
Inter-Reader Agreement of Diffusion-Weighted Magnetic Resonance Imaging for Breast Cancer Detection: A Multi-Reader Retrospective Study

 ,
, 
 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
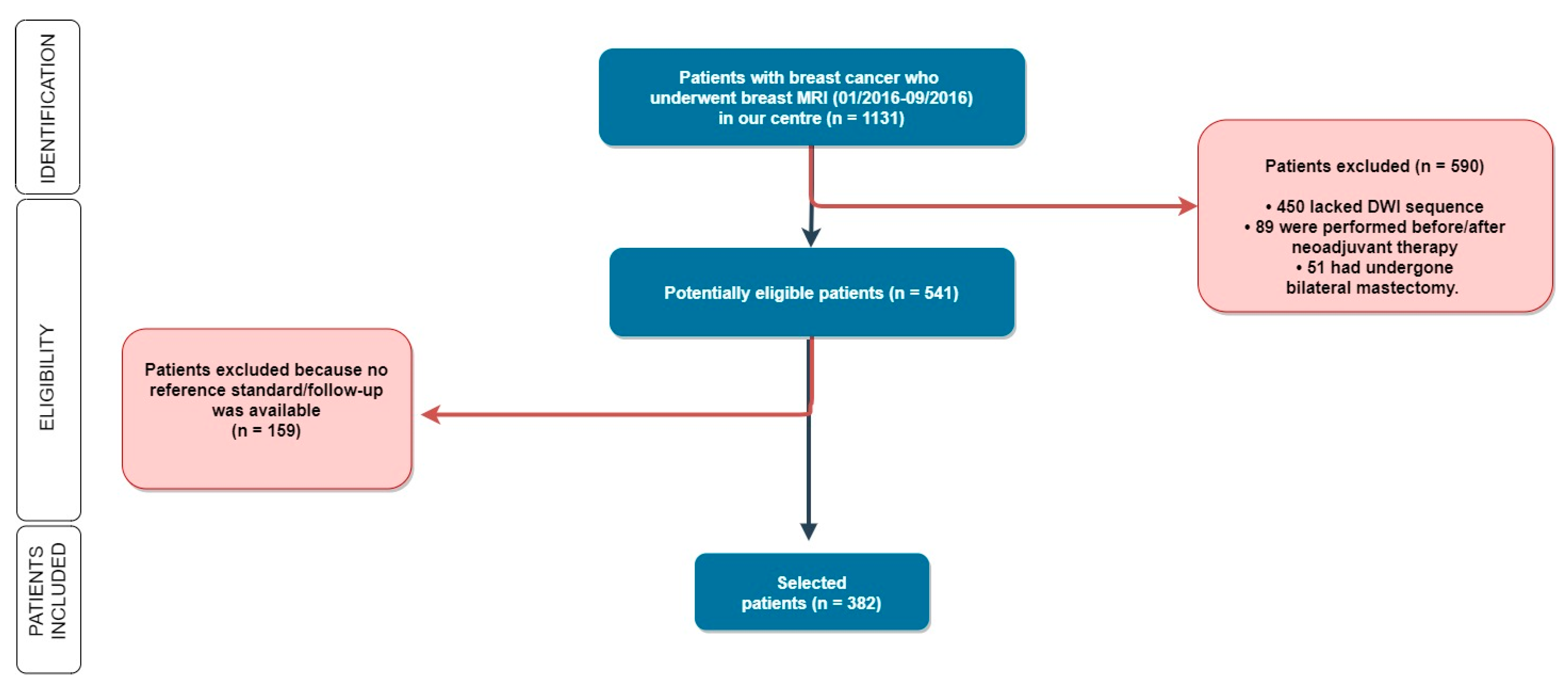
2.1. Patient Population
2.2. MRI Technique
2.3. Image Analysis and Readers’ Characteristics
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Henderson, L.M.; Hubbard, R.A.; Zhu, W.; Weiss, J.; Wernli, K.J.; Goodrich, M.E.; Kerlikowske, K.; DeMartini, W.; Ozanne, E.M.; Onega, T. Preoperative Breast Magnetic Resonance Imaging Use by Breast Density and Family History of Breast Cancer. J. Women’s Health 2018, 27, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.; Yang, M.; Yang, H.; Zhou, F.; Shen, W. Predicting the response to neoadjuvant therapy for early-stage breast cancer: Tumor-, blood-, and imaging-related biomarkers. Cancer Manag. Res. 2018, 10, 4333–4347. [Google Scholar] [CrossRef] [PubMed]
- Dogan, B.E.; Scoggins, M.E.; Son, J.B.; Wei, W.; Candelaria, R.; Yang, W.T.; Ma, J. American College of Radiology–Compliant Short Protocol Breast MRI for High-Risk Breast Cancer Screening: A Prospective Feasibility Study. Am. J. Roentgenol. 2018, 210, 214–221. [Google Scholar] [CrossRef] [PubMed]
- McGrath, A.L.; Price, E.R.; Eby, P.R.; Rahbar, H. MRI-guided breast interventions. J. Magn. Reson. Imaging 2017, 46, 631–645. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, C.K. The Changing World of Breast Cancer: A Radiologist’s Perspective. Plast. Surg. Nurs. 2016, 36, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Mann, R.M.; Balleyguier, C.; Baltzer, P.A.; Bick, U.; Colin, C.; Cornford, E.; Evans, A.N.; Fallenberg, E.M.; Forrai, G.; Fuchsjäger, M.H.; et al. Breast MRI: EUSOBI recommendations for women’s information. Eur. Radiol. 2015, 25, 3669–3678. [Google Scholar] [CrossRef] [PubMed]
- Rotili, A.; Trimboli, R.M.; Penco, S.; Pesapane, F.; Tantrige, P.; Cassano, E.; Sardanelli, F. Double reading of diffusion-weighted magnetic resonance imaging for breast cancer detection. Breast Cancer Res. Treat. 2020, 180, 111–120. [Google Scholar] [CrossRef]
- Penco, S.; Rotili, A.; Pesapane, F.; Trentin, C.; Dominelli, V.; Faggian, A.; Farina, M.; Marinucci, I.; Bozzini, A.; Pizzamiglio, M.; et al. MRI-guided vacuum-assisted breast biopsy: Experience of a single tertiary referral cancer centre and prospects for the future. Med. Oncol. 2020, 37, 1–9. [Google Scholar] [CrossRef]
- Pesapane, F.; Suter, M.B.; Rotili, A.; Penco, S.; Nigro, O.; Cremonesi, M.; Bellomi, M.; Jereczek-Fossa, B.A.; Pinotti, G.; Cassano, E. Will traditional biopsy be substituted by radiomics and liquid biopsy for breast cancer diagnosis and characterisation? Med. Oncol. 2020, 37, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Barrett, T.; Brechbiel, M.; Bernardo, M.; Choyke, P.L. MRI of tumor angiogenesis. J. Magn. Reson. Imaging 2007, 26, 235–249. [Google Scholar] [CrossRef]
- Kuhl, C.K. Abbreviated Magnetic Resonance Imaging (MRI) for Breast Cancer Screening: Rationale, Concept, and Transfer to Clinical Practice. Annu. Rev. Med. 2019, 70, 501–519. [Google Scholar] [CrossRef]
- Ko, E.S.; Morris, E.A. Abbreviated Magnetic Resonance Imaging for Breast Cancer Screening: Concept, Early Results, and Considerations. Korean J. Radiol. 2019, 20, 533–541. [Google Scholar] [CrossRef] [PubMed]
- McDonald, R.J.; McDonald, J.S.; Kallmes, D.F.; Jentoft, M.E.; Paolini, M.A.; Murray, D.L.; Williamson, E.E.; Eckel, L.J. Gadolinium Deposition in Human Brain Tissues after Contrast-enhanced MR Imaging in Adult Patients without Intracranial Abnormalities. Radiology 2017, 285, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Sardanelli, F.; Carbonaro, L.A.; Montemezzi, S.; Cavedon, C.; Trimboli, R.M. Clinical Breast MR Using MRS or DWI: Who Is the Winner? Front. Oncol. 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.P.; Harmon, S.A.; Barrett, T.; Bittencourt, L.K.; Law, Y.M.; Shebel, H.; An, J.Y.; Czarniecki, M.; Mehralivand, S.; Coskun, M.; et al. Intra- and interreader reproducibility of PI-RADSv2: A multireader study. J. Magn. Reson. Imaging 2019, 49, 1694–1703. [Google Scholar] [CrossRef]
- Moran, C.J.; Cheng, J.Y.; Ms, C.M.S.; Carl, M.; Alley, M.T.; Rosenberg, J.; Daniel, B.L.; Pittman, S.M.; Rosen, E.L.; Hargreaves, B.A. Diffusion-weighted double-echo steady-state with a three-dimensional cones trajectory for non-contrast-enhanced breast MRI. J. Magn. Reson. Imaging 2021, 53, 1594–1605. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, C.K.; Schrading, S.; Strobel, K.; Schild, H.H.; Hilgers, R.-D.; Bieling, H.B. Abbreviated Breast Magnetic Resonance Imaging (MRI): First Postcontrast Subtracted Images and Maximum-Intensity Projection—A Novel Approach to Breast Cancer Screening With MRI. J. Clin. Oncol. 2014, 32, 2304–2310. [Google Scholar] [CrossRef]
- Jones, L.I.; Geach, R.; Harding, S.A.; Foy, C.; Taylor, V.; Marshall, A.; Taylor-Phillips, S.; Dunn, J.A. Can mammogram readers swiftly and effectively learn to interpret first post-contrast acquisition subtracted (FAST) MRI, a type of abbreviated breast MRI?: A single centre data-interpretation study. Br. J. Radiol. 2019, 92, 20190663. [Google Scholar] [CrossRef] [PubMed]
- Ranganathan, P.; Pramesh, C.S.; Aggarwal, R. Common pitfalls in statistical analysis: Measures of agreement. Perspect. Clin. Res. 2017, 8, 187–191. [Google Scholar] [CrossRef]
- de Vet, H.C.; Terwee, C.B.; Knol, D.L.; Bouter, L.M. When to use agreement versus reliability measures. J. Clin. Epidemiol. 2006, 59, 1033–1039. [Google Scholar] [CrossRef]
- National Institute for Standards and Technology. Guidelines for Evaluating and Expressing the Uncertainty of NIST Measurement Results. 1994. Available online: http://physics.nist.gov/Pubs/guidelines/content2020 (accessed on 1 April 2021).
- American College of Radiology (ACR). BIRADS-MRI. Breast Imaging Reporting and Data System Atlas; American College of Radiology: Washington, DC, USA, 2003. [Google Scholar]
- Landis, J.R.; Koch, G.G. (An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple observers. Biometrics 1977, 33, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Antognini, A.B.; Vagheggini, A.; Zagoraiou, M. Is the classical Wald test always suitable under response-adaptive randomization? Stat. Methods Med. Res. 2018, 27, 2294–2311. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: https://www.R-project.org (accessed on 1 April 2021).
- Patella, F.; Franceschelli, G.; Petrillo, M.; Sansone, M.; Fusco, R.; Pesapane, F.; Pompili, G.; Ierardi, A.M.; Saibene, A.M.; Moneghini, L.; et al. A multiparametric analysis combining DCE-MRI- and IVIM-derived parameters to improve differentiation of parotid tumors: A pilot study. Futur. Oncol. 2018, 14, 2893–2903. [Google Scholar] [CrossRef] [PubMed]
- Pesapane, F.; Patella, F.; Fumarola, E.M.; Panella, S.; Ierardi, A.M.; Pompili, G.G.; Franceschelli, G.; Angileri, S.A.; Biasina, A.M.; Carrafiello, G. Intravoxel Incoherent Motion (IVIM) Diffusion Weighted Imaging (DWI) in the Periferic Prostate Cancer Detection and Stratification. Med. Oncol. 2017, 34, 35. [Google Scholar] [CrossRef]
- Zhang, L.; Riethdorf, S.; Wu, G.; Wang, T.; Yang, K.; Peng, G.; Liu, J.; Pantel, K. Meta-Analysis of the Prognostic Value of Circulating Tumor Cells in Breast Cancer. Clin. Cancer Res. 2012, 18, 5701–5710. [Google Scholar] [CrossRef]
- Chen, X.; Li, W.-L.; Zhang, Y.-L.; Wu, Q.; Guo, Y.-M.; Bai, Z.-L. Meta-analysis of quantitative diffusion-weighted MR imaging in the differential diagnosis of breast lesions. BMC Cancer 2010, 10, 693. [Google Scholar] [CrossRef]
- Zhang, L.; Tang, M.; Min, Z.; Lu, J.; Lei, X.; Zhang, X. Accuracy of combined dynamic contrast-enhanced magnetic resonance imaging and diffusion-weighted imaging for breast cancer detection: A meta-analysis. Acta Radiol. 2015, 57, 651–660. [Google Scholar] [CrossRef]
- Yamada, T.; Kanemaki, Y.; Okamoto, S.; Nakajima, Y. Comparison of detectability of breast cancer by abbreviated breast MRI based on diffusion-weighted images and postcontrast MRI. Jpn. J. Radiol. 2018, 36, 331–339. [Google Scholar] [CrossRef]
- Clauser, P.; Mann, R.; Athanasiou, A.; Prosch, H.; Pinker, K.; Dietzel, M.; Helbich, T.H.; Fuchsjäger, M.; Camps-Herrero, J.; Sardanelli, F.; et al. A survey by the European Society of Breast Imaging on the utilisation of breast MRI in clinical practice. Eur. Radiol. 2018, 28, 1909–1918. [Google Scholar] [CrossRef]
- Baltzer, P.; Mann, R.M.; Iima, M.; Sigmund, E.E.; Clauser, P.; Gilbert, F.J.; Martincich, L.; Partridge, S.C.; Patterson, A.; Pinker, K.; et al. Diffusion-weighted imaging of the breast—A consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group. Eur. Radiol. 2020, 30, 1436–1450. [Google Scholar] [CrossRef] [PubMed]
- Amornsiripanitch, N.; Bickelhaupt, S.; Shin, H.J.; Dang, M.; Rahbar, H.; Pinker, K.; Partridge, S.C. Diffusion-weighted MRI for Unenhanced Breast Cancer Screening. Radiology 2019, 293, 504–520. [Google Scholar] [CrossRef]
- Tsushima, Y.; Takahashi-Taketomi, A.; Endo, K. Magnetic resonance (MR) differential diagnosis of breast tumors using apparent diffusion coefficient (ADC) on 1.5-T. J. Magn. Reson. Imaging 2009, 30, 249–255. [Google Scholar] [CrossRef]
- Baltzer, P.A.; Bickel, H.; Spick, C.; Wengert, G.; Woitek, R.; Kapetas, P.; Clauser, P.; Helbich, T.H.; Pinker, K. Potential of Noncontrast Magnetic Resonance Imaging With Diffusion-Weighted Imaging in Characterization of Breast Lesions: Intraindividual Comparison With Dynamic Contrast-Enhanced Magnetic Resonance Imaging. Investig. Radiol. 2018, 53, 229–235. [Google Scholar] [CrossRef]
- Wisner, D.J.; Rogers, N.; Deshpande, V.S.; Newitt, D.N.; Laub, G.A.; Porter, D.A.; Kornak, J.; Joe, B.N.; Hylton, N.M. High-resolution diffusion-weighted imaging for the separation of benign from malignant BI-RADS 4/5 lesions found on breast MRI at 3T. J. Magn. Reson. Imaging 2014, 40, 674–681. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indication | Number of Patients | % |
|---|---|---|
| Screening in high-risk patients | 156 | 41 |
| Problem solving for inconclusive mammogram or US examination | 74 | 20 |
| Preoperative staging | 67 | 18 |
| Follow-up in previous breast cancer | 63 | 16 |
| Nipple discharge | 7 | 2 |
| Needle biopsy showing borderline lesions (B3) | 6 | 1 |
| CUP syndrome | 5 | 1 |
| Post-operative positive margins | 4 | 1 |
| Total | 382 | 100 |
| Inclusion Criteria: | Exclusion Criteria: |
|---|---|
| ≥18 years old women | pregnancy or breastfeeding |
| at least one year of clinical and radiological follow-up or histological analysis through biopsy or surgery | patients who underwent surgery or follow-up in other hospitals/centres |
| written informed consent for MRI must be signed and dated by both the patient and the radiologist | patients undergoing neoadjuvant chemotherapy |
| common contraindications to MRI (presence of pacemaker non-MRI-safety or claustrophobia) |
| Performance Index | Expert_1 | Expert_2 | NonExpert_1 | NonExpert_2 |
|---|---|---|---|---|
| Sensitivity | 89/96 (93%, 86–96%) | 83/96 (87%, 78–93%) | 81/96 (84%, 82–93%) | 77/96 (80%, 76–89%) |
| Specificity | 562/609 (93%, 90–94%) | 538/609 (88%, 86–91%) | 526/609 (86%, 83–89%) | 511/609 (83%, 81–879%) |
| Accuracy | 645/724 (89%, 87–92%) | 698/724 (96%, 92–98%) | 640/724 (88%, 86–92%) | 615/724 (84%, 82–98%) |
| Tumor Size | Sensitivity of Double Reading of Expert_1 and Expert_2) | p-Value |
|---|---|---|
| ≤ 10 mm | 25/33(75%, 52–86%) | 0.010 |
| > 10–20 mm | 44/48 (92%, 82–99%) | |
| > 20 mm | 36/39 (92%, 78–98%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pesapane, F.; Rotili, A.; Penco, S.; Montesano, M.; Agazzi, G.M.; Dominelli, V.; Trentin, C.; Pizzamiglio, M.; Cassano, E. Inter-Reader Agreement of Diffusion-Weighted Magnetic Resonance Imaging for Breast Cancer Detection: A Multi-Reader Retrospective Study. Cancers 2021, 13, 1978. https://doi.org/10.3390/cancers13081978
Pesapane F, Rotili A, Penco S, Montesano M, Agazzi GM, Dominelli V, Trentin C, Pizzamiglio M, Cassano E. Inter-Reader Agreement of Diffusion-Weighted Magnetic Resonance Imaging for Breast Cancer Detection: A Multi-Reader Retrospective Study. Cancers. 2021; 13(8):1978. https://doi.org/10.3390/cancers13081978
Chicago/Turabian StylePesapane, Filippo, Anna Rotili, Silvia Penco, Marta Montesano, Giorgio Maria Agazzi, Valeria Dominelli, Chiara Trentin, Maria Pizzamiglio, and Enrico Cassano. 2021. "Inter-Reader Agreement of Diffusion-Weighted Magnetic Resonance Imaging for Breast Cancer Detection: A Multi-Reader Retrospective Study" Cancers 13, no. 8: 1978. https://doi.org/10.3390/cancers13081978
APA StylePesapane, F., Rotili, A., Penco, S., Montesano, M., Agazzi, G. M., Dominelli, V., Trentin, C., Pizzamiglio, M., & Cassano, E. (2021). Inter-Reader Agreement of Diffusion-Weighted Magnetic Resonance Imaging for Breast Cancer Detection: A Multi-Reader Retrospective Study. Cancers, 13(8), 1978. https://doi.org/10.3390/cancers13081978