
Overweight and Obesity Determine the Risk for Gastrointestinal Cancer in a Sex-Dependent Manner: A Retrospective Cohort Study of 287,357 Outpatients in Germany

 ,
, 
 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Database
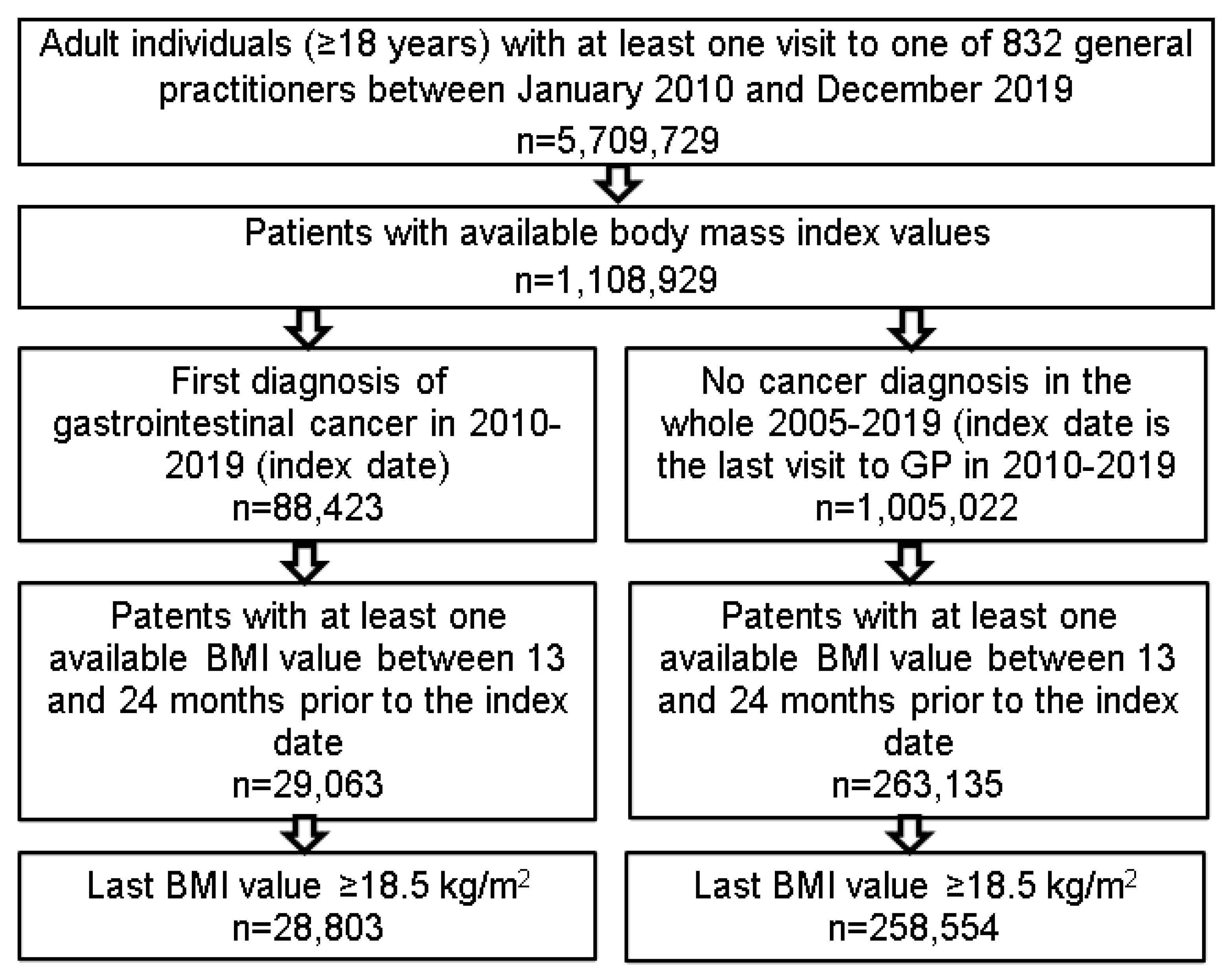
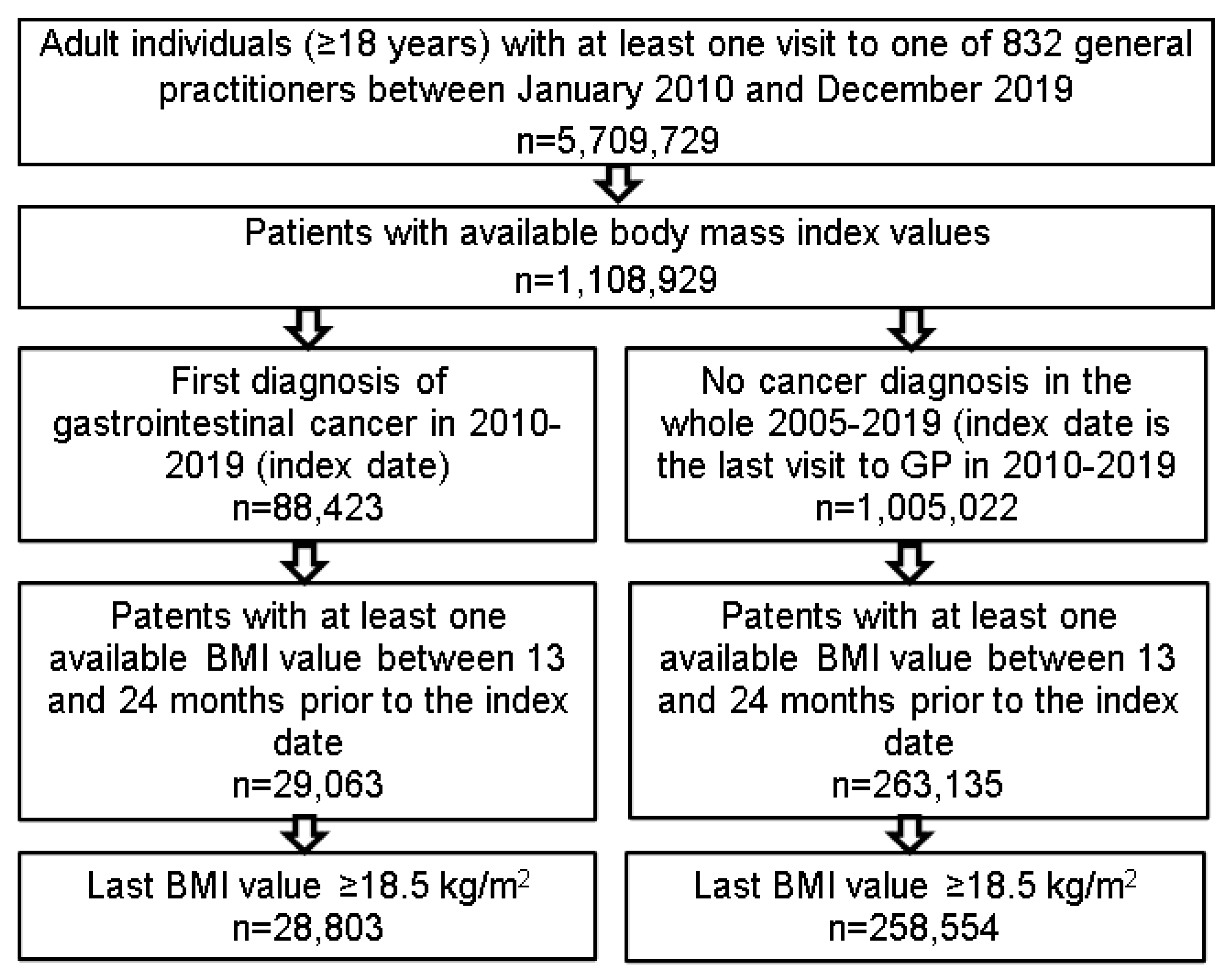
2.2. Study Population
2.3. Study Outcomes
2.4. Statistical Analyses
3. Results
3.1. Basic Characteristics of the Study Cohort
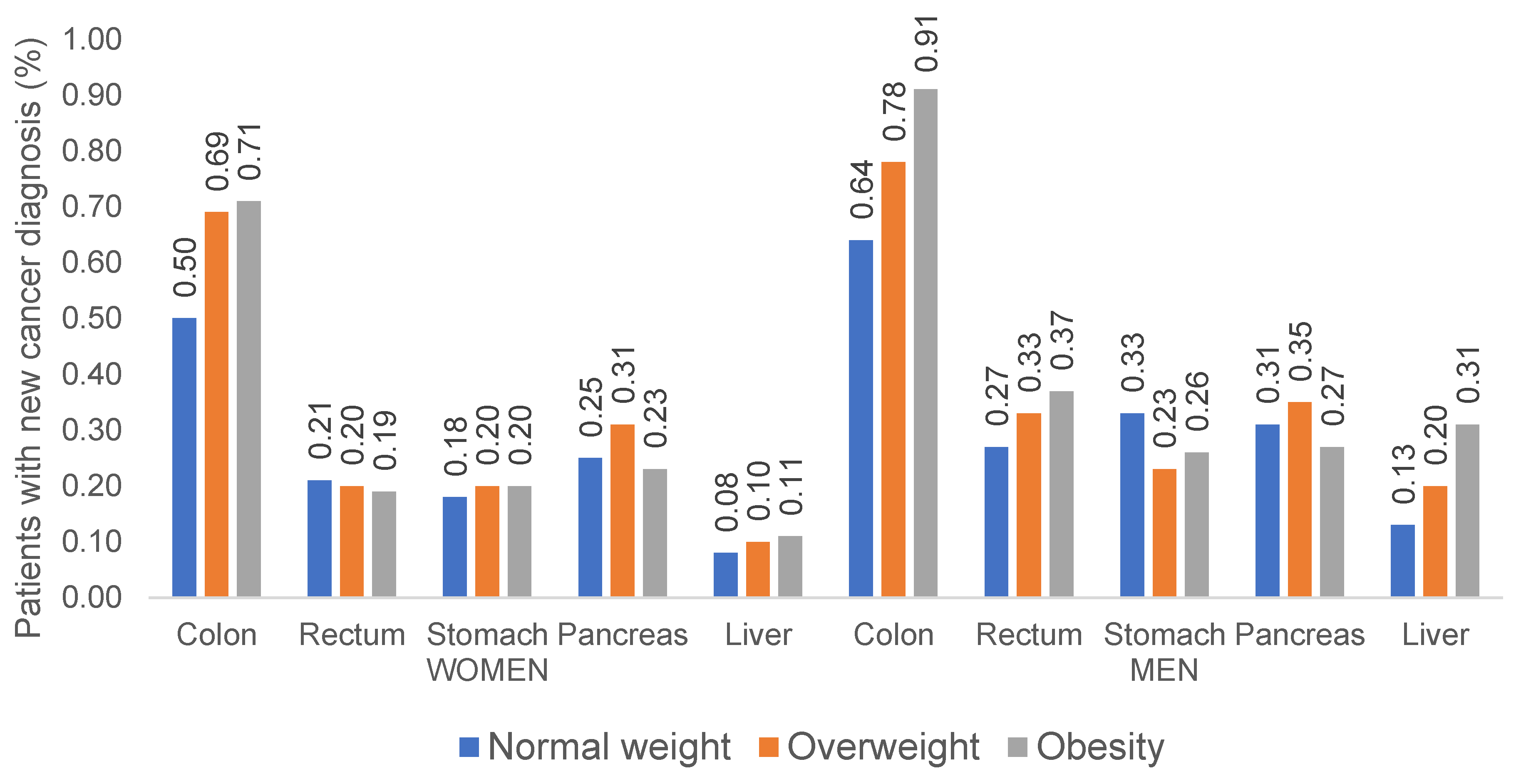
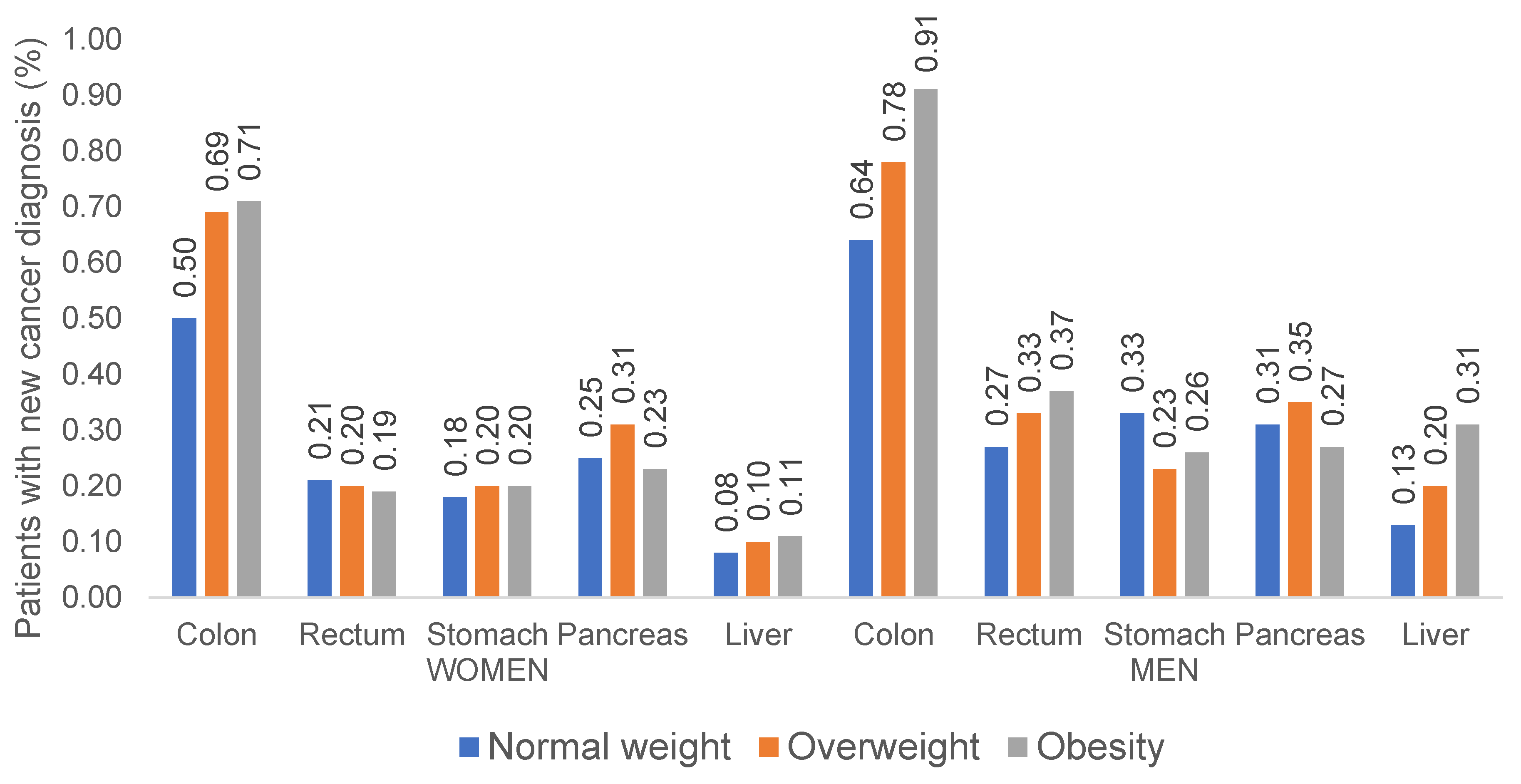
3.2. Incidence Rates of Gastrointestinal Cancers in Normal Weight, Pre-Obese and Obese Outpatients in Germany
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ghose, A.; Moschetta, M.; Pappas-Gogos, G.; Sheriff, M.; Boussios, S. Genetic Aberrations of Dna Repair Pathways in Prostate Cancer: Translation to the Clinic. Int. J. Mol. Sci. 2021, 22, 9783. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zhu, W.; Thompson, P.; Hannun, Y.A. Evaluating Intrinsic and Non-Intrinsic Cancer Risk Factors. Nat. Commun. 2018, 9, 3490. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Li, H. Obesity: Epidemiology, Pathophysiology, and Therapeutics. Front. Endocrinol. 2021, 12, 12. [Google Scholar] [CrossRef]
- Krupa-Kotara, K.; Dakowska, D. Impact of Obesity on Risk of Cancer. Cent. Eur. J. Public Health 2021, 29, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Ancellin, R.; Bessette, D. Overweight, Obesity and Cancer Risks. Oncologie 2013, 15, 193–201. [Google Scholar] [CrossRef]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [Green Version]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-Mass Index and Incidence of Cancer: A Systematic Review and Meta-Analysis of Prospective Observational Studies. Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, L.; Wang, X.; Wang, J.; Yan, Z.; Cheng, J.; Gong, G.; Li, G. Body Mass Index and Risk of Gastric Cancer:Ameta-Analysis of a Population with More than Ten Million from 24 Prospective Studies. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1395–1408. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Wang, X.; Wang, J.; Yan, Z.; Luo, J. Excess Body Weight and the Risk of Primary Liver Cancer: An Updated Meta-Analysis of Prospective Studies. Eur. J. Cancer 2012, 48, 2137–2145. [Google Scholar] [CrossRef]
- Genkinger, J.M.; Spiegelman, D.; Anderson, K.E.; Bernstein, L.; van den Brandt, P.A.; Calle, E.E.; English, D.R.; Folsom, A.R.; Freudenheim, J.L.; Fuchs, C.S.; et al. A Pooled Analysis of 14 Cohort Studies of Anthropometric Factors and Pancreatic Cancer Risk. Int. J. Cancer 2011, 129, 1708–1717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathmann, W.; Bongaerts, B.; Carius, H.J.; Kruppert, S.; Kostev, K. Basic Characteristics and Representativeness of the German Disease Analyzer Database. Int. J. Clin. Pharmacol. Ther. 2018, 56, 459–466. [Google Scholar] [CrossRef]
- Loosen, S.H.; Kostev, K.; Luedde, M.; Luedde, T.; Roderburg, C. Low Blood Levels of High-Density Lipoprotein (HDL) Cholesterol Are Positively Associated with Cancer. J. Cancer Res. Clin. Oncol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Loosen, S.H.; Kostev, K.; Keitel, V.; Tacke, F.; Roderburg, C.; Luedde, T. An Elevated FIB-4 Score Predicts Liver Cancer Development: A Longitudinal Analysis from 29,999 NAFLD Patients. J. Hepatol. 2021, 76, 247–248. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Spyrou, N.; Mantzoros, C.S.; Dalamaga, M. Obesity and Cancer Risk: Emerging Biological Mechanisms and Perspectives. Metab. Clin. Exp. 2019, 92, 121–135. [Google Scholar] [CrossRef]
- Islami, F.; Goding Sauer, A.; Miller, K.D.; Siegel, R.L.; Fedewa, S.A.; Jacobs, E.J.; McCullough, M.L.; Patel, A.V.; Ma, J.; Soerjomataram, I.; et al. Proportion and Number of Cancer Cases and Deaths Attributable to Potentially Modifiable Risk Factors in the United States. CA A Cancer J. Clin. 2018, 68, 31–54. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Lawless, M.W. Stop Feeding Cancer: Pro-Inflammatory Role of Visceral Adiposity in Liver Cancer. Cytokine 2013, 64, 626–637. [Google Scholar] [CrossRef]
- Pietrzyk, L.; Torres, A.; Maciejewski, R.; Torres, K. Obesity and Obese-Related Chronic Low-Grade Inflammation in Promotion of Colorectal Cancer Development. Asian Pac. J. Cancer Prev. 2015, 16, 4161–4168. [Google Scholar] [CrossRef] [Green Version]
- Dumas, J.F.; Brisson, L. Interaction between Adipose Tissue and Cancer Cells: Role for Cancer Progression. Cancer Metastasis Rev. 2021, 40, 31–46. [Google Scholar] [CrossRef]
- Revythis, A.; Shah, S.; Kutka, M.; Moschetta, M.; Ozturk, M.A.; Pappas-Gogos, G.; Ioannidou, E.; Sheriff, M.; Rassy, E.; Boussios, S. Unraveling the Wide Spectrum of Melanoma Biomarkers. Diagnostics 2021, 11, 1341. [Google Scholar] [CrossRef]
- Bhardwaj, P.; Brown, K.A. Obese Adipose Tissue as a Driver of Breast Cancer Growth and Development: Update and Emerging Evidence. Front. Oncol. 2021, 11, 11. [Google Scholar] [CrossRef]
- Rangel, N.; Villegas, V.E.; Rondón-Lagos, M. Obesity and Androgen Receptor Signaling: Associations and Potential Crosstalk in Breast Cancer Cells. Cancers 2021, 13, 2218. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.A. Metabolic Pathways in Obesity-Related Breast Cancer. Nat. Rev. Endocrinol. 2021, 17, 350–363. [Google Scholar] [CrossRef] [PubMed]
- Argyrakopoulou, G.; Dalamaga, M.; Spyrou, N.; Kokkinos, A. Gender Differences in Obesity-Related Cancers. Curr. Obes. Rep. 2021, 10, 100–115. [Google Scholar] [CrossRef] [PubMed]
- Kampman, E.; Potter, J.D.; Slattery, M.L.; Caan, B.J.; Edwards, S. Hormone Replacement Therapy, Reproductive History, and Colon Cancer: A Multicenter, Case-Control Study in the United States. Cancer Causes Control 1997, 8, 146–158. [Google Scholar] [CrossRef] [PubMed]
- Slattery, M.L.; Potter, J.D.; Curtin, K.; Edwards, S.; Ma, K.-N.; Anderson, K.; Schaffer, D.; Samowitz, W.S. Estrogens Reduce and Withdrawal of Estrogens Increase Risk of Microsatellite Instability-Positive Colon Cancer. Cancer Res. 2001, 61, 126–130. [Google Scholar]
- Yoon, K.; Kim, N. Roles of Sex Hormones and Gender in the Gut Microbiota. J. Neurogastroenterol. Motil. 2021, 27, 314–325. [Google Scholar] [CrossRef]
- Labenz, C.; Huber, Y.; Michel, M.; Nagel, M.; Galle, P.R.; Kostev, K.; Schattenberg, J.M. Nonalcoholic Fatty Liver Disease Increases the Risk of Anxiety and Depression. Hepatol. Commun. 2020, 4, 1293–1301. [Google Scholar] [CrossRef]
- Roderburg, C.; Loosen, S.H.; Hoyer, L.; Luedde, T.; Kostev, K. Prevalence of Diabetes Mellitus among 80,193 Gastrointestinal Cancer Patients in Five European and Three Asian Countries. J. Cancer Res. Clin. Oncol. 2021. [Google Scholar] [CrossRef]
- Huber, Y.; Labenz, C.; Michel, M.; Wörns, M.A.; Galle, P.R.; Kostev, K.; Schattenberg, J.M. Tumor Incidence in Patients with Non-Alcoholic Fatty Liver Disease. Dtsch. Arztebl. Int. 2020, 117, 719–724. [Google Scholar] [CrossRef]
- Jacob, L.; Loosen, S.H.; Kalder, M.; Luedde, T.; Roderburg, C.; Kostev, K. Impact of the COVID-19 Pandemic on Cancer Diagnoses in General and Specialized Practices in Germany. Cancers 2021, 13, 408. [Google Scholar] [CrossRef] [PubMed]
- Labenz, C.; Kostev, K.; Galle, P.R.; Wörns, M.-A.; Labenz, J.; Tanislav, C.; Adarkwah, C.C. Proton Pump Inhibitor Use Is Associated with a Variety of Infections in Patients with Liver Cirrhosis. Medicine 2020, 99, e23436. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | All Patients | Normal Weight | Overweight | Obesity | p Values |
|---|---|---|---|---|---|
| N | 287,357 | 84,339 | 109,917 | 93,101 | |
| Age (years) (mean, SD) | 57.9 (18.2) | 64.6 (15.7) | 64.0 (15.0) | <0.001 | |
| Age ≤50 (%) | 22.8 | 33.4 | 18.5 | 18.1 | <0.001 |
| Age 51–60 (%) | 22.1 | 23.1 | 21.6 | 21.8 | <0.001 |
| Age 61–70 (%) | 21.3 | 17.0 | 21.6 | 24.7 | <0.001 |
| Age >70 (%) | 33.8 | 26.5 | 38.2 | 35.4 | <0.001 |
| Males (%) | 48.2 | 37.2 | 55.9 | 49.1 | <0.001 |
| Co-Diagnoses (%): | |||||
| Diabetes mellitus | 32.5 | 14.6 | 30.3 | 51.2 | <0.001 |
| Thyroid gland disorders | 21.7 | 31.5 | 30.9 | 32.8 | <0.001 |
| Hypertension | 60.6 | 39.3 | 62.8 | 77.2 | <0.001 |
| Ischemic heart diseases | 19.3 | 12.2 | 21.2 | 23.4 | <0.001 |
| Heart failure | 11.6 | 6.7 | 11.5 | 16.3 | <0.001 |
| Lipid metabolism disorders | 44.0 | 33.2 | 47.6 | 49.6 | <0.001 |
| Chronic obstructive bronchitis or lung disease | 16.8 | 14.4 | 16.5 | 19.5 | <0.001 |
| Diseases of esophagus, stomach, and duodenum | 42.2 | 40.2 | 43.1 | 43.0 | <0.001 |
| Liver diseases | 15.8 | 9,5 | 16.0 | 21.1 | <0.001 |
| Depression | 26.8 | 26.7 | 25.8 | 28.2 | <0.001 |
| Odds Ratio (95% CI) + | |||||
|---|---|---|---|---|---|
| Colon (C18) | Rectum (C20) | Stomach (C16) | Pancreas (C25) | Liver (C22) | |
| Women | |||||
| Overweight | 1.11 (0.93–1.34) | 0.82 (0.61–1.12) | 0.91 (0.66–1.25) | 0.87 (0.66–1.14) | 0.85 (0.53–1.37) |
| Obesity | 1.23 (1.03–1.48) * | 0.83 (0.61–1.14) | 0.97 (0.71–1.34) | 0.61 (0.45–0.82) * | 0.83 (0.51–1.35) |
| Men | |||||
| Overweight | 1.12 (0.92–1.36) | 1.11 (0.82–1.50) | 0.65 (0.48–0.87) * | 1.01 (0.76–1.34) | 1.28 (0.84–1.95) |
| Obesity | 1.43 (1.17–1.74) * | 1.36 (1.01–1.84) * | 0.79 (0.58–1.06) | 0.77 (0.56–1.06) | 1.79 (1.17–2.73) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loosen, S.H.; Roderburg, C.; Jördens, M.S.; Fluegen, G.; Luedde, T.; Kostev, K. Overweight and Obesity Determine the Risk for Gastrointestinal Cancer in a Sex-Dependent Manner: A Retrospective Cohort Study of 287,357 Outpatients in Germany. Cancers 2022, 14, 931. https://doi.org/10.3390/cancers14040931
Loosen SH, Roderburg C, Jördens MS, Fluegen G, Luedde T, Kostev K. Overweight and Obesity Determine the Risk for Gastrointestinal Cancer in a Sex-Dependent Manner: A Retrospective Cohort Study of 287,357 Outpatients in Germany. Cancers. 2022; 14(4):931. https://doi.org/10.3390/cancers14040931
Chicago/Turabian StyleLoosen, Sven H., Christoph Roderburg, Markus S. Jördens, Georg Fluegen, Tom Luedde, and Karel Kostev. 2022. "Overweight and Obesity Determine the Risk for Gastrointestinal Cancer in a Sex-Dependent Manner: A Retrospective Cohort Study of 287,357 Outpatients in Germany" Cancers 14, no. 4: 931. https://doi.org/10.3390/cancers14040931
APA StyleLoosen, S. H., Roderburg, C., Jördens, M. S., Fluegen, G., Luedde, T., & Kostev, K. (2022). Overweight and Obesity Determine the Risk for Gastrointestinal Cancer in a Sex-Dependent Manner: A Retrospective Cohort Study of 287,357 Outpatients in Germany. Cancers, 14(4), 931. https://doi.org/10.3390/cancers14040931