
Rituximab and Bendamustine (BR) Compared with Rituximab, Bendamustine, and Cytarabine (R-BAC) in Previously Untreated Elderly Patients with Mantle Cell Lymphoma

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Partecipants
2.2. Efficacy and Toxicity Outcomes
2.3. Statistical Analysis
3. Results
3.1. Patients
3.2. Administered Cycles, Dose Reductions, and Tumor Response
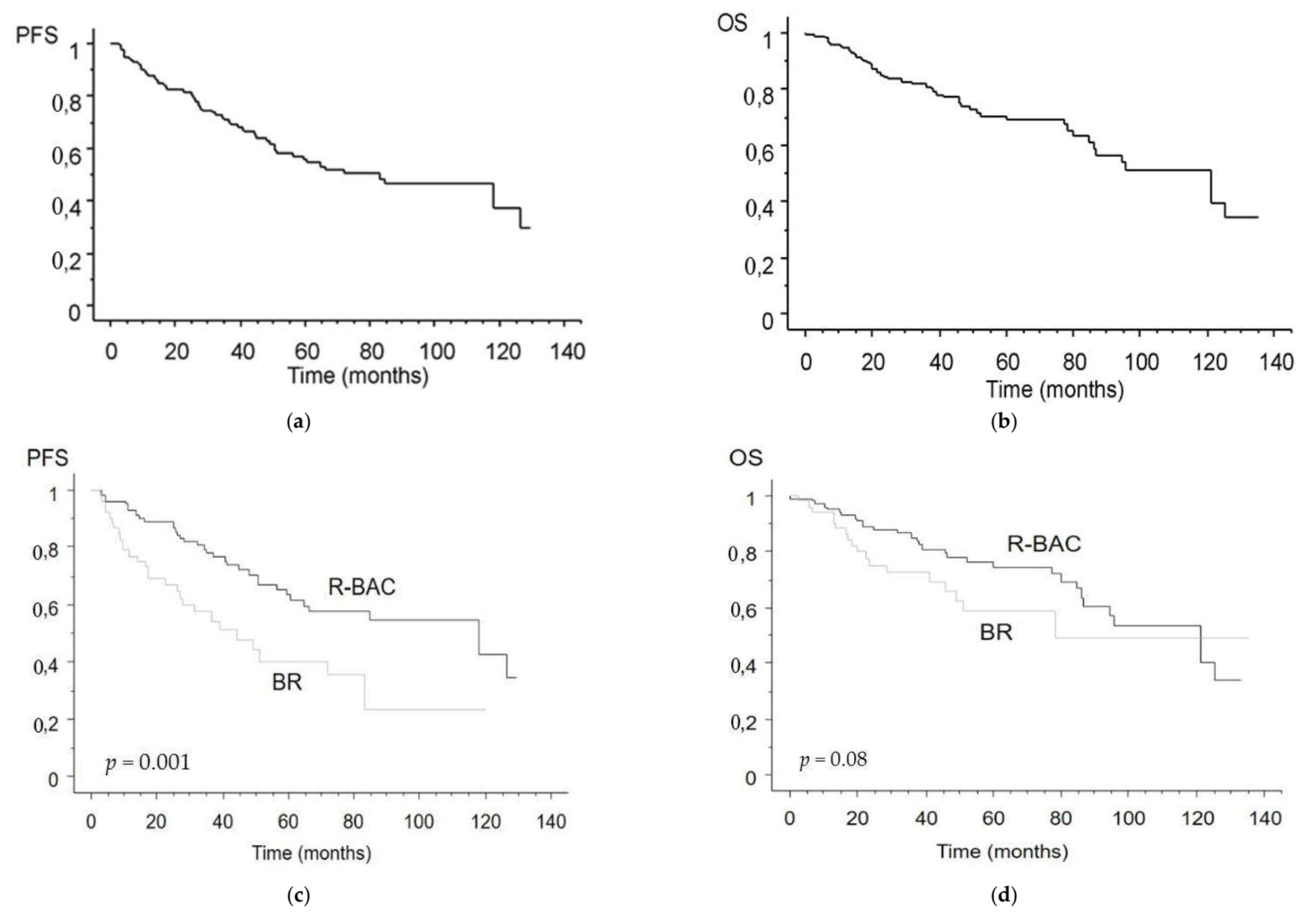
3.3. Survival Analysis
3.4. Toxicity
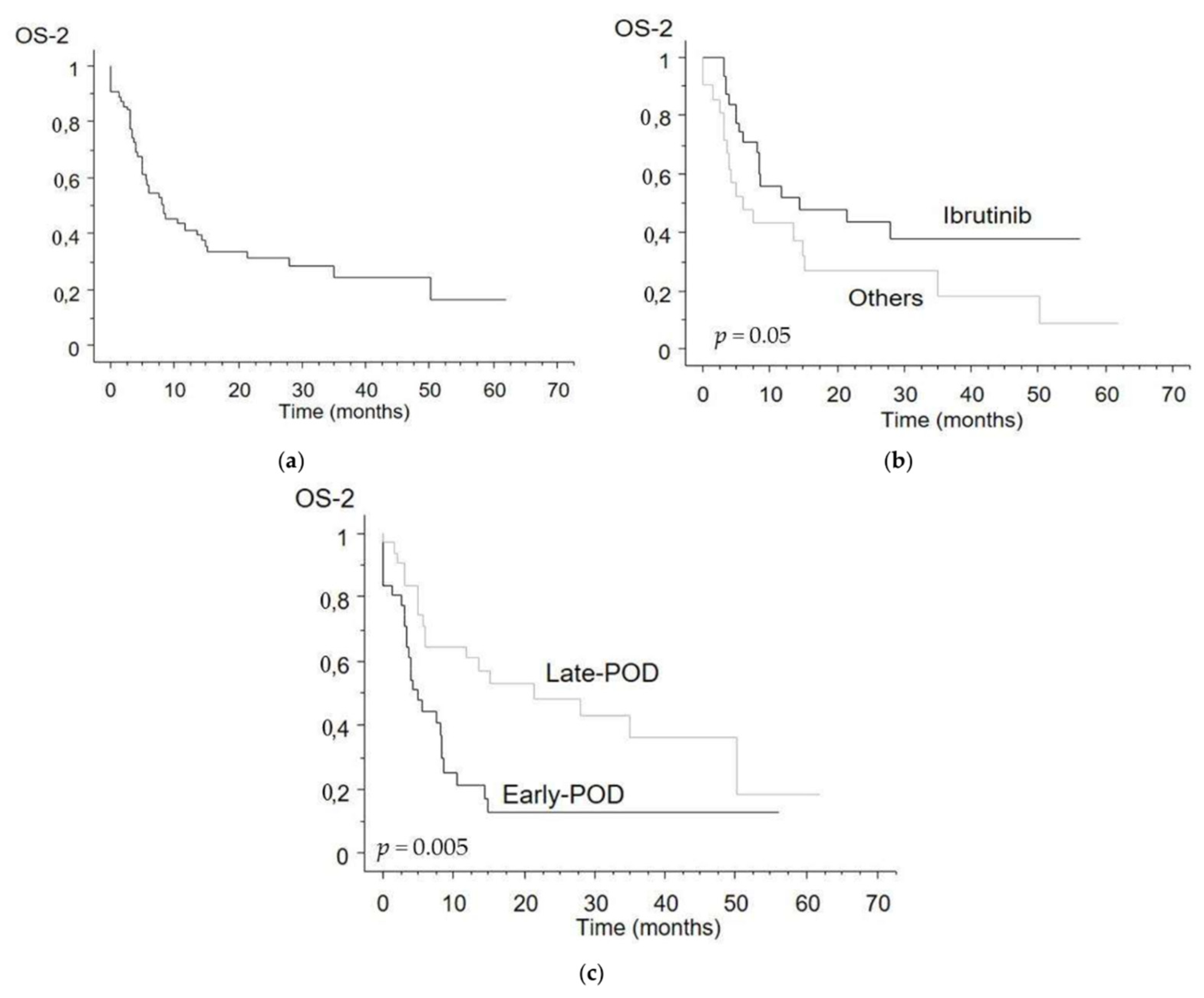
3.5. Second Line Treatments and Survival, POD-24
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herrmann, A.; Hoster, E.; Zwingers, T.; Brittinger, G.; Engelhard, M.; Meusers, P.; Reiser, M.; Forstpointner, R.; Metzner, B.; Peter, N.; et al. Improvement of Overall Survival in Advanced Stage Mantle Cell Lymphoma. J. Clin. Oncol. 2009, 27, 511–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephens, D.M.; Spurgeon, S.E. Ibrutinib in mantle cell lymphoma patients: Glass half full? Evidence and opinion. Ther. Adv. Hematol. 2015, 6, 242–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kluin-Nelemans, H.; Hoster, E.; Hermine, O.; Walewski, J.; Trneny, M.; Geisler, C.; Stilgenbauer, S.; Thieblemont, C.; Vehling-Kaiser, U.; Doorduijn, J.; et al. Treatment of Older Patients with Mantle-Cell Lymphoma. N. Engl. J. Med. 2012, 367, 520–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robak, T.; Smolewski, P.; Robak, P.; Dreyling, M. Mantle cell lymphoma: Therapeutic options in transplant-ineligible patients. Leuk. Lymphoma 2019, 60, 2622–2634. [Google Scholar] [CrossRef] [PubMed]
- Rummel, M.J.; Niederle, N.; Maschmeyer, G.; Banat, G.A.; von Grünhagen, U.; Losem, C.; Kofahl-Krause, D.; Heil, G.; Welslau, M.; Balser, C.; et al. Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: An open-label, multicentre, randomised, phase 3 non-inferiority trial. Lancet 2013, 381, 1203–1210. [Google Scholar] [CrossRef]
- Flinn, I.W.; Van Der Jagt, R.; Kahl, B.S.; Wood, P.R.; Hawkins, T.E.; Macdonald, D.; Hertzberg, M.; Kwan, Y.-L.; Simpson, D.M.; Craig, M.; et al. Randomized trial of bendamustine-rituximab or R-CHOP/R-CVP in first-line treatment of indolent NHL or MCL: The BRIGHT study. Blood 2014, 123, 2944–2952. [Google Scholar] [CrossRef] [PubMed]
- Visco, C.; Chiappella, A.; Nassi, L.; Patti, C.; Ferrero, S.; Barbero, D.; Evangelista, A.; Spina, M.; Molinari, A.; Rigacci, L.; et al. Rituximab, bendamustine, and low-dose cytarabine as induction therapy in elderly patients with mantle cell lymphoma: A multicentre, phase 2 trial from Fondazione Italiana Linfomi. Lancet Haematol. 2017, 4, e15–e23. [Google Scholar] [CrossRef] [Green Version]
- Flinn, I.W.; Van Der Jagt, R.; Kahl, B.; Wood, P.; Hawkins, T.; Macdonald, D.; Simpson, D.; Kolibaba, K.; Issa, S.; Chang, J.; et al. First-Line Treatment of Patients With Indolent Non-Hodgkin Lymphoma or Mantle-Cell Lymphoma with Bendamustine Plus Rituximab versus R-CHOP or R-CVP: Results of the BRIGHT 5-Year Follow-Up Study. J. Clin. Oncol. 2019, 37, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Dreyling, M.; Campo, E.; Hermine, O.; Jerkeman, M.; le Gouill, S.; Rule, S.; Shpilberg, O.; Walewski, J.; Ladetto, M. Newly diagnosed and relapsed mantle cell lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv62–iv71. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. B-Cell Lymphomas (Version 4.2021). Available online: https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf (accessed on 5 May 2021).
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheson, B.D. Staging and Evaluation of the Patient with Lymphoma. Hematol. Clin. N. Am. 2008, 22, 825–837. [Google Scholar] [CrossRef] [PubMed]
- Rule, S.; Barreto, W.G.; Briones, J.; Carella, A.M.; Casasnovas, O.; Pocock, C.; Wendtner, C.-M.; Zaja, F.; Robson, S.; MacGregor, L.; et al. Efficacy and safety assessment of prolonged maintenance with subcutaneous rituximab in patients with relapsed or refractory indolent non-Hodgkin lymphoma: Results of the Phase III MabCute study. Haematologica 2021. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Wang, M. Mantle cell lymphoma: 2019 update on the diagnosis, pathogenesis, prognostication, and management. Am. J. Hematol. 2019, 94, 710–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Visco, C.; Di Rocco, A.; Evangelista, A.; Quaglia, F.M.; Tisi, M.C.; Morello, L.; Zilioli, V.R.; Rusconi, C.; Hohaus, S.; Sciarra, R.; et al. Outcomes in first relapsed-refractory younger patients with mantle cell lymphoma: Results from the MANTLE-FIRST study. Leukemia 2021, 35, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Visco, C.; Tisi, M.C.; Evangelista, A.; Di Rocco, A.; Zoellner, A.-K.; Zilioli, V.R.; Hohaus, S.; Sciarra, R.; Re, A.; Tecchio, C.; et al. Time to progression of mantle cell lymphoma after high-dose cytarabine-based regimens defines patients risk for death. Br. J. Haematol. 2018, 185, 940–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bond, D.A.; Switchenko, J.M.; Villa, D.; Maddocks, K.; Churnetski, M.C.; Gerrie, A.S.; Goyal, S.; Shanmugasundaram, K.; Calzada, O.; Kolla, B.; et al. Early Relapse Identifies MCL patients with Inferior Survival after Intensive or Less Intensive Frontline Therapy. Blood Adv. 2021. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variation | Data (n = 156) | BR (n = 53) | R-BAC (n = 103) | p-Values |
|---|---|---|---|---|
| Median age (years) | 72 (53–80) | 73 (53–80) | 69 (54–80) | 0.012 |
| Sex | ||||
| Male | 109 (70%) | 37 (70%) | 72 (70%) | 0.890 |
| Female | 47 (30%) | 16 (30%) | 31 (30%) | |
| Ann Arbor stage | ||||
| I–II | 11 (10%) | 4 (8%) | 7 (7%) | 0.862 |
| III–IV | 145 (90%) | 49 (92%) | 96 (93%) | |
| Bone marrow involvement | ||||
| Yes | 127 (81%) | 52 (98%) | 75 (73%) | 0.623 |
| No | 29 (19%) | 1 (2%) | 28 (27%) | |
| Morphological variants | ||||
| Classical | 138 (89%) | 46 (87%) | 92 (89%) | 0.901 |
| Pleomorphic-Blastoid | 18 (11%) | 7 (13%) | 11 (11%) | |
| Ki 67 index | ||||
| <30% | 73 (47%) | 21 (40%) | 52 (50%) | 0.442 |
| ≥30% | 47 (30%) | 14 (26%) | 33 (32%) | |
| n.d. | 36 (23%) | 18 (34%) | 18 (18%) | |
| MIPI | ||||
| Low risk | 11 (7%) | 5 (10%) | 6 (6%) | 0.751 * |
| Intermediate risk | 45 (29%) | 15 (28%) | 30 (29%) | |
| High risk | 100 (64%) | 33 (62%) | 67 (65%) |
| Variation | BR (n = 53) | R-BAC (n = 103) | p-Value |
|---|---|---|---|
| Number of cycles | |||
| <4 | 8 (15%) | 2 (2%) | 0.001 |
| ≥4 | 11 (21%) | 41 (40%) | 0.016 |
| 6 | 34 (64%) | 60 (58%) | 0.474 |
| Dose reduction | |||
| ≥25% | 10 (19%) | 52 (51%) | 0.008 |
| Two-day schedule | 42 (41%) | ||
| Toxicities | |||
| Anaemia grade 3–4 | 8 (15%) | 32 (31%) | 0.121 |
| Neutropenia grade 3–4 | 20 (38%) | 49 (48%) | 0.531 |
| Thrombocytopenia grade 3–4 | 9 (17%) | 52 (50%) | 0.004 |
| Nonhaematological toxicity grade 3–4 | 13 (24%) | 25 (24%) | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bega, G.; Olivieri, J.; Riva, M.; Scapinello, G.; Paolini, R.; Finotto, S.; Sartori, R.; Lucchini, E.; Guandalini, G.; Facchinelli, D.; et al. Rituximab and Bendamustine (BR) Compared with Rituximab, Bendamustine, and Cytarabine (R-BAC) in Previously Untreated Elderly Patients with Mantle Cell Lymphoma. Cancers 2021, 13, 6089. https://doi.org/10.3390/cancers13236089
Bega G, Olivieri J, Riva M, Scapinello G, Paolini R, Finotto S, Sartori R, Lucchini E, Guandalini G, Facchinelli D, et al. Rituximab and Bendamustine (BR) Compared with Rituximab, Bendamustine, and Cytarabine (R-BAC) in Previously Untreated Elderly Patients with Mantle Cell Lymphoma. Cancers. 2021; 13(23):6089. https://doi.org/10.3390/cancers13236089
Chicago/Turabian StyleBega, Giulia, Jacopo Olivieri, Marcello Riva, Greta Scapinello, Rossella Paolini, Silvia Finotto, Roberto Sartori, Elisa Lucchini, Gianmarco Guandalini, Davide Facchinelli, and et al. 2021. "Rituximab and Bendamustine (BR) Compared with Rituximab, Bendamustine, and Cytarabine (R-BAC) in Previously Untreated Elderly Patients with Mantle Cell Lymphoma" Cancers 13, no. 23: 6089. https://doi.org/10.3390/cancers13236089
APA StyleBega, G., Olivieri, J., Riva, M., Scapinello, G., Paolini, R., Finotto, S., Sartori, R., Lucchini, E., Guandalini, G., Facchinelli, D., Tisi, M. C., Basso, M., Ballotta, L., Piazza, F., Ferrarini, I., & Visco, C. (2021). Rituximab and Bendamustine (BR) Compared with Rituximab, Bendamustine, and Cytarabine (R-BAC) in Previously Untreated Elderly Patients with Mantle Cell Lymphoma. Cancers, 13(23), 6089. https://doi.org/10.3390/cancers13236089