
Quality of Life in the First Year of Follow-Up in a Randomized Multicenter Trial Assessing the Role of Imaging after Radical Surgery of Stage IIB-C and III Cutaneous Melanoma (TRIM Study)

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Quality of Life Related Assessments and Instruments
2.3. Statistics
3. Results
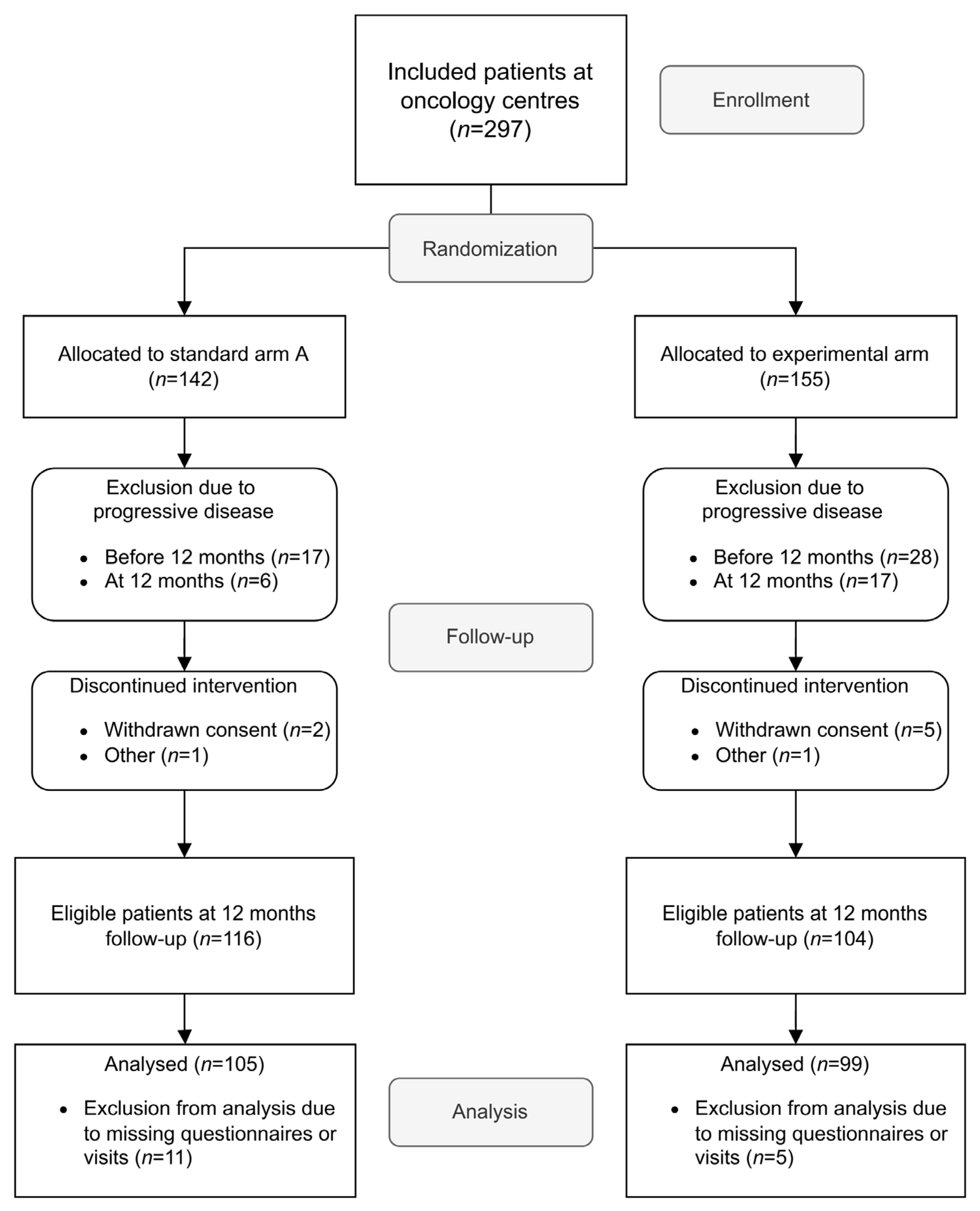
3.1. Characteristics of Included Patients
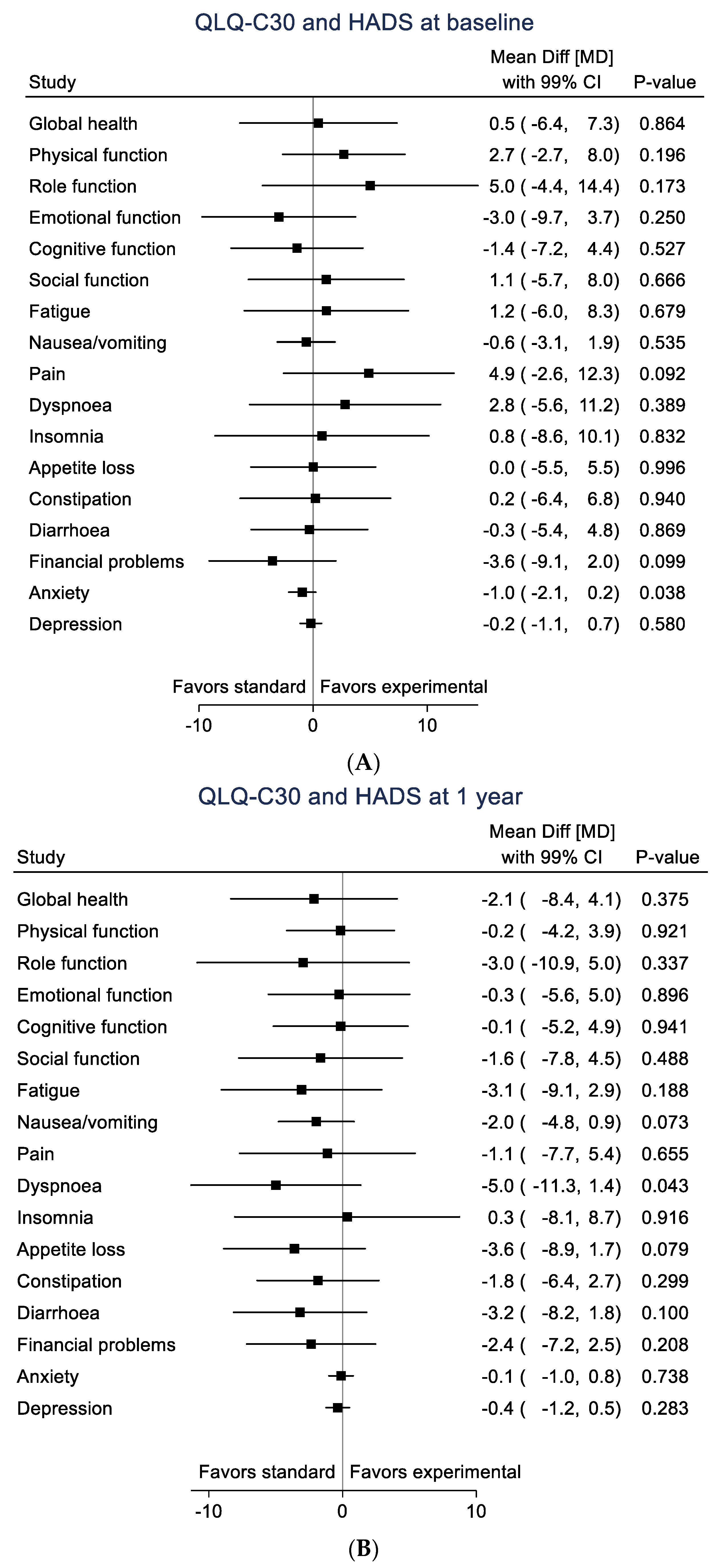
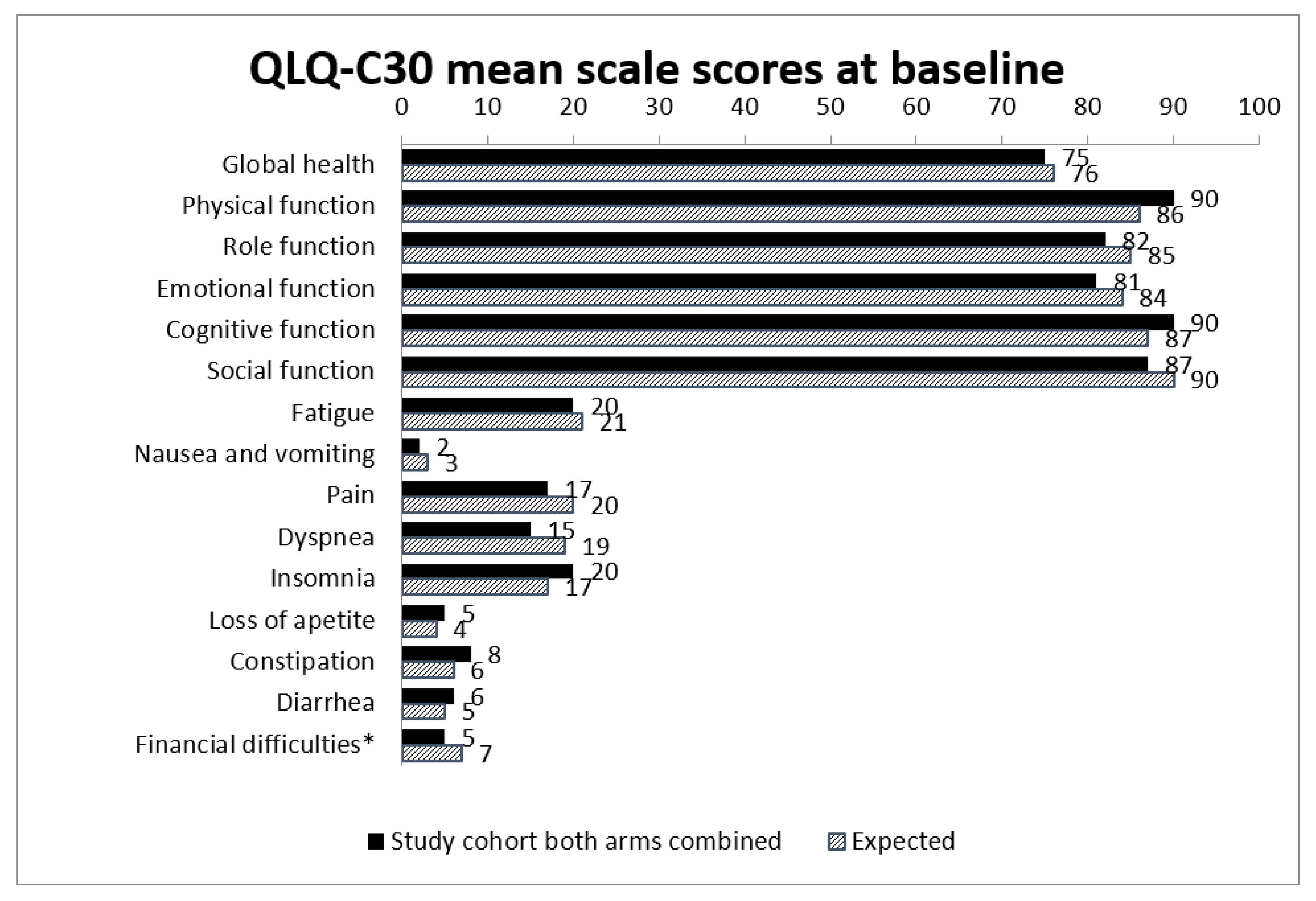
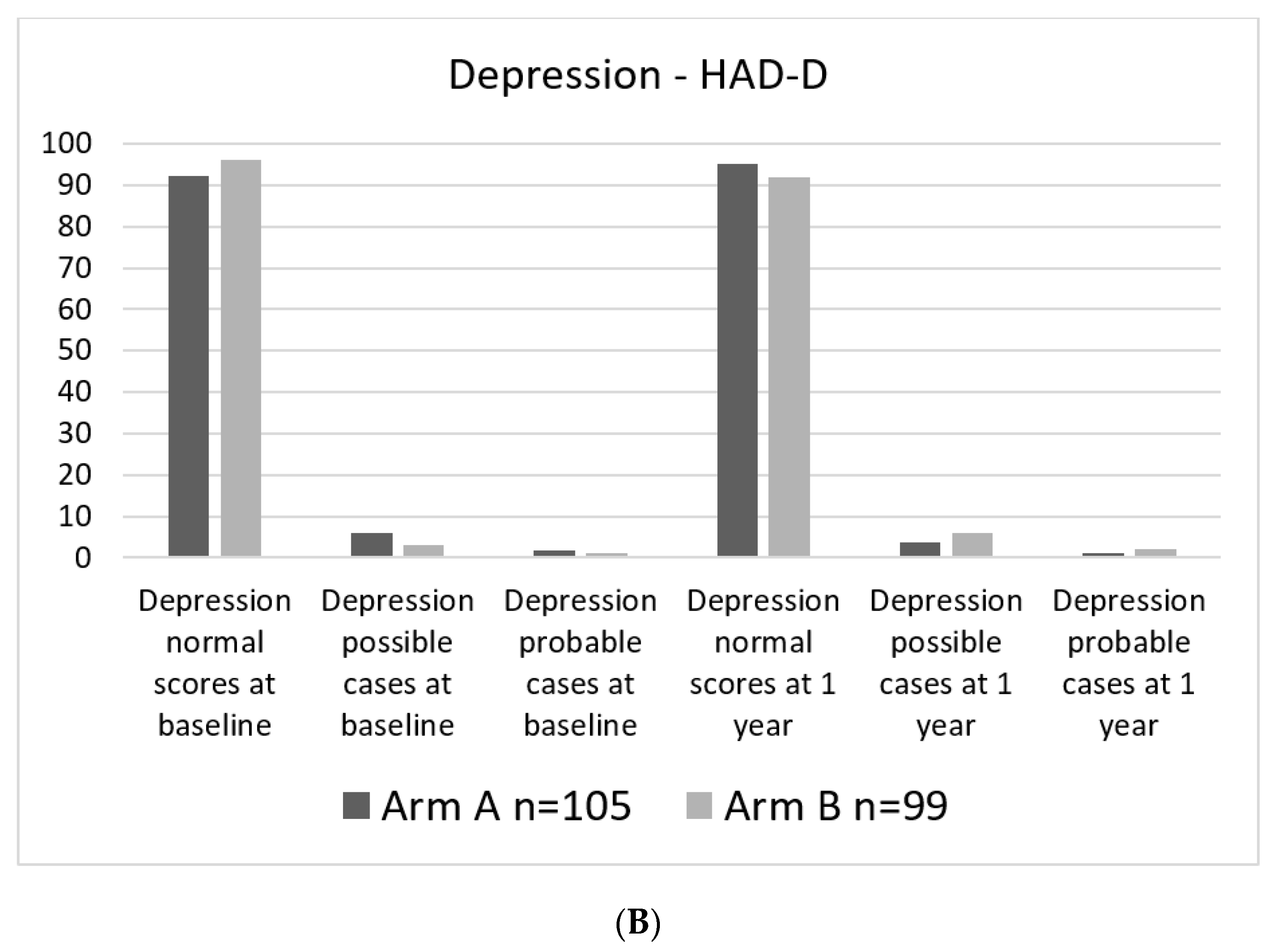
3.2. Health Related Quality of Life (HRQoL) and Anxiety/Depressive Symptoms
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pavri, S.N.; Clune, J.; Ariyan, S.; Narayan, D. Malignant melanoma: Beyond the basics. Plast. Reconstr. Surg. 2016, 138, 330e–340e. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, J.; Beasley, G.M.; Agnese, D.; Kendra, K.; Olencki, T.E.; Terando, A.; Howard, J.H. Surveillance strategies in the follow-up of melanoma patients: Too much or not enough? J. Surg. Res. 2017, 214, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Lewin, J.; Sayers, L.; Kee, D.; Walpole, I.; Sanelli, A.; Te Marvelde, L.; Herschtal, A.; Spillane, J.; Gyorki, D.; Speakman, D.; et al. Surveillance imaging with FDG-PET/CT in the post-operative follow-up of stage 3 melanoma. Ann. Oncol. 2018, 29, 1569–1574. [Google Scholar] [CrossRef] [PubMed]
- Podlipnik, S.; Carrera, C.; Sanchez, M.; Arguis, P.; Olondo, M.L.; Vilana, R.; Rull, R.; Vidal-Sicart, S.; Vilalta, A.; Conill, C.; et al. Performance of diagnostic tests in an intensive follow-up protocol for patients with American Joint Committee on Cancer (AJCC) stage IIB, IIC, and III localized primary melanoma: A prospective cohort study. J. Am. Acad. Dermatol. 2016, 75, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, G.V.; Eroglu, Z.; Infante, J.; Patel, S.; Daud, A.; Johnson, D.B.; Gonzalez, R.; Kefford, R.; Hamid, O.; Schuchter, L.; et al. Long-term outcomes in patients with BRAF V600–mutant metastatic melanoma who received dabrafenib combined with trametinib. J. Clin. Oncol. 2018, 36, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbour, A.; Guminski, A.; Liu, W.; Menzies, S.; Morton, R.; Cancer Council Australia Melanoma Guidelines Working Party. Clinical question: How should patients at each stage of melanoma be followed after initial definitive treatment? In Clinical Practice Guidelines for the Diagnosis and Management of Melanoma; Melanoma Institute: Sydney, Australia, 2018; Available online: https://wiki.cancer.org.au/australia/Guidelines:Melanoma (accessed on 11 November 2021).
- NICE Guideline Melanoma: Assessment and Management [NG14]. Available online: www.nice.org/uk/guidance/ (accessed on 10 November 2021).
- Opfølgningsprogram for Modermærkekræft/Melanom. Available online: https://www.sst.dk/da/udgivelser/2015/opfoelgningsprogram-for-melanom (accessed on 11 November 2021).
- Helvind, N.M.; Aros Mardones, C.A.; Holmich, L.R.; Hendel, H.W.; Bidstrup, P.E.; Sorensen, J.A.; Chakera, A.H. Routine PET-CT scans provide early and accurate recurrence detection in asymptomatic stage IIB-III melanoma patients. Eur. J. Surg. Oncol. 2021, 47, 3020–3037. [Google Scholar] [CrossRef] [PubMed]
- Nationellt Vårdprogram Malignt Melanom. Available online: https://kunskapsbanken.cancercentrum.se/diagnoser/hudmelanom/vardprogram/ (accessed on 11 November 2021).
- Nijhuis, A.A.G.; Dieng, M.; Khanna, N.; Lord, S.J.; Dalton, J.; Menzies, A.M.; Turner, R.M.; Allen, J.; Saw, R.P.M.; Nieweg, O.E.; et al. False-positive results and incidental findings with annual CT or PET/CT surveillance in asymptomatic patients with resected stage III melanoma. Ann. Surg. Oncol. 2019, 26, 1860–1868. [Google Scholar] [CrossRef] [PubMed]
- Naeser, Y.; Helgadottir, H.; Brandberg, Y.; Hansson, J.; Bagge, R.O.; Elander, N.O.; Ingvar, C.; Isaksson, K.; Flygare, P.; Nilsson, C.; et al. TRIM study protocol—A prospective randomized multicenter Trial to assess the Role of Imaging during follow-up after radical surgery of stage IIB-C and III cutaneous malignant Melanoma. BMC Cancer 2020, 20, 1197. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Michelson, H.; Bolund, C.; Nilsson, B.; Brandberg, Y. Health-related quality of life measured by the EORTC QLQ-C30-reference values from a large sample of Swedish population. Acta Oncol. 2000, 39, 477–484. [Google Scholar] [PubMed]
- Brandberg, Y.B.C.; Sigurdardottir, V.; Sjödén, P.O.; Sullivan, M. Anxiety and depressive symptoms at different stages of malignant melanoma. Psycho-Oncol. 1992, 1, 71–78. [Google Scholar] [CrossRef]
- Fayers, P.M.A.N.; Bjordal, K.; Groenvold, M.; Curran, D.; Bottomley, A.; on behalf of the EORTC Quality of Life Group. The EORTC QLQ-C30 Scoring Manual, 3rd ed.; European Organisation for Research and Treatment of Cancer: Brussels, Belgium, 2001. [Google Scholar]
- Osoba, D.; Rodrigues, G.; Myles, J.; Zee, B.; Pater, J. Interpreting the significance of changes in health-related quality-of-life scores. J. Clin. Oncol. 1998, 16, 139–144. [Google Scholar] [CrossRef]
- Brandberg, Y.; Aamdal, S.; Bastholt, L.; Hernberg, M.; Stierner, U.; Von der Maase, H.; Hansson, J. Health-related quality of life in patients with high-risk melanoma randomised in the Nordic phase 3 trial with adjuvant intermediate-dose interferon alfa-2b. Eur. J. Cancer 2012, 48, 2012–2019. [Google Scholar] [CrossRef] [PubMed]
- Impact of follow-up testing on survival and health-related quality of life in breast cancer patients. A multicenter randomized controlled trial. The GIVIO Investigators. JAMA 1994, 271, 1587–1592. [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Standard Arm (n = 105) | Experimental Arm (n = 99) |
|---|---|---|
| Sex | ||
| Female | 43 (41%) | 36 (37%) |
| Male | 62 (59%) | 62 (63%) |
| Age median (IQR *) | 67 (56, 73) | 61 (50, 71) |
| Stage | ||
| IIB | 33 (31%) | 24 (24%) |
| IIC | 12 (11%) | 13 (13%) |
| IIIA | 16 (15%) | 15 (15%) |
| IIIB-C | 9 (9%) | 11 (11%) |
| IIIB-D (incl T0) | 31 (30%) | 32 (32%) |
| IINX or III (tx) | 4 (4%) | 4 (4%) |
| Lymph node dissection performed | 17 (16%) | 14 (14%) |
| Post-operative treatment | ||
| Radiotherapy | 0 (0%) | 3 (3%) |
| Systemic treatment | 23 (22%) | 19 (19%) |
| Subscale | Standard Arm Mean Value and (SD) | Experimental Arm Mean Value and (SD) |
|---|---|---|
| Global health (QL) | 79 (20) | 77 (19) |
| Physical function (PF) | 89 (17) | 91 (13) |
| Role function (RF) | 88 (22) | 86 (25) |
| Emotional function (EF) | 87 (15) | 85 (19) |
| Cognitive function (CF) | 89 (15) | 88 (16) |
| Social function (SF) | 91 (18) | 89 (18) |
| Fatigue (FA) | 18 (20) | 20 (21) |
| Nausea and vomiting (NV) | 1.4 (5.2) | 3.7 (11) |
| Pain (PA) | 15 (24) | 13 (19) |
| Dyspnea (DY) | 15 (23) | 18 (24) |
| Insomnia (SL) | 20 (27) | 20 (29) |
| Loss of appetite (AP) | 2.5 (11) | 6.1 (19) |
| Constipation (CO) | 6.7 (16) | 8.4 (17) |
| Diarrhea (DI) | 4.8 (12) | 8.1 (18) |
| Financial difficulties related to disease (FI) | 2.5 (11) | 6.7 (19) |
| Anxiety (HAD-A) | 3.1 (2.9) | 3.9 (3.6) |
| Depression (HAD-D) | 2.5 (2.7) | 3.0 (2.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naeser, Y.; Helgadottir, H.; Hansson, J.; Ingvar, C.; Elander, N.O.; Flygare, P.; Nilsson, C.; Jakobsson, F.; Valachis, A.; Papantoniou, D.; et al. Quality of Life in the First Year of Follow-Up in a Randomized Multicenter Trial Assessing the Role of Imaging after Radical Surgery of Stage IIB-C and III Cutaneous Melanoma (TRIM Study). Cancers 2022, 14, 1040. https://doi.org/10.3390/cancers14041040
Naeser Y, Helgadottir H, Hansson J, Ingvar C, Elander NO, Flygare P, Nilsson C, Jakobsson F, Valachis A, Papantoniou D, et al. Quality of Life in the First Year of Follow-Up in a Randomized Multicenter Trial Assessing the Role of Imaging after Radical Surgery of Stage IIB-C and III Cutaneous Melanoma (TRIM Study). Cancers. 2022; 14(4):1040. https://doi.org/10.3390/cancers14041040
Chicago/Turabian StyleNaeser, Ylva, Hildur Helgadottir, Johan Hansson, Christian Ingvar, Nils O. Elander, Petra Flygare, Cecilia Nilsson, Frida Jakobsson, Antonios Valachis, Dimitrios Papantoniou, and et al. 2022. "Quality of Life in the First Year of Follow-Up in a Randomized Multicenter Trial Assessing the Role of Imaging after Radical Surgery of Stage IIB-C and III Cutaneous Melanoma (TRIM Study)" Cancers 14, no. 4: 1040. https://doi.org/10.3390/cancers14041040
APA StyleNaeser, Y., Helgadottir, H., Hansson, J., Ingvar, C., Elander, N. O., Flygare, P., Nilsson, C., Jakobsson, F., Valachis, A., Papantoniou, D., Nordin Danfors, A., Johansson, H., Sundin, A., Brandberg, Y., & Ullenhag, G. J. (2022). Quality of Life in the First Year of Follow-Up in a Randomized Multicenter Trial Assessing the Role of Imaging after Radical Surgery of Stage IIB-C and III Cutaneous Melanoma (TRIM Study). Cancers, 14(4), 1040. https://doi.org/10.3390/cancers14041040