
Osteoradionecrosis of the Jaws Due to Teeth Extractions during and after Radiotherapy: A Systematic Review

 , ,
, ,  ,
,  , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Search Strategy and Selection of Studies
2.3. Data Collection
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
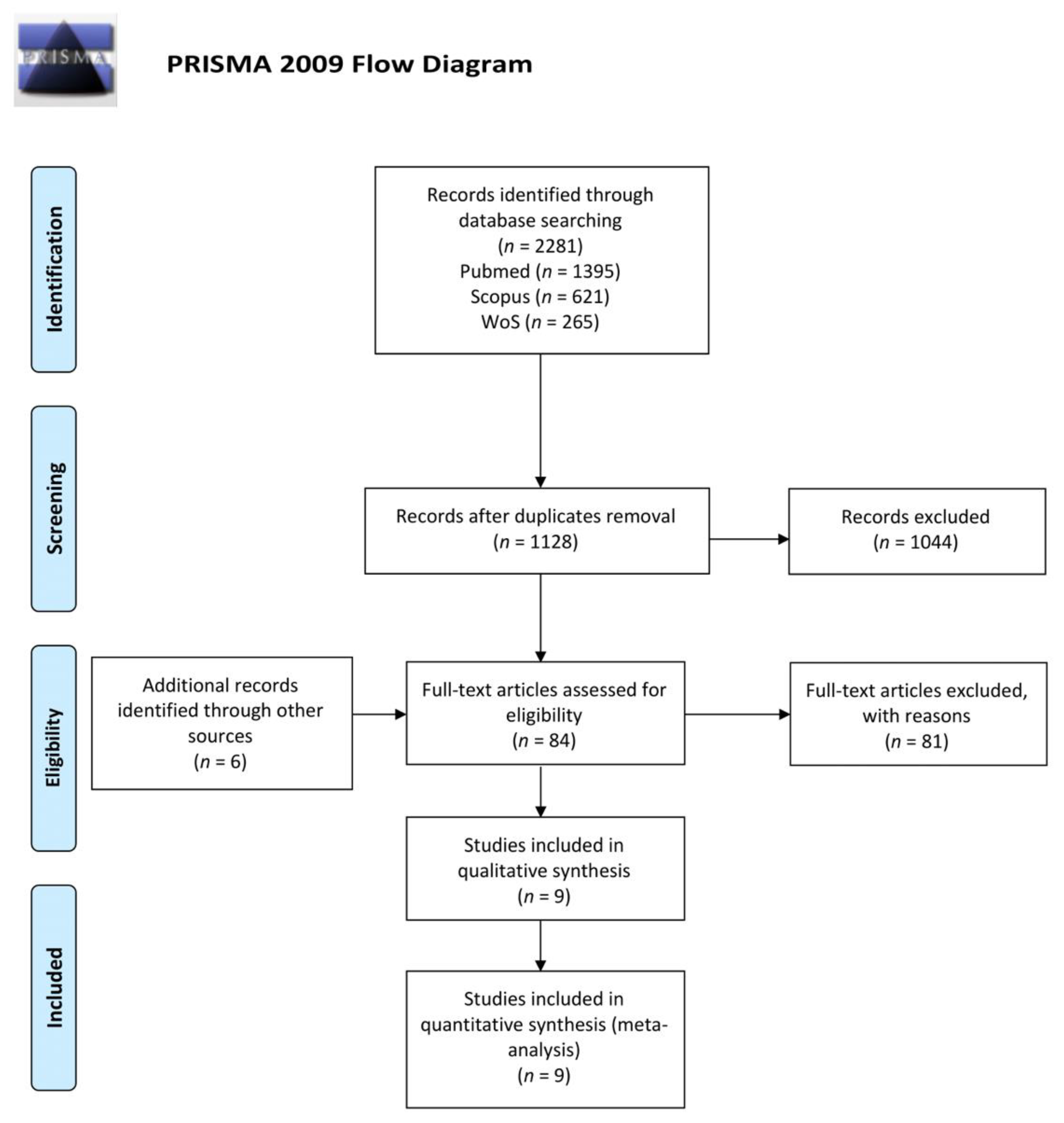
3.1. Results of Search and Study Selection
3.2. Study Characteristics and Summary of Results

{kind=link}
{kind=link}
| Study | Study Design | Included Patients | Mean Age | Mean Follow-Up | RT Technique | Mean Dose § | Patients Receiving Tooth Extraction | Cases of ORN | ORN Due to Tooth Extraction | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tot | M | F | Years | Months | EBR | IMRT | BT | Gy | n. | n. | n. | ||
| Morrish et al., 1981 [19] | R | 100 | 60 | 40 | 65 | 23 | 100 | 0 | 0 | 66 | 18 | 22 | 9 a |
| Beumer et al., 1983 [15] | R | 72 | - | - | - | * | 72 | 0 | 0 | - | 72 | 16 | 16 a |
| Marx et al., 1985 [20] | RCT | 74 | - | - | - | * | - | - | - | 68 | 74 | 13 | 13 b |
| Epstein et al., 1987 [21] | R | 146 | 103 | 43 | 54.7 | 60 | 140 | 0 | 6 | - | 54 | 8 | 3 a |
| Maxymiw et al., 1991 [12] | P | 72 | - | - | 57.4 | 57.6 | 72 | 0 | 0 | 50 | 72 | 0 | 0 b |
| Lambert et al., 1997 [22] | R | 47 | - | - | - | 35.3 | - | - | - | 60.6 | 46 | 0 | 0 b |
| David et al., 2001 [23] | R | 24 | 13 | 11 | 61 | 10.3 | - | - | - | - | 24 | 0 | 0 b |
| Ben-David et al., 2007 [14] | R | 176 | 128 | 48 | 55 | 35 | 0 | 176 | 0 | 54.6 | 13 | 0 | 0 c |
| Al-Bazie et al., 2016 [11] | R | 89 | 55 | 34 | 41.8 | 63 | - | - | - | 65.4 | 89 | 0 | 0 b |
| Study | Patients | Time from RT to Teeth Extraction | N. of Teeth Extraction | ORN Patients | ORN Sites | ||
|---|---|---|---|---|---|---|---|
| Months | Tot | Maxilla | Mandible | ||||
| Morrish et al., 1981 [19] | 18 | - | - | 9 | 9 | - | - |
| Beumer et al., 1983 [15] | 72 | 31 | 27 | 16 | 16 | 3 | 13 |
| Marx et al., 1985 [20] | 74 | - | 291 | 13 | 35 | 0 | 35 |
| Epstein et al., 1987 [21] | 54 | 32.4 | 173 | 3 | 3 | 0 | 3 |
| Maxymiw et al., 1991 [12] | 72 | - | 449 | 0 | 0 | 0 | 0 |
| Lambert et al., 1997 [22] | 46 | - | 704 | 0 | 0 | 0 | 0 |
| David et al., 2001 [23] | 24 | - | 54 | 0 | 0 | 0 | 0 |
| Ben-David et al., 2007 [14] | 13 | - | - | 0 | 0 | 0 | 0 |
| Al-Bazie et al., 2016 [11] | 89 | 15 | 232 | 0 | 0 | 0 | 0 |
3.3. Risk of Bias Assessment
| Cohort Studies | Selection | Comparability | Outcome | Modified Newcastle-Ottawa Score (Risk of Bias) | |||||||
| Author | Representativeness of cohort | Selection of non-exposed cohort | Ascertainment of exposure | Outcome of interest not present at onset | Control of confounding factors (extraction) | Control of confounding factors (field of radiation, timing, extraction protocol) | Assessment of outcome | Length of follow-up | Lost to follow-up | ||
| Morrish et al., 1981 [19] | x | x | x | x | x | x | x | x | 8 | ||
| Beumer et al., 1983 [15] | x | x | x | x | x | x | x | 7 | |||
| Epstein et al., 1987 [21] | x | x | x | x | x | x | x | 7 | |||
| Maxymiw et al., 1991 [12] | x | x | x | x | x | x | x | 7 | |||
| Lambert et al., 1997 [22] | x | x | x | x | x | x | 6 | ||||
| David et al., 2001 [23] | x | x | x | x | x | x | x | x | 8 | ||
| Ben-David et al., 2007 [14] | x | x | x | x | x | x | x | x | 8 | ||
| Al-Bazie et al., 2016 [11] | x | x | x | x | x | x | x | x | 8 | ||
| RCT Studies | Randomization | Blinding | Description of Withdrawal and Dropouts | Jadad Scale | |||||||
| Author | 1 point if randomization is mentioned | 1 point if the method of randomization is appropriate | Deduct 1 point if the method of randomization is inappropriate | 1 point if blinding is mentioned | 1 point if the method of blinding is appropriate | Deduct 1 point if the method of blinding is inappropriate | 1 point if withdrawal and dropouts are described | ||||
| Marx et al., 1985 [20] | x | ||||||||||
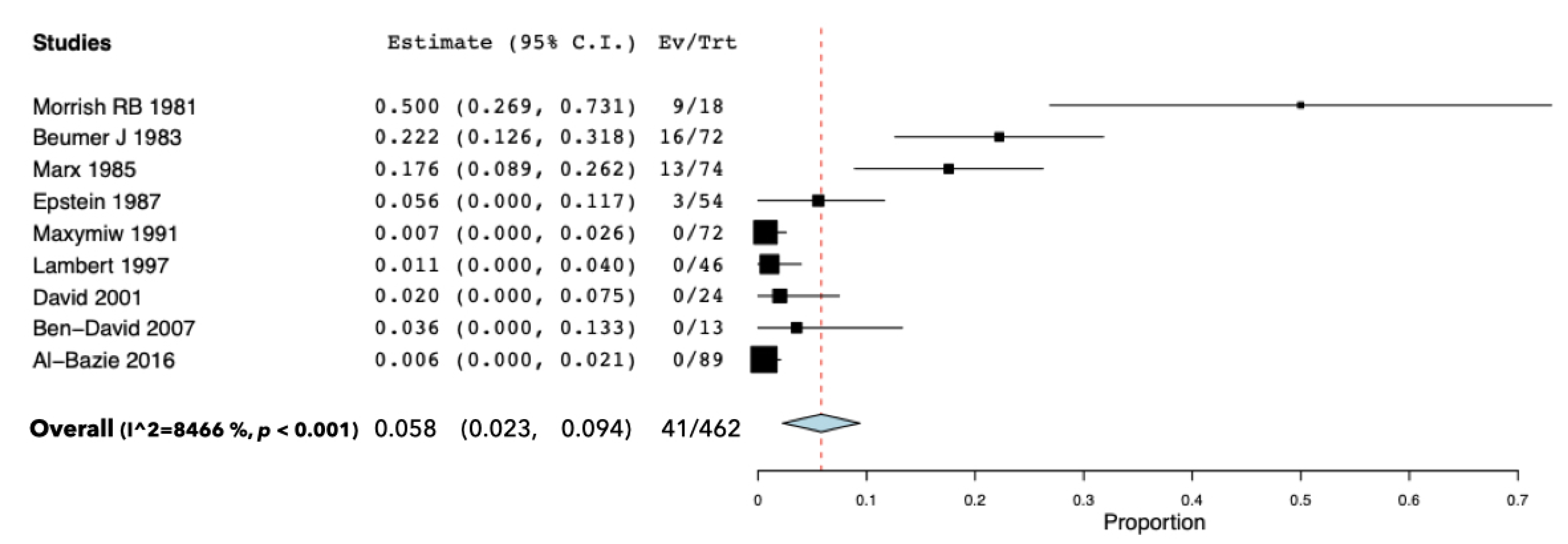
3.4. Results of Individual Studies
3.5. Excluded Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.; Torre, L.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries 2018. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Ratko, T.; Douglas, G.; de Souza, J.; Belinson, S.; Aronson, N. Radiotherapy Treatments for Head and Neck Cancer Update [Internet]; (Comparative Effectiveness Review, No. 144.); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2014. Available online: https://www.ncbi.nlm.nih.gov/books/NBK269018 (accessed on 14 November 2021).
- Kielbassa, A.; Hinkelbein, W.; Hellwig, E.; Meyer-Lückel, H. Radiation-related damage to dentition. Lancet Oncol. 2006, 7, 326–335. [Google Scholar] [CrossRef]
- Nadella, K.; Kodali, R.; Guttikonda, L.; Jonnalagadda, A. Osteoradionecrosis of the Jaws: Clinico-Therapeutic Management: A Literature Review and Update. J. Maxillofac. Oral Surg. 2015, 14, 891–901. [Google Scholar] [CrossRef]
- Chronopoulos, A.; Zarra, T.; Ehrenfeld, M.; Otto, S. Osteoradionecrosis of the jaws: Definition, epidemiology, staging and clinical and radiological findings. A concise review. Int. Dent. J. 2018, 68, 22–30. [Google Scholar] [CrossRef]
- Marx, R. Osteoradionecrosis: A new concept of its pathophysiology. J. Oral Maxillofac. Surg. 1983, 41, 283–288. [Google Scholar] [CrossRef]
- Miniello, T.G.; Araújo, J.P.; Silva, M.L.G.; Paulo Kowalski, L.; Rocha, A.C.; Jaguar, G.C.; Abreu Alves, F. Influence of bisphosphonates on clinical features of osteoradionecrosis of the maxilla and mandible. Oral Dis. 2019, 25, 1344–1351. [Google Scholar] [CrossRef]
- Delanian, S.; Lefaix, J. The radiation-induced fibroatrophic process: Therapeutic perspective via the antioxidant pathway. Radiother. Oncol. 2004, 73, 119–131. [Google Scholar] [CrossRef]
- Nabil, S.; Samman, N. Incidence and prevention of osteoradionecrosis after dental extraction in irradiated patients: A systematic review. Int. J. Oral Maxillofac. Surg. 2011, 40, 229–243. [Google Scholar] [CrossRef]
- Marx, R.; Johnson, R. Studies in the radiobiology of osteoradionecrosis and their clinical significance. Oral Surg. Oral Med. Oral Pathol. 1987, 64, 379–390. [Google Scholar] [CrossRef]
- Al-Bazie, S.; Bahatheq, M.; Al-Ghazi, M.; Al-Rajhi, N.; Ramalingam, S. Antibiotic protocol for the prevention of osteoradionecrosis following dental extractions in irradiated head and neck cancer patients: A 10 years prospective study. J. Cancer Res. Ther. 2016, 12, 565–570. [Google Scholar] [CrossRef]
- Maxymiw, W.; Wood, R.; Liu, F. Post-radiation dental extractions without hyperbaric oxygen. Oral Surg. Oral Med. Oral Pathol. 1991, 72, 270–274. [Google Scholar] [CrossRef]
- Buglione, M.; Cavagnini, R.; Di Rosario, F.; Sottocornola, L.; Maddalo, M.; Vassalli, L.; Magrini, S.M. Oral toxicity management in head and neck cancer patients treated with chemotherapy and radiation: Dental pathologies and osteoradionecrosis (Part 1) literature review and consensus statement. Crit. Rev. Oncol. Hematol. 2016, 97, 131–142. [Google Scholar] [CrossRef] [PubMed]
- Ben-David, A.; Diamante, M.; Radawski, J.; Vineberg, K.; Stroup, C.; Murdoch-Kinch, C.; Eisbruch, A. Lack of Osteoradionecrosis of the Mandible after IMRT for Head and Neck Cancer: Likely Contributions of both Dental Care and Improved Dose Distribution. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 392–402. [Google Scholar] [CrossRef]
- Beumer, J.; Harrison, R.; Sanders, B.; Kurrasch, M. Postradiation Dental Extractions: A Review of the Literature and A Report of 72 Episodes. Head Neck Surg. 1983, 6, 581–586. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Jadad, A.; Moore, R.; Carroll, D.; Jenkinson, C.; Reynolds, D.; Gavaghan, D.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Morrish, R.J.; Chan, E.; Silverman, S.J.; Meyer, J.; Fu, K.; Greenspan, D. Osteonecrosis in patients irradiated for head and neck carcinoma. Cancer 1981, 47, 1980–1983. [Google Scholar] [CrossRef]
- Marx, R.; Johnson, R.; Kline, S. Prevention of osteoradionecrosis: A randomized prospective clinical trial of hyperbaric oxygen versus penicillin. J. Am. Dent. Assoc. 1985, 111, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.; Rea, G.; Wong, F.; Spinelli, J.; Stevenson-Moore, P. Osteonecrosis: Study of the relationship of dental extractions in patients receiving radiotherapy. Head Neck Surg. 1987, 10, 48–54. [Google Scholar] [CrossRef]
- Lambert, P.; Intriere, N.; Eichstaedt, R. Management of dental extractions in irradiated jaws: A protocol with hyperbaric oxygen therapy. J. Oral Maxillofac. Surg. 1997, 55, 268–274. [Google Scholar] [CrossRef]
- David, L.; Sàndor, G.; Evans, A.; Brown, D. Hyperbaric oxygen therapy and mandibular osteoradionecrosis: A retrospective study and analysis of treatment outcomes. J. Can. Dent. Assoc. 2001, 67, 384. [Google Scholar]
- Schweiger, J. Oral complications following radiation therapy: A five-year retrospective report. J. Prosthet. Dent. 1987, 58, 78–82. [Google Scholar] [CrossRef]
- Saito, I.; Hasegawa, T.; Kawashita, Y.; Kato, S.; Yamada, S.I.; Kojima, Y.; Ueda, N.; Umeda, M.; Shibuya, Y.; Kurita, H.; et al. Association between dental extraction after radiotherapy and osteoradionecrosis: A multi-centre retrospective study. Oral Dis. 2021, in press. [Google Scholar] [CrossRef]
- Kubota, H.; Miyawaki, D.; Mukumoto, N.; Ishihara, T.; Matsumura, M.; Hasegawa, T.; Akashi, M.; Kiyota, N.; Shinomiya, H.; Teshima, M.; et al. Risk factors for osteoradionecrosis of the jaw in patients with head and neck squamous cell carcinoma. Radiat. Oncol. 2021, 16, 1. [Google Scholar] [CrossRef]
- Gomez-Millan, J.; Fernández, J.; Medina Carmona, J. Current status of IMRT in head and neck cancer. Rep. Pract. Oncol. Radiother. 2013, 20, 361–365. [Google Scholar] [CrossRef][Green Version]
- Schuurhuis, J.; Stokman, M.; Witjes, M.; Dijkstra, P.; Vissink, A.; Spijkervet, F. Evidence supporting pre-radiation elimination of oral foci of infection in head and neck cancer patients to prevent oral sequelae. A systematic review. Oral Oncol. 2015, 51, 212–220. [Google Scholar] [CrossRef]
- Brennan, M.; Woo, S.; Lockhart, P. Dental treatment planning and management in the patient who has cancer. Dent. Clin. North Am. 2008, 52, 19–37. [Google Scholar] [CrossRef] [PubMed]
- Lajolo, C.; Gioco, G.; Rupe, C.; Troiano, G.; Cordaro, M.; Lucchese, A.; Giuliani, M. Tooth extraction before radiotherapy is a risk factor for developing osteoradionecrosis of the jaws: A systematic review. Oral Dis. 2020, 27, 1595–1605. [Google Scholar] [CrossRef]
- Beaumont, S.; Bhatia, N.; McDowell, L.; Fua, T.; McCullough, M.; Celentano, A.; Yap, T. Timing of dental extractions in patients undergoing radiotherapy and the incidence of osteoradionecrosis: A systematic review and meta-analysis. Br. J. Oral Maxillofac. Surg. 2021, 59, 511–523. [Google Scholar] [CrossRef]
- Schuurhuis, J.; Stokman, M.; Roodenburg, J.; Reintsema, H.; Langendijk, J.; Vissink, A.; Spijkervet, F.K. Efficacy of routine pre-radiation dental screening and dental follow-up in head and neck oncology patients on intermediate and late radiation effects. A retrospective evaluation. Radiother. Oncol. 2011, 101, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Batstone, M.; Cosson, J.; Marquart, L.; Acton, C. Platelet rich plasma for the prevention of osteoradionecrosis. A double blinded randomized cross over controlled trial. Int. J. Oral Maxillofac. Surg. 2012, 41, 2–4. [Google Scholar] [CrossRef]
- Teng, M.; Futran, N. Osteoradionecrosis of the mandible. Curr. Opin. Otolaryngol. Head Neck Surg. 2005, 13, 217–221. [Google Scholar] [CrossRef]
- Støre, G.; Boysen, M. Mandibular Osteoradionecrosis: Clinical behaviour and diagnostic aspects. Clin. Otolaryngol. Allied Sci. 2000, 25, 378–384. [Google Scholar] [CrossRef]
- Saia, G.; Blandamura, S.; Bettini, G.; Tronchet, A.; Totola, A.; Bedogni, G.; Bedogni, A. Occurrence of bisphosphonate-related osteonecrosis of the jaw after surgical tooth extraction. J. Oral Maxillofac. Surg. 2010, 68, 797–804. [Google Scholar] [CrossRef]
- Hinchy, N.; Jayaprakash, V.; Rossitto, R.; Anders, P.; Korff, K.; Canallatos, P.; Sullivan, M.A. Osteonecrosis of the jaw—Prevention and treatment strategies for oral health professionals. Oral Oncol. 2013, 49, 878–886. [Google Scholar] [CrossRef]
- Shaw, R.; Butterworth, C. Hyperbaric oxygen in the management of late radiation injury to the head and neck. Part II: Prevention. Br. J. Oral Maxillofac. Surg. 2011, 49, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Chuang, S. Limited evidence to demonstrate that the use of hyperbaric oxygen (HBO) therapy reduces the incidence of osteoradionecrosis in irradiated patients requiring tooth extraction. J. Evid. Based Dent. Pract. 2012, 12 (Suppl. S3), 248–250. [Google Scholar] [CrossRef] [PubMed]
- Lyons, A.; Ghazali, N. Osteoradionecrosis of the jaws: Current understanding of its pathophysiology and treatment. Br. J. Oral Maxillofac. Surg. 2008, 46, 653–660. [Google Scholar] [CrossRef]


| Inclusion Criteria |
| Full papers, literature in English language, published after 1978 in peer-reviewed journals |
| Observational clinical studies, both prospective and retrospective (cohort and case-control), and RCTs |
| Minimum sample size of 10 patients who underwent tooth extractions after radiotherapy in an H&N district |
| No previous ORN at the extraction site |
| Mean 6 months follow-up after tooth extractions |
| Unhealed sockets followed up for at least 3 months |
| Exclusion criteria |
| Case reports, reviews, cross-sectional studies |
| Studies in which no clear definition of ORN was reported |
| Studies not specifying whether ORN developed at the extraction site. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lajolo, C.; Rupe, C.; Gioco, G.; Troiano, G.; Patini, R.; Petruzzi, M.; Micciche’, F.; Giuliani, M. Osteoradionecrosis of the Jaws Due to Teeth Extractions during and after Radiotherapy: A Systematic Review. Cancers 2021, 13, 5798. https://doi.org/10.3390/cancers13225798
Lajolo C, Rupe C, Gioco G, Troiano G, Patini R, Petruzzi M, Micciche’ F, Giuliani M. Osteoradionecrosis of the Jaws Due to Teeth Extractions during and after Radiotherapy: A Systematic Review. Cancers. 2021; 13(22):5798. https://doi.org/10.3390/cancers13225798
Chicago/Turabian StyleLajolo, Carlo, Cosimo Rupe, Gioele Gioco, Giuseppe Troiano, Romeo Patini, Massimo Petruzzi, Francesco Micciche’, and Michele Giuliani. 2021. "Osteoradionecrosis of the Jaws Due to Teeth Extractions during and after Radiotherapy: A Systematic Review" Cancers 13, no. 22: 5798. https://doi.org/10.3390/cancers13225798
APA StyleLajolo, C., Rupe, C., Gioco, G., Troiano, G., Patini, R., Petruzzi, M., Micciche’, F., & Giuliani, M. (2021). Osteoradionecrosis of the Jaws Due to Teeth Extractions during and after Radiotherapy: A Systematic Review. Cancers, 13(22), 5798. https://doi.org/10.3390/cancers13225798