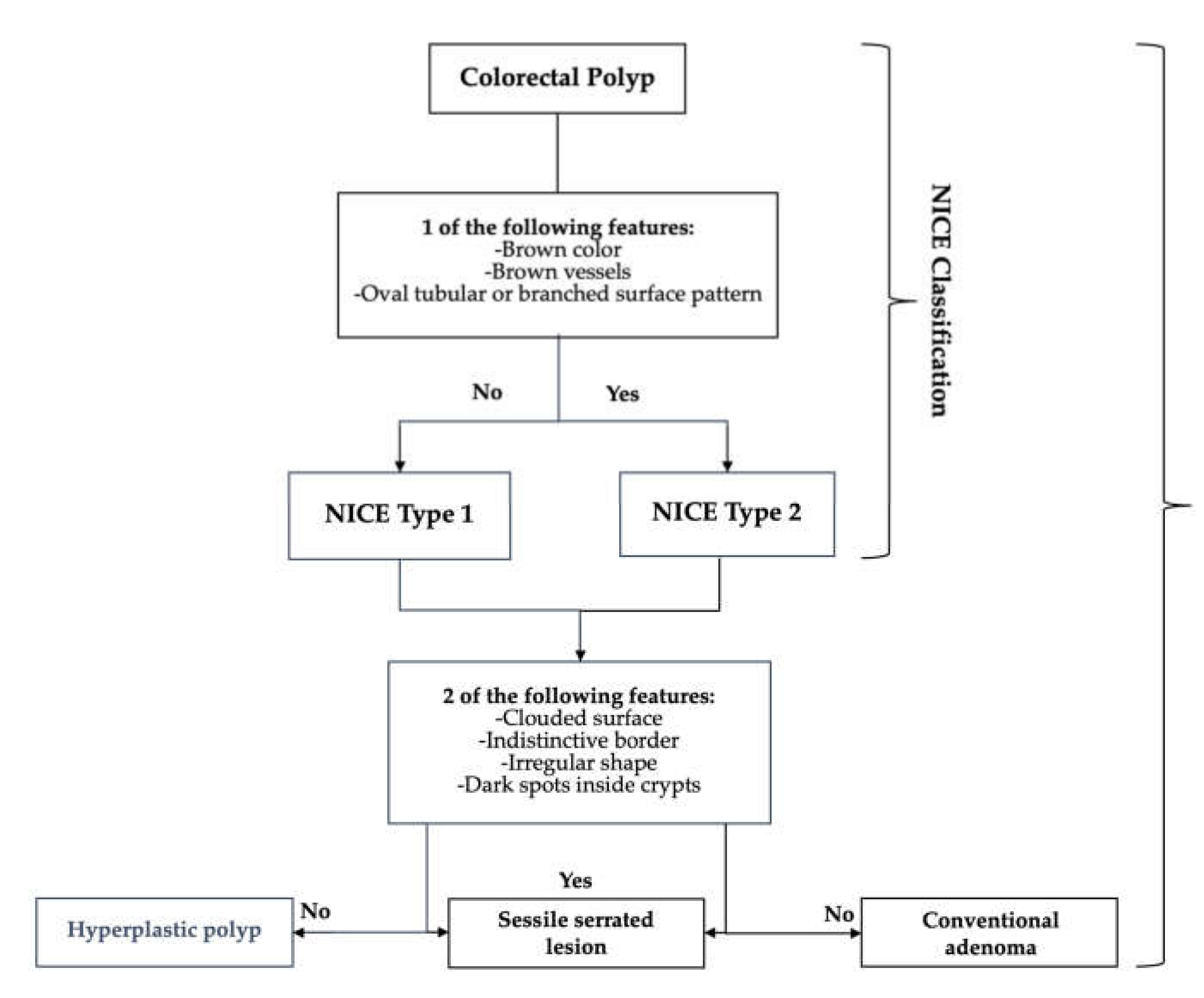
2. Approach to Diagnosis and Staging
3. Endoscopic Approaches to Therapy
3.1. Endoscopic Mucosal Resection
3.2. Endoscopic Full-Thickness Resection
3.3. Endoscopic Submucosal Dissection
4. Surgical Approaches to Therapy
4.1. Transanal Approaches
4.2. Locally Advanced Rectal Cancer
5. Future Directions
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Brenner, H.; Stock, C.; Hoffmeister, M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: Systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ 2014, 348, g2467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaukat, A.; Kaltenbach, T.; Dominitz, J.A.; Robertson, D.J.; Anderson, J.C.; Cruise, M.; Burke, C.A.; Gupta, S.; Lieberman, D.; Syngal, S.; et al. Endoscopic Recognition and Management Strategies for Malignant Colorectal Polyps: Recommendations of the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology 2020, 159, 1916–1934.e2. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Jung, S.A.; Shim, K.N.; Cho, W.; Keum, B.; Byeon, J.; Huh, K.; Jang, B.; Chang, D.; Jung, H.; et al. Meta-analysis of predictive clinicopathologic factors for lymph node metastasis in patients with early colorectal carcinoma. J. Korean Med. Sci. 2015, 30, 398–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pimentel-Nunes, P.; Dinis-Ribeiro, M.; Ponchon, T.; Repici, A.; Vieth, M.; De Ceglie, A.; Amato, A.; Berr, F.; Bhandari, P.; Bialek, A.; et al. Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2015, 47, 829–854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakajima, T.; Saito, Y.; Tanaka, S.; Iishi, H.; Kudo, S.; Ikematsu, H.; Igarashi, M.; Saitoh, Y.; Inoue, Y.; Kobayashi, K.; et al. Current status of endoscopic resection strategy for large, early colorectal neoplasia in Japan and Other Interventional Techniques. Surg. Endosc. 2013, 27, 3262–3270. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. National Comprehensive Cancer Network Guidelines, Rectal Cancer; Version 2.2021. 2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf (accessed on 7 February 2022).
- Kiriyama, S.; Saito, Y.; Matsuda, T.; Nakajima, T.; Mashimo, Y.; Joeng, H.; Moriya, Y.; Kuwano, H. Comparing endoscopic submucosal dissection with transanal resection for non-invasive rectal tumor: A retrospective study. J. Gastroenterol. Hepatol. 2011, 26, 1028–1033. [Google Scholar] [CrossRef]
- Sagae, V.M.T.; Ribeiro, I.B.; de Moura, D.T.H.; Brunaldi, V.; Logiudice, F.; Funari, M.; Baba, E.; Bernardo, W.; de Moura, E. Endoscopic submucosal dissection versus transanal endoscopic surgery for the treatment of early rectal tumor: A systematic review and meta-analysis. Surg. Endosc. 2020, 34, 1025–1034. [Google Scholar] [CrossRef]
- Kudo, S.; Hirota, S.; Nakajima, T.; Hosobe, S.; Kusaka, H.; Kobayashi, T.; Himori, M.; Yagyuu, A. Colorectal Tumours and Pit Pattern. J. Clin. Pathol. 1994, 47, 880–885. [Google Scholar] [CrossRef] [Green Version]
- Jspeert, J.E.; Bastiaansen, B.A.; van Leerdam, M.E.; Meijer, G.A.; van Eeden, S.; Sanduleanu, S.; Schoon, E.J.; Bisseling, T.M.; Spaander, M.C.; van Lelyveld, N.; et al. Dutch Workgroup serrAted polypS & Polyposis (WASP). Development and validation of the WASP classification system for optical diagnosis of adenomas, hyperplastic polyps and sessile serrated adenomas/polyps. Gut 2016, 65, 963–970. [Google Scholar] [CrossRef]
- Bisschops, R.; Hassan, C.; Bhandari, P.; Coron, E.; Neumann, H.; Pech, O.; Correale, L.; Repici, A. BASIC (BLI Adenoma Serrated International Classification) classification for colorectal polyp characterization with blue light imaging. Endoscopy 2018, 50, 211–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, N.; Tanaka, S.; Hewett, D.G.; Kaltenbach, T.R.; Sano, Y.; Ponchon, T.; Saunders, B.P.; Rex, D.K.; Soetiko, R.M. Endoscopic prediction of deep submucosal invasive carcinoma: Validation of the Narrow-Band Imaging International Colorectal Endoscopic (NICE) classification. Gastrointest. Endosc. 2013, 78, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Aihara, H.; Perbtani, Y.B.; Wang, A.Y.; Aadam, A.A.; Tomizawa, Y.; Hwang, J.H.; Zou, B.; Natov, N.S.; Siegel, A.; et al. Safety and efficacy of endoscopic submucosal dissection for rectal neoplasia: A multicenter North American experience. Endosc. Int. Open 2019, 7, E1714–E1722. [Google Scholar] [CrossRef] [Green Version]
- Kudo, S.; Lambert, R.; Allen, J.I.; Fujii, H.; Fujii, T.; Kashida, H.; Matsuda, T.; Mori, M.; Saito, H.; Shimoda, T.; et al. Nonpolypoid neoplastic lesions of the colorectal mucosa. Gastrointest. Endosc. 2008, 68, S3–S47. [Google Scholar] [CrossRef] [PubMed]
- Uraoka, T.; Saito, Y.; Matsuda, T.; Ikehara, H.; Gotoda, T.; Saito, D.; Fujii, T. Endoscopic indications for endoscopic mucosal resection of laterally spreading tumours in the colorectum. Gut 2006, 55, 1592–1597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogie, R.; Veldman, M.; Snijders, L.; Winkens, B.; Kaltenbach, T.; Masclee, A.; Matsuda, T.; Rondagh, E.; Soetikno, R.; Tanaka, S.; et al. Endoscopic subtypes of colorectal laterally spreading tumors (LSTs) and the risk of submucosal invasion: A meta-analysis. Endoscopy 2018, 50, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Fuccio, L.; Repici, A.; Hassan, C.; Ponchon, T.; Bhandari, P.; Jover, R.; Triantafyllou, K.; Mandolesi, D.; Frazzoni, L.; Bellisario, C.; et al. Why attempt en bloc resection of non-pedunculated colorectal adenomas? A systematic review of the prevalence of superficial submucosal invasive cancer after endoscopic submucosal dissection. Gut 2018, 67, 1464–1474. [Google Scholar] [CrossRef]
- Rausa, E.; Kelly, M.E.; Bonavina, L.; O’Connell, P.R.; Winter, D.C. A systematic review examining quality of life following pelvic exenteration for locally advanced and recurrent rectal cancer. Color. Dis. 2017, 19, 430–436. [Google Scholar] [CrossRef]
- Wrenn, S.M.; Cepeda-Benito, A.; Ramos-Valadez, D.I.; Cataldo, P.A. Patient perceptions and quality of life after colon and rectal surgery: What do patients really want? In Diseases of the Colon and Rectum; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2018; Volume 61, pp. 971–978. [Google Scholar] [CrossRef]
- D’Amico, F.; Amato, A.; Iannone, A.; Trovato, C.; Romana, C.; Angeletti, S.; Maselli, R.; Radaelli, F.; Fiori, G.; Viale, E.; et al. Risk of Covert Submucosal Cancer in Patients With Granular Mixed Laterally Spreading Tumors. Clin. Gastroenterol. Hepatol. 2020, 19, 1395–1401. [Google Scholar] [CrossRef]
- Medina-Prado, L.; Hassan, C.; Dekker, E.; Bisschops, R.; Alfieri, S.; Bhandari, P.; Bourke, M.; Bravo, R.; Bustamante-Balen, M.; Dominitz, J.; et al. When and How To Use Endoscopic Tattooing in the Colon: An International Delphi Agreement. Clin. Gastroenterol. Hepatol. 2021, 19, 1038–1050. [Google Scholar] [CrossRef]
- Worrell, S.; Horvath, K.; Blakemore, T.; Flum, D. Endorectal ultrasound detection of focal carcinoma within rectal adenomas. Am. J. Surg. 2004, 187, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Bipat, S.; Glas, A.S.; Slors, F.J.M.; Zwinderman, A.H.; Bossuyt, P.M.M.; Stoker, J. Rectal cancer: Local staging and assessment of lymph node involvement with endoluminal US, CT, and MR imaging—A meta-analysis. Radiology 2004, 232, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Balyasnikova, S.; Brown, G. Optimal Imaging Strategies for Rectal Cancer Staging and Ongoing Management. Curr. Treat. Options Oncol. 2016, 17, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lutz, M.P.; Zalcberg, J.R.; Glynne-Jones, R.; Ruers, T.; Ducreaux, M.; Arnold, D.; Aust, D.; Brown, G.; Bujko, K.; Cunninghan, C.; et al. Second St. Gallen European Organisation for Research and Treatment of Cancer Gastrointestinal Cancer Conference: Consensus recommendations on controversial issues in the primary treatment of rectal cancer. Eur. J. Cancer 2016, 63, 11–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkinson, N. Management of Rectal Cancer. Surg. Clin. N. Am. 2020, 100, 615–628. [Google Scholar] [CrossRef] [PubMed]
- Oka, S.; Tanaka, S.; Saito, Y.; Iishi, H.; Kudo, S.; Ikematsu, H.; Igarashi, M.; Saitoh, Y.; Inoue, Y.; Kobayashi, K.; et al. Local recurrence after endoscopic resection for large colorectal neoplasia: A multicenter prospective study in Japan. Am. J. Gastroenterol. 2015, 110, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Tutticci, N.J.; Hewett, D.G. Cold EMR of large sessile serrated polyps at colonoscopy (with video). Gastrointest. Endosc. 2018, 87, 837–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tate, D.; Awadie, H.; Bahin, F.; Desomer, L.; Lee, R.; Heitman, S.; Goodrick, K.; Bourke, M. Wide-field piecemeal cold snare polypectomy of large sessile serrated polyps without a submucosal injection is safe. Endoscopy 2018, 50, 248–252. [Google Scholar] [CrossRef]
- Thoguluva Chandrasekar, V.; Spadaccini, M.; Aziz, M.; Maselli, R.; Hassan, S.; Fuccio, L.; Duvvuri, A.; Frazzoni, L.; Desai, M.; Fugazza, A.; et al. Cold snare endoscopic resection of nonpedunculated colorectal polyps larger than 10 mm: A systematic review and pooled-analysis. Gastrointest. Endosc. 2019, 89, 929–936.e3. [Google Scholar] [CrossRef] [Green Version]
- Van Hattem, W.; Shahidi, N.; Vosko, S.; Hartley, I.; Britto, K.; Sidhu, M.; Bar-Yishay, I.; Schoeman, S.; Tate, D.; Byth, K.; et al. Piecemeal cold snare polypectomy versus conventional endoscopic mucosal resection for large sessile serrated lesions: A retrospective comparison across two successive periods. Gut 2020, 70, 1691–1697. [Google Scholar] [CrossRef]
- Kimoto, Y.; Sakai, E.; Inamoto, R.; Kurebayashi, M.; Takayanagi, S.; Hirata, T.; Suzuki, Y.; Ishii, R.; Konishi, T.; Kanda, K.; et al. Safety and Efficacy of Cold Snare Polypectomy Without Submucosal Injection for Large Sessile Serrated Lesions: A Prospective Study. Clin. Gastroenterol. Hepatol. 2020, 20, e132–e138. [Google Scholar] [CrossRef] [PubMed]
- Mcwhinney, C.D.; Vemulapalli, K.C.; El Rahyel, A.; Abdullah, N.; Rex, D.K. Adverse events and residual lesion rate after cold endoscopic mucosal resection of serrated lesions. Gastrointest. Endosc. 2021, 93, 2021. [Google Scholar] [CrossRef] [PubMed]
- Klein, A.; Tate, D.J.; Jayasekeran, V.; Hourigan, L.; Singh, R.; Brown, G.; Bahin, F.F.; Burgess, N.; Williams, S.J.; Lee, E.; et al. Thermal Ablation of Mucosal Defect Margins Reduces Adenoma Recurrence After Colonic Endoscopic Mucosal Resection. Gastroenterology 2019, 156, 604–613.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sidhu, M.; Shahidi, N.; Gupta, S.; Desomer, L.; Vosko, S.; Arnout van Hattem, W.; Hourigan, L.F.; Lee, E.Y.T.; Moss, A.; Raftopoulos, S.; et al. Outcomes of Thermal Ablation of the Mucosal Defect Margin After Endoscopic Mucosal Resection: A Prospective, International, Multicenter Trial of 1000 Large Nonpedunculated Colorectal Polyps. Gastroenterology 2021, 161, 163–170.e3. [Google Scholar] [CrossRef]
- Chandan, S.; Facciorusso, A.; Ramai, D.; Deliwala, S.; Mohan, B.P.; Kassab, L.L.; Draganov, P.V.; Othman, M.O.; Kochhar, G.S. Snare tip soft coagulation (STSC) after endoscopic mucosal resection (EMR) of large (>20 mm) non pedunculated colorectal polyps: A systematic review and meta-analysis. Endosc. Int. Open 2022, 10, E74–E81. [Google Scholar] [CrossRef]
- Trindade, A.; Kumta, N.; Bhutani, M.; Chandrasekhara, V.; Jirapinyo, P.; Krishnan, K.; Melson, J.; Pannala, R.; Parsi, M.; Schulman, A.; et al. Devices and techniques for endoscopic treatment of residual and fibrotic colorectal polyps (with videos). Gastrointest. Endosc. 2020, 92, 474–482. [Google Scholar] [CrossRef]
- Zwager, L.; Bastiaansen, B.; Bronzwaer, M.; Van Der Spek, B.; Heine, G.; Haasnoot, K.; Van Der Sluis, H.; Perk, L.; Boonstra, J.; Rietdijk, S.; et al. Endoscopic full-thickness resection (eFTR) of colorectal lesions: Results from the Dutch colorectal eFTR registry. Endoscopy 2020, 52, 1014–1023. [Google Scholar] [CrossRef]
- Tanaka, S.; Kashida, H.; Saito, Y.; Yahagi, N.; Yamano, H.; Saito, S.; Hisabe, T.; Yao, T.; Watanabe, M.; Yoshida, M.; et al. Japan Gastroenterological Endoscopy Society guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig. Endosc. 2020, 32, 219–239. [Google Scholar] [CrossRef]
- Lopimpisuth, C.; Simons, M.; Akshintala, V.S.; Prasongdee, K.; Nanavati, J.; Ngamruengphong, S. Traction-assisted endoscopic submucosal dissection reduces procedure time and risk of serious adverse events: A systematic review and meta-analysis. Surg. Endosc. 2021. [Google Scholar] [CrossRef]
- Tsuji, K.; Yoshida, N.; Nakanishi, H.; Takemura, K.; Yamada, S.; Doyama, H. Recent traction methods for endoscopic submucosal Dissection. World J. Gastroenterol. 2016, 22, 5917–5926. [Google Scholar] [CrossRef]
- Zhao, H.J.; Yin, J.; Ji, C.Y.; Wang, X.; Wang, N. Endoscopic mucosal resection versus endoscopic submucosal dissection for colorectal laterally spreading tumors: A meta-analysis. Rev. Esp. Enferm. Dig. 2020, 112, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, X.H.; Ge, J.; Yang, C.M.; Liu, J.Y.; Zhao, S.L. Endoscopic submucosal dissection vs endoscopic mucosal resection for colorectal tumors: A meta-analysis. World J. Gastroenterol. 2014, 20, 8282–8287. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, N.; Yoshitake, N.; Hirahara, Y.; Konishi, J.; Saito, Y.; Matsuda, T.; Ishikawa, T.; Sekiguchi, R.; Fujimori, T. Matched case-control study comparing endoscopic submucosal dissection and endoscopic mucosal resection for colorectal tumors. J. Gastroenterol. Hepatol. 2012, 27, 728–733. [Google Scholar] [CrossRef] [PubMed]
- Kotzev, A.; Yang, D.; Draganov, P. How to master endoscopic submucosal dissection in the USA. Dig. Endosc. 2019, 31, 94–100. [Google Scholar] [CrossRef] [PubMed]
- McCarty, T.R.; Aihara, H. Current state of education and training for endoscopic submucosal dissection: Translating strategy and success to the USA. Dig. Endosc. 2020, 32, 851–860. [Google Scholar] [CrossRef]
- Draganov, P.; Aihara, H.; Karasik, M.; Ngamruengphong, S.; Aadam, A.; Othman, M.; Sharma, N.; Grimm, I.; Rostom, A.; Elmunzer, B.; et al. Endoscopic Submucosal Dissection in North America: A Large Prospective Multicenter Study. Gastroenterology 2021, 160, 2317–2327.e2. [Google Scholar] [CrossRef]
- Saito, Y.; Fukuzawa, M.; Matsuda, T.; Fukunaga, S.; Sakamoto, T.; Uraoka, T.; Nakajima, T.; Ikehara, H.; Fu, K.; Itoi, T.; et al. Clinical outcome of endoscopic submucosal dissection versus endoscopic mucosal resection of large colorectal tumors as determined by curative resection. Surg. Endosc. 2010, 24, 343–352. [Google Scholar] [CrossRef]
- Fujiya, M.; Tanaka, K.; Dokoshi, T.; Tominaga, M.; Ueno, N.; Inaba, Y.; Ito, T.; Moriichi, K.; Kohgo, Y.; Asahikawa, P.; et al. Efficacy and adverse events of EMR and endoscopic submucosal dissection for the treatment of colon neoplasms: A meta-analysis of studies comparing EMR and endoscopic submucosal dissection. Gastrointest. Endosc. 2015, 81, 583–595. [Google Scholar] [CrossRef]
- Shergill, A.; Lightdale, M.; Bruining, D.; Acosta, R.; Chandrasekhara, V.; Chatadi, K.; Anton Decker, G.; Early, D.; Evans, J.; Fanelli, R.; et al. The role of endoscopy in inflammatory bowel disease. Gastrointest. Endosc. 2015, 81, 1101–1121.e13. [Google Scholar] [CrossRef]
- Chen, W.; Zhang, Y.L.; Zhao, Y.; Yang, A.M.; Qian, J.M.; Wu, D. Endoscopic resection for non-polypoid dysplasia in inflammatory bowel disease: A systematic review and meta-analysis. Surg. Endosc. 2021, 35, 1534–1543. [Google Scholar] [CrossRef]
- Quirke, P.; Steele, R.; Monson, J.; Grieve, R.; Khanna, S.; Couture, J.; O’Callaghan, C.; Myint, A.; Bessell, E.; Thompson, L.; et al. Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: A prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. Lancet 2009, 373, 821–828. [Google Scholar] [CrossRef] [Green Version]
- Guillou, P.; Quirke, P.; Thorpe, H.; Walker, J.; Jayne, D.; Smith, A.; Heath, R.; Brown, J. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): Multicentre, randomised controlled trial. Lancet 2005, 365, 1718–1726. [Google Scholar] [CrossRef]
- Fleshman, J.; Branda, M.; Sargent, D.; Boller, A.; George, V.; Abbas, M.; Peters, W.; Maun, D.; Chang, G.; Herline, A.; et al. Effect of laparoscopic-assisted resection vs open resection of stage II or III rectal cancer on pathologic outcomes the ACOSOG Z6051 randomized clinical trial. JAMA J. Am. Med. Assoc. 2015, 314, 1346–1355. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, A.; Solomon, M.; Lumley, J.; Hewett, P.; Clouston, A.; Gebski, V.; Davies, L.; Wilson, K.; Hague, W.; Simes, J. Effect of laparoscopic-assisted resection vs open resection on pathological outcomes in rectal cancer: The ALaCaRT randomized clinical trial. JAMA J. Am. Med. Assoc. 2015, 314, 1356–1363. [Google Scholar] [CrossRef] [Green Version]
- Jayne, D.; Pigazzi, A.; Marshall, H.; Croft, J.; Corrigan, N.; Copeland, J.; Quirke, P.; West, N.; Rautio, T.; Thomassen, N.; et al. Effect of robotic-assisted vs conventional laparoscopic surgery on risk of conversion to open laparotomy among patients undergoing resection for rectal cancer the rolarr randomized clinical trial. JAMA J. Am. Med. Assoc. 2017, 318, 1569–1580. [Google Scholar] [CrossRef]
- Taylor, F.; Quirke, P.; Heald, R.; Moran, B.; Blomqvist, L.; Swift, I.; Sebag-Montefiore, D.; Tekkis, P.; Brown, G. Preoperative high-resolution magnetic resonance imaging can identify good prognosis stage I, II, and III rectal cancer best managed by surgery alone: A prospective, multicenter, European study. Ann. Surg. 2011, 253, 711–719. [Google Scholar] [CrossRef]
- Law, W.L.; Chu, K.W.; Choi, H.K. Total pelvic exenteration for locally advanced rectal cancer. J. Am. Coll. Surg. 2000, 190, 78–83. [Google Scholar] [CrossRef]
- PelvEx Collaborative. Surgical and Survival Outcomes Following Pelvic Exenteration for Locally Advanced Primary Rectal Cancer: Results From an International Collaboration. Ann. Surg. 2019, 269, 315–321. [Google Scholar] [CrossRef]
- Akiyoshi, T.; Watanabe, T.; Miyata, S.; Kotake, K.; Muto, T.; Sugihara, K. Results of a Japanese nationwide multi-institutional study on lateral pelvic lymph node metastasis in low rectal cancer: Is it regional or distant disease? Ann. Surg. 2012, 255, 1129–1134. [Google Scholar] [CrossRef]
- Peacock, O.; Chang, G.J. The Landmark Series: Management of Lateral Lymph Nodes in Locally Advanced Rectal Cancer. Ann. Surg. Oncol. 2020, 27, 2723–2731. [Google Scholar] [CrossRef]
- Kusters, M.; Valentini, V.; Calvo, F.A.; Krempien, R.; Nieuwenhujizen, G.; Martijn, H.; Doglietto, G.; del Valle, E.; Roeder, F.; Buchler, M.; et al. Results of European pooled analysis of IORT-containing multimodality treatment for locally advanced rectal cancer: Adjuvant chemotherapy prevents local recurrence rather than distant metastases. Ann. Oncol. 2009, 21, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- Hwang, M.; Lee, S.W.; Park, K.C.; Sul, H.J.; Kwon, D.S. Evaluation of a robotic arm-assisted endoscope to facilitate endoscopic submucosal dissection (with video). Gastrointest. Endosc. 2020, 91, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Chiu, P.W.Y.; Ho, K.Y.; Phee, S.J. Colonic endoscopic submucosal dissection using a novel robotic system (with video). Gastrointest. Endosc. 2021, 93, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Mainenti, P.P.; Stanzione, A.; Guarino, S.; Romeo, V.; Ugga, L.; Romano, F.; Storto, G.; Maurea, S.; Brunetti, A. Colorectal cancer: Parametric evaluation of morphological, functional and molecular tomographic imaging. World J. Gastroenterol. 2019, 25, 5233–5256. [Google Scholar] [CrossRef]
- Hassan, C.; Spadaccini, M.; Iannone, A.; Maselli, R.; Jovani, M.; Chandrasekar, V.T.; Antonelli, G.; Yu, H.; Areia, M.; Dinis-Ribeiro, M.; et al. Performance of artificial intelligence in colonoscopy for adenoma and polyp detection: A systematic review and meta-analysis. Gastrointest. Endosc. 2021, 93, 77–85.e6. [Google Scholar] [CrossRef] [PubMed]
- Barua, I.; Vinsard, D.G.; Jodal, H.C.; Løberg, M.; Kalager, M.; Holme, Ø.; Misawa, M.; Bretthauer, M.; Mori, Y. Artificial intelligence for polyp detection during colonoscopy: A systematic review and meta-analysis. Endoscopy 2021, 53, 277–284. [Google Scholar] [CrossRef]
- Keller, D.S.; Berho, M.; Perez, R.O.; Wexner, S.D.; Chand, M. The multidisciplinary management of rectal cancer. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 414–429. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| High Risk | Low Risk |
|---|---|
| Poor differentiation | Well and moderate differentiation |
| >1 mm (1000 mm) of SMI | <1 mm (1000 mm) of SMI |
| Presence of tumor budding | Absence of tumor budding |
| Presence of lymphovascular invasion | Absence of lymphovascular invasion |
| Large polyp size (≥2 cm) | |
| Depressed or sessile morphology in nongranular lateral spreading tumors (LST-NG) | |
| Discrete nodules in granular lateral spreading tumors (LST-G) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Ghamdi, S.S.; Leeds, I.; Fang, S.; Ngamruengphong, S. Minimally Invasive Endoscopic and Surgical Management of Rectal Neoplasia. Cancers 2022, 14, 948. https://doi.org/10.3390/cancers14040948
Al Ghamdi SS, Leeds I, Fang S, Ngamruengphong S. Minimally Invasive Endoscopic and Surgical Management of Rectal Neoplasia. Cancers. 2022; 14(4):948. https://doi.org/10.3390/cancers14040948
Chicago/Turabian StyleAl Ghamdi, Sarah S., Ira Leeds, Sandy Fang, and Saowanee Ngamruengphong. 2022. "Minimally Invasive Endoscopic and Surgical Management of Rectal Neoplasia" Cancers 14, no. 4: 948. https://doi.org/10.3390/cancers14040948
APA StyleAl Ghamdi, S. S., Leeds, I., Fang, S., & Ngamruengphong, S. (2022). Minimally Invasive Endoscopic and Surgical Management of Rectal Neoplasia. Cancers, 14(4), 948. https://doi.org/10.3390/cancers14040948