
Systematic Review with Meta-Analysis: Comparison of the Risk of Hepatocellular Carcinoma in Antiviral-Naive Chronic Hepatitis B Patients Treated with Entecavir versus Tenofovir: The Devil in the Detail


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
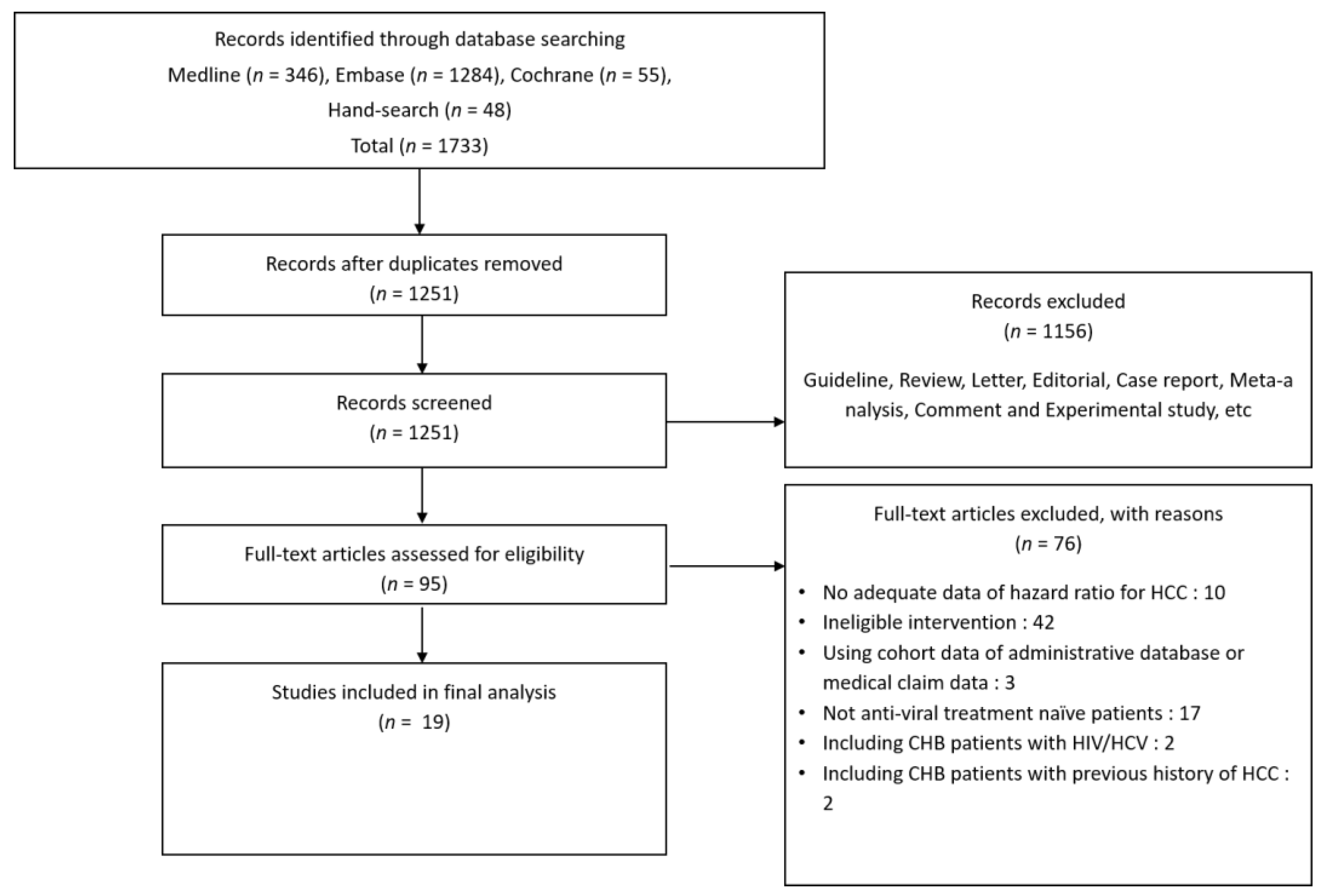
2.1. Data and Literature Source
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Assessment of Methodological Quality
2.5. Statistical Analysis
3. Results
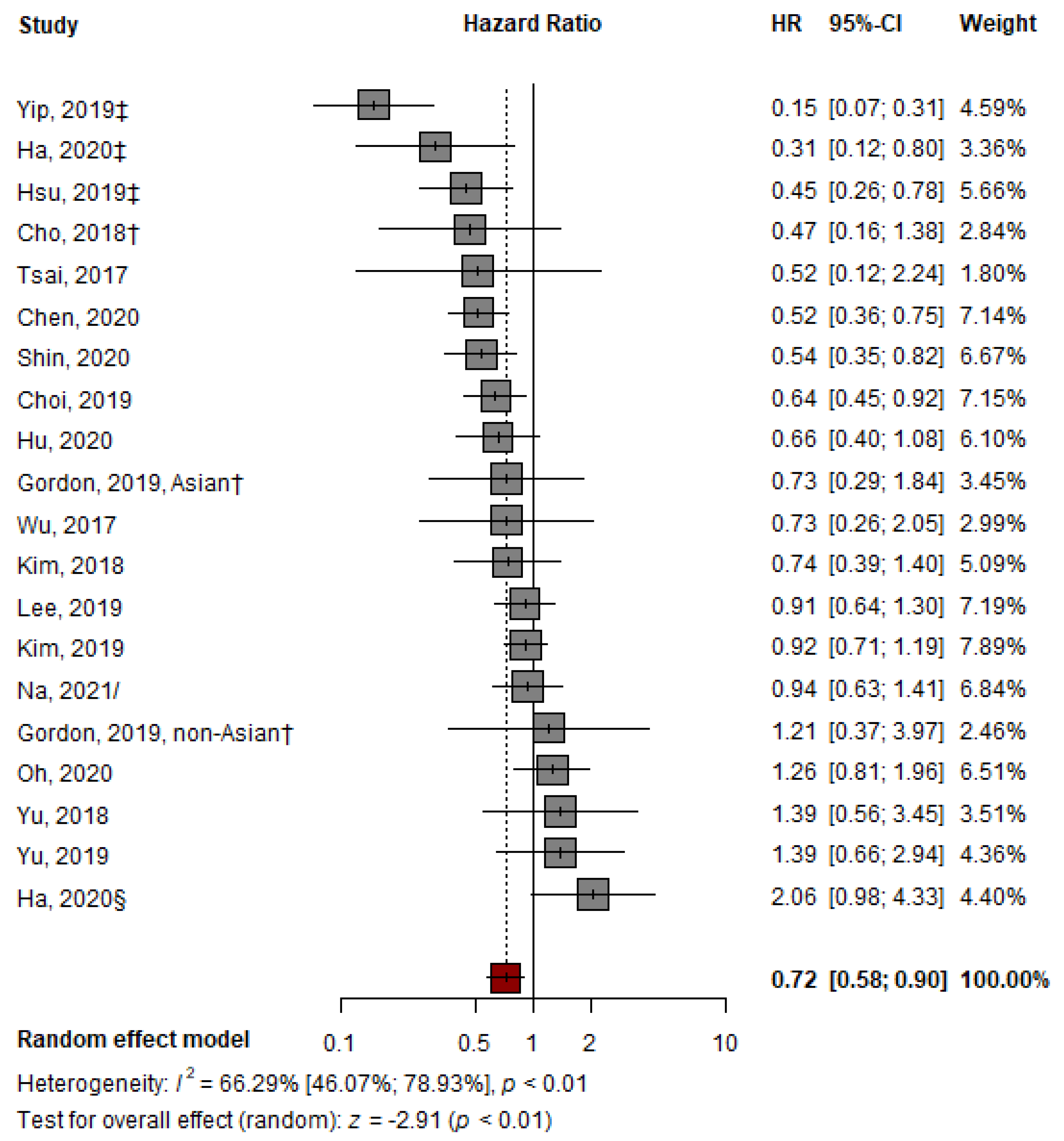
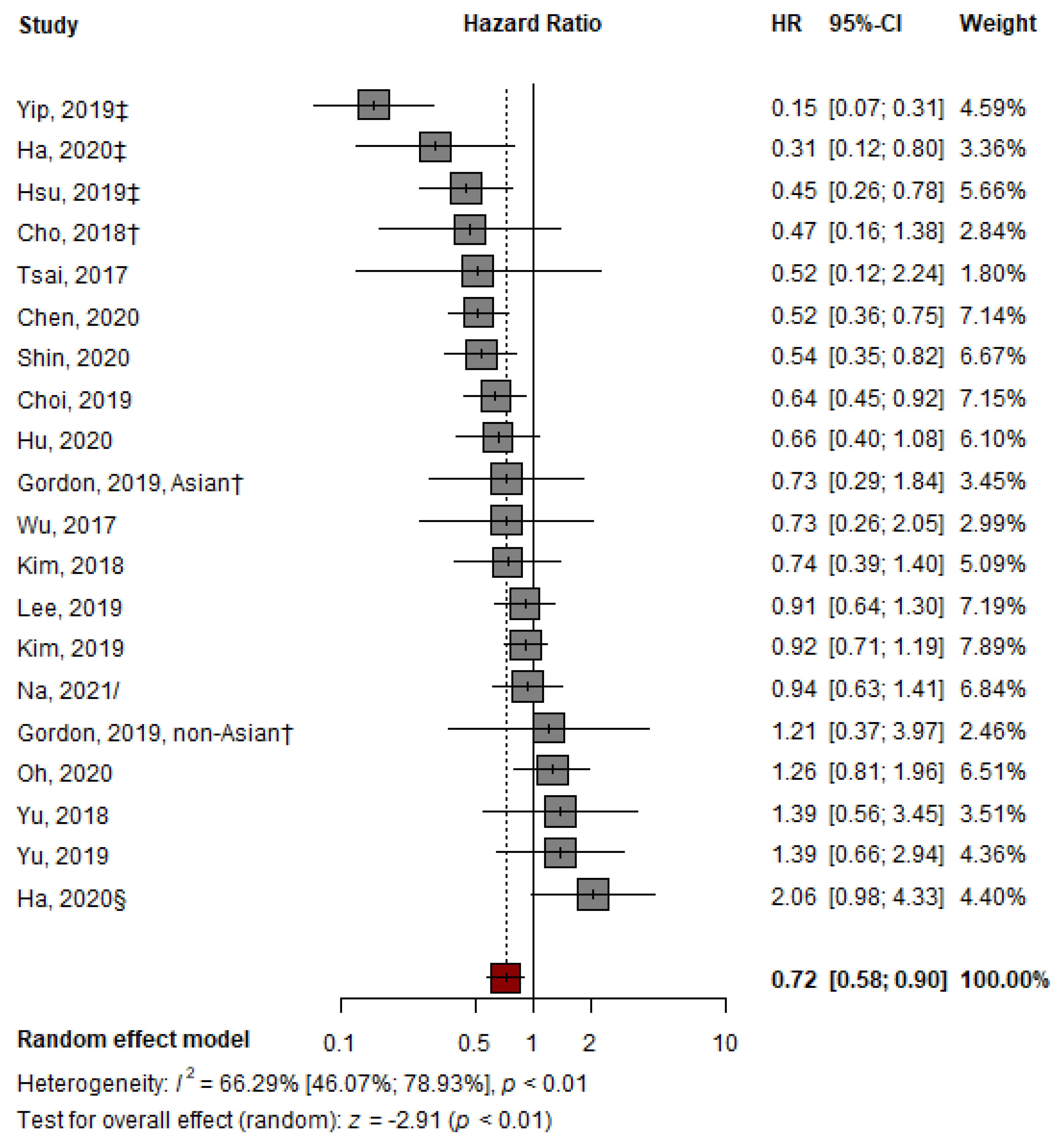
3.1. Pooled Analysis of Representative HRs Presented in Individual Papers
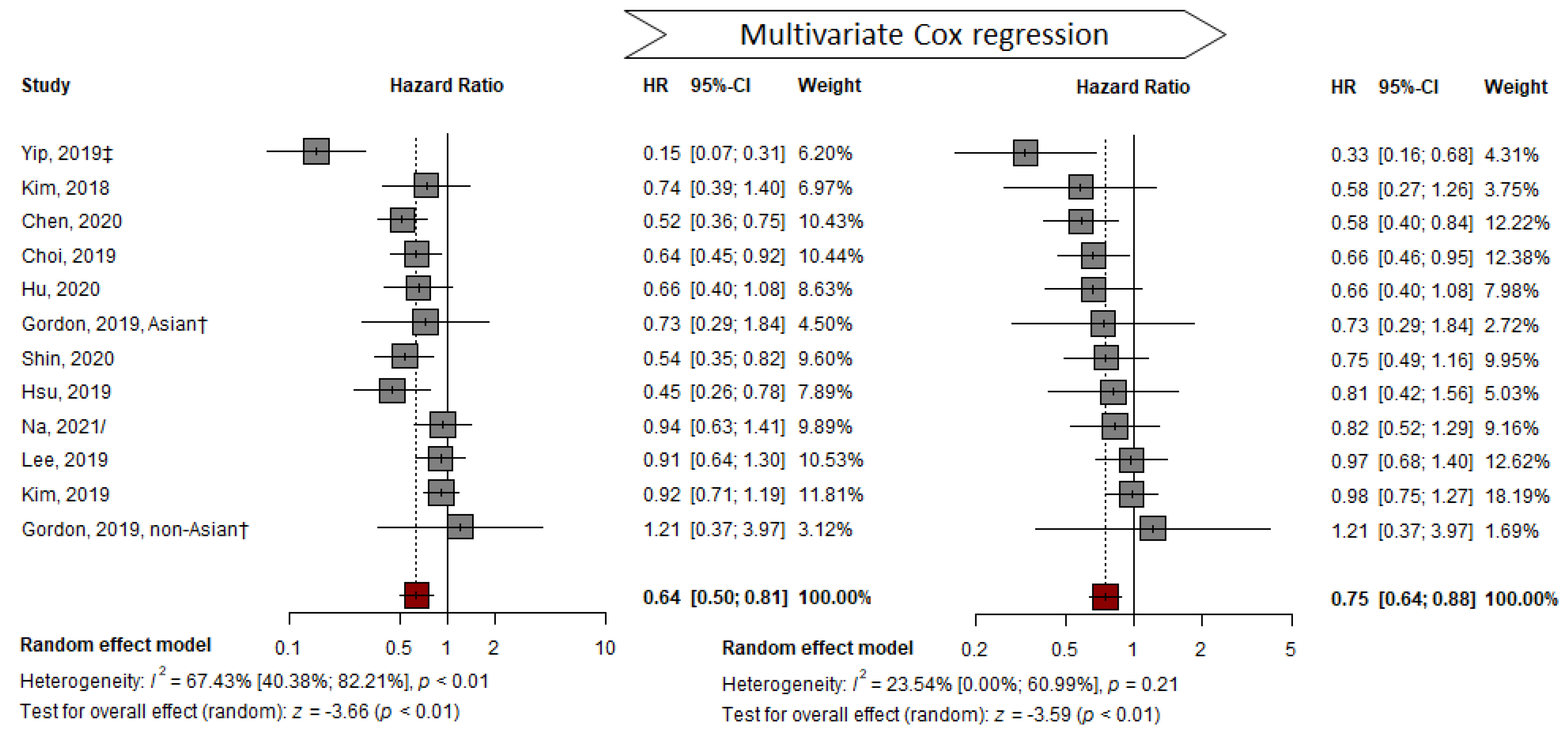
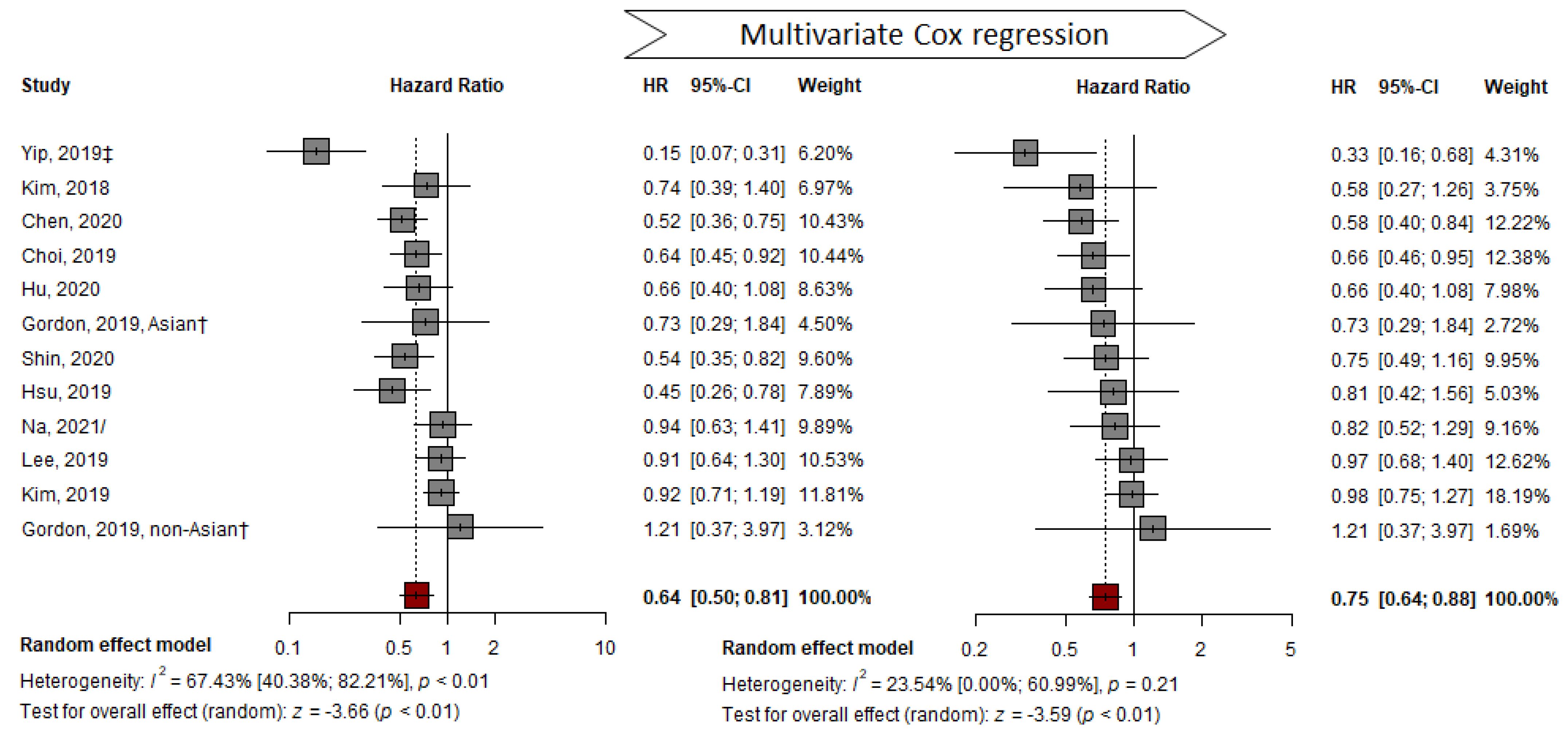
3.2. Adjusted HR by Multivariable Analysis
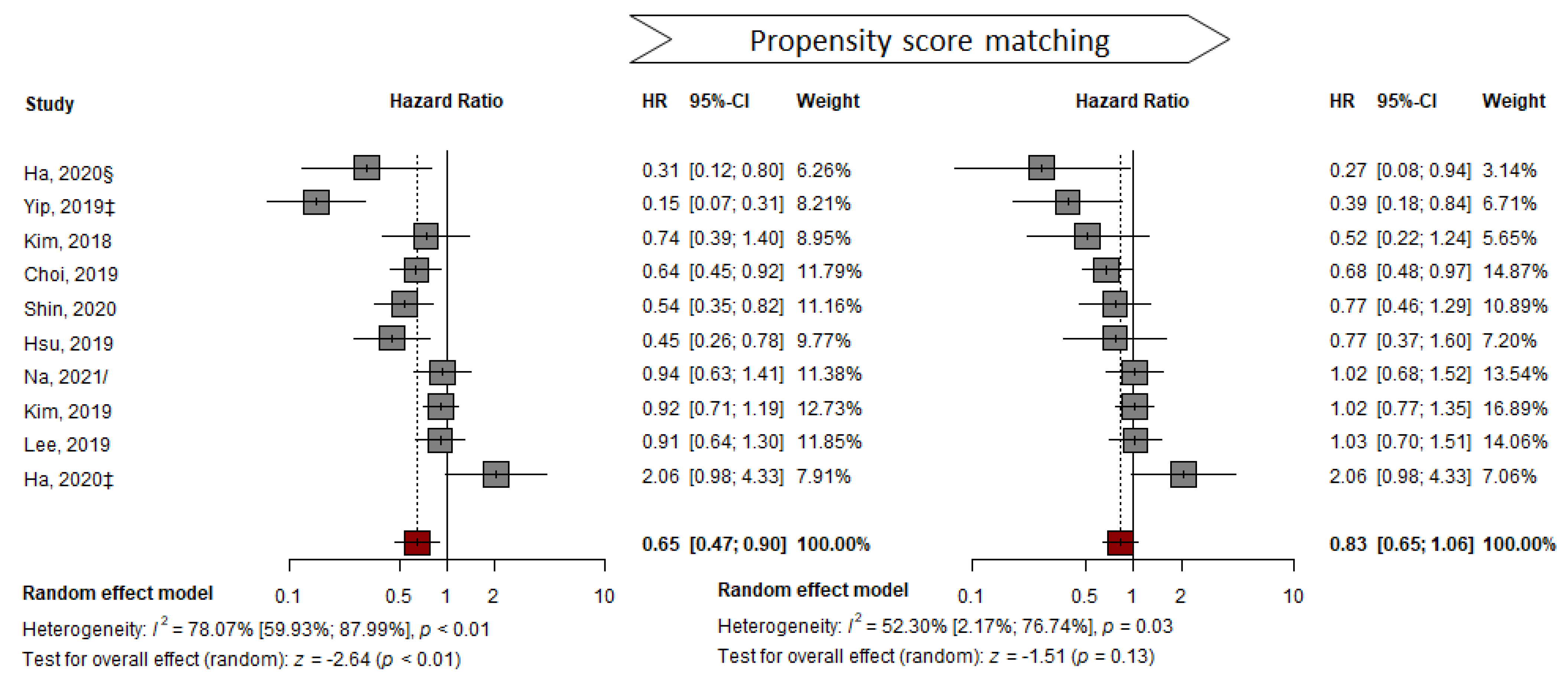
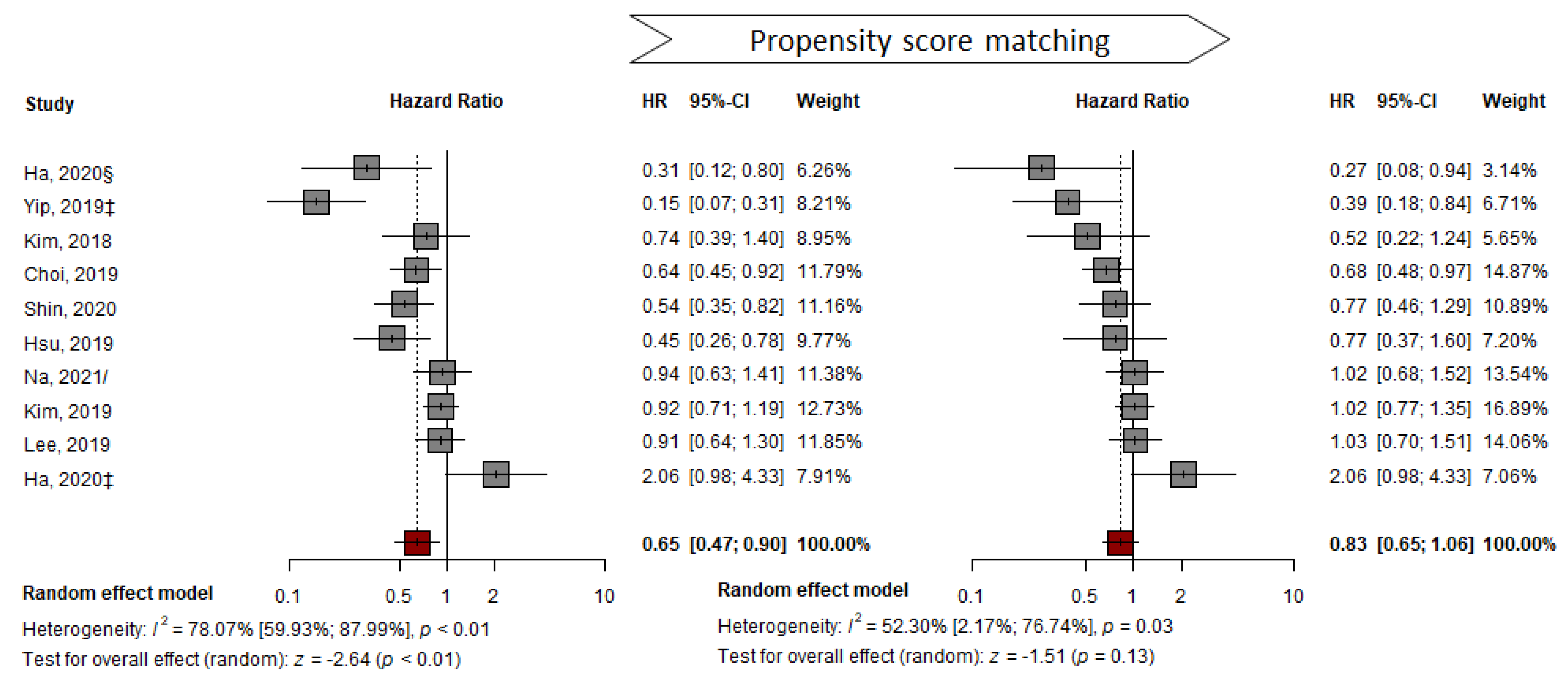
3.3. PS-Matched Population
3.4. Cirrhotic Subcohort
3.5. Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Hepatitis B. 27 July 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 18 April 2021).
- Hui, V.W.; Chan, S.L.; Wong, V.W.; Liang, L.Y.; Yip, T.C.; Lai, J.C.; Yuen, B.W.; Luk, H.W.; Tse, Y.K.; Lee, H.W.; et al. Increasing antiviral treatment uptake improves survival in patients with HBV-related HCC. JHEP Rep. 2020, 2, 100152. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.U.; Seo, Y.S.; Lee, H.A.; Kim, M.N.; Lee, E.J.; Shin, H.J.; Lee, Y.R.; Lee, H.W.; Park, J.Y.; Kim, D.Y.; et al. Hepatocellular Carcinoma Risk Steadily Persists over Time Despite Long-Term Antiviral Therapy for Hepatitis B: A Multicenter Study. Cancer Epidemiol. Biomark. Prev. 2020, 29, 832–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.L.; Kim, G.A.; Park, J.A.; Kang, H.R.; Lee, E.K.; Lim, Y.S. Cost-effectiveness of antiviral treatment in adult patients with immune-tolerant phase chronic hepatitis B. Gut 2020, 70, 2172–2182. [Google Scholar] [CrossRef] [PubMed]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef] [PubMed]
- EASL. 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.; Kim, H.J.; Lee, J.; Cho, S.; Ko, M.J.; Lim, Y.S. Risk of Hepatocellular Carcinoma in Patients Treated with Entecavir vs. Tenofovir for Chronic Hepatitis B: A Korean Nationwide Cohort Study. JAMA Oncol. 2019, 5, 30–36. [Google Scholar] [CrossRef] [Green Version]
- Yuan, J.; Peng, Y.; Hao, F.B.; Wang, Y.Q.; Wang, C.R.; Zhong, G.C. No difference in hepatocellular carcinoma risk in chronic hepatitis B patients treated with tenofovir vs. entecavir: Evidence from an updated meta-analysis. Aging 2021, 13, 7147–7165. [Google Scholar] [CrossRef]
- Dave, S.; Park, S.; Murad, M.H.; Barnard, A.; Prokop, L.; Adams, L.A.; Singh, S.; Loomba, R. Comparative Effectiveness of Entecavir Versus Tenofovir for Preventing Hepatocellular Carcinoma in Patients with Chronic Hepatitis B: A Systematic Review and Meta-Analysis. Hepatology 2021, 73, 68–78. [Google Scholar] [CrossRef]
- Choi, W.M.; Choi, J.; Lim, Y.S. Effects of Tenofovir vs. Entecavir on Risk of Hepatocellular Carcinoma in Patients with Chronic HBV Infection: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2021, 19, 246–258.e9. [Google Scholar] [CrossRef]
- Xia, Z.; He, L.; Xiong, L.; Wen, T. The comparison of different antiviral therapies on the prognosis of hepatitis B virus-related hepatocellular carcinoma after curative treatments: A network meta-analysis. Medicine 2020, 99, e20877. [Google Scholar] [CrossRef]
- Wang, X.; Liu, X.; Dang, Z.; Yu, L.; Jiang, Y.; Wang, X.; Yan, Z. Nucleos(t)ide Analogues for Reducing Hepatocellular Carcinoma in Chronic Hepatitis B Patients: A Systematic Review and Meta-Analysis. Gut Liver 2020, 14, 232–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tseng, C.-H.; Hsu, Y.-C.; Chen, T.-H.; Ji, F.; Chen, I.S.; Tsai, Y.-N.; Hai, H.; Thuy, L.T.T.; Hosaka, T.; Sezaki, H.; et al. Hepatocellular carcinoma incidence with tenofovir versus entecavir in chronic hepatitis B: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2020, 5, 1039–1052. [Google Scholar] [CrossRef]
- Teng, Y.X.; Li, M.J.; Xiang, B.D.; Zhong, J.H. Tenofovir may be superior to entecavir for preventing hepatocellular carcinoma and mortality in individuals chronically infected with HBV: A meta-analysis. Gut 2020, 69, 1900–1902. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Shi, Y.; Hayden, J.C.; Ryan, P.M.; Rahmani, J.; Yu, G. Tenofovir Treatment Has Lower Risk of Hepatocellular Carcinoma than Entecavir Treatment in Patients with Chronic Hepatitis B: A Systematic Review and Meta-Analysis. Liver Cancer 2020, 9, 468–476. [Google Scholar] [CrossRef]
- Li, M.; Lv, T.; Wu, S.; Wei, W.; Wu, X.; Ou, X.; Ma, H.; Chow, S.C.; Kong, Y.; You, H.; et al. Tenofovir versus entecavir in lowering the risk of hepatocellular carcinoma development in patients with chronic hepatitis B: A critical systematic review and meta-analysis. Hepatol. Int. 2020, 14, 105–114. [Google Scholar] [CrossRef]
- Gu, L.; Yao, Q.; Shen, Z.; He, Y.; Ng, D.M.; Yang, T.; Chen, B.; Chen, P.; Mao, F.; Yu, Q. Comparison of tenofovir versus entecavir on reducing incidence of hepatocellular carcinoma in chronic hepatitis B patients: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2020, 35, 1467–1476. [Google Scholar] [CrossRef]
- Cheung, K.S.; Mak, L.Y.; Liu, S.H.; Cheng, H.M.; Seto, W.K.; Yuen, M.F.; Lai, C.L. Entecavir vs. Tenofovir in Hepatocellular Carcinoma Prevention in Chronic Hepatitis B Infection: A Systematic Review and Meta-Analysis. Clin. Transl. Gastroenterol. 2020, 11, e00236. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhou, Y.; Yang, J.; Hu, K.; Huang, Y. The effectiveness of TDF versus ETV on incidence of HCC in CHB patients: A meta analysis. BMC Cancer 2019, 19, 511. [Google Scholar] [CrossRef] [Green Version]
- Jeong, S.; Cho, Y.; Park, S.M.; Kim, W. Differential Effectiveness of Tenofovir and Entecavir for Prophylaxis of Hepatocellular Carcinoma in Chronic Hepatitis B Patients Depending on Coexisting Cirrhosis and Prior Exposure to Antiviral Therapy: A Systematic Review and Meta-analysis. J. Clin. Gastroenterol. 2021, 55, e77–e86. [Google Scholar] [CrossRef]
- Kunz, L.M.; Normand, S.L.; Sedrakyan, A. Meta-analysis of rate ratios with differential follow-up by treatment arm: Inferring comparative effectiveness of medical devices. Stat. Med. 2015, 34, 2913–2925. [Google Scholar] [CrossRef] [Green Version]
- Choi, W.M.; Yip, T.C.; Lim, Y.S.; Wong, G.L.; Kim, W.R. Methodological challenges of performing meta-analyses to compare the risk of hepatocellular carcinoma between chronic hepatitis B treatments. J. Hepatol. 2022, 76, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Gordon, S.C.; Zhou, Y.; Li, J.; Rupp, L.B.; Boscarino, J.A.; Daida, Y.G.; Schmidt, M.A.; Trudeau, S.; Lu, M. Effect of treatment of hepatitis B patients with tenofovir disoproxil or entecavir on risk of hepatocellular cancer death in a U.S. Cohort. J. Hepatol. 2019, 70, e147. [Google Scholar] [CrossRef]
- Kim, B.G.; Park, N.H.; Lee, S.B.; Lee, H.; Lee, B.U.; Park, J.H.; Jung, S.W.; Jeong, I.D.; Bang, S.J.; Shin, J.W. Mortality, liver transplantation and hepatic complications in patients with treatment-naïve chronic hepatitis B treated with entecavir vs. tenofovir. J. Viral Hepat. 2018, 25, 1565–1575. [Google Scholar] [CrossRef]
- Shin, J.W.; Jeong, J.; Jung, S.W.; Lee, S.B.; Park, B.R.; Kim, M.-J.; Park, E.J.; Park, N.H. Comparable Incidence of Hepatocellular Carcinoma in Chronic Hepatitis B Patients Treated with Entecavir or Tenofovir. Dig. Dis. Sci. 2020, 66, 1739–1750. [Google Scholar] [CrossRef]
- Kim, S.U.; Seo, Y.S.; Lee, H.A.; Kim, M.N.; Lee, Y.R.; Lee, H.W.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Han, K.H.; et al. A multicenter study of entecavir vs. tenofovir on prognosis of treatment-naïve chronic hepatitis B in South Korea. J. Hepatol. 2019, 71, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Kwon, J.H.; Lee, H.L.; Yoo, S.H.; Nam, H.C.; Sung, P.S.; Nam, S.W.; Bae, S.H.; Choi, J.Y.; Yoon, S.K.; et al. Comparison of tenofovir and entecavir on the risk of hepatocellular carcinoma and mortality in treatment-naïve patients with chronic hepatitis B in Korea: A large-scale, propensity score analysis. Gut 2020, 69, 1301–1308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, M.C.; Chen, C.H.; Hu, T.H.; Lu, S.N.; Lee, C.M.; Wang, J.H.; Hung, C.H. Long-term outcomes of hepatitis B virus-related cirrhosis treated with nucleos(t)ide analogs. J. Formos. Med. Assoc. 2017, 116, 512–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yip, T.C.; Wong, V.W.; Chan, H.L.; Tse, Y.K.; Lui, G.C.; Wong, G.L. Tenofovir Is Associated with Lower Risk of Hepatocellular Carcinoma Than Entecavir in Patients with Chronic HBV Infection in China. Gastroenterology 2020, 158, 215–225.e216. [Google Scholar] [CrossRef]
- Yu, J.H.; Jin, Y.J.; Lee, J.W.; Lee, D.H. Remaining hepatocellular carcinoma risk in chronic hepatitis B patients receiving entecavir/tenofovir in South Korea. Hepatol. Res. 2018, 48, 862–871. [Google Scholar] [CrossRef]
- Yu, J.H.; Suh, Y.J.; Jin, Y.J.; Heo, N.Y.; Jang, J.W.; You, C.R.; An, H.Y.; Lee, J.W. Prediction model for hepatocellular carcinoma risk in treatment-naive chronic hepatitis B patients receiving entecavir/tenofovir. Eur. J. Gastroenterol. Hepatol. 2019, 31, 865–872. [Google Scholar] [CrossRef]
- Wu, I.T.; Hu, T.H.; Hung, C.H.; Lu, S.N.; Wang, J.H.; Lee, C.M.; Chen, C.H. Comparison of the efficacy and safety of entecavir and tenofovir in nucleos(t)ide analogue-naive chronic hepatitis B patients with high viraemia: A retrospective cohort study. Clin. Microbiol. Infect. 2017, 23, 464–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, Y.C.; Wong, G.L.; Chen, C.H.; Peng, C.Y.; Yeh, M.L.; Cheung, K.S.; Toyoda, H.; Huang, C.F.; Trinh, H.; Xie, Q.; et al. Tenofovir Versus Entecavir for Hepatocellular Carcinoma Prevention in an International Consortium of Chronic Hepatitis B. Am. J. Gastroenterol. 2020, 115, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Cho, B.W.; Jang, J.W.; Chae, H.B.; Kim, S.B.; Song, I.H. Long-term clinical outcomes of chronic Hepatitis B patients treated with Entecavir vs. Tenofovir: A retrospective, obseravational, comparative study. In Hepatology; Posters (Abstracts 301–2389); Wiley: Hoboken, NJ, USA, 2018; Volume 68, pp. 184–1353. [Google Scholar]
- Ha, I.; Chung, J.W.; Jang, E.S.; Jeong, S.H.; Kim, J.W. Comparison of the on-treatment risks for hepatocellular carcinoma between entecavir and tenofovir: A propensity score matching analysis. J. Gastroenterol. Hepatol. 2020, 35, 1774–1781. [Google Scholar] [CrossRef]
- Oh, H.; Yoon, E.L.; Jun, D.W.; Ahn, S.B.; Lee, H.Y.; Jeong, J.Y.; Kim, H.S.; Jeong, S.W.; Kim, S.E.; Shim, J.J.; et al. No Difference in Incidence of Hepatocellular Carcinoma in Patients with Chronic Hepatitis B Virus Infection Treated with Entecavir vs. Tenofovir. Clin. Gastroenterol. Hepatol. 2020, 18, 2793–2802.e2796. [Google Scholar] [CrossRef] [PubMed]
- Ha, Y.; Chon, Y.E.; Kim, M.N.; Lee, J.H.; Hwang, S.G. Hepatocellular carcinoma and death and transplantation in chronic hepatitis B treated with entecavir or tenofovir disoproxil fumarate. Sci. Rep. 2020, 10, 13537. [Google Scholar] [CrossRef]
- Hu, T.H.; Yueh-Hsia Chiu, S.; Tseng, P.L.; Chen, C.H.; Lu, S.N.; Wang, J.H.; Hung, C.H.; Kee, K.M.; Lin, M.T.; Chang, K.C.; et al. Five-year comparative risk of hepatocellular carcinoma development under entecavir or tenofovir treatment-naïve patients with chronic hepatitis B-related compensated cirrhosis in Taiwan. Aliment. Pharm. Ther. 2020, 52, 1695–1706. [Google Scholar]
- Chen, C.H.; Chen, C.Y.; Wang, J.H.; Lai, H.C.; Hung, C.H.; Lu, S.N.; Peng, C.Y. Comparison of incidence of hepatocellular carcinoma between chronic hepatitis B patients with cirrhosis treated with entecavir or tenofovir in Taiwan—A retrospective study. Am. J. Cancer Res. 2020, 10, 3882–3895. [Google Scholar]
- Na, J.E.; Sinn, D.H.; Lee, J.H.; Jang, H.J.; Baek, S.Y.; Kim, K.A.; Kang, W.S.; Gwak, G.Y.; Paik, Y.H.; Kim, Y.J.; et al. Efficacy of entecavir versus tenofovir in preventing hepatocellular carcinoma in patients with chronic hepatitis B with maintained virologic response. J. Viral Hepat. 2021, 28, 1392–1399. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle–Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [Green Version]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 10 October 2021).
- Rücker, G.; Schwarzer, G.; Carpenter, J. Arcsine test for publication bias in meta-analyses with binary outcomes. Stat. Med. 2008, 27, 746–763. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Papatheodoridis, G.V.; Dalekos, G.N.; Idilman, R.; Sypsa, V.; Van Boemmel, F.; Buti, M.; Calleja, J.L.; Goulis, J.; Manolakopoulos, S.; Loglio, A.; et al. Similar risk of hepatocellular carcinoma during long-term entecavir or tenofovir therapy in Caucasian patients with chronic hepatitis B. J. Hepatol. 2020, 73, 1037–1045. [Google Scholar] [CrossRef]
- Lim, S.G.; Amarapurkar, D.N.; Chan, H.L.; Crawford, D.H.; Gane, E.J.; Han, K.H.; Ahn, S.H.; Jafri, W.; Jia, J.; Kao, J.H.; et al. Reimbursement policies in the Asia-Pacific for chronic hepatitis B. Hepatol. Int. 2015, 9, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.Q.; Duan, Z.; Dai, E.; Zhang, S.; Han, G.; Wang, Y.; Zhang, H.; Zou, H.; Zhu, B.; Zhao, W.; et al. Tenofovir to Prevent Hepatitis B Transmission in Mothers with High Viral Load. N. Engl. J. Med. 2016, 374, 2324–2334. [Google Scholar] [CrossRef] [PubMed]
- Nathani, P.; Gopal, P.; Rich, N.; Yopp, A.; Yokoo, T.; John, B.; Marrero, J.; Parikh, N.; Singal, A.G. Hepatocellular carcinoma tumour volume doubling time: A systematic review and meta-analysis. Gut 2021, 70, 401–407. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.; Jun, D.W.; Lee, I.H.; Ahn, H.J.; Kim, B.O.; Jung, S.; Nguyen, M.H. Increasing comorbidities in a South Korea insured population-based cohort of patients with chronic hepatitis B. Aliment. Pharmacol. Ther. 2020, 52, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Hsieh, S.Y.; Lin, J.L.; Liu, M.S.; Yen, T.H. Hepatocellular carcinoma in patients with chronic kidney disease. World J. Gastroenterol. 2013, 19, 2466–2472. [Google Scholar] [CrossRef]
- Miyauchi, T.; Kanda, T.; Shinozaki, M.; Kamezaki, H.; Wu, S.; Nakamoto, S.; Kato, K.; Arai, M.; Mikami, S.; Sugiura, N.; et al. Efficacy of lamivudine or entecavir against virological rebound after achieving HBV DNA negativity in chronic hepatitis B patients. Int. J. Med. Sci. 2013, 10, 647–652. [Google Scholar] [CrossRef] [Green Version]
- Koyanagi, K.; Kubota, T.; Kobayashi, D.; Kihara, T.; Yoshida, T.; Miisho, T.; Miura, T.; Sakamoto, Y.; Takaki, J.; Seo, T.; et al. Prescription Factors Associated with Medication Non-adherence in Japan Assessed from Leftover Drugs in the SETSUYAKU-BAG Campaign: Focus on Oral Antidiabetic Drugs. Front. Pharmacol. 2016, 7, 212. [Google Scholar] [CrossRef] [Green Version]
- Chun, H.S.; Park, S.; Lee, M.; Cho, Y.; Kim, H.S.; Choe, A.R.; Kim, H.Y.; Yoo, K.; Kim, T.H. Association of Physical Activity with the Risk of Hepatocellular Carcinoma in Patients with Chronic Hepatitis B. Cancers 2021, 13, 3424. [Google Scholar] [CrossRef] [PubMed]
- Dhanasekaran, R.; Nault, J.C.; Roberts, L.R.; Zucman-Rossi, J. Genomic Medicine and Implications for Hepatocellular Carcinoma Prevention and Therapy. Gastroenterology 2019, 156, 492–509. [Google Scholar] [CrossRef]
- Park, C.H.; Jeong, S.H.; Yim, H.W.; Kim, J.D.; Bae, S.H.; Choi, J.Y.; Yoon, S.K. Family history influences the early onset of hepatocellular carcinoma. World J. Gastroenterol. 2012, 18, 2661–2667. [Google Scholar] [CrossRef] [PubMed]
- Hui, V.W.; Yip, T.C.; Wong, V.W.; Tse, Y.K.; Chan, H.L.; Lui, G.C.; Wong, G.L. Aspirin Reduces the Incidence of Hepatocellular Carcinoma in Patients with Chronic Hepatitis B Receiving Oral Nucleos(t)ide Analog. Clin. Transl. Gastroenterol. 2021, 12, e00324. [Google Scholar] [CrossRef] [PubMed]
- Goh, M.J.; Sinn, D.H.; Kim, S.; Woo, S.Y.; Cho, H.; Kang, W.; Gwak, G.Y.; Paik, Y.H.; Choi, M.S.; Lee, J.H.; et al. Statin Use and the Risk of Hepatocellular Carcinoma in Patients with Chronic Hepatitis B. Hepatology 2020, 71, 2023–2032. [Google Scholar] [CrossRef]
- Marchese, S.; Polo, A.; Ariano, A.; Velotto, S.; Costantini, S.; Severino, L. Aflatoxin B1 and M1: Biological Properties and Their Involvement in Cancer Development. Toxins 2018, 10, 214. [Google Scholar] [CrossRef] [Green Version]
- Leone, P.; Solimando, A.G.; Fasano, R.; Argentiero, A.; Malerba, E.; Buonavoglia, A.; Lupo, L.G.; De Re, V.; Silvestris, N.; Racanelli, V. The Evolving Role of Immune Checkpoint Inhibitors in Hepatocellular Carcinoma Treatment. Vaccines 2021, 9, 532. [Google Scholar] [CrossRef]
- Lee, H.W.; Lee, J.I.; Kim, S.; Kim, S.; Chang, H.Y.; Lee, K.S. Cumulative incidence of hepatocellular carcinoma and hepatitis B surface antigen Seroclearance after Nucleos(t) ide analogue-induced hepatitis B e antigen Seroclearance. BMC Gastroenterol. 2020, 20, 11360. [Google Scholar] [CrossRef]
- Jang, H.; Yoon, J.S.; Park, S.Y.; Lee, H.A.; Jang, M.-j.; Kim, S.U.; Sinn, D.H.; Seo, Y.S.; Kim, H.Y.; Kim, S.E.; et al. Impact of HBeAg on Hepatocellular Carcinoma Risk During Oral Antiviral Treatment in Patients with Chronic Hepatitis B. Clin. Gastroenterol. Hepatol. 2022, 20, 1343–1353. [Google Scholar] [CrossRef]
- Wong, G.L.; Chan, H.L.; Yiu, K.K.; Lai, J.W.; Chan, V.K.; Cheung, K.K.; Wong, E.W.; Wong, V.W. Meta-analysis: The association of hepatitis B virus genotypes and hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2013, 37, 517–526. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
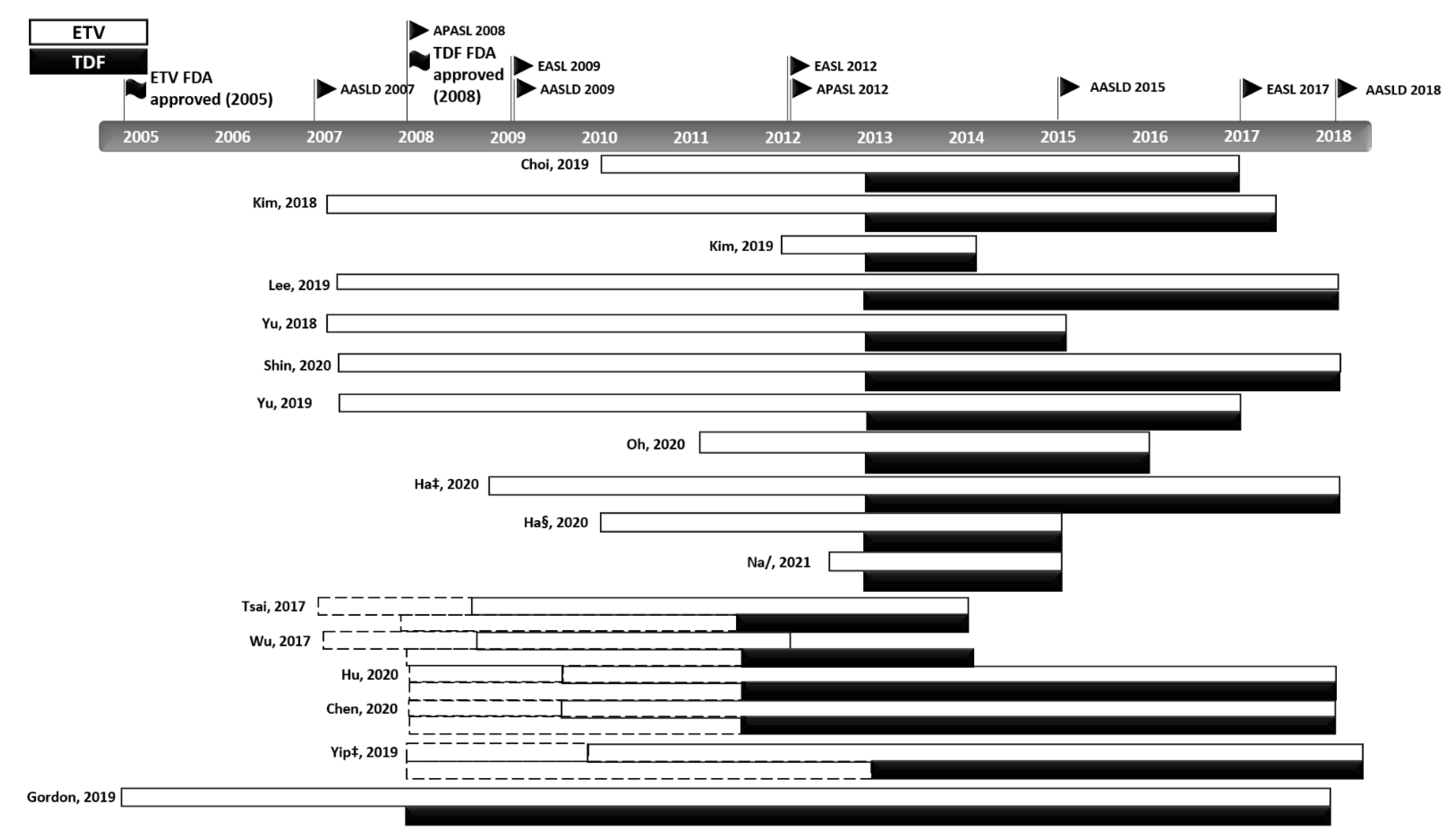
| Author Year Country | Enrolment Year | Duration (Months) TDF ETV | Cirrhosis (%) | Patients (n) | Age (Mean (±SD)) | Sex (Male%) | HBV_DNA | HBeAg Positive | HR (Naïve Only) |
|---|---|---|---|---|---|---|---|---|---|
| TDF ETV | TDF ETV | TDF ETV | (log10) (IU/mL) | TDF (%) ETV (%) | (Ref: ETV) | ||||
| Choi 2019 Korea [7] | 2010.01–2016.12 | 32 (23–43) 48 (36–48) | 653 (57.2) 935 (59.9) | 1560 1141 | 48.1 ± 10.5 49.2 ± 10.5 | 692 (60.6) 965 (61.9) | 6.4 (5.4–7.6) 6.7 (5.6–7.9) | 641 (56.2) 853 (54.7) | uHR 0.64 (0.45–0.93) aHR 0.66 (0.46–0.96) PHR 0.68 (0.49–0.99) C_HR 0.65 (0.45–0.94) C_aHR 0.64 (0.43–0.95) |
| Gordon 2019 † U.S.A. [23] | 2005–2017 | 3.2 years (TDF + ETV) | NA | 415 407 | 49.5 ± 11.3 | NA | NA | aHR 0.73 (0.29–1.84) | |
| Kim, 2018 Korea [24] | 2007.01–2017.04 | 33 (21–46) 66 (36–88) | 267 (44.2) 346 (48.0) | 604 721 | 50 ± 11 50 ± 11 | 363 (60.1) 471 (65.3) | 6.0 ± 1.6 6.4 ± 1.4 | 376 (62.3) 430 (59.7) | HR 1.36 (0.72–2.56) aHR 1.71 (0.79–3.70) C_HR 0.96 (0.5–1.84) C_aHR 1.47 (0.65–3.30) PHR 1.89 (0.8–4.5) C_PHR 1.25 (0.51–3.09) |
| Shin, 2020 Korea [25] | 2007.01–2018.01 | 3.8 (2.7–5.0) years 6.9 (4.3–8.8) years | 375 (41.67) 440 (49.22) | 900 894 | 51 ± 11 52 ± 11 | 571 (63.44) 597 (66.78) | 5.22 (3.32–6.97) 6.45 (5.32–7.81) | 565 (62.78) 537 (60.07) | uHR 0.538 (0.352–0.822) aHR 0.752 (0.489–1.155) PHR 0.769 (0.460–1.288) |
| Kim 2019 Korea [26] | 2012.01–2014.12 | 59.2 (Median) (TDF + ETV) | Compensated 411 (29.1) 499 (33.6) | 1413 1484 | 48.8 ± 12.0 48.2 ± 11.5 | 913 (64.6) 889 (59.9) | 5.4 ± 2.1 5.7 ± 2.1 | 694 (49.1) 758 (51.1) | HR 0.917 (0.705–1.191) aHR 0.975 (0.747–1.272) PHR 1.021 (0.773–1.349) IHR 0.998 (0.771–1.293) C_HR 0.848 (0.621–1.158) C_aHR 0.831 (0.606–1.139) C_aHR 0.854 (0.612–1.193) C_IHR 0.824 (0.605–1.123) |
| Lee 2019 Korea [27] | 2007.02–2018.01 | Mean 36.4 Median 36.6 Mean 60 Median 51.5 | 563 (39.12) 640 (40.43) | 1439 1583 | 47.29 ± 11.16 46.66 ± 11.76 | 841 (58.44) 926 (58.50) | 6.41 (5.34, 7.49) 6.49 (5.28, 7.67) | 823 (57.19) 974 (61.53) | HR 0.912 (0.638–1.303) aHR 0.971 (0.676–1.396) PHR 1.03 (0.703–1.509) PaHR 1.077 (0.518–2.241) C_HR 0.923 (0.420–2.028) C_aHR 0.99 (0.66–1.48) C_PHR 0.956 (0.614–1.488) C_PaHR 1.077 (0.435–2.662) |
| Tsai 2017 Taiwan [28] | 2007.01–2013.12 | 20.3 ± 6.4 43.8 ± 18.2 | 100 | 83 359 | 54.9 ± 10.9 57.8 ± 10.8 | 64 (77.1) 258 (71.9) | 6.4 ± 1.2 6.3 ± 1.3 | 19 (23) 84 (23) | HR 0.52 (0.12–2.22) |
| Yip 2019 ‡ Hongkong [29] | 2008.01–2018.06 | 2.8 years 3.7 years | 35 (3) 3650 (13) | 1309 28041 | 43.2 ± 13.1 53.4 ± 13.0 | 591 (45.1) 18094 (64.5) | 5.3 4.8 | 723 (55) 8306 (30) | sHR 0.15 (0.07–0.29) asHR 0.33 (0.16–0.67) PsHR(1:1) 0.39 (0.18–0.84) |
| Yu 2018 Korea [30] | 2007.01–2015.12 | 33.6 (6.3–60.5) 69.9 (6–119.4) | 77 (43.8) 148 (36.5) | 176 406 | 49 (20–84) 53 (18–84) | 104 (59.1) 272 (67.0) | NA | 104 (59.1) 212 (52.2) | HR 1.39 (0.56–3.45) |
| Yu 2019 Korea [31] | 2007.02–2017.01 | 48.6 (29–69.7) (TDF + ETV) | 371 (39.3) (TDF + ETV) | 342 601 | 50 (41–57) (TDF + ETV) | 586 (62) (TDF + ETV) | NA | 528 (55.9) (TDF + ETV) | HR 1.39 (0.658–2.941) |
| Wu 2017 Taiwan [32] | (T)2011.10–2014.01 (E)2007.01–2012.01 | 37.9 ± 7.2 49 ± 19.1 | 29 (27.4) 94 (30) | 106 313 | 47.1 ± 12.1 47 ± 12.3 | 74 (69.8) 230 (73.5) | 7.35 ± 0.7 7.18 ± 0.74 | 50 (47.1) 172 (55) | HR 0.73 (0.26–2.05) |
| Hsu 2019 ‡ Worldwide [33] | 2005.04.07–2018.12.23 | 38.7 (23.8–56.2) 60 (39.6–60) | 131 (18.7) 1344 (27.8) | 700 4837 | 45.74 ± 0.47 50.81 ± 0.17 | 456 (65.1) 3328 (68.8) | 4.99 ± 0.09 5.48 ± 0.03 | 208 (33.7) 1537 (33.0) | sHR 0.45 (0.26–0.79) asHR 0.81 (0.42–1.56) PsHR 0.77 (0.37–1.60) PasHR 0.89 (0.41–1.92) C_sHR 0.68 (0.27–1.68) |
| Cho 2018 † Korea [34] | NA | NA | NA | 217 517 | NA | NA | NA | NA | HR 0.47(0.16–1.37) |
| Ha 2020 ‡ Korea [35] | 2008.11–2017.12 | NA | 39 (9.3) 259 (28) | 419 921 | 45 ± 16 48 ± 15 | 266 (63) 558 (61) | 6.67 (2.63) 6.36 (2.31) | 261 (62) 488 (53) | PsHR 2.06 (0.98–4.33) PasHR 1.84 (0.9–3.79) |
| Oh 2020 Korea [36] | (T)2012.01–2015.12 (E)2011.01–2014.01 | Mean (years) 4.5 ± 1.1 Median (years) 4.7 (3.8, 5.4] Mean (years) 4.7 ± 1.0 Median (years) 4.9 [4.4, 5.5] | 310 (38.4) 315 (41.8) | 807 753 | 46.3 ± 11.2 48.7 ± 11.4 | 503 (62.3) 480 (63.7) | 6.6 [5.5, 7.7] 6.5 [5.4, 7.6] | 484 (60.0) 451 (61.4) | HR 1.26 (0.81–1.97) |
| Ha 2020 § Korea [37] | 2010–2015 | 49.1 (37.7–62.2) 64.0 (30.5–84.3) | 78 (34.8) 67 (37.2) | 224 180 | 44.5 ± 11.4 45.4 ± 10.8 | 120 (53.6) 106 (58.9) | 7.44 (6.33, 8.53) 7.71 (6.74, 8.64) | 128 (57.1) 118 (67.4) | HR 0.31 (0.12–0.79) PHR 0.27 (0.08–0.98) IHR 0.32 (0.13–0.80) C_HR 0.30 (0.11–0.84) |
| Hu 2020 Taiwan [38] | 2008.01–2018.03 | NA (5 years sub cohort) | 100% | 216 678 | 56.1 ± 11.6 59.4 ± 11.1 | 162 (75) 491 (72.4) | NA | 41 (19.0) 125 (18.4) | aHR 0.66 (0.40–1.08) ‖ PaHR 0.66 (0.38–1.14) ‖ |
| Chen 2020 Taiwan [39] | (T) 2011–2018 (E) 2008–2018 | NA | NA | 1353 (TDF + ETV) | NA | NA | NA | NA | HR 0.523 (0.363–0.752) aHR 0.582 (0.401–0.843) C_HR 0.534 (0.355–0.805) C_aHR 0.576 (0.379–0.877) |
| Na 2021 * Korea [40] | 2012.06–2015.12 | 3.8 (2.9, 4.9) (years) 5.2 (3.4, 6.2) (years) | 302 (45.4) 377 (56.2) | 665 671 | 49 (42, 56) 51 (44, 57) | 384 (57.7) 392 (58.4) | 5.9 (4.6, 7.1) 5.7 (4.6, 6.6) | 291 (43.7) 196 (29.2) | HR 0.94 (0.63–1.41) aHR 0.82 (0.52–1.29) PHR 1.02 (0.68–1.52) IHR 1.11 (0.74–1.66) |
| Author Year Country | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Choi 2019 Korea [7] | Treatment naïve patients Treatment > 6 months Korean adults (Age ≥ 20 and ≤ 79 years) | Serum HBV DNA at baseline <2000 IU/mL (or undetectable) More than two weeks of previous treatment with other antiviral agents Loss of hbsag within 6 months of treatment initiation Death or liver transplantation within 6 months of treatment HCC diagnosis within 1 year of treatment initiation Co-infection with human immunodeficiency virus or other hepatotrophic viruses History of any malignant disease |
| Gordon 2019 † U.S.A. [23] | Treatment naïve 80% (642/822) | Liver transplantation HIV co-infection ETV and TDF combine therapy |
| Kim, 2018 Korea [24] | Treatment naïve patients Age ≥ 18 Treatment > 12 months | Co-infection with human immunodeficiency virus or other hepatotrophic viruses Serum HBV DNA at baseline <2000 IU/mL Creatinine > 1.5 mg/dL Death within 6 months of treatment HCC diagnosis within 1 year of treatment initiation History of HCC before treatment Liver transplantation Decompensated LC patients Adherence rate < 80% |
| Shin, 2020 Korea [25] | Treatment naïve patients Age ≥ 18 Treatment > 12 months | Co-infection HCV, HDV, HIV History of any malignant disease Decompensated LC patients or Child–Pugh score ≥ 7 Creatinine > 1.5 mg/dL Death within 6 months of treatment HCC diagnosis within 1 year of treatment initiation |
| Kim 2019 Korea [26] | Treatment naïve patients Age ≥ 19 Treatment > 12 months | Coinfection with other hepatitis virus Prior organ transplant or hcc HCC, liver transplant, or death < 6 months after enrolment Decompensated cirrhosis Significant medical illness |
| Lee 2019 Korea [27] | Treatment naïve patients Treatment > 6 months | Co-infection with HCV, HIV HCC, liver transplant < 6 months after enrolment History of any malignant disease Prior organ transplant or HCC Decompensated cirrhosis |
| Tsai 2017 Taiwan [28] | Treatment naïve patients Cirrhotic patients only HBV DNA ≥ 2000 IU | HIV, HCV, HDV, HEV coinfection HCC < 6 months after enrolment History of HCC before treatment DILI/alcohol > 50 g/d |
| Yip 2019 Hongkong [29] | Treatment naïve patients Treatment > 6 months | HIV, HCV, HDV coinfection Autoimmune disease, metabolic liver disease History of HCC before treatment History of any malignant disease HCC, death < 6 months after enrolment Prior liver transplant or liver transplant < 6 months after enrolment ETV and TDF combined therap |
| Yu 2018 Korea [30] | Treatment naïve patients Age ≥ 18 Treatment > 6 months | Other viral hepatitis, Autoimmune disease, Metabolic liver disease History of HCC before treatment History of any malignant disease |
| Yu 2019 Korea [31] | Treatment naïve patients Age ≥ 18 Treatment > 12 months | Other viral hepatitis, autoimmune disease, metabolic liver disease History of HCC before treatment History of any malignant disease |
| Wu 2017 Taiwan [32] | Treatment naïve patients Treatment > 12 months High viral load >6 log10 (IU/mL) | Co-infection Alcoholic, autoimmune hepatitis HCC < 12 months of enrolment |
| Hsu 2019 Worldwide [33] | Treatment naïve patients Age ≥ 18 Monotherapy treatment > 12 months | Any malignant disease at the initiation HCC or death < 12 months of enrolment History of solid organ transplantation or significant use of immunosuppression Co-infection ETV and TDF combined therapy |
| Cho 2018 † Korea [34] | Treatment naïve patients | Na |
| Ha 2020 ǂ Korea [35] | Treatment naïve patients Age > 18 Treatment > 12 months | Serum HBV DNA at baseline <2000 IU/mL HCC, death, liver transplant < 6 months of enrolment Prior liver transplant or HCC before inclusion |
| Oh 2020 Korea [36] | Treatment naïve patients Age ≥ 18 Treatment > 12 months | Co-infection HCV, HIV History of any malignant over the preceding 5 years HCC, death, treatment modification < 12 months after enrolment |
| Ha 2020 § Korea [37] | Treatment naïve patients Age 18–80 years, Treatment > 6 months | Co-infection with other viral infection HCC, seroconversion, any malignancy, organ transplant < 6 months of enrolment |
| Hu 2020 Taiwan [38] | Cirrhotic patients only (Treatment naïve sub cohort) Treatment > 6 months | Co-infection HCV, HDV, HIV HCC < 6 months after enrolment ETV and TDF combined therapy or switching History of HCC before treatment Decompensated LC patients Alcoholic, autoimmune disease |
| Chen 2020 Taiwan [39] | Cirrhotic patients only Treatment naïve patients Age ≥ 18 Monotherapy treatment > 12 months | Co-infection HCV, HDV, HIV Alcoholic, autoimmune disease Liver transplant or HCC before inclusion or < 12 months after enrolment |
| Na 2021 Korea [40] | Treatment naïve patients Follow-up duration > 12 months Age ≥ 18 | Co-infection HCV, HIV Liver transplant or HCC before inclusion or < 12 months after enrolment Prior or concurrent malignancy including HCC and organ transplantation Did not achieve MVR during NAs therapy (<20 IU/mL) Development of HCC or received liver transplantation before CVR or within one year after achieving CVR Incident malignancy other than HCC during follow-up Follow-up duration less than one year after achieving CVR Switch to other NAS |
| Subgroup | Number of Studies | HR (95% CI) | I2 (%) |
|---|---|---|---|
| Treatment duration less than 6 months vs. 12 months | |||
| 6 months | 6 | 0.56 (0.34–0.92) * | 80 † |
| 12 months | 10 | 0.83 (0.63–1.08) | 66 † |
| Exclusion of patients diagnosed with HCC within 6 months vs. 12 months | |||
| 6 months | 7 | 0.64 (0.39–1.04) | 82 † |
| 12 months | 8 | 0.69 (0.54–0.88) † | 54 * |
| Interval of over three years in the start point of patient enrolment | |||
| <3 years | 5 | 0.83 (0.62–1.12) | 61 * |
| >3 years | 13 | 0.69 (0.51–0.92)/ | 68 † |
| Exclusion of patients with baseline HBV DNA levels of <2000 IU/mL | |||
| Yes | 4 | 0.87 (0.50–1.52) | 63 |
| No | 13 | 0.69 (0.52–0.90) † | 74 † |
| Exclusion of patients with significant alcoholic liver disease | |||
| Yes | 4 | 0.58 (0.44–0.76) † | 0 |
| No | 11 | 0.75 (0.57–1.00) | 76 † |
| Exclusion of patients with CKD or baseline creatinine >1.5 mg/dL | |||
| Yes | 3 | 0.74 (0.51–1.05) | 55 |
| No | 14 | 0.72 (0.53–0.97) * | 74 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, H.; Lee, H.Y.; Kim, J.; Kim, Y.J. Systematic Review with Meta-Analysis: Comparison of the Risk of Hepatocellular Carcinoma in Antiviral-Naive Chronic Hepatitis B Patients Treated with Entecavir versus Tenofovir: The Devil in the Detail. Cancers 2022, 14, 2617. https://doi.org/10.3390/cancers14112617
Oh H, Lee HY, Kim J, Kim YJ. Systematic Review with Meta-Analysis: Comparison of the Risk of Hepatocellular Carcinoma in Antiviral-Naive Chronic Hepatitis B Patients Treated with Entecavir versus Tenofovir: The Devil in the Detail. Cancers. 2022; 14(11):2617. https://doi.org/10.3390/cancers14112617
Chicago/Turabian StyleOh, Hyunwoo, Hyo Young Lee, Jihye Kim, and Yoon Jun Kim. 2022. "Systematic Review with Meta-Analysis: Comparison of the Risk of Hepatocellular Carcinoma in Antiviral-Naive Chronic Hepatitis B Patients Treated with Entecavir versus Tenofovir: The Devil in the Detail" Cancers 14, no. 11: 2617. https://doi.org/10.3390/cancers14112617
APA StyleOh, H., Lee, H. Y., Kim, J., & Kim, Y. J. (2022). Systematic Review with Meta-Analysis: Comparison of the Risk of Hepatocellular Carcinoma in Antiviral-Naive Chronic Hepatitis B Patients Treated with Entecavir versus Tenofovir: The Devil in the Detail. Cancers, 14(11), 2617. https://doi.org/10.3390/cancers14112617